

Abstract
Objectives:
The Milan System for Reporting Salivary Gland Cytopathology (MSRSGC) established a standardized, tiered reporting system for salivary gland fine-needle aspiration (FNA) that has gained international acceptance among cytologists. Our goal was to review the key features of the MSRSGC to familiarize the surgical community with this system and its application to the FNA evaluation of salivary gland masses.
Methods:
A comprehensive review of the MSRSGC and its application in clinical practice.
Results:
The MSRSGC consists of six major diagnostic categories: 1) nondiagnostic, 2) non-neoplastic, 3) atypia of undetermined significance, 4) neoplasm (benign or salivary gland neoplasm of uncertain malignant potential), 5) suspicious for malignancy, and 6) malignant. Each diagnostic category is associated with an implied risk of malignancy with implications for clinical management.
Conclusions:
The MSRSGC is similar to the system used for reporting thyroid FNA, which is familiar to most otolaryngologists and head and neck surgeons. As this reporting system continues to gain popularity among pathologists, widespread understanding by surgeons will be important to standardize communication and classification of salivary gland cytopathology to improve clinical care.
Keywords: Fine-needle aspiration, salivary gland, cytopathology, Milan system
INTRODUCTION
Proper management of salivary gland disease is often predicated on accurate cytopathologic diagnosis. Along with clinical history, physical exam, and radiologic imaging, fine-needle aspiration (FNA) plays an important role at most large institutions in the presurgical evaluation of salivary gland masses.1–3 Salivary gland FNA is an effective means of diagnosing a majority of the most common neoplastic (e.g., pleomorphic adenoma and Warthin tumor) and non-neoplastic salivary gland lesions, which has direct implications on clinical management.4–9 Furthermore, FNA can also be useful to stratify low- and high-grade malignancies. Nonetheless, given the heterogeneity of salivary pathology, there is still a subset of salivary gland lesions where a specific diagnosis cannot be made based on cytologic features alone. Without a standardized reporting system, cytologic evaluation and reporting is a challenge.
Historically, there has been inconsistency in the terminology used for reporting the results of salivary gland FNA. This has resulted in confusion amongst clinicians and difficulty communicating clinically meaningful data between cytologists and treating clinicians, as well as standardizing treatment algorithms. To overcome these limitations, the ideal salivary gland FNA interpretation should be succinct, unambiguous, and clinically applicable. Furthermore, a standardized salivary gland FNA reporting system incorporating these principles should be universally accepted, much like The Bethesda System for Reporting Thyroid Cytopathology has become.10 Many of the guiding principles for creating an effective, universally accepted cytopathologic grading system were pioneered by The Bethesda System for Reporting Cervical/Vaginal Cytologic Diagnoses in 1988.11 Subsequently, there has been a significant trend toward the uniform reporting of cytology results for a variety of other specimen and tissue types, including thyroid, urine, breast, and effusions.
To address the need for a tiered diagnostic framework for salivary gland FNA, the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC) was developed in 2015 by an international taskforce of cytopathologists, surgical pathologists, and head and neck surgeons through the American Society of Cytopathology and the International Academy of Cytology.12 Similar to that of The Bethesda System for Reporting Thyroid Cytopathology, the objective of the MSRSGC is to standardize reporting of salivary gland cytology, promote better communication between clinicians and institutions, and ultimately improve patient care.12 The MSRSGC has gained widespread international acceptance among cytologists, and is already used to report cytology results at many institutions in the United States and worldwide.
The MSRSGC consists of six diagnostic categories: 1) nondiagnostic, 2) non-neoplastic, 3) atypia of undetermined significance (AUS), 4) neoplasm (subdivided into benign and salivary gland neoplasm of uncertain malignant potential), 5) suspicious for malignancy (SM), and 6) malignant (Table I). In comparison to existing descriptions and schema for salivary gland FNAs, the MSRSGC is able to correlate and stratify cytologic diagnosis with a risk of malignancy (ROM), which more easily facilitates its integration and use in clinical management algorithms. As such, the MSRSGC is transferable and practical for institutions with all levels of experience and expertise in salivary gland cytology. Here, we present an overview of each diagnostic category with proposed management strategies to familiarize clinicians and promote widespread acceptance of the MSRSGC in clinical practice.
TABLE I.
The Milan System for Reporting Salivary Gland Cytopathology: Implied Risk of Malignancy and Recommended Clinical Management.
| Diagnostic Category | Risk of Malignancy (%) | Usual Management* |
|---|---|---|
| Nondiagnostic | 25 | Repeat FNA, clinical and radiological follow-up |
| Non-neoplastic | 10 | Clinical and radiological follow-up |
| Atypia of undetermined significance | 20 | Repeat FNA or surgery |
| Neoplasm: benign | <5 | Surgery or clinical and radiological follow-up |
| Neoplasm: salivary gland neoplasm of uncertain malignant potential | 35 | Surgery |
| Suspicious for malignancy | 60 | Surgery |
| Malignant | >90 | Surgery |
Actual management may depend on other factors (clinical, radiographic) besides the FNA interpretation.
FNA = fine-needle aspiration.
