

Abstract
Aims
A reduction of habitual physical activity due to prolonged COVID‐19 quarantine can have serious consequences for patients with cardiovascular diseases, such as heart failure. This study aimed to explore the effect of COVID‐19 nationwide quarantine on accelerometer‐assessed physical activity of heart failure patients.
Methods and results
We analysed the daily number of steps in 26 heart failure patients during a 6‐week period that included 3 weeks immediately preceding the onset of the quarantine and the first 3 weeks of the quarantine. The daily number of steps was assessed using a wrist‐worn accelerometer worn by the patients as part of an ongoing randomized controlled trial. Multilevel modelling was used to explore the effect of the quarantine on the daily step count adjusted for weather conditions. As compared with the 3 weeks before the onset of the quarantine, the step count was significantly lower during each of the first 3 weeks of the quarantine (P < 0.05). When the daily step count was averaged across the 3 weeks before and during the quarantine, the decrease amounted to 1134 (SE 189) steps per day (P < 0.001), which translated to a 16.2% decrease.
Conclusions
The introduction of the nationwide quarantine due to COVID‐19 had a detrimental effect on the level of habitual physical activity in heart failure patients, leading to an abrupt decrease of daily step count that lasted for at least the 3‐week study period. Staying active and maintaining sufficient levels of physical activity during the COVID‐19 pandemic are essential despite the unfavourable circumstances of quarantine.
Keywords: COVID‐19, Physical activity, Accelerometer, Heart failure, Quarantine, Lockdown
Background
In a reaction to the COVID‐19 pandemic, a large number of governments worldwide have imposed nationwide quarantine to contain the spread of the virus. In the Czech Republic, the first case of COVID‐19 was reported on 1 March 2020, and since 16 March, the Czech government approved a nationwide quarantine that prohibited movement in public spaces except under special circumstances, which included travelling to and from work and necessary journeys to procure food and supplies; notably, going outside for a walk in a park or the countryside was allowed. These measures are crucial to disperse the pressure on healthcare systems and limit the number of deaths. 1 Still, they inflict substantial collateral damage, such as economic slowdown and deleterious effects on mental health and psychological well‐being. 2 A reduction of habitual physical activity (PA) is another potentially harmful effect of prolonged quarantine 3 that can have serious consequences for cardiometabolic morbidity and mortality in both healthy individuals 4 and patients with cardiovascular diseases, 5 such as heart failure (HF).
Aims
This study aimed to explore the effect of a nationwide quarantine on accelerometer‐assessed habitual PA of HF patients.
Methods
We analysed the daily number of steps in HF patients during a 6‐week period that included 3 weeks immediately preceding the onset of the quarantine (24 February to 15 March 2020) and the first 3 weeks of the quarantine (16 March to 5 April 2020). These patients were participants of an ongoing multicentre randomized controlled trial of a 6‐month intervention in the form of an unsupervised, individual, outside walking programme that combined weekly step goals, self‐monitoring, and regular phone‐based counselling, followed by a 6‐month follow‐up period. 6 As part of the intervention, the patients were requested to wear a wrist‐worn accelerometer, and they were recommended to continue wearing it during the follow‐up period and beyond. All patients, those still participating in the intervention and those in the follow‐up phase and beyond, were included in this study, provided their accelerometer data were available.
The wrist‐worn accelerometer, Garmin vívofit, has been validated for measuring steps in the HF population 7 and enables sharing step data in 15‐min epochs online. Non‐wear time was identified as bouts of ≥60 consecutive minutes with zero steps, and only days with at least 10 h of wear time were deemed valid and included in the analysis. 8 Only patients with at least four valid days, including one weekend day, in both 3‐week periods before and during the quarantine were included in the analysis.
