

Abstract
Objective. To review the literature regarding the use of learning style frameworks in health science education, with particular attention to learning outcomes and use for self-awareness.
Findings. Of the 415 articles identified in an initial search of the literature, 31 articles involving learning style frameworks were included after screening titles, abstracts, and full texts. Multiple learning style frameworks, including VARK, Kolb Learning Style Inventory, Honey and Mumford Learning Style Questionnaire, and Pharmacist Inventory of Learning Styles, have been used in various health science education disciplines, including medicine, nursing, and pharmacy. Most publications were descriptive in nature, reporting the learning styles of the given student cohort. Most studies that attempted to find a correlation between learning style and learning outcomes found none. In cases where a correlation was found, it was weak or inconsistent with findings from other published studies. No identified studies described use of learning style frameworks for increasing self-awareness in learners.
Summary. While several different learning style inventories have been used to assess health science education students, their utility for predicting learning outcomes appears to be weak. Using learning style inventories to improve learner self-awareness is an unexplored area of education and research.
Keywords: health science education, learning style, affective domain
INTRODUCTION
Self-awareness, which includes being aware of one’s knowledge, attitudes, behaviors, and emotions, is a foundation on which successful professional development is built.1 Self-awareness is an element of emotional intelligence and impacts a health professional’s ability to provide effective patient care.1-3 Therefore, having self-awareness is crucial for pharmacists and pharmacy learners. The 2016 Standards for Doctor of Pharmacy (PharmD) degree programs published by the Accreditation Council for Pharmacy Education include self-awareness as an essential component for students to develop.4 Since the release of Standards 2016, several papers examining ways to assess, document, and improve the self-awareness of student pharmacist have been published,3,5 but a single method that works for all colleges and schools of pharmacy has not been identified.
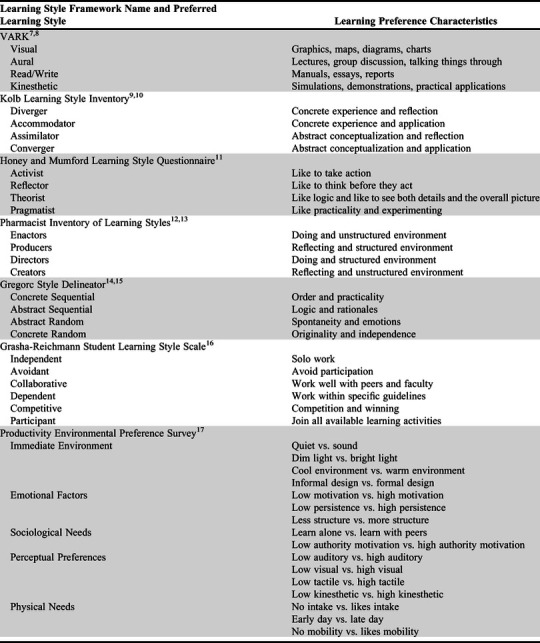
Learning style frameworks have been used by educators with learners at different educational levels in attempts to improve the learning ability. Learning styles can be defined as “the manner in which individuals choose to or are inclined to approach a learning situation.”6 Several learning style frameworks have been described in the literature, including the Visual, Aural, Read/Write, Kinesthetic (VARK) model, the Kolb Learning Style Inventory (LSI), the Honey and Mumford Learning Style Questionnaire (LSQ), the Pharmacist Inventory of Learning Styles (PILS), the Gregorc Style Delineator (GSD), the Grasha-Reichmann Student Learning Style Scale (GRSLSS), and the Productivity Environmental Preference Survey (PEPS). Some learning style frameworks, such as VARK, focus on how learners obtain information, which is usually through the senses. In the VARK framework, learners commonly have multiple learning preferences, termed multimodal.7,8 The Kolb LSI, PILS, and Honey and Mumford LSQ assess learners based on how they perceive experiences,9-13 with PILS being developed specifically for pharmacists and pharmacy learners.12,13 The GSD assesses perception and ordering,14,15 while the GRSLSS assesses learning style in relation to interaction with others.16 The PEPS evaluates how learning preference and environmental factors affect learning.17 A description of each learning style and the corresponding learning preference(s) is included in Table 1.