Nondiagnostic
The nondiagnostic category includes salivary gland FNA samples limited by cellularity or preservation artifacts. Examples of nondiagnostic specimens include nonmucinous cyst contents, normal salivary gland elements in the setting of a clinically and radiographically defined mass, and samples with very scant or absent cellularity but without atypia. Specimens that should not be considered nondiagnostic include those containing mucinous cyst contents, atypia, abundant acellular matrix material, or inflammatory cells without an epithelial component. The nondiagnostic category carries a ROM of 25%.
If a nondiagnostic specimen is obtained, repeat FNA should be strongly considered. Ultrasound guidance (USG) is often useful for acquiring repeat samples when the original attempt was performed via palpation alone. If subsequent FNA specimens are also nondiagnostic despite USG and satisfactory sample preparation, ancillary studies may be necessary. Contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) should be considered if cross-sectional imaging has not yet been performed. When a patient’s clinical picture or imaging is concerning for malignancy, or if the nature of the lesion is in doubt, USG core needle biopsy (CNB), open biopsy, or surgical excision can be considered. However, both CNB and open biopsy are controversial due to the inherent risk of tumor spillage, and it is our belief that a standard parotidectomy approach (or submandibular gland resection) to these lesions, including facial nerve identification and dissection followed by frozen pathologic analysis, is preferred.
If a nondiagnostic sample returns with cyst contents only, complete aspirate of cyst contents under USG is warranted. If a solid component remains after aspiration, the lesion should be resampled. If the lesion disappears completely, ultrasound should be repeated in 3 to 4 months. Repeat FNA at the time of ultrasound surveillance is indicated when there is evidence of a recurrent lesion or if alternative surveillance imaging modalities such as CT or MRI redemonstrate the lesion.
Non-neoplastic
Non-neoplastic lesions of the salivary glands are common.13,14 The non-neoplastic category of the MSRSGC consists of benign entities such as reactive, metaplastic, and inflammatory changes associated with acute or chronic inflammation, sialolithiasis, or infection (Fig. 1). The implied ROM for the non-neoplastic category is approximately 10%, with studies ranging from 0% to 20%.15–17
Fig. 1.
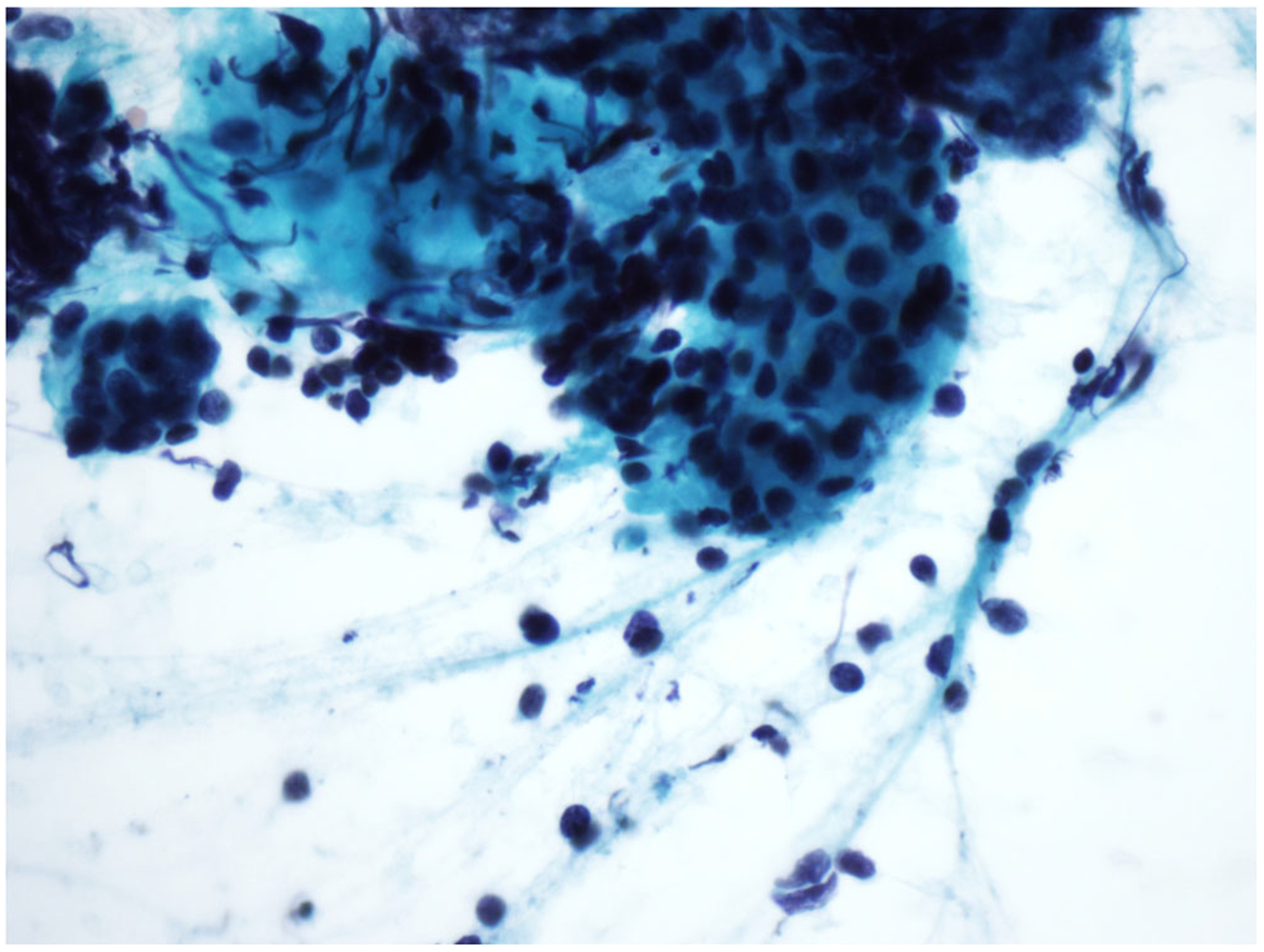
Non-neoplastic. This salivary gland fine-needle aspiration FNA sample shows features of chronic sialadenitis (Papanicolau stain, 600×).