Patient characteristics (Table 1 ) were taken from the most recent assessment conducted as part of the randomized trial. The number of days elapsed from enrolment into the trial and whether the patient was in the intervention or follow‐up phase was also recorded. Additionally, following the 6‐week period, the patients were contacted by phone and asked a series of questions about their life circumstances that could moderate the impact of quarantine on their habitual PA, such as the size of their residential town, distance to the countryside, household size and composition, and employment circumstances. The answers were dichotomized for further analysis (Table 2 ). Furthermore, the weather conditions that substantially impact daily PA (maximum daily temperature and daily hours of sunshine) 9 were downloaded from publicly available webpages (https://www.in-pocasi.cz/archiv/) of the meteorological stations nearest to the place of living of each patient for each of the analysed days.
TABLE 1.
Patient characteristics
| n = 26 | |
|---|---|
| Age (years) | 58.8 (9.8) |
| Female/male (n) | 8/18 |
| HFpEF/HFrEF (n) | 7/19 |
| NYHA II/NYHA III (n) | 23/3 |
| Body mass index (kg/m2) | 31.5 (5.4) |
| Left ventricular ejection fraction (%) | 37.2 (12.1) |
| 6‐min walk test (m) | 391 (70) |
| NT‐proBNP (pg/mL) | 778 (726) |
| Beck Depression Inventory‐II score (points) | 6.1 (3.7) |
| General Self‐Efficacy Scale (points) | 31.6 (5.7) |
| Days elapsed since randomization into the trial | 219 (137) |
| Intervention/follow‐up phase of the trial (n) | 12/14 |
HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; NYHA, New York Heart Association; NT‐proBNP, N‐terminal pro‐brain natriuretic peptide.
Data are presented as mean (standard deviation) or n (number of patients).
TABLE 2.
Patient life circumstances
| Circumstance A vs. B | A | B |
|---|---|---|
| Living in a city with more vs. less than 10 000 inhabitants | 8 | 18 |
| Living in a flat vs. house with garden | 8 | 18 |
| Walking distance to countryside: less vs. more than 10 min | 15 | 11 |
| Number of adults living with the patient in one household: none or one vs. two or more | 17 | 9 |
| Living with kids up to 15 years in one household: yes vs. no | 5 | 21 |
| Having a dog that requires walking outside: yes vs. no | 11 | 15 |
| Employed vs. not employed | 9 | 17 |
Data are presented as number of patients living under Circumstance A vs. B.
To examine the effect of the quarantine on daily PA, we conducted a series of linear mixed‐effects models. Firstly, we modelled the daily number of steps as a function of the week number (1–6). Secondly, we modelled the daily number of steps as a function of the presence or absence of the quarantine. Weather conditions entered both models as fixed effects, and the day of the week nested within the subject entered the models as random effects. Thirdly, we used the model to calculate a percentage change in the daily number of steps following the onset of the quarantine for individual patients. The percentage change was then used as the dependent variable in a full linear model that included all potential covariates from among the patients' characteristics and their life circumstances as fixed effects. The covariates that did not demonstrate significant associations (P < 0.05) with the percentage change were eliminated from the full model one by one, and only those with significant associations were included in the final model, and their P‐values were reported.
The study protocol was approved by the Ethics Committee of the General University Hospital, Prague (20/16 Grant VES 2017 AZV VFN), and the study was conducted according to the principles of the Declaration of Helsinki. The patients signed an informed consent document to participate in the study.
Results
Thirty‐two trial participants wore the accelerometer and shared their data online during the analysed 6‐week period. Of those, 26 patients from five study centres had enough valid days (mean 34 ± 9) and were included in the analysis; their characteristics are listed in Table 1 . As compared with the 3 weeks before the onset of the quarantine, their step count was significantly lower during each of the first 3 weeks of the quarantine (Figure 1 ). When the daily step count was averaged across the 3 weeks before and during the quarantine, the decrease amounted to 1134 (SE 189) steps per day (P < 0.001), which translated to a 16.2% decrease. Of various patients' characteristics and life circumstances, living in a flat rather than in a house (P = 0.014) and living in a household with at least two other adult persons (P = 0.041) worsened the deleterious effect of quarantine on daily step count.
