

Abstract
Introduction Coronavirus disease 2019 (COVID-19) is an acute infection caused by the new coronavirus (SARS-CoV-2) and it is highly transmissible, especially through respiratory droplets. To prepare the health system for the care of these patients also led to a restriction in the activity of several medical specialties. Physicians who work with patients affected by diseases of the head and neck region constitute one of the populations most vulnerable to COVID-19 and also most affected by the interruption of their professional activities.
Objective The aim of the present study was to assess the impact of the COVID-19 pandemic on the practice of head and neck surgeons and otorhinolaryngologists in Brazil.
Methods An anonymous online survey of voluntary participation was applied, containing 30 questions regarding demographic aspects, availability of personal protective equipment (PPE), and impact on the routine of head and neck surgeons and otorhinolaryngologists, as well as clinical oncologists and radiation oncologists who work with head and neck diseases.
Results Seven hundred and twenty-nine answers were received in a period of 4 days, ∼ 40 days after the 1 st confirmed case in Brazil. With professionals working in public and private services, there was a high level of concerns with the disease and its consequences, limited availability of PPE and a significant decrease in the volume of specialized medical care.
Conclusion The study demonstrated a direct impact of the COVID-19 pandemic on the clinical practice of specialties related to the treatment of patients with diseases of the head and neck region already in the beginning of the illness management in Brazil.
Keywords: COVID-19, pandemics, occupational groups, health personnel, work
Introduction
Infection by the new coronavirus (SARS-CoV-2) started in late 2019 in Wuhan, in the province of Hubei, in China. The virus spread very fast across Asia and quickly became a pandemic. It is a highly contagious disease, with many oligosymptomatic or even asymptomatic patients, with high mortality rates for vulnerable patients (those with chronic disease, immunocompromised and/or elderly). 1
Another striking feature of the disease is the prolonged hospitalization of severe cases, which makes physicians and other health professionals very exposed to the virus. The main route of contamination by the disease is by droplets and aerosol dispersion, which makes professionals who deal with diseases of the upper airways tract particularly more susceptible to contamination. 2 3 In this context, the correct use and availability of personal protective equipment (PPE) is essential to protect the healthcare providers (HCPs). 4 5 6 7
To prepare the healthcare system to receive these patients has led to a major change in the routine of most healthcare services. Many institutions have restricted their activities only to the management of patients affected by the coronavirus 2019 (COVID-19), practically interrupting other treatments, especially the elective ones. This fact directly affected the care of patients with other health problems and also the professional activity of several medical specialties.
Thus, the aim of the present study was to assess the impact of the COVID-19 pandemic on the practice of physicians working in the areas of otolaryngology and head and neck oncology in Brazil.
Methods
A web-based survey was created using the SurveyMonkey audience platform. Information on how data are collected, stored and exported may be obtained in: www.surveymonkey.com/mp/audience . Demographic, professional, and clinical practice data were collected through 30 questions of different formats: multiple choice, dropdown lists, and text boxes, with the possibility to add commentaries as open text in some questions. Specifically, we collected data regarding the impact of de COVID-19 pandemic on: 1) the amount and type of outpatient appointments, surgeries and exams with the risk of generating aerosols; 2) availability of adequate PPE in different settings and practices; 3) the preparedness of the responder's health institution in orienting their HCPs and developing strategies to manage COVID-19 suspected and confirmed patients.
Pilot testing of the survey was performed with members of the research team, and questions were modified to improve readability and adequacy. The target population consisted of specialists who worked in the field of the head and neck, particularly otorhinolaryngologists, head and neck surgeons, oncologists, and radiation oncologists. The survey platform generated a link to access the survey that was distributed electronically, through email and social media, to members and participants of the involved medical organizations (Grupo Brasileiro de Cabeça e Pescoço, Fundação Otorrinolaringologia, Sociedade Brasileira de Oncologia Clínica, Sociedade Brasileira de Cirurgia de Cabeça e Pescoço, Sociedade Brasileira de Radioterapia, Disciplinas de Otorrinolaringologia, Cirurgia de Cabeça e Pescoço, Oncologia e Radioterpia da Faculdade de Medicina da Universidade de São Paulo)
Participation in the survey was voluntary, and all data that could identify the responder was kept anonymous in all phases of the study. The survey collected responses from April 13 th to 17 th 2020, when the pandemic was ongoing for 7 weeks in Brazil, after the first diagnosed case. A short period of data collection was planned beforehand to capture a specific moment of the COVID-19 pandemic, as many responses could change during the progression of the disease. Each physician could participate only once in the survey.
The data was imported to an Excel spreadsheet and then submitted to procedures to ensure data consistency and, finally, it was imported to SPSS version 26.0 (IBM Corp., Armonk, NY, USA) for statistical analyses. Categorical data was compared with chi-square tests. Non-parametric Spearman was used to test the correlation between ordinal variables. The study was considered as exploratory, and neither sample size calculation nor correction for multiple comparisons were performed.
