

Abstract
Introduction:
Interpersonal trust behavior is an important target for the identification and treatment of psychiatric disorders with interpersonal dysfunction. Adolescent depression is a highly interpersonal disorder marked by impaired social interactions. However, trust has received little empirical attention. The examination of reward-related decision-making using behavioral economic methods is a relatively novel approach for studying trust in adolescent depression. The present study employed a modified trust game to examine whether depressive adolescents exhibited perturbed reward-related decision-making in social and/or nonsocial contexts.
Methods:
One-hundred and thirty adolescent girls (65 depressive, 65 healthy comparisons) played a modified trust game under two conditions, interpersonal risk-taking (trust) and general risk-taking (lottery), and completed self-report psychopathology measures.
Results:
Three-way repeated measures ANCOVA analyses revealed a significant group x game interaction such that while the depressive group invested more across trials in the trust game they invested similarly to healthy comparisons in the lottery condition.
Discussion:
Findings highlight the interpersonal nature of adolescent depression. Future research may help determine whether increased trust behavior is characteristic of depression in adolescent girls. Behavioral economic games, like the trust game, may serve as valuable therapeutic tools for improving social interaction style among depressive adolescents.
Keywords: Major Depressive Disorder, MDD, adolescence, social reward, decision-making
Introduction
Adolescent depression is a highly interpersonal disorder marked by impaired social interactions (Davey, Yücel, & Allen, 2008; Joiner, 1999; Mufson, Dorta, Moreau, & Weissman, 2011). Depressed adolescents have shown to be more critical in their interaction style, evoking negative emotional and behavioral reactions in their partners, resulting in more rejection and less popularity among their peers (Baker, Milich, & Malonis, 1996; Connolly, Geller, Marton, & Kutcher, 1992). Researchers have naturally turned to the study of social cognition, or the mental processes involved in perceiving, attending to, remembering, thinking about, and making sense of the people in our social world (Moskowitz 2005), in an effort to elucidate interpersonal impairment in adolescent depression. Social-cognitive deficits have been evidenced (Kyte & Goodyer, 2008), however, Weightman and colleagues’ (2014) review of the greater depression literature reveals discrepant findings across several aspects of social cognition. Although there appears to be an inverse relation between depression severity and social-cognitive performance (i.e., on mental state inference and emotion identification), a number of studies did not yield findings supporting this trend, showing non-significant differences in task performance between depressed and control groups.
Theoretical and methodological limitations of traditional social-cognitive approaches may help explain these discrepancies (Sharp, 2012). Theoretically, social cognition has been widely assumed to exist within an individual rather than occurring as a dynamic interaction between individuals. As such, traditional social-cognitive methods include a single individual, in isolation, who performs under largely hypothetical scenarios thus ignoring the moment-to-moment mental state inferences required during real-life social interactions. The hypothetical nature of traditional social-cognitive tasks therefore limits participant emotional and behavioral investment. In addition, the use of retrospective self-report of social interactions, or predictions of future social behavior under hypothetical scenarios, is subject to reporter bias and/or to the expression of socially desirable responses. Re-conceptualizing social cognition as reward-related decision-making is a relatively novel, alternative methodological approach (Sharp, 2012; Sharp, Monterosso, & Montague, 2012). This approach relies on the tools (games) of behavioral economics to examine real-time interpersonal interaction with real-life consequences.
Social behavioral economic games, or “games of social exchange” (Camerer, 2003) typically include two players, with one or both deciding how to divide some currency between them to maximize pay-offs. The game outcome provides a numerical representation of players’ preferences (Camerer 2003). Game theory informs these games which serve as ecologically-valid proxies for real-world social interaction and provide a means to mathematically predict, explain, and prescribe human behavior (Sharp et al., 2012; Camerer, 2003). Players’ in-game strategic interaction decisions require them to infer co-player mental states. This makes social behavioral economic games excellent tools for probing a range of constructs (i.e., interpersonal trust, reciprocity, and fairness), higher-order social cognition, and potential social-cognitive biases (Lee & Harris, 2013; Frith & Singer, 2008; Fehr & Camerer, 2007; Sharp, 2012; King-Casas & Chiu, 2012). As explained by Mellick, Sharp, and Ernst (2015), these games can parametrically delineate important interpersonal mechanisms that may maintain or exacerbate adolescent depression.
Interpersonal trust (hereon referred to as trust) is a particularly promising target for the identification and treatment of psychiatric disorders with deficits in interpersonal functioning because trust is essential for productive social interaction and exchange (Montague, Lohrenz, & Dayan, 2015). The traditional trust game (Berg, Dickhaut, & McCabe, 1995) is the behavioral economic tool for studying trust and involves two players, an investor and a trustee. The investor starts the game with an endowment from which s/he invests some portion in the trustee (x). The amount is tripled (3x) as it is sent to the trustee. The trustee then decides how much of the tripled amount to keep and how much to repay the investor. S/he may keep everything if s/he so chooses. The investor’s initial investment in the trustee is indicative of trust because there is no assurance of (“sufficient”) repayment. This uncertainty qualifies trust as risky (Camerer, 2003). Per King-Casas and Chiu (2012), and in support of reclassifying psychiatric disorders on dimensions of observable behavior, quantitative benchmarks of normative behavior can be developed using aggregate trust game data against which pathological deviations can be evaluated and supported or rejected.
Early evidence suggests depression may be characterized by increased trust game investments (Mellick et al., 2015; Koshelev et al., 2010). Indeed, Koshelev and colleagues’ (2010) study recruited adult patient samples to play the trust game as investors with healthy control trustee co-players. Patient diagnoses were successfully identified using quantitative interaction data, including major depressive disorder which was classified by greater investments and repayments. The only other two known adult depression trust game studies, with depressed players acting as investors, resulted in non-significant findings probably related to insufficient statistical power (Unoka et al., 2009) and low level of depression severity (Clark, Thorne, Hardy, & Cropsey, 2013). Although depression effects were null in Unoka et al. (2009), there was a main effect of trials such that both healthy and depressed players exhibited a linear increase in investments over time.