Table 1.
Learning Style Frameworks and Associated Learning Preference Characteristics
Given the number of easily accessible learning style frameworks, they are attractive tools for educators to use in improving students’ learning or other outcomes. However, it is unknown whether any learning style framework can be used as a tool for increasing the self-awareness of a student pursuing a professional degree. The objective of this systematic review was to identify the ways in which learning style frameworks have been used in pharmacy and other health science education, with a focus on their use for enhancing student self-awareness.
METHODS
Multiple databases, including PubMed (1966-2018), Ebsco’s CINAHL (1982-2018), Education Full Text (1983-2018), Professional Development Collection (1930-2018), ProQuest’s ERIC database (1966-2018), and Web of Science (1864-2018) were searched in November 2018. The database search was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18 The searches used subject headings and truncated, phrase-searched (as appropriate) keywords for the concepts of personality and learning style assessment and health professions. Sample search terms included “learning style,” “learning style inventory,” “Kolb learning style inventory,” “VARK,” and “PILS.” The search encompassed multiple health science education disciplines, including medicine, pharmacy, dentistry, nursing, veterinary medicine, physician assistant, occupational therapy, physical therapy, dietetics, speech language pathology, and allied health professions. A sample PubMed search string is included in Appendix 1. No date restrictions or limitations on study type were used in the search, but the limit of English language was used. Additionally, key pharmacy education journals were hand searched using the term “learning style.”
After removal of any duplicates, two authors independently reviewed the titles and abstracts to ensure the articles were relevant to learning style and/or personality framework use in health science students. Any discrepancies over whether an article should be included were discussed until consensus was reached. Next, full-text versions of the articles based on pre-set inclusion/exclusion criteria, (ie, use of a learning style or personality framework in health science education students) were reviewed. The following exclusion criteria were applied to both the title and abstract and the full text review: no students included in the study, no learning style or personality framework used, only undergraduate non-health professions students included, article not in English, validation of instrument study, no full-text available, and article type was a commentary. Articles were further divided based on the type of framework used: learning style, personality, or both.
Extracted data from the articles included citation details, study type, type of health science study included, learning style and/or personality framework used, and any outcomes reported (learning or non-cognitive). Articles using the same framework were grouped and evaluated for how the framework was used with health science students.
RESULTS
Following the initial database search, 415 articles were identified for evaluation. After removing duplicates, 302 unique results remained. After review of titles and abstracts, the authors agreed on either the inclusion or exclusion of 272 of 302 titles and/or abstracts (90% agreement). For the 30 titles or abstracts on which there were differences of opinion, the screening authors came to a consensus about inclusion or exclusion. The most common disagreement among the authors involved articles that included only applicants to a health science education program but no currently enrolled students. During discussion, the authors decided to exclude these articles. Overall, 142 articles were excluded during title and abstract review. The 160 articles remaining required a full-text review. Of these articles, 59 were excluded after applying the inclusion/exclusion criteria to the full texts. This left 101 articles: 30 used at least one learning style framework, 70 used at least one personality framework, and one used both a learning style and a personality framework. A summarized search strategy is included as a PRISMA diagram in Figure 1.
Figure 1.

Frequency of Personality and Learning Style Frameworks in Health Science Education
Of the articles identified involving learning style frameworks, 17 used the VARK framework alone, five used Kolb alone, two used VARK and Kolb, one used both VARK and Honey and Mumford LSQ, two used Honey and Mumford LSQ alone, one used PILS alone, one used GSD and PILS, one used GRSLSS alone, and one used PEPS alone. The most commonly reported learning style preference within each framework by health science discipline student type are reported in Table 2. Select results of studies that used learning style frameworks are presented in Table 3.
Table 2.
Most Common Learning Style Preferences by Framework and Health Science Discipline
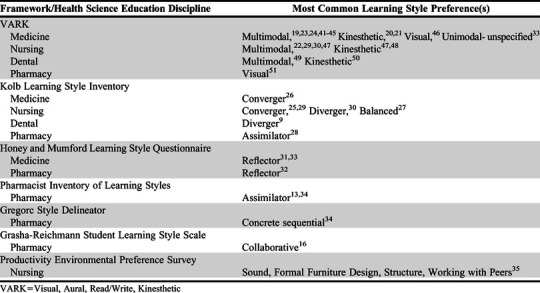
Table 3.