Results
The survey was answered by 729 physicians; 228 head and neck surgeons, 293 otorhinolaryngologists, 111 clinical oncologists, and 97 radiation oncologists. The demographic and professional characteristics of the physicians are shown in Table 1 . There were differences in some of these characteristics in relation to the specialties. Head and neck surgeons and otorhinolaryngologists had more practice time than clinical specialists, and the proportion of head and neck surgeons in both sectors of care (private and public) was greater than that of physicians in other specialties.
Table 1. Demographic characteristics of participant physicians.
| Area of expertise | Head and neck surgery | Otorhinolaryngology | Clinical oncology | Radiation oncology | Total | P -value * | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 228 | 31.3% | 293 | 40.2% | 111 | 15.2% | 97 | 13.3% | 729 | 100.0% | ||
| Years after residency | |||||||||||
| Resident | 7 | 3.1% | 3 | 1.0% | 6 | 5.4% | 10 | 10.3% | 26 | 3.6% | < 0.001 |
| < 5 years | 36 | 15.8% | 39 | 13.3% | 27 | 24.3% | 25 | 25.8% | 127 | 17.4% | |
| 5–10 years | 45 | 19.7% | 57 | 19.5% | 27 | 24.3% | 21 | 21.6% | 150 | 20.6% | |
| 10–20 years | 73 | 32.0% | 84 | 28.7% | 36 | 32.4% | 28 | 28.9% | 221 | 30.3% | |
| 20–30 years | 41 | 18.0% | 71 | 24.2% | 13 | 11.7% | 7 | 7.2% | 132 | 18.1% | |
| > 30 years | 26 | 11.4% | 39 | 13.3% | 2 | 1.8% | 6 | 6.2% | 73 | 10.0% | |
| Geographic area of practicing | |||||||||||
| North | 8 | 3.5% | 4 | 1.4% | 3 | 2.7% | 5 | 5.2% | 20 | 2.7% | 0.486 |
| Northeast | 44 | 19.3% | 47 | 16.0% | 20 | 18.0% | 18 | 18.6% | 129 | 17.7% | |
| Central West | 21 | 9.2% | 22 | 7.5% | 4 | 3.6% | 7 | 7.2% | 54 | 7.4% | |
| Southeast | 135 | 59.2% | 185 | 63.1% | 69 | 62.2% | 59 | 60.8% | 448 | 61.5% | |
| South | 20 | 8.8% | 35 | 11.9% | 15 | 13.5% | 8 | 8.2% | 78 | 10.7% | |
| Area | |||||||||||
| Metropolitan | 173 | 75.9% | 200 | 68.3% | 78 | 70.3% | 74 | 76.3% | 525 | 72.0% | 0.188 |
| Countryside | 55 | 24.1% | 93 | 31.7% | 33 | 29.7% | 23 | 23.7% | 204 | 28.0% | |
| Type of service | |||||||||||
| Private | 34 | 14.9% | 138 | 47.1% | 46 | 41.4% | 28 | 28.9% | 246 | 33.7% | < 0.001 |
| Public | 13 | 5.7% | 8 | 2.7% | 9 | 8.1% | 17 | 17.5% | 47 | 6.4% | |
| Both | 181 | 79.4% | 147 | 50.2% | 56 | 50.5% | 52 | 53.6% | 436 | 59.8% | |
P -value (chi-square test).
We asked how physicians self-perceived their risk of developing severe forms of COVID-19, according to their age and the presence of comorbidities. There were no differences between specialties: 57.3% considered themselves without risk of developing severe forms, 27% at low risk, and only 15.6% considered themselves at high risk ( p = 0.43).
There was a remarkable reduction in the volume of medical care, both in the private and public scenarios. The reduction was more evident in the private sector than in the public services ( p < 0.001), with ∼ 50% of the physicians who assist in the private sector referring to a reduction of 75% or more in the volume of care ( Table 2 ). The reduction in the volume of medical care was not uniform among the responders. The impact was greater in surgical specialties (head and neck surgery and otolaryngology), than in oncology clinics (clinical oncology and radiation oncology), both in the private sector ( p < 0.001) and in the public services ( p < 0.001) ( Table 3 ).
Table 2. Medical practice situation after COVID-19 pandemic.
| Reduction in outpatient care | Private | Public | P -value * | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| 100% (full-stop) | 118 | 17.1% | 83 | 16.9% | < 0.001 |
| 75–99% | 226 | 32.7% | 86 | 17.5% | |
| 50–74% | 169 | 24.4% | 95 | 19.3% | |
| 25–49% | 76 | 11.0% | 70 | 14.3% | |
| 1–24% | 50 | 7.2% | 69 | 14.1% | |
| No change | 53 | 7.7% | 88 | 17.9% | |
| Total | 692 | 100% | 491 | 100% | |
P -value (chi-square test).
