

This cohort substudy investigates whether the addition of high-sensitivity troponin level to guideline-derived atherosclerotic cardiovascular disease risk can improve risk classification and downstream treatment recommendations.
Key Points
Question
Can high-sensitivity troponin complement the American Heart Association/American College of Cardiology cholesterol management guidelines to improve atherosclerotic cardiovascular disease (ASCVD) risk classification?
Findings
Among 8635 patients in this cohort substudy, patients with lower-risk ASCVD and a high-sensitivity troponin I level exceeding 6 ng/L had the same rate of cardiovascular events as patients classified as having very high-risk ASCVD. Analogously, patients with very high-risk ASCVD and undetectable high-sensitivity troponin I level had event rates similar to those of patients classified as having lower-risk ASCVD.
Meaning
The findings of this cohort substudy suggest that incorporation of high-sensitivity troponin into a guideline-derived ASCVD risk algorithm provides enhanced risk stratification and reclassifies patients to ensure that risk-appropriate medical therapy is offered.
Abstract
Importance
The 2018 American Heart Association/American College of Cardiology (AHA/ACC) cholesterol management guidelines identified 2 distinct groups of patients with atherosclerotic cardiovascular disease (ASCVD) prompting different treatment recommendations.
Objective
To investigate whether the addition of high-sensitivity troponin (hsTn) testing to guideline-derived ASCVD risk can improve risk classification and downstream treatment recommendations.
Design, Setting, and Participants
A prospective cohort biomarker substudy was performed that included 8635 patients enrolled in the Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54) trial. Patients were assigned to risk groups of either very high-risk ASCVD or lower-risk ASCVD based on their cardiovascular history and comorbidities, in line with the 2018 AHA/ACC cholesterol management guidelines criteria. Patients were also classified on the basis of hsTnI level (ARCHITECT assay; Abbott) using cut points of 2 ng/L (limit of detection) and 6 ng/L (risk threshold), followed by joint classification on the basis of clinical features and hsTnI level. The setting was a nested prospective cohort study in a completed multinational trial. Participants were all patients who had a myocardial infarction 1 to 3 years before enrollment, were at least 50 years of age, and had at least 1 high-risk feature. The study dates were October 2010 to December 2014. The dates of analysis were June 2019 to January 2020.
Main Outcomes and Measures
The primary end point was a composite of cardiovascular death, myocardial infarction, or stroke.
Results
Among 8635 patients enrolled in the PEGASUS-TIMI 54 trial, the median age was 65 years (interquartile range, 58-71 years), and 6614 (76.6%) were men; 8340 (96.6%) were White individuals and 176 (2.0%) were Black individuals. Patients meeting clinical criteria for the very high-risk ASCVD group had a primary end point 3-year event rate of 8.8% compared with 5.0% in the lower-risk ASCVD group (hazard ratio, 2.01; 95% CI, 1.58-2.57; P < .001). When patients in the very high-risk ASCVD group were further risk stratified by hsTnI level, 614 of 6789 patients (9.0%) with an undetectable hsTnI level had a 3-year event rate of 2.7% (<1% per year), which was less than the overall rate in the lower-risk ASCVD group. Analogously, in the lower-risk ASCVD group, 417 of 1846 patients (22.6%) with an hsTnI level exceeding 6 ng/L had an event rate of 9.1%, comparable to the overall rate in the very high-risk ASCVD group. The addition of hsTnI to guideline-derived ASCVD risk led to a net reclassification index at event rate of 0.15 (95% CI, 0.10-0.21). Overall, use of hsTnI reclassified 1031 of 8635 patients (11.9%) (1 in 11 with very high-risk ASCVD and 1 in 4 with lower-risk ASCVD).
Conclusions and Relevance
The findings of this cohort substudy suggest that a strategy incorporating hsTn into a guideline-derived ASCVD risk algorithm provides enhanced risk stratification and reclassifies 11.9% of patients into a more appropriate risk group. This application of hsTn testing might be used to optimize the care of patients with ASCVD.
Introduction
High-sensitivity troponin (hsTn) has demonstrated a strong association with recurrent events in patients with stable atherosclerotic cardiovascular disease (ASCVD),1,2,3,4,5,6,7 yet it is still not routinely being used in clinical practice in this population. A recent study8 in patients with hypertension suggests that hsTnI could be used to refine risk categorization and better identify who should receive antihypertensive therapies. Decisions about cholesterol management may be another opportunity to incorporate hsTnI testing into clinical risk algorithms that inform downstream treatment recommendations.