Despite mixed findings in adult depression, there is good reason to expect positive findings, by way of increased trust, in adolescent depression (Mellick et al., 2015). The directionality of this association would be consistent with Koshelev et al. (2010) and other adult depression behavioral economic findings, with other games, showing depressed players to make greater allocations to co-players than healthy controls (Destoop et al., 2012; Scheele et al. 2013). Atypical trust would expectedly align with interpersonal and interactional theories of depression whereby deviations from normative social behavior, covering various facets of interpersonal interaction, contribute to impaired social functioning and rejection in depression (Coyne, 1976; Joiner, 1999; Downey & Feldman, 1996). One example, for instance, may be that depressed adolescent players, potentially higher in rejection sensitivity (Feldman & Downey, 1996), make greater investments in the trust game to maintain interpersonal connection in the threat of exclusion (Allen & Badcock, 2003; Destoop et al., 2012).
Developmental and social-cognitive neuroscience research lends additional support for this working hypothesis. This literature shows adolescence to be a unique period in which social cognition and trust undergo significant maturational changes (van den Bos, Westenberg, van Dijk, & Crone, 2010). Social cognition becomes more “finely tuned” while trust increases across adolescence (Crone, 2013). The “social reorientation” of adolescence, where the focus shifts from parents to peers, occurs with parallel changes in neurobiology (i.e., reward system maturation) and social decision-making (Nelson et al., 2005; Steinberg, 2005; Galván, 2010). Trust stands out as a critical process in these collective processes. Whether trust (interpersonal risk-taking) and/or risk-taking in general is anomalous in adolescent depression is an important consideration (Lee & Harris, 2013; Unoka et al., 2009). Though general risk-taking behavior did not distinguish depressed players in Unoka et al. (2009), other decision-making studies (i.e., Smoski et al., 2008) suggest risk aversion in nonsocial contexts is present in depression.
Against this background, the present study employed a modified version of the original trust game (Unoka et al., 2009; Kosfeld, Heinrichs, Zak, Fishcbacher, & Fehr, 2005) to examine reward-related decision making in social (trust) and nonsocial (lottery) contexts in adolescent depression. Adolescent girls were specifically recruited since depression begins to disproportionately affect females during adolescence (Rudolph & Flynn, 2009). Hypotheses were three-fold: (1) Depressive adolescent girls, relative to healthy comparisons, would invest more in the trust game. (2) Depressive, relative to healthy, adolescent girls would invest less in the trust game in the nonsocial (lottery) condition. (3) Consistent with Unoka et al. (2009) and other behavioral economic research (Camerer, 2003), a linear increase in investments across trials was expected irrespective of group.
Methods
Participants and Procedures
The present study recruited 130 adolescent girls (65 Depressive, 65 healthy comparisons [HCs]) for participation. Table 1 provides an overview of the samples with respect to sociodemographic and clinical characteristics. Differences in racial composition between groups was apparent with more Caucasian participants in the depressive group and more Asian participants in the HC group. Depressive participants were required to report mild depression (total score ≥ 14) on the Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996) and score above clinical cut-off (t-score ≥ 65) for Affective Problems on the Youth Self-Report (YSR; Achenbach & Rescorla, 2001). HCs, in turn, were to report no clinically significant elevations on the YSR Affective Problems and Total Problems scales, and scores below cut-off for mild depression on the BDI-II. Further inclusion criteria required all participants to be between 12 and 18 years of age, be fluent in English, possess sufficient reading skills as determined by the Wide Range Achievement Test–Version 4 (WRAT-IV; Wilkonson & Robertson, 2006), and have adequate cognitive capacity to participate, defined as absence of schizophrenia spectrum disorder and mental retardation. Failure to meet all inclusion criteria resulted in exclusion from the study.
Table 1.
Participant characteristics and group comparisons
| Depressive (n = 65) |
HC (n = 65) |
t/F/χ2 | P | d | |
|---|---|---|---|---|---|
| Age | 15.02 (1.17) | 15.12 (1.11) | 0.539 | 0.591 | 0.088 |
| BDI-II | 38.43 (7.02) | 5.74 (3.26) | 924.169 | < 0.001 | 5.743 |
| YSR Affective | 77.86 (9.27) | 51.63 (2.96) | 377.347 | < 0.001 | 3.811 |
| YSR Anxiety | 62.95 (8.88) | 52.60 (3.45) | 64.423 | < 0.001 | 1.536 |
| YSR Externalizing | 64.97 (8.55) | 44.57 (9.06) | 146.761 | < 0.001 | 2.316 |
| Race | 37.417 | 0.521 | |||
| African American | 12 (18.5%) | 19 (29.2%) | < 0.001 | ||
| Caucasian | 26 (40.0%) | 7 (10.8%) | |||
| Latina/Hispanic | 19 (29.2%) | 17 (26.2%) | |||
| Asian | 2 (3.1%) | 22 (33.8%) | |||
| Other | 6 (9.2%) | 0 |
Note: Data are mean (standard deviation) aside from race. Independent t-test performed on age, Chi-square test of independence performed on race, and ANCOVAs controlling for age and race performed on symptom variables. Effect sizes reported as Cohen’s d aside for race, which is reported as Cramer’s V statistic.
The appropriate institutional review boards approved this study. Depressive patients were recruited from the adolescent acute inpatient unit of a 16-bed county psychiatric hospital. Recruitment began upon admission where parents were asked to provide consent, and, if given, adolescents were approached for assent. Assessments on the unit were routinely completed within 2–3 days of admission in quiet, private rooms well removed from the unit’s community area. HCs were recruited separately from local high schools through various means, in the same community served by the psychiatric hospital. For instance, local school board approval was received so that, with teacher approval, research staff were able to present the study to students and answer any questions. Take-home packets containing study information, consent, and assent forms were provided for interested students whom completed them with parent(s). Assessments were then scheduled and completed during school hours in a private area of the school library. Research staff also formed a partnership with a local youth venture scout group chapter to bolster recruitment. Clinical psychology graduate students (or other research staff) conducted assessments only after completing training under supervision of the principal investigator. Participation was completely voluntary and withdrawal was permitted without justification. A $40 gift card to a popular nation-wide retail department store chain was provided as compensation.