Table 3. Medical practice situation of all specialties after the COVID-19 pandemic.
| Reduction in outpatient care | Head and neck surgery | Otorhinolaryngology | Clinical oncology | Radiation oncology | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Private | Public | Private | Public | Private | Public | Private | Public | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| 100% (full-stop) | 38 | 17.2% | 22 | 11.2% | 75 | 26.0% | 56 | 36.4% | 4 | 4.0% | 4 | 5.6% | 1 | 1.2% | 1 | 1.4% |
| 75–99% | 96 | 43.4% | 43 | 21.9% | 115 | 39.8% | 36 | 23.4% | 5 | 5.0% | 5 | 6.9% | 10 | 12.2% | 2 | 2.9% |
| 50–74% | 51 | 23.1% | 51 | 26.0% | 75 | 26.0% | 25 | 16.2% | 25 | 25.0% | 9 | 12.5% | 18 | 22.0% | 10 | 14.5% |
| 25–49% | 24 | 10.9% | 38 | 19.4% | 17 | 5.9% | 4 | 2.6% | 22 | 22.0% | 16 | 22.2% | 13 | 15.9% | 12 | 17.4% |
| 1–24% | 9 | 4.1% | 23 | 11.7% | 3 | 1.0% | 9 | 5.8% | 26 | 26.0% | 24 | 33.3% | 12 | 14.6% | 13 | 18.8% |
| No change | 3 | 1.4% | 19 | 9.7% | 4 | 1.4% | 24 | 15.6% | 18 | 18.0% | 14 | 19.4% | 28 | 34.1% | 31 | 44.9% |
| Total | 221 | 100% | 196 | 100% | 289 | 100% | 154 | 100% | 100 | 100% | 72 | 100% | 82 | 100% | 69 | 100% |
Another impacting factor in determining the volume of care reduction was the self-perceived risk of developing serious forms of COVID-19. In the private sector, the reduction of 75% or more in the volume of assistance was 66.4%, 51.1%, and 44.5% for the high, low, and risk-free groups, respectively ( p < 0.001). In the public services, these proportions were 52.1%, 36.2%, and 28.9%, respectively ( p = 0.001)
Faced with the reduction in the volume of medical appointments, physicians have been looking for another way to serve their patients. However, the face-to-face appointment still corresponds to more than 70% of the attendance for 49.6% of the physicians. Telemedicine is not yet a reality in our country: 77.2% of the physicians use it in less than 10% of their visits. For ⅔ of physicians (66.9%), contact with patients by phone or social media corresponded to less than 30% of the appointments.
Physicians reported a decrease in the performance of potentially aerosol-generating exams. A decrease of 50% or more in oroscopy, nasofibroscopy, and laryngoscopy was reported by 53.1%, 81.9%, and 81.3% of the respondents, respectively. If we consider who reported almost complete interruption of the exams (reduction of 90–100%), these values were 23.1%, 64.3% and 62.4%, respectively.
The impact of COVID-19 was particularly significant on the reduction of operating volume of surgeons who responded to the survey. An almost complete (90–100%) decrease in thyroidectomies, elective surgeries in the pediatric range, and nasosinusal surgeries was reported, respectively, by 60.7%, 91.1%, and 90.3% of the surgeons who normally perform them. Even in those surgeries that were supposed to continue during the pandemic, a drastic reduction in comparison to prepandemic period was mentioned. Tracheostomies and surgeries for resection of head and neck cancer had a reduction of 50% or more reported by 65.4% and 49.3% of physicians, respectively. If we consider who reported near interruption of the surgeries (reduction of 90–100%), these values were 44.8% and 24.8%, respectively.
Most surgeons reported difficulties in scheduling elective surgeries both in the private sector (78.7%) and in the public services (75.5%), chiefly due to guidance from the hospital itself in not allowing such appointments.
The performance of surgical interventions in confirmed COVID-19 patients was small in the studied group (22 cases, 4.6%). These cases were operated mainly because they were urgencies, oncological cases, or tracheostomies. Of the 22 operated patients, 19 had no complications or had complications as expected for the procedure, and 3 patients had serious complications or died.
Most of the interviewed physicians (74.8%) reported knowing a professional colleague with confirmed COVID-19 infection. The median of professionals (physicians or other HCPs) infected was 2 (P25%: 2; P75%: 6; minimum: 0; maximum: 94). Thirty-two (4.4%) of the physicians interviewed reported having become infected with the disease. Of these, 11 were head and neck surgeons, 9 were radiation oncologists, 7 were oncologists, and 5 were otorhinolaryngologists.