FIGURE 1.
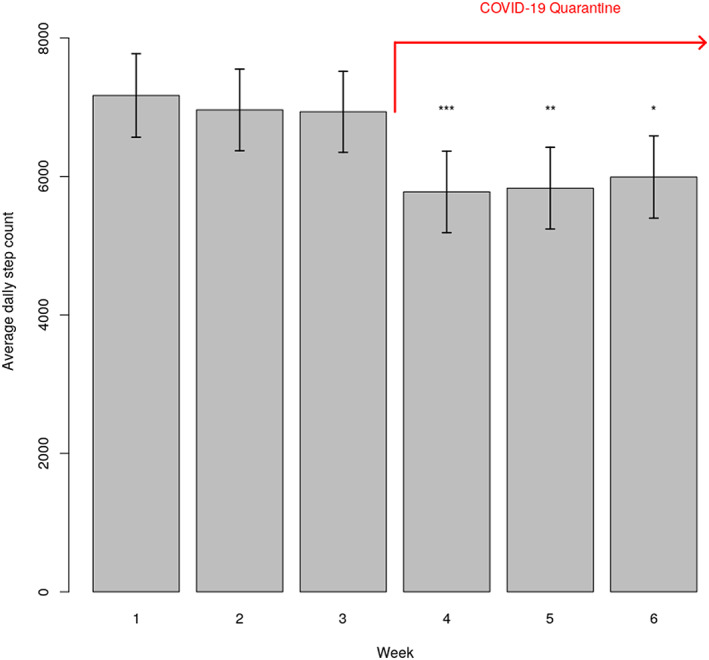
Average daily step count (± standard error) during 3 weeks preceding the onset of the quarantine (Weeks 1–3) and the first 3 weeks during the quarantine (Weeks 4–6). *** P < 0.001 for comparison with Weeks 1–3; ** P < 0.001 for comparison with Week 1 and P < 0.01 for comparison with Weeks 2 and 3; and * P < 0.01 for comparison with Weeks 1 and 2 and P < 0.05 for comparison with Week 3.
Discussion
Our study found that immediately after the onset of the quarantine, HF patients abruptly decreased their habitual PA by over 1100 steps (16.2%) per day and maintained this reduced level for at least 3 weeks into the quarantine. Even though we did not assess patients' fitness before and after this 3‐week period, other studies suggest that such a decrease in PA leads to a substantial deterioration of physical fitness, 10 which is an important predictor of HF morbidity and mortality. 11 Furthermore, even after the end of the quarantine, we cannot be sure that patients' PA would return to their pre‐quarantine levels because not engaging in regular PA could easily become a new habit after 3 weeks of inactivity. 12 Thus, the detrimental effect of quarantine on PA can potentially result in a longer‐term worsening of patients' health status and prognosis.
Our finding of a 16% decrease in step count fits well with the large‐scale analysis of Fitbit users in the Czech Republic who decreased their daily step count in the first week following the onset of the quarantine by 20% compared with the same time of the previous year. 13 The Fitbit analysis also demonstrated the variability of the step count decreases among countries with different levels of lockdown measures. 13 As such, our finding can only be generalized to the countries with similar levels of restrictions on outside activities, such as the UK, Germany, or Poland, where outside activities were allowed albeit limited to the people from the same household. However, in countries where outside activities were strictly limited to performing them in isolation near the home (e.g. Italy and France), or where outdoor activities were outright banned (Spain), the impact of the quarantine on the PA of HF patients would likely be much more detrimental.