Select Outcomes of Learning Style Framework Studies
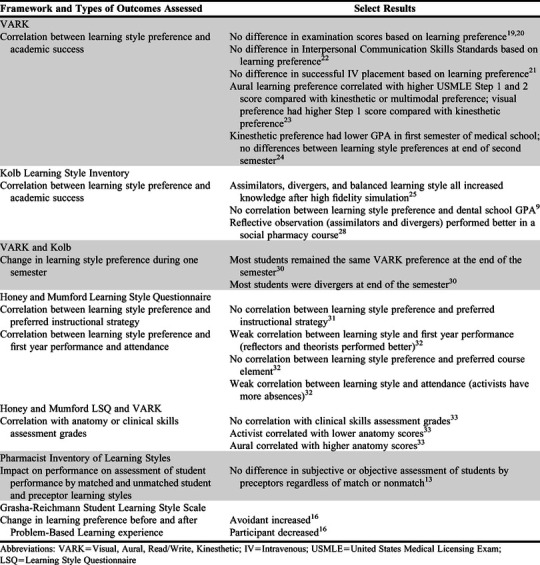
Of the articles that used the VARK framework alone, 11 involved medical students, three involved nursing students, two involved dental students, and one involved pharmacy students. Most identified publications were descriptive in nature, employing a cross-sectional study design by administering the VARK assessment one time in a given student cohort. These studies most commonly found that students preferred a multimodal approach to learning (Table 2). Four of the six studies attempting to find a correlation between the VARK framework and an academic outcome (eg, grades on a specific assessment, ability to perform a skill) did not find a significant correlation (Table 3).19-22 These studies were cross-sectional in nature, assessing VARK preference one time and comparing those results with an academic outcome.19-22 The two studies that found a significant correlation between a VARK preference and a learning outcome were conducted by Kim and Gilbert and Paiboonsithiwong and colleagues.23,24 Kim and Gilbert surveyed 62 applicants to a general surgery residency program and found that medical students with an aural learning preference performed better on the United States Medical Licensing Examination Step 1 and Step 2 compared with medical students with a kinesthetic or multimodal learning preference.23 Additionally, they found that those with a visual preference had higher Step 1 scores than those with a kinesthetic preference.23 The study found no other significant differences. Paiboonsithiwong and colleagues surveyed 140 first-year medical students and found that medical students with a kinesthetic learning preference had lower GPAs in the first semester, but found no other differences among learning preferences, including in second semester GPA.24 They also found no differences between VARK preference and Perceived Stress Scale score.24 None of the identified studies described how learners used the results to increase their self-awareness.
Of the reports that used the Kolb Learning Style Inventory alone, two involved nursing students; one involved dental students; one involved orthopedic residency applicants, residents, and faculty members; and one involved pharmacy students. Two of the studies were descriptive, cross-sectional studies that identified the breakdown of Kolb learning preferences in their cohorts.25,26 One of the three studies that attempted to correlate Kolb learning preferences with a learning outcome found no association between dental students’ learning style preference and either GPA or the senior students’ choice of specialty practice.9 The other two studies attempting to find a correlation were conducted by Shinnick and Woo and Tsingos and colleagues.27,28 Shinnick and Woo conducted a cross-sectional study in 161 nursing students and found that students who were classified as assimilators had the highest increase in pretest to posttest score after a heart failure simulation (mean change of 16.7 points), compared to students who were classified as other learning styles (mean change of 7 points).27 Tsingos and colleagues surveyed pharmacy students and found a significantly higher academic performance in a social pharmacy course among those students who prefer to use reflective observation to process information, which are the diverger and assimilator preferences (64.1 for reflective observers, 61.5 for non-reflective observers).28 None of the identified publications described how the learning style results were used by learners to develop self-awareness.