The limitation in the availability of complete PPE for exams that potentially generate aerosol is shown in Fig. 1 . To facilitate understanding, only the extremes of availability (0–10% and 90–100%) were represented. Complete PPE available in only 0 to 10% of examinations was reported by ∼ 20% of physicians working in the private sector, and by 25% of those working in the public services. At the other end of the analysis, complete equipment available in 90 to 100% of examinations was reported by ∼ 55% and 45% of physicians in the private and public sectors, respectively. The lack of PPE was greater in the public sector in relation to oroscopies ( p = 0.01) and laryngoscopies ( p = 0.024). For nasofibroscopies, no difference was observed ( p = 0.068). We assessed whether the lack of PPE for the exams could have influenced the decrease in the volume of each exam (oroscopy, nasofibroscopy, and laryngoscopy). In both the private and public sectors, we did not find significant correlations for any of the tests mentioned (data not shown—Spearman test).
Fig. 1.
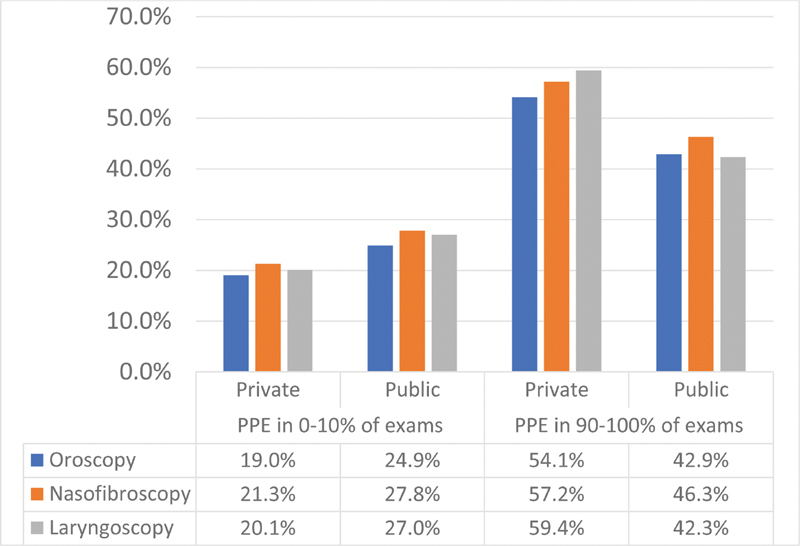
Availability of complete personal protective equipment for exams that generate droplets and aerosol.
Fig. 2 shows the availability of masks for patient care in the private and public sectors. Although surgical masks are available in both services ( p = 0.157), the type N95 mask had more restricted and lower availability in public services, when compared with private ones ( p < 0.001). Again, only the availability extremes (0–10% and 90–100%) were represented. The opinion of 48.0% of respondents in the private and 69.1% in the public sector was that PPE would end during the pandemic ( p < 0.001), in a time interval ranging from 1 to more than 10 weeks, with a median of 4 weeks, both in the public and private sectors.
Fig. 2.
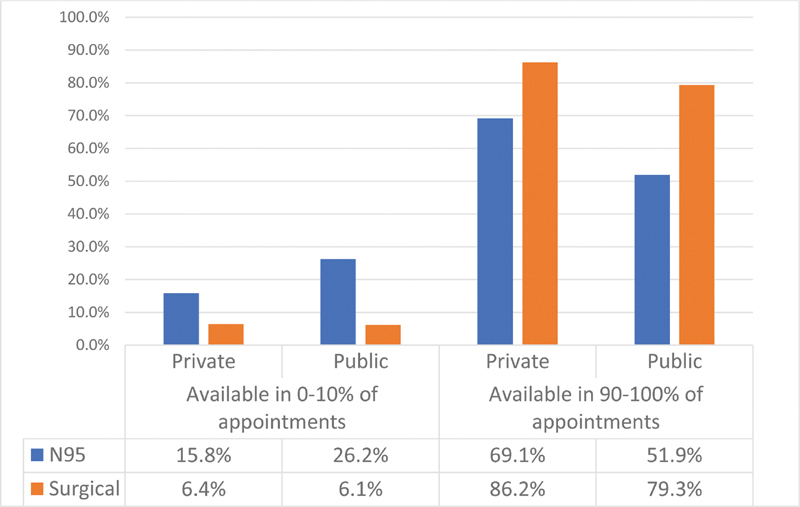
Availability of masks for medical care in the private and public sectors.
When asked whether, in the absence of suitable PPE, the colleague would postpone or refuse care for a suspected or confirmed COVID-19 patient, 20.3% replied that they would still attend. The main consideration for care in these circumstances was urgencies or medical emergencies. We observed that this attitude was greater in clinical specialties (oncologists and radiation therapists) than in surgical specialties ( p = 0.004) and was not related to time of clinical practice or risk of developing serious disease due to COVID-19 ( Table 4 ).