Measures
Social and non-social risk-taking
A modified version of the trust game (Unoka et al., 2009) was played under two counterbalanced conditions, each consisting of five consecutive trials. One condition (social condition) assessed interpersonal trust exchanges, i.e., interpersonal risk-taking, between the participant and an anonymous peer co-player (fictional) over the internet. An anonymous peer co-player was chosen as anonymity begets generalized trust, which underlies all social interactions (Rotenberg et al., 2005; van den Bos et al., 2010). In each round, the participant, always acting as the investor, allocated anywhere between 0 and 12 monetary units (MUs) to their co-player (the trustee). The investor kept as many MUs as they desired (x) and sent the remaining MUs (12 – x) to the anonymous trustee. As MUs were sent, they were tripled along the way, 3(12 – x). Participants were told that the trustee would then decide how many MUs to send back to the investor for each trial. In the second condition (nonsocial condition), the structure of the game was identical. Instead of a fictional person, however, a lottery system was used in this nonsocial condition. Participants were told that a computerized lottery system would randomly determine repayment. The amount of MUs invested by the participant (x) indicated the degree of trust in the other player or degree of general risk-taking in the lottery condition. During both conditions, subjects did not receive feedback after each trial regarding amount of repayment of investments. The absence of feedback creates uncertainty in the outcome of the decision-making therefore ensuring risk-taking (Kosfeld et al., 2005).
Game administration
Games were explained to participants via power-point presentation, and participants were informed that the objective of each game was to earn as many MUs as possible, but that they would not be told of their cumulative earnings until afterwards. Players were informed that the order of games would be randomly determined. Participants’ demonstration of understanding of game rules was required prior to administration. The assessor then pretended to contact a co-administrator, via phone call or text message, to ensure that the (fictional) trustee was “logged on” to play. Games were designed to mimic an online computer game and were played on Inquisit 2.0 software (Seattle, WA). Participants were first presented with a screen that confirmed they were being connected to the game (i.e., “Please wait while the other player logs on…”). After each trial investment, participants were told to please wait while the other player (or lottery) determined how many points were sent back. Afterwards, research staff asked participants the degree to which they believed they were playing with another teenager over the internet, which was rated on a 1 to 7 scale (“Did not believe at all” to “Totally believed”). Given that deception was used (there was no trustee and cumulative points were not calculated), players were debriefed immediately following administration and asked not to share details about the task with others. Debriefing was conducted ethically in compliance with accepted standards (Wendler & Miller, 2004).
Psychopathology
Depression, anxiety, and externalizing psychopathology symptoms were assessed with the YSR (Achenbach & Rescorla, 2001), which is suitable for adolescents aged 11 to 18 years. The Affective Problems scale score confirmed the presence or absence of clinically-significant depressive symptoms. The Anxiety Problems and Externalizing Problems scale scores were utilized in group comparisons and also served as covariates. Cronbach’s alpha, internal consistency, in the current study was α = 0.92 for Affective Problems, α = 0.74 for Anxiety Problems, and α = 0.94 for Externalizing Problems.
The BDI-II (Beck et al., 1996), in addition to the YSR Affective Problems, determined group assignment. Specifically, the presence or absence of significant depressive symptoms was determined using the mild depression BDI-II cut-off. Both internal consistency (r = .92) and stability (r = .93) for the BDI-II have been demonstrated (Beck et al., 1996). Cronbach’s alpha in the current study was α = 0.97.
Data analytic strategy
Chi-square tests of independence and independent samples t-tests compared groups on sociodemographic and clinical variables with effect sizes reported in Cohen’s d and Cramer V statistics, respectively. Analyses of covariance (ANCOVAs) compared groups’ mean game investments. A three-way repeated measures ANCOVA, with group as the between-subjects factor and game type and trials as within-subject factors, was performed to test for game order effects and for primary analyses with effect sizes reported in partial-eta squared (η2). Effect sizes for η2 were considered small, medium, or large at values of 0.01, 0.06, and 0.14, respectively (Cohen, 1988; Miles & Shevlin, 2001). Multiple covariates were included in analyses to reduce within-group error variance and provide a clearer effect of depression on game investments (Field, 2016). Age was included as a covariate of nuisance because of its strong relation to adolescent trust and known effects on gameplay (Crone, 2013; Gorrese, 2016; Camerer, 2003). Anxiety symptoms were included because they highly co-occur with depression (Kessler, Avenevoli, & Merikangas, 2001). Lastly, externalizing symptoms were included because they are frequently present among inpatients and may influence trust game behavior (Sharp, Ha, & Fonagy, 2011; Sharp et al., 2016). The identification of these covariates was both a priori and objective (Pocock et al., 2002).
Results
Participant characteristics
Table 1 summarizes participant characteristics and group comparison results. Groups significantly differed in racial composition, χ2 (4, N = 130) = 37.417, p < 0.001, with the HC group consisting of more Asian, p < 0.001, White, p < 0.001, and Other-identified participants, p = 0.028. This warranted statistically controlling for race in subsequent analyses. The depressive group reported significantly higher scores on the YSR Affective, Anxiety, and Externalizing Problems scales as well as on the BDI-II, ps < 0.001. BDI-II scores for depressive girls were in the severe range on average (≥ 29; Beck et al., 1996) with the minimum score in the moderate range (see Table 1).
Testing for an order effect
Game order effects were tested (i.e. trust followed by lottery, lottery followed by trust) prior to conducting primary analyses. Mean investments did not vary as a function of game order: trust game first, F (1, 124) = 1.868, p = 0.174; lottery condition first, F (1, 124) = 0.585, p = 0.446. Moreover, there were no significant order-based main effects or interactions, ps ≥ 0.104, per repeated-measures ANCOVA results.