Management of non-neoplastic samples is largely nonsurgical. Patients may be followed closely until there is a change in physical examination or imaging, at which point repeat FNA would be warranted to confirm the cytological diagnosis. It is important to consider USG FNA to decrease inadequate sampling and false negative diagnoses. If FNA findings are insufficient or do not correlate to clinical or radiographic findings, tissue sampling should be repeated. For reactive lymph nodes, flow cytometry studies are useful to confirm reactive lymphadenopathy and to exclude a low-grade lymphoproliferative lesion.
Atypia of undetermined significance (AUS)
The AUS category represents samples with morphological overlap between neoplastic and non-neoplastic processes, in which a clear distinction between the two cannot be made.18 The goal of AUS is to reduce the number of false-negative diagnoses in the non-neoplastic category while maintaining the significance of the neoplastic category.12 The MSRSGC recommendation is that atypical diagnoses comprise less than 10% of all FNA diagnoses.18 Examples of AUS include reactive and reparative atypia, low cellularity samples suggestive but not diagnostic of a neoplasm, cystic lesions with abundant mucin and/or a scant epithelial component, and salivary gland lesions ambiguous for a lymphoproliferative disorder. The ROM for AUS is approximately 20%.16,19–21
The suggested management of AUS begins with repeat FNA. USG FNA should be utilized if the initial sample was obtained by palpation alone. Cross-sectional imaging may also be used to further characterize these lesions. CNB, open biopsy, or surgical resection should be considered when clinical presentation is concerning for malignancy (e.g., coexisting facial nerve changes or history of cutaneous malignancy). Clinical judgment should guide the interval between follow- up, with 3 to 6 months as a general rule.
Neoplasm
Salivary gland neoplasms make up 6% of all head and neck tumors, with the parotid gland most commonly involved.13,15,22–25 The MSRSGC’s neoplasm category is subdivided into two groups: 1) benign and 2) salivary gland neoplasm of uncertain malignant potential (SUMP). The general expectation for management of these categories is cross-sectional imaging, followed by tumor resection with a narrow cuff or margin of normal tissue.
Benign
This subcategory is assigned to aspirates whose features satisfy the classical cytomorphologic criteria for benign lesions. Specific examples include pleomorphic adenoma, Warthin tumor, lipoma, hemangioma and schwannoma (Fig. 2). The ROM for the benign neoplasm category is <5%.
Fig. 2.
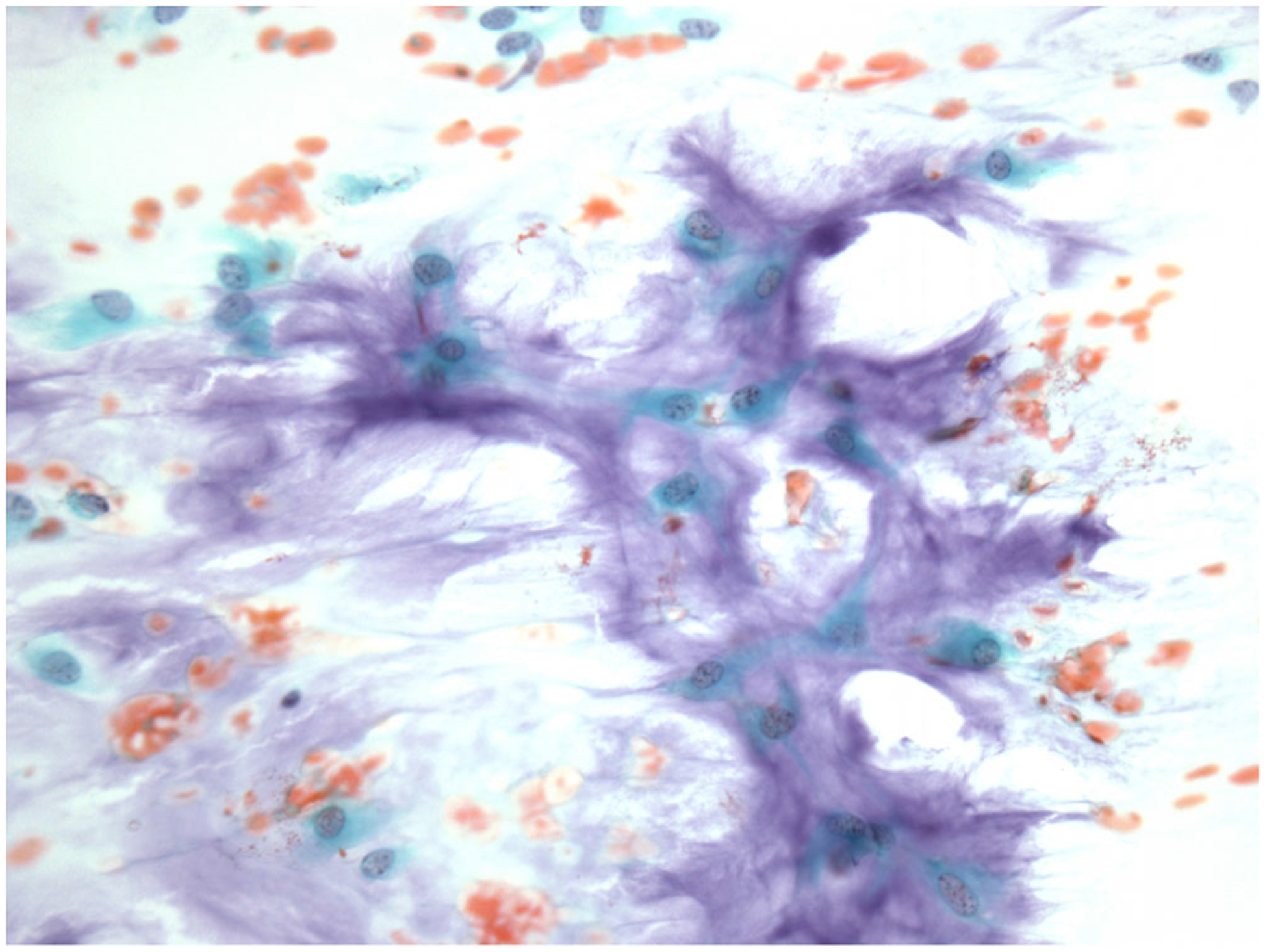
Neoplasm: benign. This salivary gland fine-needle aspiration sample shows classical features of pleomorphic adenoma (Papanicolau stain, 400×).