Table 4. Opinion on the performance of care of suspected or confirmed COVID-19 patients in the absence of suitable personal protective equipment.
| No | Yes | P -value * | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Area of expertise | |||||
| Head and neck surgery | 187 | 82.0% | 41 | 18.0% | 0.004 |
| Otorhinolaryngology | 246 | 84.0% | 47 | 16.0% | |
| Clinical oncology | 80 | 72.1% | 31 | 27.9% | |
| Radiation oncology | 68 | 70.1% | 29 | 29.9% | |
| Risk of severe forms of COVID-19 | |||||
| No | 324 | 77.5% | 94 | 22.5% | 0.127 |
| Yes, low risk | 159 | 80.7% | 38 | 19.3% | |
| Yes, high risk | 98 | 86.0% | 16 | 14.0% | |
| Years after residency | |||||
| Resident | 22 | 84.6% | 4 | 15.4% | 0.858 |
| < 5 years | 99 | 78.0% | 28 | 22.0% | |
| 5–10 years | 116 | 77.3% | 34 | 22.7% | |
| 10–20 years | 181 | 81.9% | 40 | 18.1% | |
| 20–30 years | 104 | 78.8% | 28 | 21.2% | |
| > 30 years | 59 | 80.8% | 14 | 19.2% | |
P -value (chi-square test).
Although the pandemic is already in its 7 th week in Brazil, since the identification of the 1 st case, 45.3% and 48.8% of physicians in the private and public sectors, respectively, reported that they had not received face-to-face or distance training in the management of confirmed or suspected patients with COVID- 19. On the other hand, health services in both the private and public sectors seem to have been prepared to manage the COVID-19 crisis. According to the physicians interviewed, 71.1% and 76.8% of the private and public services, respectively, created a crisis management committee and institutional protocols for the management of these patients. The commitment to the management of suspected or confirmed patients with COVID-19 was considered to be good or excellent by 79.5% and 65.2% of physicians in private and public services, respectively ( p < 0.001). Presence of pretreatment screening areas were equivalent in the private (53.5%) and public (55.2%) sectors. The presence of an isolated hospitalization area for patients with suspected or confirmed COVID-19 was reported by 83.7% of physicians in the public sector and by only 67.3% of those in the private services ( p < 0.001).
Discussion
Physicians who work in the field of the head and neck are among the HCPs most infected with SARS-CoV-2 in different regions of the world. 5 8 9 10 11 Patients with COVID-19 usually present with symptoms seen by these specialists, such as cough, sore throat, headache, increased sputum production and anosmia. Half of these patients do not present fever at the onset, lowering the index of suspicion of the disease. 8 12 Furthermore, physical examination in these specialties require exposure to the nasal and oral cavities and oropharynx. These regions present high concentrations of SARS-CoV-2, even in the asymptomatic patients, who may also spread the disease. 8 9 13
This survey aimed to quantify the impact of the COVID-19 pandemic in the daily practice of otorhinolaryngologists, head and neck surgeons, clinical oncologists, and radiation oncologists. It revealed a drastic reduction in outpatient visits, and in the number of exams and surgical procedures.
Some degree of reduction in the volume of outpatients was expected, as many institutions and medical societies have suggested postponing non-urgent appointments, in response to the elevated occupational hazard of these specialists. 5 8 9 12 14 15 Furthermore, on March 20th 2020, due to the progression of the pandemic, the Brazilian Federal Council of Medicine recommended cancelling appointments and elective procedures for all physicians in Brazil. 16 Finally, patients may be reluctant to seek medical care, due to the fear that the physician or the health care unit may be a source of COVID-19 contagion. 14 This fear seems to play a major role on the side of the physician as well. The amount of reduction in outpatient visits was associated with the physician's self-perceived risk of developing severe forms of COVID-19, both in the private and the public sectors.
The decrease in the volume of outpatient appointments was higher among surgical specialties and in the private sector. In this group, the majority of responders referred a decrease of more than 75% of visits. This reduction, without previous planning, will impact not only the financial income of physicians, but will probably impair the expedited diagnosis and treatment of progressive diseases, such as cancer, thus influencing their morbidity and mortality rates.
One alternative to keep the flow of outpatients would be an increased use of telemedicine, which has been recently regulated by the Ministry of Health (Ordinance N. 467 of 20/3/2020), to mitigate the problem of providing adequate healthcare during the COVID-19 pandemic. 12 17 However, probably due to the recent regulation and lack of familiarity by both physicians and patients, it is still not commonly used among us. Our study demonstrated that when telemedicine was adopted as an alternative to face to face appointments, it was usually employed in less than 10% of cases.