Two studies used both the VARK and Kolb frameworks and both involved nursing students. One study was descriptive and cross-sectional in nature and characterized the preferences of master’s level nursing students.29 Mitchell and colleagues looked at how learning preference changed over one semester, administering the VARK and Kolb assessments to 96 nursing students at the beginning and end of the semester. On the VARK assessment, 45% of the learners had the same preference as they did at the beginning of the semester, but 30% became more multi-modal learners.30 On the Kolb assessment, there was a 40% increase in the number of students with diverging learning preferences, with 57% of students changing their learning preference.30
Two studies used the Honey and Mumford LSQ, one with pharmacy and chemistry students and one with medical students, and a third study used the LSQ in combination with the VARK in medical students. Bhalli and colleagues surveyed 77 medical students to determine not only their learning style preference, but also their preferred instructional strategies.31 They found that the students preferred active-learning strategies, but there was no correlation between LSQ preference and preferred instructional strategy.31 Sharif and colleagues investigated the difference in learning styles and learning outcomes between 275 first-year pharmacy students and 127 first-year chemistry students.32 They found that reflectors and theorists tended to do better on first year examinations, while activists tended to do worse on first-year examinations; however, the Pearson coefficients found were small (0.2 for reflectors and -0.2 for activists).32 There was no relationship between learning style and second, third, or fourth-year examinations.32 O’Mahony and colleagues explored whether a preference for the LSQ and/or VARK framework was associated with grades in anatomy or clinical skills assessment in 327 medical students.33 There were no significant associations between any kind of preference and grades in clinical skills assessment.33 There was an association between activist type and poorer anatomy scores, as well as between aural preference and better anatomy scores.33 However the R2 value was only 0.16, indicating that these preferences did not account for significant variability in the grades.33 None of the identified studies described how students used the results for self-awareness.
The PILS was used in two studies in pharmacy students. One study used both PILS and GSD to compare learning styles between pharmacy students and faculty members,34 and the most common student preferences found are included in Table 2. Robles and colleagues used PILS to identify learning styles of both pharmacy students and pharmacy preceptors, as well as any impact on learning when the preceptors and students had matched learning styles vs unmatched learning styles.13 There were no significant differences in either subjective (competency assessment) or objective (final examination) evaluations by preceptors of students with matched vs unmatched learning styles.13 There was no description of how the pharmacy students used their PILS and/or GSD results for self-awareness.
Novak and colleagues compared second-year pharmacy students’ GRSLSS before and after a problem-based learning (PBL) experience in a cross-sectional study.16 There was a significant increase in the number of students with the avoidant learning style and a significant decrease in those with the participant learning style.16 The publication did not describe how the results were shared with students in a way that increased their self-awareness.
Hallin described the differences in PEPS in nursing students between two campuses and over multiple semesters.35 Overall, there was only one difference in learning style preference: tactile learning was more preferred at one campus.35 The most common preference differed for most semesters.35 The authors did not describe how the nursing students used the results for self-awareness.
DISCUSSION
Multiple learning-style frameworks have been used in different health science education disciplines, as evidenced by this systematic review. Most of the identified published studies merely described the learning styles of a given population of learners (and possibly other groups, too) with no assessment of learning outcomes. For those studies that attempted to correlate learning style with a learning outcome, there often was no correlation, and if a correlation was present, the correlation tended to be weak. This finding is consistent with learners across different levels of education, which has given rise to criticism of the use of learning style frameworks for predicting learning outcomes in education entirely.36-38 Therefore, these results should give pharmacy educators pause in using learning style frameworks to assess or predict any learning outcomes for a given cohort of students.
What was notably absent in all of the identified published studies was how the classification of learning style was used by the learner to increase their self-awareness or metacognition. For example, none of the identified studies described the learner’s reaction to discovering their learning style or whether identification of their learning style influenced the way the learner studied, changed the way the learner preferred to study, or helped the learner improve their own personal learning results. These are outcomes that could be explored in future research using any or all of the learning style frameworks identified in this review. An additional avenue for future research would be to conduct a broader systematic review of other educational literature, including educational psychology literature, for guidance on how learning style frameworks might be applied to professional health science education students. For example, Gardner’s Theory of Multiple Intelligences, which is similar to learning styles, has been applied to many K-12 educational settings to foster learning in different modalities. However, in this review, we found no direct evidence of use of his theories in health science education.39,40
One of the strengths of this review is the inclusion of all health science education disciplines rather than limiting it to just pharmacy education. An additional strength was the inclusion of multiple databases in the literature search, rather than limiting the search to just PubMed. A limitation of the study is the possibility that some relevant studies were missed because they were not indexed in the searched databases; however, a hand search of selected pharmacy education journals was conducted to try to limit this risk. Additionally, the literature search was conducted in November 2018, so publications that are more recent would not have been found in the formal search process. Pharmacy educators should continue to review current literature in this area to determine the best way to use learning style frameworks for student self-awareness.