Trust and lottery investment
A full factorial three-way repeated-measures ANCOVA, controlling for age, race, YSR Anxiety and Externalizing Problems, revealed a significant group x game interaction, F (1, 122) = 3.93, p = 0.050, η2 = 0.031, such that while both groups invested similarly in the lottery condition, depressive girls invested significantly more across trials (over time) in the trust game (see Figures 1 and 2). There was a main effect of group on mean trust game investment, depressive girls (Marginal Mean [MM] = 4.82, Standard Error [SE] = 0.33, 95% CI [4.18, 5.46]) versus HCs (MM = 3.64, SE = 0.33, 95% CI, [3.01, 4.28]), F (1, 122) = 4.40, p = 0.038, η2 = 0.035. In contrast, there was no group effect on mean lottery condition investment, depressive girls (MM = 4.53, SE = 0.34, 95% CI [3.87, 5.19]) versus HCs (MM = 4.00 MUs, SE = 0.34, 95% CI [3.33, 4.66]), F (1, 122) = 0.841, p = 0.361, η2 = 0.007. Exploratory post-hoc tests with Bonferroni correction revealed that it was not until trial 3 when the depressive group (MM = 4.83, SE = 0.40) invested significantly more than HCs (MM = 3.46, SE = 0.40) in the trust game, p = 0.047, η2 = 0.032. While group differences were non-significant in trial 4 (p = 0.365), a significant difference again emerged in trial 5 with the depressive girls (MM = 5.67, SE = 0.48) investing more than HCs (M = 3.16, SE = 0.48), p = 0.003, η2 = 0.069. Thus, depressive girls’ increased investment became apparent as the game progressed with the difference becoming larger with time.
Figure 1.
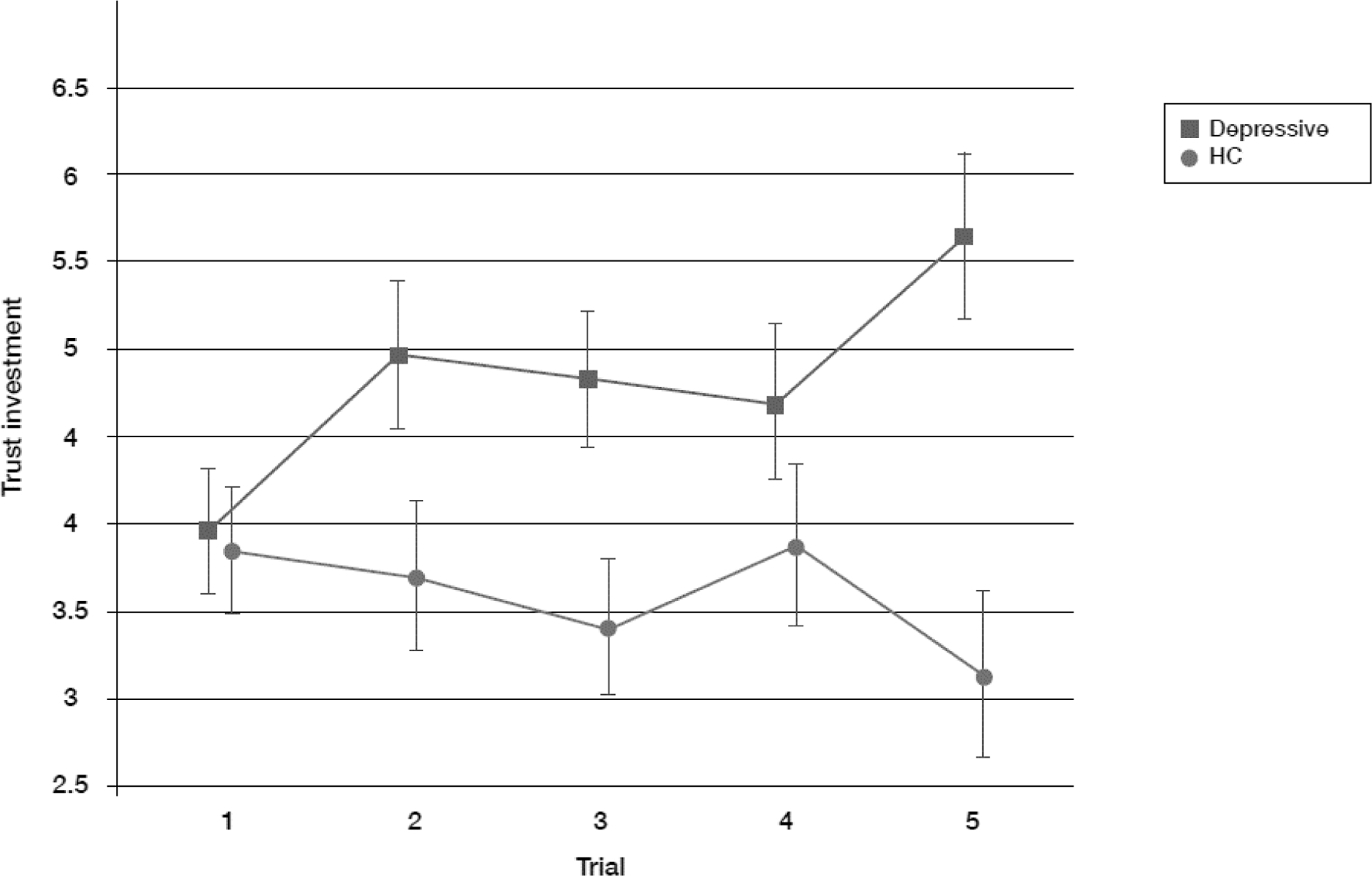
Mean trust investments across trials by group
Marginal mean investments (in MUs) presented with standard error bars.
Figure 2.