Complete resection is generally suggested for benign neoplastic lesions. For parotid gland lesions, cross-sectional imaging should be performed for all lesions, with an exception for very small lesions with clearly palpable borders. Lesions may be excised via either extracapsular dissection or nerve-sparing parotidectomy. Patients who are poor surgical candidates or those who do not accept the risk of nerve injury may be closely followed clinically without surgery. Management of submandibular gland lesions includes cross-sectional imaging, followed by surgical resection of the lesion en bloc, with the submandibular gland in a suprafascial plane, with care and attention to the marginal mandibular branch of the facial nerve to avoid unintended injury.
Salivary gland neoplasm of uncertain malignant potential (SUMP)
The SUMP subcategory designates aspirates for which a specific diagnosis cannot be made, but cytomorphologic features are consistent with a neoplastic process.12,26 Importantly, a malignant neoplasm cannot be entirely excluded with the differential diagnosis for SUMP aspirates including both benign and malignant lesions. The majority of corresponding pathologies will include cellular benign neoplasms, neoplasms with limited atypical features, and low-grade carcinomas. So-called basaloid neoplasms will typically be diagnosed by FNA in this category (Fig. 3). The ROM associated with SUMP aspirates is 35%.
Fig. 3.
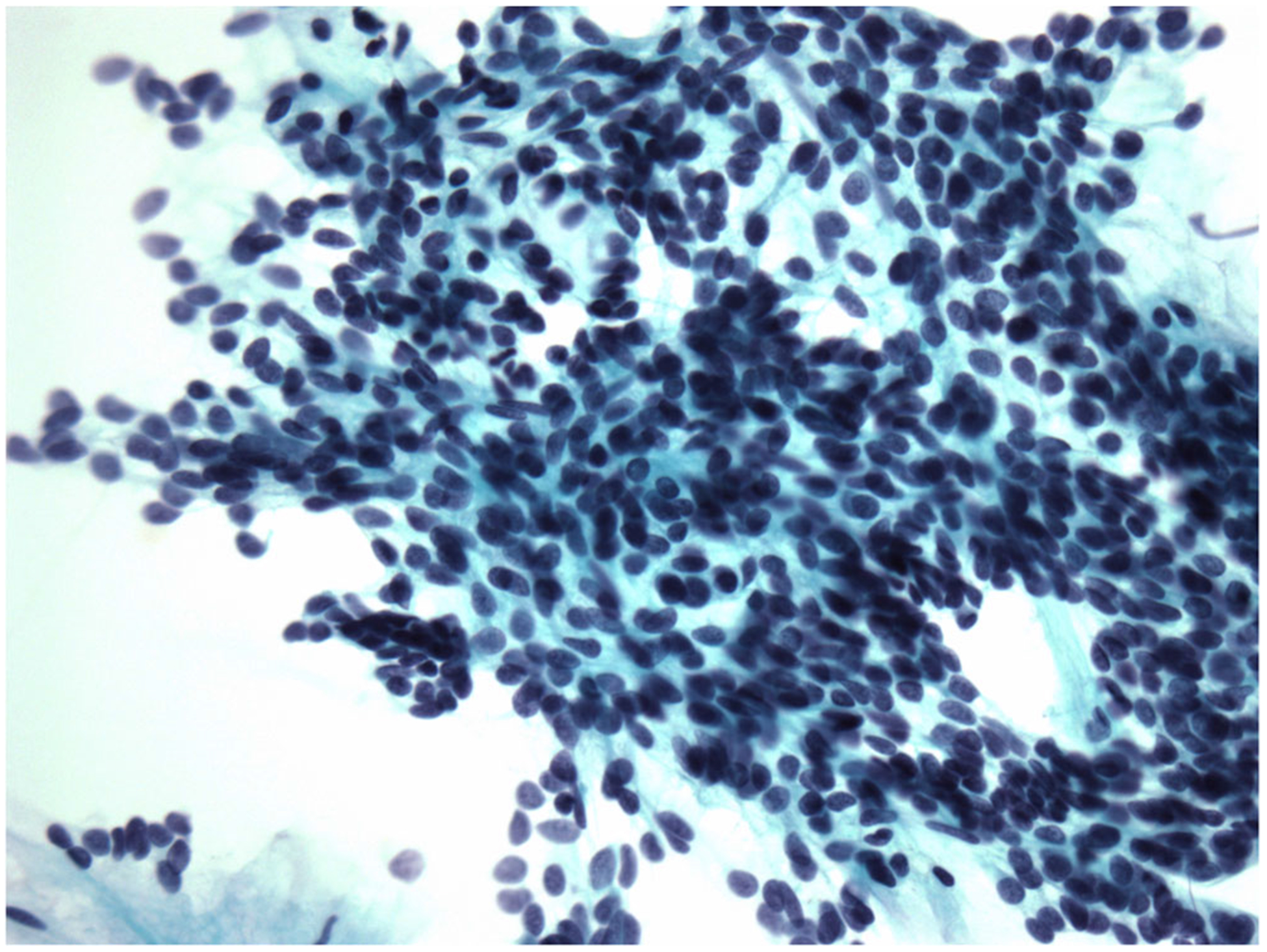
Neoplasm: salivary gland neoplasm of uncertain malignant potential. This basaloid neoplasm was diagnosed at resection as a basal cell adenoma (Papanicolaou stain, 400×).
Management with conservative surgical resection is necessary given the increased risk of low-grade malignancy. Intraoperative frozen section can be useful for improved histologic classification, which may also influence the decision for concomitant neck dissection (i.e., for intermediate and high-grade malignancies). For SUMP lesions involving the parotid gland, size and location of the tumor will dictate the type of parotidectomy and approach performed. Nerve-sparing parotidectomy is the most oncologically safe option and preferred by our group. For SUMP lesions of the submandibular gland, suprafascial excision should be performed, with the planned skin incision placed low enough to allow for neck dissection given the higher proportion of malignancy.
Suspicious for malignancy (SM)
Similar to AUS and SUMP, SM is an indeterminate diagnostic category. SM aspirates are highly suggestive of malignant neoplasms, but the cytomorphologic features alone are not definitive. Examples of SM specimens include those with a few markedly atypical cells or those suggestive of lymphoma without an adequate sample for immunophenotyping. Aspirates designated SM carry a ROM of 60% in the MSRSGC, with contributing studies reporting risk as high as 83%.27 Furthermore, the risk of a neoplastic lesion with SM samples is roughly 95%.27,28