CONCLUSION
In this review, we found use of a wide range of learning style frameworks in health science education. Most of the articles identified were descriptive studies and others had little impact on educational outcomes. Given that there is little published data on effective ways to use learning style frameworks in health science education and a complete lack of information on their use to improve student self-awareness, future research should seek to answer these questions.
Appendix 1. Sample PubMed Search String
(“learning style*”[tiab] OR “learning style inventory”[tiab] OR “kolb learning style inventory”[tiab] OR “Kolb learning style questionnaire”[tiab] OR VARK[tiab] OR “VARK questionnaire”[tiab] OR “H-PILS”[tiab] OR “Health Professionals Inventory of Learning Styles”[tiab] OR ”StrengthsFinder”[tiab]) AND ("medical education"[tiab] OR "medical student"[tiab] OR "pharmacy education"[tiab] OR "pharmacy student"[tiab] OR "dental education"[tiab] OR "dental student"[tiab] OR "nursing education"[tiab] OR "nursing student"[tiab] OR "veterinary medicine education"[tiab] OR "veterinary student"[tiab] OR "physician assistant education"[tiab] OR "physician assistant student"[tiab] OR "occupational therapy student"[tiab] OR "occupational therapy education"[tiab] OR "physical therapy student"[tiab] OR "physical therapy education"[tiab] OR "dietetics education"[tiab] OR "dietetics student"[tiab] OR "speech language pathology education"[tiab] OR "speech-language pathology education"[tiab] OR "speech-language pathology student"[tiab] OR "allied health education"[tiab] OR "allied health student"[tiab])
REFERENCES
- 1.Erich T. What self-awareness really is (and how to cultivate it). https://hbr.org/2018/01/what-self-awareness-really-is-and-how-to-cultivate-it. Accessed July 6, 2020.
- 2.Romanelli F, Cain J, Smith KM. Emotional intelligence as a predictor of academic and/or professional success. Am J Pharm Educ. 2006;70(3):Article 69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maxwell WD, Grant AD, Fabel PH, et al. Impact of the Birkman method assessment on pharmacy student self-confidence, self-perceptions, and self-awareness. Am J Pharm Educ. 2016;80(9):Article 148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Accreditation Council for Pharmacy Education. Accreditation Standards and Key Elements for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree. February 2015. https://www.acpe-accredit.org/pharmd-program-accreditation/. Accessed July 6, 2020.
- 5.Hughes JA, Cleven AJ, Ross J, et al. A comprehensive reflective journal-writing framework for pharmacy students to increase self-awareness and develop actionable goals. Am J Pharm Educ 2019;83(3):Article 6554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cassidy S. Learning styles: an overview of theories, models, and measures. Int J Exp Educ Psychol. 2004;24(4):419-444. [Google Scholar]
- 7.Fleming ND. I’m different not dumb. Modes of presentation (VARK) in the tertiary classroom. Res Dev Higher Educ. 1995;18:308-313. [Google Scholar]
- 8.Vark Learn Limited. The VARK modalities. http://vark-learn.com/introduction-to-vark/the-vark-modalities/. Accessed July 6, 2020.