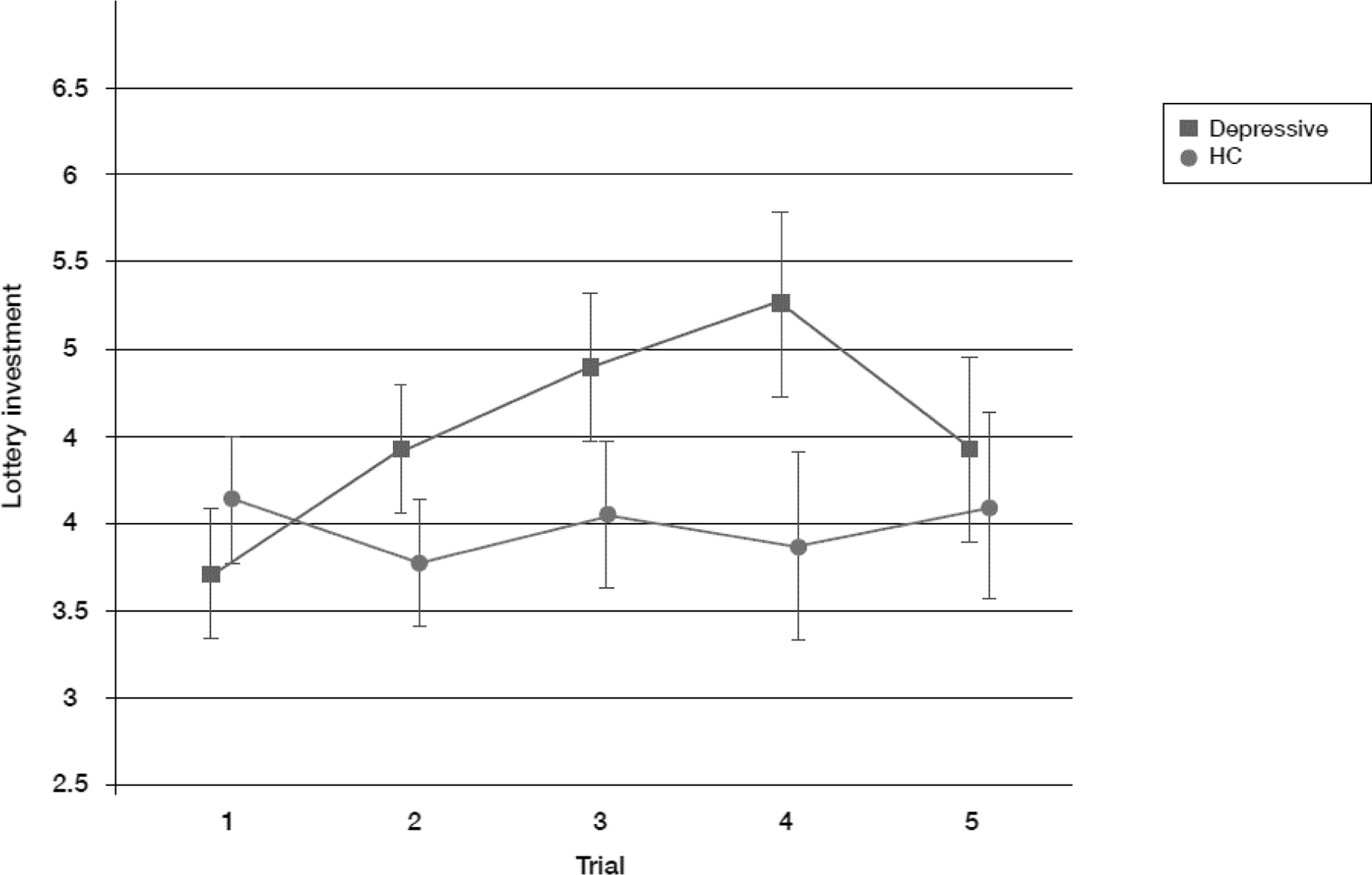
Mean lottery investments across trials by group
Marginal mean investments (in MUs) presented with standard error bars.
Although the group x game x trials interaction was non-significant (p = 0.163, η2 = 0.014), the game x trials interaction was significant, F (1, 123) = 3.02, p = 0.024, η2 = 0.024, and mirrored results from the group x game interaction, such that significant differences between games emerged later on. Specifically, the increased investment in the trust game was evident between trials 3 through 5 (3 to 4, p = 0.047, η2 = 0.032; 4 to 5, p = 0.003, η2 = 0.069) whereas no such statistically significant increase was observed in the lottery condition. The group x trials interaction as well as all other interactions and main effects were non-significant (ps ≥ 0.081). Post-hoc analyses without controlling for anxiety and externalizing symptoms revealed non-significant differences in mean investments in either condition, Fs ≤ 0.891, ps ≥ 0.347, and other main effects and interactions in repeated measures ANCOVA analyses were also non-significant, Fs ≤ 2.92, ps ≥ 0.090 (group x game; F [1, 124] = 1.87, p = 0.174, η2 = 0.015). Main effects and all interaction effects of age (ps ≥ 0.087) and race (ps ≥ 0.081) were non-significant in both ad-hoc and post-hoc analyses.
Among the participants for whom “believability” data were collected (n = 61 HCs), average ratings (M = 3.90, SD = 1.841) indicated that participants moderately believed they were playing the trust game with another teenager. Median-split analyses with believability data, forming groups of high versus low believers (n’s ≥ 23), were performed to substantiate self-report results. Whether the median split was at “3” or “4” for Likert-scale ratings, there were no significant group main effects or interaction effects with group, whether sociodemographic variables were statistically controlled for or not (p’s ≥ 0.088).
Discussion
To our knowledge, this study is the first to apply the trust game to better characterize social decision-making in adolescent depression. Utilization of a version of the trust game that included comparison with a lottery condition provided the means to examine both social (trust, interpersonal risk-taking) and nonsocial (lottery, general risk-taking) decision-making. Depressive adolescent girls made significantly greater investments in the trust game, but not lottery condition, compared to healthy comparisons. Moreover, this increased trust became statistically significant with later trials, emerging not until midway through the game. Although the group x game interaction was marginally significant, the effect size was in the small-to-moderate range, which is consistent with prior social cognition-depression research (Sullivan & Feinn, 2012; Weightman et al., 2014). The fact that depressive girls exhibited atypical social decision-making, specifically, is consistent with the interpersonal nature of adolescent depression (Joiner, 1999). This study supports the extension of social behavioral economic methods in depression from adults to adolescents. In doing so, these preliminary findings may inform future modeling of depressed adolescents’ social decision-making in an effort to better understand and further classify disrupted social relations in adolescent depression.
The small-to-moderate effect of depression on trust in the present study could be surprising given that past research in pediatric community samples has evidenced negative associations between self-reported trust and depressive symptoms (Bosacki et al., 2007; Gorrese, 2016). There are important theoretical and methodological distinctions between these studies and the present study, in addition to differences in sample type and depression levels. Attachment theory guided prior youth trust studies whereas principles of behavioral game theory (Camerer, 1997) and the reward literature guided present study methods. Additionally, attachment-based trust was captured through self-report measures in these studies, e.g., a subscale of the Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1987). The goal of these works was to examine trust specifically in the context of intimate relationships with parents and peers. Accordingly, the construct of trust in studies of attachment differs from that examined here.