The 2018 American Heart Association/American College of Cardiology (AHA/ACC) cholesterol management guidelines9 identified 2 distinct groups of patients with ASCVD. The first is a very high-risk group classified by the presence of 2 or more major cardiovascular (CV) events or 1 major event with multiple high-risk conditions. The second group includes the remainder of patients with ASCVD, designated in the cholesterol management guidelines as not at very high risk, who have established atherosclerotic disease but do not meet the 2018 AHA/ACC guidelines criteria for very high risk and are hereafter referred to as lower risk. Based on this clinical risk stratification, the recommendations for the 2 groups differ in 3 important ways. First, patients in the very high-risk ASCVD group are to be treated with high-intensity statin independent of age, as opposed to the lower-risk ASCVD group, in which statin therapy is a class I recommendation only for patients 75 years or younger. Second, ezetimibe is a class IIa recommendation in very high-risk ASCVD and only a class IIb recommendation in lower-risk ASCVD. Third, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors are recommended as class IIa for patients in the very high-risk ASCVD group with low-density lipoprotein cholesterol (LDL-C) levels of 70 mg/dL or higher but are not recommended for the lower-risk ASCVD group (to convert cholesterol level to millimoles per liter, multiply by 0.0259).
The clinical distinctions made in the AHA/ACC cholesterol management guidelines9 are a step toward a more personalized approach to treating most patients with ASCVD. However, inherent to the success of such a strategy is the robustness of risk stratification. The present study investigated whether the addition of hsTn to guideline-derived ASCVD risk can improve risk classification and guide downstream treatment recommendations.
Methods
Study Population
A prospective cohort biomarker substudy was performed that included 8635 patients enrolled in the Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54) trial.10 PEGASUS-TIMI 54 was a multinational randomized trial comparing ticagrelor with placebo in patients with prior myocardial infarction (MI). The study design and results of the trial have previously been published.10 The present exploratory analysis uses data from the prospective cohort biomarker substudy to evaluate hsTnI level for risk evaluation within the framework of the 2018 AHA/ACC cholesterol management guidelines.9 The analysis includes all consenting patients with available blood samples in the prospective cohort biomarker substudy. Data from this analysis will not be made publicly available. Informed consent was obtained from all participating individuals. The trial protocol was reviewed and approved by the institutional review board or ethics committee at each participating center.
For this analysis, patients were assigned to guideline-derived risk groups of either very high-risk ASCVD or a lower-risk ASCVD based on their CV history and comorbidities, in line with the 2018 AHA/ACC cholesterol management guidelines9 criteria. Patients were also classified on the basis of hsTnI level (ARCHITECT assay; Abbott) using cut points of 2 ng/L (limit of detection) and 6 ng/L (risk threshold) and joint classification on the basis of clinical features and hsTnI level. The setting was a nested prospective cohort study in a completed multinational trial. Participants were all patients who had an MI 1 to 3 years before enrollment, were at least 50 years of age, and had at least 1 high-risk feature. The study dates were October 2010 to December 2014. The dates of analysis were June 2019 to January 2020.
To qualify for the very high-risk ASCVD group, patients had to have either (1) at least 2 prior major CV events (acute coronary syndrome within the past 12 months, history of MI before the preceding 12 months, history of ischemic stroke, or peripheral vascular disease, as defined by revascularization, amputation, or claudication, with documented ankle-brachial index <0.90) or (2) a single prior major event plus multiple high-risk conditions (age ≥65 years, prior coronary revascularization, diabetes, hypertension, current smoking, apolipoprotein B [apoB] level ≥90 mg/dL [to convert apoB level to grams per liter, multiply by 0.01] despite statin therapy, prior congestive heart failure, or chronic kidney disease [estimated glomerular filtration rate <60 mL/min/1.73 m2]). The apoB level was used as a surrogate for LDL-C level because it was the atherogenic lipoprotein measurement available in the PEGASUS-TIMI 54 trial.10 The threshold of 90 mg/dL for apoB level approximates 100 mg/dL for LDL-C level.11,12 The remainder of patients qualified for the lower-risk ASCVD group because of their established atherosclerosis as evident by a prior MI.