Given the high ROM, salivary gland lesions in the SM group require cross-sectional imaging to evaluate extent of disease and staging prior to resection.29,30 Metastatic workup with chest imaging should also be performed. For parotid gland lesions, parotidectomy with facial nerve dissection and complete mass excision is required. The patient should also be informed and consented regarding facial nerve sacrifice, which will be dictated by intraoperative findings and frozen section. In this scenario, up-front facial reanimation procedures should also be discussed including, at a minimum, interposition grafting, nerve transfer, static slings, eye lid weight, and conservative measures such as eye care.
Elective, selective neck dissection should be performed for the clinically and radiographically N0 neck for tumors with size greater than 4 cm, high-grade features on frozen section of the primary site, extraglandular extension on imaging or intraoperative findings, or preoperative facial weakness.31,32 For SM aspirates with preoperative evidence of neck disease, selective neck dissection should be performed. Extent of dissection is based on location and stage of disease; however, levels II to IV are almost always required. When frozen section is unavailable, final histopathology may be used to guide the decision regarding a staged neck dissection. For all patients, the role of adjuvant radiation therapy versus neck dissection should be made in a multidisciplinary setting to optimize and standardize care.
Management of SM aspirates of the SMG is predicated on clinical and radiographic findings. For benign-appearing SM lesions without nodal disease, suprafascial SMG excision with a low skin incision should be considered, with concomitant selective neck dissection reserved for intermediate- or high-grade malignancies on frozen section. Submandibular gland excision with up-front neck dissection should be performed if cross-sectional imaging suggests a malignant process, frozen section shows a primary SMG malignancy, and pathological nodes are present.
Malignant
The malignant category includes primary salivary gland neoplasms, lymphomas, and sarcomas as well as metastatic carcinomas to salivary gland lymph nodes (Fig. 4). The application of ancillary immunohistochemical or molecular markers can be used to increase the specificity of the FNA diagnosis. To improve clinical management, FNA specimens should be classified when possible as low-grade or high-grade malignancy.33–35 For FNA cases where the grade is indeterminate, a definitive grade should not be assigned. The latter group will include a subset of difficult-to-grade, low-grade, and high-grade salivary gland cancers as well as most intermediate grade cancers. Additionally, an attempt should be made to correlate the FNA diagnosis with a specific diagnostic category as described in the 2017 World Health Organization Classification of Head and Neck Tumors.36
Fig. 4.