The trust game employed in the current study captures generalized trust behaviorally which pertains to all forms of social interaction (Kosfeld et al., 2005; Rotenberg et al., 2005; van den Bos et al., 2010). Behavioral data on trust may well be more accurate than attitudinal self-report trust data (Glaeser, Laibson, Scheinkman, & Soutter, 2000). However, distinctions between methods in definitions of trust may render this point moot. To this end, each respective trust framework may be informative. Perhaps infusing attachment theory with the trust game may help bridge this gap in the literature. For instance, as executed by Venta and colleagues (2017), this could be tested by having adolescents play the game with their mothers as compared to an unknown woman of a similar age.
Present findings are consistent with Koshevev et al. (2010) who found depressed players to invest more than healthy controls in the trust game. However, findings stand in contrast to those by Unoka and colleagues (2009) who used the same modified trust game with depressed adult men and women. Null findings by Unoka et al. (2009) suggests that the relation between depression and trust might vary with development. Accordingly, trust behavior increases and peaks during mid-adolescence before stabilizing in adulthood (Sutter & Kocher, 2007; van den Bos et al., 2010). Therefore, adolescence may present a vulnerable developmental period when depression influences trust. Indeed, the mean age of fifteen years-old of the girls in our sample corresponds to the time when trust peaks. A developmental perspective (i.e., Cicchetti & Rogasch, 2002) would suggest that psychopathology interacts with typical developmental processes, resulting in trajectories that deviate from an expected course. In this case, an over-shooting (or magnification) of the ontogenic changes in trust observed in adolescence may characterize depressive adolescents. Developmental differences aside, the depressed sample in Unoka et al.’s (2009) study was small (n = 25) and included many men.
Interestingly, depressive girls invested more in the trust game than HCs as trials progressed, despite starting at comparable levels. This could possibly suggest that depressive girls experienced anxiety or worry about maintaining an interpersonal connection with their co-player. If so, it would be reminiscent of excessive reassurance-seeking (ERS) or “the tendency to excessively ask others for reassurance of worth,” a key component of Coyne’s interactional theory of depression (Coyne, 1976; Joiner, 1999). In progressively increasing trusting over time, depressive girls may have been expecting increased reciprocity from the trustee, effectively generating assurance of self-worth. Clearly, this is speculative as moment-to-moment (increasing state of) worry, anxiety, or ERS went unmeasured nor were in-game player cognitions assessed. Future behavioral economic studies of depression may incorporate interpersonal variables (like ERS) that have received much empirical attention and support.
Contrary to expectations, depressive and healthy girls’ investments did not significantly differ in the lottery condition suggesting the two groups were similarly risk averse. Importantly, adult depression findings supporting the rejected lottery condition hypothesis used a different behavioral task, which could have been important. Scheele et al.’s (2013) task provided aversive feedback to risky decisions whereas the present task provided no feedback. However, lack of feedback emulates common real world interpersonal interactions in which decisional outcomes are uncertain and delayed (Kiyonari, Yamagishi, Cook, & Cheshire, 2006). An alternate perspective is that reward sensitivity, the opposite of risk aversion, in depressed adolescent girls may not be reduced as shown in depressed adult females (Mellick, Sharp, & Alfano, 2014). Regardless of non-significant general risk-taking findings, the restriction of anomalous decision-making to the social reward system in the present study emphasizes the importance of integrating social reward paradigms in adolescent depression research (see Forbes & Dahl, 2012).
While it was hypothesized that investments would significantly increase across trials irrespective of group or game, this was only found in the trust game. Random repayment from a computerized lottery may not have sufficiently activated “trustworthy” expectancies (or anticipated reciprocity) resulting in more stable, rather than increased, investment across trials.
This study is not without limitations. Effects of depression on game investments “edged” statistical significance. However, the observed effect size (small-to-medium) may be more informative than p-values for results interpretation (Sullivan & Feinn, 2012; Feise, 2002). Game currency’s social value could not be parsed out, but this does not limit the study of the intended construct (Kishida, King-Casas, & Montague, 2010). Basing participant compensation on in-game earnings may have ensured better emotional and behavioral engagement (Camerer, 2003). Half the sample completed the post-game believability check because the item was a late addition to the study battery. Despite similar ratings to other published trust game studies (i.e., Venta et al., 2017), believability ratings were substantiated with post-hoc analyses. No significant effects were found with believability groups (high, low) suggesting that self-reported believability (or lack thereof) did not influence game play. It remains uncertain whether collected data would generalize to all participants. However, standardized task administration was consistent across assessment settings. Importantly, though, research participants in other behavioral economic studies make similar economic decisions regardless of whether situations are hypothetical or real (Lagorio & Madden, 2005). Moreover, players make investments just the same regardless of whether they believed the game manipulation, in this case deception (Camerer, 2003). Some sociodemographic data were lacking (i.e., socioeconomic status), which could affect economic decision-making (Camerer, 2003). Prior findings (Eckel, 2003) motivated statistically controlling for race beyond group differences. However, it is noteworthy that, in general, effects of race on behavioral economic gameplay have generated mixed findings in the greater literature (Camerer, 2003). Statistically controlling for race therefore may be viewed as a conservative approach, but we felt it important to do so to partially mitigate concern over discrepancy in sample characteristics. To avoid losing statistical power to potential sex differences the present sample was composed solely of girls (Haselhuhn, Kennedy, Kray, Van Zant, & Schweitzer, 2015). Whether findings generalize to boys, i.e., because of sex differences in trust behavior (Buchan, Croson, & Solnick, 2008), is to be determined. Finally, the present study lacked formal diagnostic assessment so whether results translate to major depressive disorder requires testing.
The high levels of co-occurring psychiatric symptoms in the clinical sample were made evident by the fact that removing symptom covariates yielded null primary findings. As shown in Table 1, depressive girls scored in the borderline-clinical range on externalizing symptoms and just below clinical range on anxiety symptoms. Neither main effects nor interactions (i.e., externalizing problems x game type) of these symptom covariates were significant suggesting increased trust may be unique to depression. Future adolescent depression trust game studies may seek to recruit more “purely” depressive adolescents for greater clarity in interpretation of findings. Then again, present findings may in fact be more generalizable since high comorbidity commonly exists with depression in clinical practice. Teasing apart symptoms’ statistical effects hopefully increases the extent to which this study may inform future behavioral economic research.