To organize the flow of outpatients, it would be productive to categorize them in tiers: those who would need to be seen face to face (urgent cases, in which physical exam is essential), those appropriate for telemedicine or telephone visit, and those who could be simply rescheduled. 18
Our study also revealed a marked reduction of exams considered aerosol generating procedures (AGPs), especially nasofibroscopies and laryngoscopies. In these exams droplets and aerosols may be generated, especially in the event the patient sneezes or coughs during the procedure, 13 leading to an increased risk of transmission. Surgical masks are not protective against aerosols, and aerosolized particles of SARS-CoV-2 have been shown to remain viable in the air for at least 3 hours. 19 Therefore, most experts recommend that AGPs should be performed with adequate PPE, including: long sleeve gown, gloves, face shield and N95 mask. 5 9 12 18 20 Nonetheless, the role of aerosols in the transmission of COVID-19, both in the community and to HCPs, is not known. In SARS patients, a meta-analysis showed a consistent association between tracheal intubation and transmission of SARS-CoV to HCPs. Lower-quality studies have demonstrated increased risk of SARS infection with tracheostomy, non-invasive ventilation and mask ventilation before intubation. Twenty other AGPs were assessed, and none demonstrated an increased risk of SARS transmission. 21 So far, SARS-CoV-2 is considered, at most, an opportunistic airborne pathogen, 13 and, according to the World Health Organization (WHO), COVID-19 is primarily transmitted through respiratory droplets and contact routes. 22
The availability of complete PPE for AGPs, as suggested, was investigated in our study. Of concern was the finding that 20 to 25% of responders referred that complete PPE were available in less than 10% of the procedures. The shortage of PPE was more pronounced in the public sector. There was no association between the availability of PPE and the amount of reduction of AGPs, suggesting that the shortage of PPE was not the main reason to explain the reduction of exams. Probably, the decrease in the volume of outpatients impacted the amount on exams performed.
The availability of surgical masks for outpatient appointments was adequate in both public and private sectors. The same was not observed for N95 masks. They were available in less than 10% of appointments in 26% of public facilities and 16% of private ones, with the difference being statistically significant. There are conflicting recommendations regarding mask use under low risk situations, as in routine clinical care. The WHO recommends surgical masks, while the Centers for Disease Control and Prevention (CDC) recommends N95 masks. 13 Given the possibility of transmission of COVID-19 from asymptomatic patients, at least surgical masks should be used by HCPs in all outpatient visits. 12
There is, actually, little evidence to support the superiority of N95 masks over standard surgical masks in the scenario of routine clinical care. A recent meta-analysis failed to demonstrate the superiority of N95 masks over surgical masks in preventing influenzae infection in HCPs. The lack of compliance with proper fit and adequate use, due to the discomfort associated to its use may have influenced the results. 23 Furthermore, not only compliance to the adequate use of mask during exposure but appropriate doffing of PPE is vital to prevent contagion, even in AGPs. 9 20 Moreover, in a case report regarding 41 HCPs who took care of a patient with COVID-19 and pneumonia and were exposed during various AGPs (tracheal intubation, extubation, and non-invasive ventilation), none of them got infected, despite 85% having used only surgical masks during the procedures. Proper hand hygiene and standard procedures were adopted by all HCPs. The authors emphasize the limitations of a case report study, but suggest that the superiority of N95 masks for AGPs should be questioned and that further studies are necessary to determine how best to protect HCPs from COVID-19. 24
Our study also confirmed a marked disruption in surgical practice, including elective sinonasal procedures, surgeries in children, and thyroidectomies. Surgery will probably be a component of our practice that will take longer to resume. Medical organizations and societies still recommend limiting all non-essential surgeries, to preserve needed resources and the safety of patients and HCPs. 11 Due to the high viral titers in the nasal mucosa, even in asymptomatic patients, 13 sinonasal procedures have a high risk of aerosolization and contagion 5 and should be avoided. Also in children, surgery should be postponed, if considered non-urgent. 18 When infected, children tend to be asymptomatic or to present milder symptoms and may be still contagious. 20 On the other hand, surgeries without mucosal exposure, such as thyroidectomies, are considered of lower risk of COVID-19 transmission, as compared with surgeries on the nasal cavities or pharynx. The caveat is the use of energy devices that may theoretically result in aerosolization of the virus from the bloodstream. 9 Even so, thyroidectomies have also been reduced, according to our study. As a matter of fact, most surgeons referred to difficulties in scheduling elective procedures, mainly due to restrictions imposed by the surgical center, both in the private and the public sectors.