- 9.AlQahtani DA, Al-Gahtani SM. Assessing learning styles of Saudi dental students using Kolb’s Learning Style Inventory. J Dent Educ. 2014;78(6):927-933. [PubMed] [Google Scholar]
- 10.Kolb’s learning styles and experiential learning cycle. https://www.simplypsychology.org/learning-kolb.html. Accessed July 6, 2020. [Google Scholar]
- 11.Honey P, Mumford A. The Manual of Learning Styles. 3rd ed. Maidenhead, Berkshire, UK: Honey Press; 1992. [Google Scholar]
- 12.Austin Z. Development and Validation of the Pharmacists' Inventory of Learning Styles (PILS). Am J Pharm Educ. 2004;68(2):Article 37. [Google Scholar]
- 13.Robles J, Cox CD, Seifert CF. The impact of preceptor and student learning styles on experiential performance measures. Am J Pharm Educ. 2012;76(7):Article 128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Coffield F, Moseley D, Hall E, et al. Learning styles and pedagogy in post-16 learning: a systematic and critical review. https://www.voced.edu.au/content/ngv:13692. Accessed July 6, 2020.
- 15.Gregorc AF. Anthony F. Gregorc. https://www.anthonyfgregorc.com/. Accessed July 6, 2020. [Google Scholar]
- 16.Novak S, Shah S, Wilson JP, et al. Pharmacy students’ learning styles before and after a problem-based learning experience. Am J Pharm Educ. 2006;70(4):Article 74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Productivity Environmental Preferences Survey. https://www.collegesuccess1.com/PEPS.htm. Accessed July 6, 2020.
- 18.Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Urval RP, Kamath A, Ullal S, et al. Assessment of learning styles of undergraduate medical students using the VARK questionnaire and the influence of sex and academic performance. Adv Physiol Educ. 2014;38:216-220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liew S-C, Sidhu J, Barua A. The relationship between learning preferences (styles and approaches) and learning outcomes among pre-clinical undergraduate medical students. BMC Med Educ. 2015;15:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Papanagnou D, Serrano A, Barkley K, et al. Does tailoring instructional style to a medical student’s self-perceived learning style improve performance when teaching intravenous catheter placement? A randomized controlled study. BMC Med Educ. 2016;16:205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Azari S, Mokhtari S, Mousavi H, et al. Relationship between learning styles and interpersonal communication skills of nursing student in Medical Sciences Tehran University in 2012. J Med Life. 2015;8:178-183. [PMC free article] [PubMed] [Google Scholar]
- 23.Kim RH, Gilbert T. Learning style preferences of surgical residency applicants. J Surg Res. 2015;198:61-65. [DOI] [PubMed] [Google Scholar]
- 24.Paiboonsithiwong S, Kunanitthaworn N, Songtrijuck N, et al. Learning styles, academic achievement, and mental health problems among medical students in Thailand. J Educ Eval Health Prof. 2016;13:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lee J, Lee Y, Lee S, et al. Effects of high-fidelity patient simulation led clinical reasoning course: Focused on nursing core competencies, problem solving, and academic self-efficacy. Jpn J Nurs Sci. 2016;13:20-28. [DOI] [PubMed] [Google Scholar]
- 26.Richard RD, Deegan BF, Klena JC. The learning styles of orthopedic residents, faculty, and applicants at an academic program. J Surg Educ. 2014;71(1):110-118. [DOI] [PubMed] [Google Scholar]
- 27.Shinnick MA, Woo MA. Learning style impact on knowledge gains in human patient simulation. Nurse Educ Today. 2015;35(1):63-67. [DOI] [PubMed] [Google Scholar]
- 28.Tsingos C, Bosnic-Anticevich S, Smith L. Does a learning style preference for processing information through reflection impact on the academic performance of a cohort of undergraduate pharmacy students? Pharm Educ. 2015;15(1):233-240. [Google Scholar]
- 29.McKenna L, Copnell B, Butler AE, et al. Learning style preferences of Australian accelerated postgraduate pre-registration nursing students: A cross-sectional survey. Nurs Educ Pract. 2018;28:280-284. [DOI] [PubMed] [Google Scholar]
- 30.Mitchell EKL, James S, D’Amore A. How learning styles and preferences of first-year nursing and midwifery students change. Aust J Educ. 2015;59(2):158-168. [Google Scholar]