In closing, in addition to providing a novel means to help delineate and classify psychiatric disorders, behavioral economic games may prove to be valuable therapeutic tools if used by clinicians to assist in improving social interaction style. Specifically, patients may become more sure-footed in their social decision-making through structured gameplay. In the vein of interpersonal psychotherapy (Mufson et al., 2011), depressed adolescents may play these games with intimate people in their lives in hopes that improvements in social decision-making generalize to broader interpersonal functioning.
References
- Achenbach TM & Rescorla LA (2001). Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families. [Google Scholar]
- Allen NB, & Badcock PB (2003). The social risk hypothesis of depressed mood: evolutionary, psychosocial, and neurobiological perspectives. Psychological bulletin, 129(6), 887. [DOI] [PubMed] [Google Scholar]
- Armsden GC, & Greenberg MT (1987). The inventory of parent and peer attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16, 427–454. [DOI] [PubMed] [Google Scholar]
- Baker M, Milich R, & Manolis MB (1996). Peer interactions of dysphoric adolescents. Journal of Abnormal Child Psychology, 24(3), 241–255. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, & Brown GK (1996). Manual for the Beck Depression Inventory,2nd ed. San Antonio, TX: The Psychological Corporation. [Google Scholar]
- Berg J, Dickhaut J, & McCabe K (1995). Trust, Reciprocity, and Social History. Games And Economic Behavior, 10, 122–142. doi: 10.1006/game.1995.1027 [DOI] [Google Scholar]
- Bosacki S, Dane A, Marini Z, & CURA YLC, 2007. Peer relationships and internalizing problems in adolescents: mediating role of self‐esteem. Emot. Behav. Diff 12, 261–282. [Google Scholar]
- Buchan NR, Croson RT, & Solnick S (2008). Trust and gender: An examination of behavior and beliefs in the Investment Game. Journal of Economic Behavior & Organization, 68, 466–476. [Google Scholar]
- Camerer CF (1997). Progress in behavioral game theory. Journal of economic perspectives, 11, 167–188. [Google Scholar]
- Camerer C (2003). Behavioral game theory: Experiments in strategic interaction. Princeton, NJ US: Princeton University Press. [Google Scholar]
- Cicchetti D, & Rogosch FA (2002). A developmental psychopathology perspective on adolescence. Journal of consulting and clinical psychology, 70, 6. [DOI] [PubMed] [Google Scholar]
- Clark CB, Thorne CB, Hardy S, & Cropsey KL (2013). Cooperation and depressive symptoms. Journal of affective disorders, 150, 1184–1187. [DOI] [PubMed] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences. 2nd. [Google Scholar]
- Connolly J, Geller S, Marton P, & Kutcher S (1992). Peer responses to social interaction with depressed adolescents. Journal of Clinical Child Psychology, 21(4), 365–370. [Google Scholar]
- Coyne JC (1976). Toward an interactional description of depression. Psychiatry, 39, 28–40. [DOI] [PubMed] [Google Scholar]
- Crone EA (2013). Considerations of fairness in the adolescent brain. Child Development Perspectives, 7, 97–103. [Google Scholar]
- Davey CG, Yücel M, & Allen NB (2008). The emergence of depression in adolescence: Development of the prefrontal cortex and the representation of reward. Neuroscience & Biobehavioral Reviews, 32, 1–19. [DOI] [PubMed] [Google Scholar]
- Destoop M, Schrijvers D, De Grave C, Sabbe B, & De Bruijn EA (2012). Better to give than to take? Interactive social decision-making in severe major depressive disorder. Journal of Affective Disorders, 137, 98–105. [DOI] [PubMed] [Google Scholar]
- Downey G, & Feldman SI (1996). Implications of rejection sensitivity for intimate relationships. Journal of personality and social psychology, 70(6), 1327. [DOI] [PubMed] [Google Scholar]
- Eckel CC (2003). Conditional trust: sex, race and facial expressions in a trust game.
- Fehr E, & Camerer CF (2007). Social neuroeconomics: the neural circuitry of social preferences. Trends in cognitive sciences, 11(10), 419–427. [DOI] [PubMed] [Google Scholar]
- Feise RJ (2002). Do multiple outcome measures require p-value adjustment?. BMC medical research methodology, 2(1), 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field A (2016). An adventure in statistics: the reality enigma. Sage. [Google Scholar]
- Forbes EE, & Dahl RE (2012). Research review: Altered reward function in adolescent depression: What, when and how?. Journal Of Child Psychology And Psychiatry, 53, 3–15. doi: 10.1111/j.1469-7610.2011.02477.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frith CD, & Singer T (2008). The role of social cognition in decision making. Philosophical Transactions of the Royal Society of London B: Biological Sciences, 363(1511), 3875–3886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galván A (2013). The teenage brain: Sensitivity to rewards. Current Directions In Psychological Science, 22, 88–93. doi: 10.1177/0963721413480859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glaeser EL, Laibson DI, Scheinkman JA, & Soutter CL (2000). Measuring trust. The quarterly journal of economics, 115, 811–846. [Google Scholar]
- Gorrese A (2016, April). Peer attachment and youth internalizing problems: A meta-analysis In Child & Youth Care Forum (Vol. 45, No. 2, pp. 177–204). Springer US. [Google Scholar]
- Haselhuhn MP, Kennedy JA, Kray LJ, Van Zant AB, & Schweitzer ME (2015). Gender differences in trust dynamics: Women trust more than men following a trust violation. Journal of Experimental Social Psychology, 56, 104–109. [Google Scholar]
- Joiner TE Jr (1999). A test of interpersonal theory of depression in youth psychiatric inpatients. Journal of Abnormal Child Psychology, 27, 77–85. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Avenevoli S, & Merikangas KR (2001). Mood disorders in children and adolescents: an epidemiologic perspective. Biological psychiatry, 49, 1002–1014. [DOI] [PubMed] [Google Scholar]