Even procedures that should continue during the pandemic, such as cancer resections and tracheostomies, were reduced, albeit, to a lesser degree. This finding suggests that currently, the waiting list of patients requiring surgery is gradually increasing, as cancer and diseases that lead to airway obstruction, such as recurrent respiratory papillomatosis will continue to progress. As the pandemic evolves, there will be an increasing need to resume surgeries in patients without a definite COVID-19 diagnosis. The urgency of the procedure will need to be weighed against the risk of getting a nosocomial COVID-19 infection on a case-by-case basis. That is a real concern for cancer patients, as they have been associated with poorer outcomes if they become infected with SARS-Cov-2. 25 Therefore, for initial (T1/T2) laryngeal carcinoma, radiation therapy may be an appropriate alternative to the high-risk microlaryngeal surgery with CO2 laser during the pandemic. 26 On the other hand, trying to keep a COVID-free environment is a real concern for some hospitals. Screening for SARS-CoV-2 in the 48 h prior to the procedure, although with questionable sensitivity in asymptomatic patients, may help to identify unsuspected positive patients, whose procedure could be postponed. 9
An unexpected finding in our study was the low amount of surgeries (22 cases) performed in COVID-19 patients, given the presence of more than 500 surgeons among responders, most of them with more than 10 years of experience in the field. At least, a larger amount of tracheostomies was expected, as it was the most performed surgery in SARS patients. 27 Elective tracheostomies in COVID-19 patients have a narrower range of indication, due to the increased risk of aerosolization and contagion. 9 Even so, these numbers should increase as the pandemic evolves.
According to the opinion of responders in our study, most institutions, in both the private and public sectors, are concerned with their preparedness to combat the COVID-19 pandemic. It is interesting to notice that public services were better than private ones, in regard to the presence of isolated COVID-19 inpatient areas. However, communication and orientation of HCPs seem to be limited, at best. Close to 50% of responders, in both sectors, said they did not receive any kind of training about the management of COVID-19 patients. This is a deeply worrying finding, given the high occupational risk of contagion in our field and that the pandemic is close to completing 2 months in Brazil.
Studies based on surveys are particularly prone to sampling bias, especially if they rely on open, digital recruitment, as performed in this study. However, our aim was to capture the momentary effect of an evolving pandemic on the medical practice. Other recruitment strategies would not be as efficient in providing the same yield in such a short time. The study sample revealed a predominance of physicians from the Southeast region of Brazil and from metropolitan areas. Also, surgical specialists (head and neck surgeons and ENTs) were older than oncologists and radiation therapists. These characteristics are in accordance with the medical demographics in our country. 28 Another limitation of the study refers to the representativity of the medical specialties in the sample. Considering the number of registered specialists in Brazil, 28 our study sampled 21.2% of head and neck surgeons; 13.2% of radiation oncologists; 4.6% of ENTs; and 3.1% of clinical oncologists. Although sampling bias is not prevented by higher sampling yields, ear, nose & throat (ENT) specialists and oncologists were indeed poorly represented in our sample. However, when different responses according to specialties were observed in our analyses, they tended to group among surgeons and clinicians. Therefore, we speculate that the low representativeness of ENTs and clinical oncologists might have been compensated by the higher proportion of head and neck surgeons and radiation oncologists, respectively.
Surveys such as the present one may help to quantify the impact of COVID-19 on the daily practice of physicians, their current concerns and limitations, and to suggest alternative ways to mitigate these limitations. Specifically, medical societies could broaden programs aiming to train their members about how to: 1) deal with COVID-19 suspected or infected patients in different situations, 2) proper use of telemedicine, 3) manage their waiting list for surgeries and 4) providing distance learning courses on patient management and protection during exams and surgeries.
Many aspects investigated in the present survey will probably evolve during the course of the pandemic, and follow-up studies are planned to capture these changes.
Conclusions
The present survey revealed that COVID-19 impacted Brazilian specialists that work in the head and neck field, with marked reduction in outpatient visits, exams and surgical procedures. We could also identify limitations in regard to: 1) adequate training of specialists in dealing with COVID-19 patients, 2) the availability of adequate PPE for AGPs, 3) the use of telemedicine as an alternative to face-to-face appointments.
Footnotes
Conflict of Interests The authors declare no potential conflict of interests.