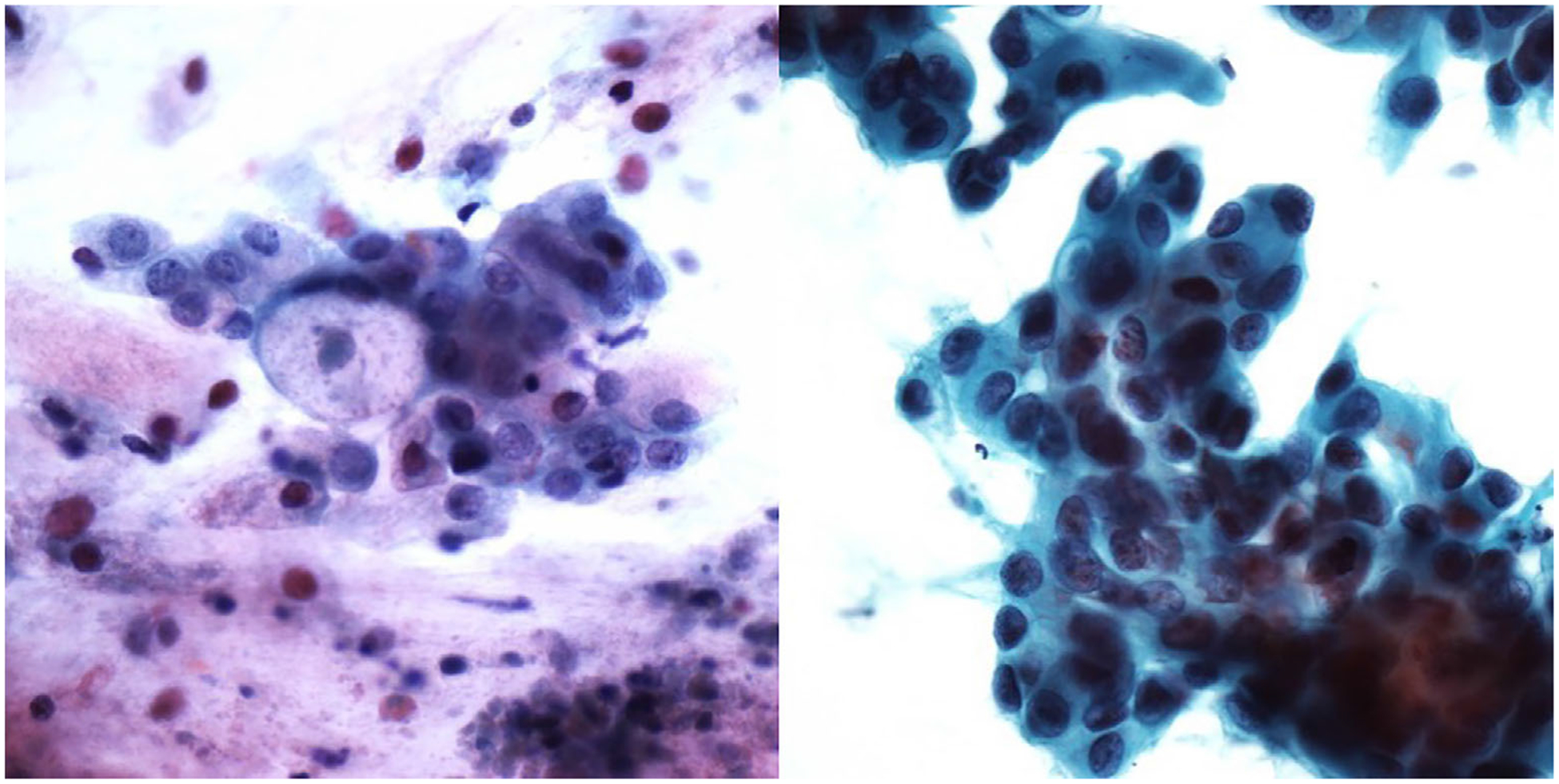
Malignant. These salivary gland fine-needle aspiration samples show characteristic cytologic features of low-grade mucoepidermoid carcinoma (left: Papanicolaou stain, 600×) and salivary duct carcinoma (right: Papanicolau stain, 400×).
After obtaining a malignant FNA sample, management should continue with CT of the neck and chest for staging and surgical planning. For low-grade parotid gland malignancies without neck involvement or other indications for neck dissection, complete excision with nerve-sparing parotidectomy is indicated. For intermediate- or high-grade malignancies, facial nerve dissection, total parotidectomy, and selective neck dissection should be performed regardless of neck status. Again, facial nerve sacrifice and reanimation procedures should be discussed preoperatively as described above.
For low-grade submandibular gland lesions without neck involvement or other indications for neck dissection, suprafascial submandibular gland resection is indicated. For intermediate or high-grade malignancies, suprafascial submandibular gland resection with selective neck dissection should be performed regardless of neck status.
For metastatic lesions with a confirmed origin, management should follow the standard of care based on primary tumor type. Cutaneous primaries often metastasize to intra- and periparotid lymph nodes and require nerve-sparing parotidectomy.37,38 A thorough skin examination for primary cutaneous lesions of the face, neck, and scalp (e.g., melanoma, Merkel cell carcinoma, cutaneous squamous cell carcinoma) should be completed by the otolaryngologist and a dermatologist. If a salivary gland lesion is metastatic from an unknown noncutaneous source, positron emission tomography/computed tomography may be indicated to locate the primary site. Selective neck dissection is usually indicated in this population, even when clinically N0, given the advanced nature of this disease.