- King-Casas B, & Chiu PH (2012). Understanding interpersonal function in psychiatric illness through multiplayer economic games. Biological psychiatry, 72(2), 119–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kishida KT, King-Casas B, & Montague PR (2010). Neuroeconomic approaches to mental disorders. Neuron, 67, 543–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiyonari T, Yamagishi T, Cook KS, & Cheshire C (2006). Does trust beget trustworthiness? Trust and trustworthiness in two games and two cultures: A research note. Social Psychology Quarterly, 69, 270–283. [Google Scholar]
- Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, & Fehr E (2005). Oxytocin increases trust in humans. Nature, 435, 673–676. [DOI] [PubMed] [Google Scholar]
- Koshelev M, Lohrenz T, Vannucci M, & Montague PR (2010). Biosensor approach to psychopathology classification. PLoS computational biology, 6(10), e1000966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lagorio CH, & Madden GJ (2005). Delay discounting of real and hypothetical rewards III: Steady-state assessments, forced-choice trials, and all real rewards. Behavioural processes, 69, 173–187. [DOI] [PubMed] [Google Scholar]
- Lee V, & Harris L (2013). How social cognition can inform social decision making. Frontiers in neuroscience, 7, 259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mellick W, Sharp C, & Alfano C (2014). The role of BIS/BAS in the vulnerability for depression in adolescent girls. Personality and Individual Differences, 69, 17–21. [Google Scholar]
- Mellick W, Sharp C, & Ernst M (2015). Neuroeconomics for the Study of Social Cognition in Adolescent Depression. Clinical Psychology: Science and Practice, 22, 255–276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miles J, & Shevlin M (2001). Applying regression and correlation: A guide for students and researchers. Sage. [Google Scholar]
- Montague PR, Lohrenz T, & Dayan P (2015). The three R’s of trust. Current Opinion in Behavioral Sciences, 3, 102–106. [Google Scholar]
- Moskowitz GB (2005). Social cognition: Understanding self and others. Guilford Press. [Google Scholar]
- Mufson L, Dorta KP, Moreau D, & Weissman MM (2011). Interpersonal psychotherapy for depressed adolescents. Guilford Press. [Google Scholar]
- Nelson EE, Leibenluft E, McClure EB, & Pine DS (2005). The social re-orientation of adolescence: a neuroscience perspective on the process and its relation to psychopathology. Psychological Medicine, 35, 163–174. [DOI] [PubMed] [Google Scholar]
- Pocock SJ, Assmann SE, Enos LE, & Kasten LE (2002). Subgroup analysis, covariate adjustment and baseline comparisons in clinical trial reporting: current practiceand problems. Statistics in medicine, 21(19), 2917–2930. [DOI] [PubMed] [Google Scholar]
- Rotenberg KJ, Fox C, Green S, Ruderman L, Slater K, Stevens K, & Carlo G (2005). Construction and validation of a children’s interpersonal trust belief scale. British Journal of Developmental Psychology, 23, 271–292. [Google Scholar]
- Rudolph KD, & Flynn M (2009). Adolescent depression. Handbook of depression, 2, 444–466. [Google Scholar]
- Scheele D, Mihov Y, Schwederski O, Maier W, & Hurlemann R (2013). A negative emotional and economic judgment bias in major depression. European archives of psychiatry and clinical neuroscience, 263, 675–683. [DOI] [PubMed] [Google Scholar]
- Sharp C (2012). The use of neuroeconomic games to examine social decision making in child and adolescent externalizing disorders. Current Directions in Psychological Science, 21(3), 183–188. [Google Scholar]
- Sharp C, Ha C, & Fonagy P (2011). Get them before they get you: Trust, trustworthiness, and social cognition in boys with and without externalizing behavior problems. Development and Psychopathology, 23, 647–658. [DOI] [PubMed] [Google Scholar]
- Sharp C, Monterosso J, & Montague PR (2012). Neuroeconomics: a bridge for translational research. Biological psychiatry, 72(2), 87–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharp C, Venta A, Vanwoerden S, Schramm A, Ha C, Newlin E, … & Fonagy P (2016). First empirical evaluation of the link between attachment, social cognition and borderline features in adolescents. Comprehensive Psychiatry, 64, 4–11. [DOI] [PubMed] [Google Scholar]
- Smoski MJ, Felder J, Bizzell J, Green SR, Ernst M, Lynch TR, & Dichter GS (2009). fMRI of alterations in reward selection, anticipation, and feedback in major depressive disorder. Journal Of Affective Disorders, 118, 69–78. doi: 10.1016/j.jad.2009.01.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L (2005). Cognitive and affective development in adolescence. Trends In Cognitive Sciences, 9, 69–74. [DOI] [PubMed] [Google Scholar]
- Sullivan GM, & Feinn R (2012). Using effect size—or why the P value is not enough. Journal of graduate medical education, 4(3), 279–282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutter M, Kocher MG (2007). Trust and trustworthiness across different age groups. Games and Economic Behavior, 59, 364–382. [Google Scholar]
- Unoka Z, Seres I, Áspán N, Bódi N, & Kéri S (2009). Trust game reveals restricted interpersonal transactions in patients with borderline personality disorder. Journal of Personality Disorders, 23, 399–409. [DOI] [PubMed] [Google Scholar]
- van den Bos W, Westenberg M, van Dijk E, Crone EA (2010). Development of trust and reciprocity in adolescence. Cognitive Development, 25, 90–102. [Google Scholar]
- Venta A, Ha C, Vanwoerden S, Newlin E, Strathearn L, & Sharp C (2017). Paradoxical Effects of Intranasal Oxytocin on Trust in Inpatient and Community Adolescents. Journal of Clinical Child & Adolescent Psychology, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weightman MJ, Air TM, & Baune BT (2014). A review of the role of social cognition in major depressive disorder. Frontiers in Psychiatry, 5, 179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wendler D, & Miller FG (2004). Deception in the pursuit of science. Archives of Internal Medicine, 164, 597–600. [DOI] [PubMed] [Google Scholar]
- Wilkinson GS, & Robertson GJ (2006). Wide Range Achievement Test 4 professional manual. Lutz, FL: Psychological Assessment Resources. [Google Scholar]