The impact of quarantine on PA was moderated by some of the patients' life circumstances. Specifically, those patients living in a flat were affected more than those living in a house. However, we do not know if this finding was due to more opportunities to perform PA within a house that usually has a larger floor area and an adjacent garden or due to a more favourable urban environment surrounding a house. Furthermore, those living with at least two other adults were more affected than those living alone or with just one other adult. One possible explanation might be that larger households shared the necessary errands and other duties requiring PA among more persons. Moreover, patients with HF might have been perceived as especially vulnerable by their family members who took over their share of duties.
The patients included in our study were participants in an intervention arm of a randomized controlled trial of a 6‐month walking intervention. 6 Running this trial at the time of the COVID‐19 pandemic has given us a unique opportunity to compare accelerometer‐assessed PA of HF patients for relatively long periods immediately before and during the early stages of quarantine, which would otherwise not be possible. Indeed, objectively assessing PA using accelerometers has been demonstrated to be superior to subjective assessments using questionnaires that are prone to recall bias. 14 Yet another strength of our study is that we adjusted the daily step count for weather conditions, specifically for maximum daily temperature and daily hours of sunshine, 9 thus avoiding bias due to weather and seasonal variations throughout the studied period.
As the patients were already wearing the accelerometers well before the analysed period, we avoided the common pitfall of PA studies when participants react to the fact that they are being monitored by temporarily increasing their habitual PA. 15 On the other hand, such a design has its limitations as the enrolment in the trial may influence the effect of the quarantine on patients' PA, due to the selection of motivated individuals and to the nature of the intervention. Indeed, the mean daily step count of the patients before the onset of the quarantine was higher than the step count usually observed in other studies focusing on HF populations. 8 , 16 However, when we entered the daily step count, the time elapsed since enrolment into the trial, and whether the patient was in the intervention or follow‐up phase of the trial as covariates into the model, neither of them had a significant effect on the percentage change, suggesting that our results can possibly be generalized to the HF populations outside a trial setting.
In conclusion, the introduction of the nationwide quarantine due to COVID‐19 had a detrimental effect on the level of habitual PA in HF patients, leading to an abrupt 16% decrease of daily step count that lasted for at least the 3‐week study period. Such a reduction in PA can lead to a deterioration of physical fitness and potentially result in a long‐term worsening of patients' health status and prognosis. Thus, staying active and maintaining sufficient levels of PA during the COVID‐19 pandemic, for example, by participating in home‐based PA programmes, 17 are essential despite the unfavourable circumstances of quarantine.
Conflict of interest
None declared.
Funding
This work was supported by the Czech Health Research Council (Agentura Pro Zdravotnický Výzkum České Republiky) of the Ministry of Health of the Czech Republic (Grant Number NV18‐09‐00146).
Vetrovsky, T. , Frybova, T. , Gant, I. , Semerad, M. , Cimler, R. , Bunc, V. , Siranec, M. , Miklikova, M. , Vesely, J. , Griva, M. , Precek, J. , Pelouch, R. , Parenica, J. , and Belohlavek, J. (2020) The detrimental effect of COVID‐19 nationwide quarantine on accelerometer‐assessed physical activity of heart failure patients. ESC Heart Failure, 7: 2093–2097. 10.1002/ehf2.12916.