CONCLUSION
Salivary gland FNA is a useful tool for the preoperative evaluation of salivary gland lesions and for guiding clinical management. The MSRSGC provides an evidence-based, tiered reporting framework for salivary gland FNA that stratifies samples, and therefore patients, based on risk of malignancy. Going forward, increased recognition and implementation of the MSRSGC will also allow for a better understanding of the risk of malignancy associated with salivary gland lesions in different diagnostic categories. Additionally, the ongoing discovery of genetic alterations and judicious use of assays such as immunohistochemistry and molecular testing will continue to increase the specificity of salivary gland FNA. The time for acceptance and implantation of a universal system for reporting salivary gland cytopathology is now. The MSRSGC is already being used by cytology labs internationally. It affords tremendous opportunity to improve patient care through standardized communication, consistent diagnosis, and safe and efficient clinical practice.
Acknowledgments
The authors have no funding, financial relationships, or conflicts of interest to disclose.
BIBLIOGRAPHY
- 1.Wang H, Fundakowski C, Khurana JS, Jhala N. Fine-needle aspiration biopsy of salivary gland lesions. Arch Pathol Lab Med 2015;139:1491–1497. [DOI] [PubMed] [Google Scholar]
- 2.Griffith CC, Pai RK, Schneider F, et al. Salivary gland tumor fine-needle aspiration cytology: a proposal for a risk stratification classification. Am J Clin Pathol 2015;143:839–853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zbaren P, Schar C, Hotz MA, Loosli H. Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope 2001;111(11 pt 1):1989–1992. [DOI] [PubMed] [Google Scholar]
- 4.Song IH, Song JS, Sung CO, et al. Accuracy of core needle biopsy versus fine needle aspiration cytology for diagnosing salivary gland tumors. J Pathol Transl Med 2015;49:136–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zbaren P, Nuyens M, Loosli H, Stauffer E. Diagnostic accuracy of fine-needle aspiration cytology and frozen section in primary parotid carcinoma. Cancer 2004;100:1876–1883. [DOI] [PubMed] [Google Scholar]
- 6.Postema RJ, van Velthuysen ML, van den Brekel MW, Balm AJ, Peterse JL. Accuracy of fine-needle aspiration cytology of salivary gland lesions in the Netherlands Cancer Institute. Head Neck 2004;26:418–424. [DOI] [PubMed] [Google Scholar]
- 7.Raymond MR, Yoo JH, Heathcote JG, McLachlin CM, Lampe HB. Accuracy of fine-needle aspiration biopsy for Warthin’s tumours. J Otolaryngol 2002;31:263–270. [DOI] [PubMed] [Google Scholar]
- 8.Al-Khafaji BM, Nestok BR, Katz RL. Fine-needle aspiration of 154 parotid masses with histologic correlation: ten-year experience at the University of Texas M. D. Anderson Cancer Center. Cancer 1998;84:153–159. [PubMed] [Google Scholar]
- 9.Eytan DF, Yin LX, Maleki Z, et al. Utility of preoperative fine needle aspiration in parotid lesions. Laryngoscope 2018;128:398–402. [DOI] [PubMed] [Google Scholar]
- 10.Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2009;19:1159–1165. [DOI] [PubMed] [Google Scholar]
- 11.Solomon D. The 1988 Bethesda System for reporting cervical/vaginal cytologic diagnoses: developed and approved at the National Cancer Institute Workshop in Bethesda, Maryland, December 12–13, 1988. Hum Pathol 1990;21:704–708. [DOI] [PubMed] [Google Scholar]
- 12.Rossi ED, Faquin WC, Baloch Z, et al. The Milan System for Reporting Salivary Gland Cytopathology: analysis and suggestions of initial survey. Cancer Cytopathol 2017;125:757–766. [DOI] [PubMed] [Google Scholar]
- 13.Faquin WC, Powers CN. Salivary Gland Cytopathology. New York, NY: Springer; 2008. [Google Scholar]
- 14.Mohan H, Tahlan A, Mundi I, Punia RPS, Dass A. Non-neoplastic salivary gland lesions: a 15-year study. Eur Arch Otorhinolaryngol 2011;268:1187–1190. [DOI] [PubMed] [Google Scholar]
- 15.Rossi ED, Wong LQ, Bizzarro T, et al. The impact of FNAC in the management of salivary gland lesions: institutional experiences leading to a risk-based classification scheme. Cancer Cytopathol 2016;124:388–396. [DOI] [PubMed] [Google Scholar]
- 16.Jain R, Gupta R, Kudesia M, Singh S. Fine needle aspiration cytology in diagnosis of salivary gland lesions: a study with histologic comparison. Cytojournal 2013;10:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stewart CJ, MacKenzie K, McGarry GW, Mowat A. Fine-needle aspiration cytology of salivary gland: a review of 341 cases. Diagn Cytopathol 2000; 22:139–146. [DOI] [PubMed] [Google Scholar]