- 31.Bhalli MA, Khan IA, Sattar A. Learning style of medical students and its correlation with preferred teaching methodologies and academic achievement. J Ayub Med Coll Abbottabad. 2015;27(4):837-842. [PubMed] [Google Scholar]
- 32.Sharif S, Gifford LA, Morris GA, et al. The relationship between learning styles, attendance, and academic performance of pharmacy undergraduates. Pharm Educ. 2010;10(2):138-143. [Google Scholar]
- 33.O’Mahony SM, Sbayeh A, Horgan M, et al. Association between learning style preferences and anatomy assessment outcomes in graduate-entry and undergraduate medical students. Anat Sci Educ. 2016;9:391-399. [DOI] [PubMed] [Google Scholar]
- 34.Crawford SY, Alhreish SK, Popovich NG. Comparison of learning styles of pharmacy students and faculty members. Am J Pharm Educ. 2012;76(10):Article 192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hallin K. Nursing students at a university - a study about learning style preferences. Nurse Educ Today. 2014;34:1443-1449. [DOI] [PubMed] [Google Scholar]
- 36.Didau D. One more nail in the learning styles coffin. https://learningspy.co.uk/myths/whats-the-difference-between-modalities-and-learning-styles/. Accessed July 6, 2020. [Google Scholar]
- 37.Education Endowment Foundation. Learning styles. https://educationendowmentfoundation.org.uk/evidence-summaries/teaching-learning-toolkit/learning-styles#closeSignup. Accessed July 6, 2020.
- 38.Kirschner PA. Stop propagating the learning styles myth. Comput Educ. 2017;106:166-171. [Google Scholar]
- 39.Multiple Intelligences Oasis. A beginner’s guide to the theory of multiple intelligences. https://www.multipleintelligencesoasis.org/a-beginners-guide-to-mi. Accessed July 6, 2020. [Google Scholar]
- 40.American Institute for Learning and Human Development. Multiple intelligences. https://www.institute4learning.com/resources/articles/multiple-intelligences/. Accessed July 6, 2020.
- 41.Almigbal TH. Relationship between the learning style preferences of medical students and academic achievement. Saudi Med J. 2015;36(3):349-355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nuzhat A, Salem RO, Al Hamdan N, et al. Gender differences in learning styles and academic performance of medical students in Saudi Arabia. Med Teach. 2013;35(S1):S78-S82. [DOI] [PubMed] [Google Scholar]
- 43.Prithishkumar IJ, Michael SA. Understanding your student: Using the VARK model. J Postgrad Med. 2014;60(2):183-186. [DOI] [PubMed] [Google Scholar]
- 44.Rahman SMN, Alam T, Alam NN, et al. Medical undergraduates preference in learning style: a single-institute experience from Bangladesh. Kuwait Med J. 2017;49(1):12-16. [Google Scholar]
- 45.Taha M, Gulfishan D, Khalid H. Assessment of learning styles of undergraduate medical students using VARK questionnaire and the influence of sex and academic performance. Indo Am J P Sci. 2018;9(5):9351-9361. [Google Scholar]
- 46.Preece RA, Cope AC. Are surgeons born or made? A comparison of personality traits and learning styles between surgical trainees and medical students. J Surg Educ. 2016;73(5):768-773. [DOI] [PubMed] [Google Scholar]
- 47.Alkhasawneh E. Using VARK to assess changes in learning preferences of nursing students at a public university in Jordan: Implications for teaching. Nurse Educ Today. 2013;33:1546-1549. [DOI] [PubMed] [Google Scholar]
- 48.Abbott MRB, Shaw P. Multiple modalities for APA instruction: addressing diverse learning styles. Teach Learn Nurs. 2018;13:63-65. [Google Scholar]
- 49.Buchanan P. The association between learning preferences and preferred methods of assessment of dental students [dissertation]. Stockton, CA: University of the Pacific; 2016. [Google Scholar]
- 50.Nazir MA, Al-Ansari A, Farooqi FA. Influence of gender, class year, academic performance, and paternal socioeconomic status on learning style preferences among dental students. J Clin Diagn Res. 2018;12(6):ZC04-ZC08. [Google Scholar]
- 51.Saleem F, Hassali MA, Ibrahim ZS, et al. Learning styles of pharmacy undergraduates: Experience from a Malaysian University. Pharm Educ. 2015;15(1):173-177. [Google Scholar]