References
- 1. Lancet T. COVID‐19: too little, too late? Lancet 2020; 395: 755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 2020; 395: 912–920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Qin F, Song Y, Nassis GP, Zhao L, Cui S, Lai L, Wu Z, Xu M, Qu C, Dong Y, Wang Z, Geng X, Zhao C, Feng Y, Han Z, Fan Z, Zhao J. Prevalence of insufficient physical activity, sedentary screen time and emotional well‐being during the early days of the 2019 novel coronavirus (COVID‐19) outbreak in China: a national cross‐sectional study. Ssrn Electron J 2020. [Google Scholar]
- 4. Chen P, Mao L, Nassis GP, Harmer P, Ainsworth BE, Li F. Coronavirus disease (COVID‐19): the need to maintain regular physical activity while taking precautions. J Sport Health Sci 2020; 9: 103–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Lippi G, Henry BM, Sanchis‐Gomar F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID‐19). Eur J Prev Cardiol 202027 9:906–908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Vetrovsky T, Siranec M, Parenica J, Griva M, Stastny J, Precek J, Pelouch R, Bunc V, Linhart A, Belohlavek J. Effect of a 6‐month pedometer‐based walking intervention on functional capacity in patients with chronic heart failure with reduced (HFrEF) and with preserved (HFpEF) ejection fraction: study protocol for two multicenter randomized controlled trials. J Transl Med 2017; 15: 153–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Vetrovsky T, Siranec M, Marencakova J, Tufano JJ, Capek V, Bunc V, Belohlavek J. Validity of six consumer‐level activity monitors for measuring steps in patients with chronic heart failure. Plos One 2019; 14: e0222569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Vetrovsky T, Clark CCT, Bisi MC, Siranec M, Linhart A, Tufano JJ, Duncan MJ, Belohlavek J. Advances in accelerometry for cardiovascular patients: a systematic review with practical recommendations. ESC Heart Failure 2020 10.1002/ehf2.12781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Klenk J, Büchele G, Rapp K, Franke S, Peter R. Walking on sunshine: effect of weather conditions on physical activity in older people. J Epidemiol Commun H 2012; 66: 474–476. [DOI] [PubMed] [Google Scholar]
- 10. Toraman NF, Ayceman N, Yaman H. Effects of six weeks of detraining on retention of functional fitness of old people after nine weeks of multicomponent training. Brit J Sport Med 2005; 39: 565–568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Bittner V, Weiner DH, Yusuf S, Rogers WJ, McIntyre KM, Bangdiwala SI, Kronenberg MW, Kostis JB, Kohn RM, Guillotte M. Prediction of mortality and morbidity with a 6‐minute walk test in patients with left ventricular dysfunction. SOLVD Investigators JAMA 1993; 270: 1702–1707. [PubMed] [Google Scholar]
- 12. Aarts H, Paulussen T, Schaalma H. Physical exercise habit: on the conceptualization and formation of habitual health behaviours. Health Educ Res 1997; 12: 363–374. [DOI] [PubMed] [Google Scholar]
- 13. Fitbit . The impact of coronavirus on global activity. 2020. [updated 2020‐03‐23;2020‐05‐26]. https://blog.fitbit.com/covid-19-global-activity/ [accessed on 23 June 2020]
- 14. Limb ES, Ahmad S, Cook DG, Kerry SM, Ekelund U, Whincup PH, Victor CR, Iliffe S, Ussher M, Fox‐Rushby J, Furness C, Ibison J, DeWilde S, Harris T. Measuring change in trials of physical activity interventions: a comparison of self‐report questionnaire and accelerometry within the PACE‐UP trial. Int J Behav Nutr Phy 2019; 16: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Clemes SA, Matchett N, Wane SL. Reactivity: an issue for short‐term pedometer studies? Brit J Sport Med. 2008; 42: 68. [DOI] [PubMed] [Google Scholar]
- 16. Baril J‐F, Bromberg S, Moayedi Y, Taati B, Manlhiot C, Ross HJ, Cafazzo J. Use of free‐living step count monitoring for heart failure functional classification: validation study. JMIR Cardio 2019; 3: e12122–e12115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Dalal HM, Taylor RS, Jolly K, Davis RC, Doherty P, Miles J, van Lingen R, Warren FC, Green C, Wingham J, Greaves C, Sadler S, Hillsdon M, Abraham C, Britten N, Frost J, Singh S, Hayward C, Eyre V, Paul K, Lang CC, Smith K. The effects and costs of home‐based rehabilitation for heart failure with reduced ejection fraction: the REACH‐HF multicentre randomized controlled trial. Eur J Prev Cardiol 2019; 26: 262–272. [DOI] [PMC free article] [PubMed] [Google Scholar]