- 18.Wang H, Malik A, Maleki Z, et al. “Atypical” salivary gland fine needle aspiration: risk of malignancy and interinstitutional variability. Diagn Cytopathol 2017;45:1088–1094. [DOI] [PubMed] [Google Scholar]
- 19.Tyagi R, Dey P. Diagnostic problems of salivary gland tumors. Diagn Cytopathol 2015;43:495–509. [DOI] [PubMed] [Google Scholar]
- 20.Brennan PA, Davies B, Poller D, et al. Fine needle aspiration cytology (FNAC) of salivary gland tumours: repeat aspiration provides further information in cases with an unclear initial cytological diagnosis. Br J Oral Maxillofac Surg 2010;48:26–29. [DOI] [PubMed] [Google Scholar]
- 21.Hughes JH, Volk EE, Wilbur DC; Cytopathology Resource Committee, College of American Pathologists. Pitfalls in salivary gland fine-needle aspiration cytology: lessons from the College of American Pathologists Interlaboratory Comparison Program in Nongynecologic Cytology. Arch Pathol Lab Med 2005;129:26–31. [DOI] [PubMed] [Google Scholar]
- 22.Viswanathan K, Sung S, Scognamiglio T, Yang GCH, Siddiqui MT, Rao RA. The role of the Milan System for Reporting Salivary Gland Cytopathology: a 5-year institutional experience. Cancer Cytopathol 2018;126:541–551. [DOI] [PubMed] [Google Scholar]
- 23.Colella G, Cannavale R, Flamminio F, Foschini MP. Fine-needle aspiration cytology of salivary gland lesions: a systematic review. J Oral Maxillofac Surg 2010;68:2146–2153. [DOI] [PubMed] [Google Scholar]
- 24.Klijanienko J, Vielh P. Fine-needle sampling of salivary gland lesions. III. Cytologic and histologic correlation of 75 cases of adenoid cystic carcinoma: review and experience at the Institut Curie with emphasis on cytologic pitfalls. Diagn Cytopathol 1997;17:36–41. [DOI] [PubMed] [Google Scholar]
- 25.Klijanienko J, Vielh P. Fine-needle sampling of salivary gland lesions. II. Cytology and histology correlation of 71 cases of Warthin’s tumor (adenolymphoma). Diagn Cytopathol 1997;16:221–225. [DOI] [PubMed] [Google Scholar]
- 26.Pusztaszeri M, Baloch Z, Vielh P, Faquin WC. Application of the Milan system for reporting risk stratification in salivary gland cytopathology. Cancer Cytopathol 2018;126:69–70. [DOI] [PubMed] [Google Scholar]
- 27.Maleki Z, Miller JA, Arab SE, et al. “Suspicious” salivary gland FNA: risk of malignancy and interinstitutional variability. Cancer Cytopathol 2018; 126:94–100. [DOI] [PubMed] [Google Scholar]
- 28.Wei S, Layfield LJ, LiVolsi VA, Montone KT, Baloch ZW. Reporting of fine needle aspiration (FNA) specimens of salivary gland lesions: a comprehensive review. Diagn Cytopathol 2017;45:820–827. [DOI] [PubMed] [Google Scholar]
- 29.Yousem DM, Kraut MA, Chalian AA. Major salivary gland imaging. Radiology 2000;216:19–29. [DOI] [PubMed] [Google Scholar]
- 30.Silvers AR, Som PM. Salivary glands. Radiol Clin North Am 1998;36: 941–966, vi. [DOI] [PubMed] [Google Scholar]
- 31.Armstrong JG, Harrison LB, Thaler HT, et al. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer 1992; 69:615–619. [DOI] [PubMed] [Google Scholar]
- 32.Frankenthaler RA, Byers RM, Luna MA, Callender DL, Wolf P, Goepfert H. Predicting occult lymph node metastasis in parotid cancer. Arch Otolaryngol Head Neck Surg 1993;119:517–520. [DOI] [PubMed] [Google Scholar]
- 33.Luna MA. Salivary mucoepidermoid carcinoma: revisited. Adv Anat Pathol 2006;13:293–307. [DOI] [PubMed] [Google Scholar]
- 34.Kim BY, Hyeon J, Ryu G, et al. Diagnostic accuracy of fine needle aspiration cytology for high-grade salivary gland tumors. Ann Surg Oncol 2013;20: 2380–2387. [DOI] [PubMed] [Google Scholar]
- 35.Schmidt RL, Hall BJ, Wilson AR, Layfield LJ. A systematic review and meta-analysis of the diagnostic accuracy of fine-needle aspiration cytology for parotid gland lesions. Am J Clin Pathol 2011;136:45–59. [DOI] [PubMed] [Google Scholar]
- 36.El-Naggar AK, Chan JKC, Rubin Grandis J, Takata T, Slootweg PJ; International Agency for Research on Cancer WHO Classification of Head and Neck Tumours. Lyon, France: International Agency for Research on Cancer; 2017. [Google Scholar]
- 37.O’Brien CJ. The parotid gland as a metastatic basin for cutaneous cancer. Arch Otolaryngol Head Neck Surg 2005;131:551–555. [DOI] [PubMed] [Google Scholar]
- 38.Chua MS, Veness MJ, Morgan G, et al. Parotid lymph-node metastases from cutaneous squamous-cell carcinomas: treatment outcome and prognostic factors following surgery and adjuvant radiotherapy. Australas Radiol 2002;46:174–179. [DOI] [PubMed] [Google Scholar]