References
- 1.Meng L, Hua F, Bian Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J Dent Res. 2020;99(05):481–487. doi: 10.1177/0022034520914246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chan J YK, Wong E WY, Lam W.Practical aspects of otolaryngologic clinical services during the 2019 Novel Coronavirus Epidemic: An Experience in Hong KongJAMA Otolaryngol Head Neck Surg2020 [DOI] [PubMed]
- 3.Koh D. Occupational risks for COVID-19 infection. Occup Med (Lond) 2020;70(01):3–5. doi: 10.1093/occmed/kqaa036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect. 2020;104(04):454–455. doi: 10.1016/j.jhin.2020.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patel Z M, Fernandez-Miranda J, Hwang P H et al. Letter: Precautions for Endoscopic Transnasal Skull Base Surgery During the COVID-19 Pandemic. Neurosurgery. 2020:nyaa125. doi: 10.1093/neuros/nyaa125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rimmer A. Covid-19: what's the current advice for UK doctors? BMJ. 2020;368:m978. doi: 10.1136/bmj.m978. [DOI] [PubMed] [Google Scholar]
- 7.Schwartz J, King C C, Yen M Y. Protecting health care workers during the COVID-19 Coronavirus Outbreak -Lessons from Taiwan's SARS response. Clin Infect Dis. 2020:ciaa255. doi: 10.1093/cid/ciaa255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cheng X, Liu J, Li N et al. Otolaryngology providers must be alert for patients with mild and asymptomatic COVID-19. Otolaryngol Head Neck Surg. 2020:1.94599820920649E14. doi: 10.1177/0194599820920649. [DOI] [PubMed] [Google Scholar]
- 9.Givi B, Schiff B A, Chinn S Bet al. Safety recommendations for evaluation and surgery of the head and neck during the COVID-19 PandemicJAMA Otolaryngol Head Neck Surg2020 [DOI] [PubMed]
- 10.Jotz G P, Voegels R L, Bento R F. Otorhinolaryngologists and Coronavirus Disease 2019 (COVID-19) Int Arch Otorhinolaryngol. 2020;24(02):e125–e128. doi: 10.1055/s-0040-1709724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.AAOHSN. Academy Supports CMS, Offers Specific Nasal Policy 26/3/2020 [Available from:https://www.entnet.org/content/academy-supports-cms-offers-specific-nasal-policy
- 12.Lavinsky J KE, Baptistella E, Roithman R et al. An update on COVID-19 for the otorhinolaryngologist - a Brazilian Association of Otolaryngology and Cervicofacial Surgery (ABORL-CCF) Position Statement. Rev Bras Otorrinolaringol (Engl Ed) 2020;885:1–8. doi: 10.1016/j.bjorl.2020.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Workman A D, Welling D B, Carter B Set al. Endonasal instrumentation and aerosolization risk in the era of COVID-19: simulation, literature review, and proposed mitigation strategiesInt Forum Allergy Rhinol2020 [DOI] [PubMed]
- 14.Kowalski L P, Sanabria A, Ridge J Aet al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practiceHead Neck2020 [DOI] [PMC free article] [PubMed]
- 15.ENTUK. Guidance for ENT during the COVID-19 pandemic 2020 [Available from:https://www.entuk.org/guidance-ent-during-covid-19-pandemic
- 16.CFM.Combate à COVID-19 - Orientação geral ao trabalho dos médicos20/3/2020 [Available from:https://portal.cfm.org.br/images/comunicadocfmcovid.jpg
- 17.Brasil. Ministério da Saúde. Portaria No. 467, de 20 de março de 2020. Dispõe, em caráter excepcional e temporário, sobre as ações de Telemedicina, com o objetivo de regulamentar e operacionalizar as medidas de enfrentamento da emergência de saúde pública de importância internacional previstas no art. 3° da Lei n° 13.979, de 6 de fevereiro de 2020, decorrente da epidemia de COVID-19. Diário Oficial da União 23/03/2020 - Edição: 56-B - Seção: 1
- 18.Parikh S R, Avansino J R, Dick A Aet al. Collaborative multi-disciplinary incident command at seattle children's hospital for rapid preparatory pediatric surgery countermeasures to the COVID-19 PandemicJ Am Coll Surg2020;S1072-7515(20)30319-7 [DOI] [PMC free article] [PubMed]
- 19.van Doremalen N, Bushmaker T, Morris D H et al. Aerosol and surface stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564–1567. doi: 10.1056/NEJMc2004973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Vukkadala N, Qian Z J, Holsinger F C, Patel Z M, Rosenthal E.COVID-19 and the otolaryngologist - preliminary evidence-based reviewLaryngoscope2020 [DOI] [PMC free article] [PubMed]
- 21.Tran K, Cimon K, Severn M, Pessoa-Silva C L, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(04):e35797. doi: 10.1371/journal.pone.0035797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.WHO.Modes of transmission of virus causing COVID- 19:implications for IPC precaution recommendations. 26/3/2020 [This version updates the 27 March publication by providing definitions of droplets by particle size and adding three relevant publications.]Available from:https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations
- 23.Long Y, Hu T, Liu Let al. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysisJ Evid Based Med2020 [DOI] [PMC free article] [PubMed]
- 24.Ng K, Poon B H, Kiat Puar T Het al. COVID-19 and the Risk to Health Care Workers: A Case ReportAnn Intern Med2020 [DOI] [PMC free article] [PubMed]
- 25.Liang W, Guan W, Chen R et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21(03):335–337. doi: 10.1016/S1470-2045(20)30096-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bann D V, Patel V A, Saadi Ret al. Impact of coronavirus (COVID-19) on otolaryngologic surgery: Brief commentaryHead Neck2020 [DOI] [PMC free article] [PubMed]
- 27.Tay J K, Khoo M L, Loh W S.Surgical considerations for tracheostomy during the COVID-19 Pandemic: lessons learned from the severe acute respiratory syndrome outbreakJAMA Otolaryngol Head Neck Surg2020 [DOI] [PubMed]
- 28.Scheffer M. São Paulo, SP: FMUSP, CFM, Cremesp; 2018. Demografia médica no Brasil 2018; p. 286. [Google Scholar]