Troponin Assay
Patients had baseline blood samples collected at the time of study enrollment. Cardiac troponin I level was measured centrally (at the TIMI Clinical Trials Laboratory, Boston, Massachusetts) using a now clinically available, high-sensitivity assay (ARCHITECT assay; Abbott), which has a limit of detection of 2 ng/L, and previous studies13,14,15,16,17,18 have demonstrated thresholds of risk in the range of 5 to 7 ng/L. Therefore, we categorized patients into the following 3 a priori groups for risk stratification based on hsTnI results: undetectable (<2 ng/L), low (2-6 ng/L), and high (>6 ng/L). These values chosen for risk stratification in this cohort of stable patients are well below the 99th percentile upper reference limit of 26 ng/L19 (34 ng/L in men and 16 ng/L in women) recommended for the diagnosis of acute MI.20 The coefficient of variation at the 99th percentile of the assay is 5.6%.20
End Points
The prespecified primary end point of the trial was a composite of CV death, MI, or stroke. Secondary end points included the individual components of the primary outcome, as well as death from coronary heart disease and death from any cause. Patients were followed up for a median of 33 months (interquartile range, 27-38 months). All CV end points were adjudicated by a central clinical events committee that was blinded to treatment assignment and baseline hsTnI level.
Statistical Analysis
Baseline characteristics stratified by guideline-derived ASCVD risk group and by hsTnI level are listed in the Table. Continuous variables within each group are presented as median and interquartile range and compared using the Wilcoxon rank sum test. Categorical variables between ASCVD risk groups were compared using the χ2 test. Continuous variables were analyzed by analysis of variance with P for linear trend, and categorical variables were analyzed using the Cochran-Armitage test for trend. Three-year event rates were estimated using the Kaplan-Meier method. Hazard ratios (HRs) and 95% CIs were generated using a Cox proportional hazards regression model. Adjusted regression models for the association of hsTnI level with clinical outcomes included age, sex, history of peripheral artery disease, diabetes, hypertension, smoking, apoB level, prior congestive heart failure, estimated glomerular filtration rate, stroke, and coronary artery bypass graft. The net reclassification index at event rate21 and integrated discrimination improvement index22 were calculated in models with guideline-derived ASCVD only and with hsTnI level added. To evaluate the incremental value of hsTnI level beyond guideline-derived ASCVD risk, the likelihood ratio test was used.23 All reported P values are 2 sided at a statistical significance level of .05. All analyses were performed with SAS software (version 9.4; SAS Institute Inc).
Table. Baseline Characteristics by Guideline-Derived ASCVD Risk Group and hsTnI Levela.
| Variable | ASCVD risk group, No./total No. (%) | hsTnI level, No./total No. (%) | ||||
|---|---|---|---|---|---|---|
| Lower-risk ASCVD (n = 1846) | Very high-risk ASCVD (n = 6789) | <2 ng/L (n = 920) | 2-6 ng/L (n = 5028) | >6 ng/L (n = 2687) | P value | |
| Demographics | ||||||
| Age, median (IQR), y | 60 (55-64) | 67 (60-72) | 61 (55-66) | 65 (58-70) | 67 (60-73) | <.001 |
| Age ≥65 y | 397 (21.5) | 4186 (61.7) | 337 (36.6) | 2658 (52.9) | 1588 (59.1) | <.001 |
| Female | 232 (12.6) | 1789 (26.4) | 330 (35.9) | 1137 (22.6) | 554 (20.6) | <.001 |
| Medical history | ||||||
| Prior MI | 1846 (100) | 6789 (100) | 920 (100) | 5028 (100) | 2687 (100) | NA |
| History of peripheral artery disease | 24 (1.3) | 540 (8.0) | 29 (3.2) | 296 (5.9) | 239 (8.9) | <.001 |
| Prior coronary revascularization | 1753 (95.0) | 6346/6788 (93.5) | 877 (95.3) | 4720/5027 (93.9) | 2502 (93.1) | .02 |
| Diabetes | 87 (4.7) | 2489 (36.7) | 269 (29.2) | 1391 (27.7) | 916 (34.1) | <.001 |
| Hypertension | 752 (40.7) | 6012 (88.6) | 644 (70.0) | 3905 (77.7) | 2215 (82.4) | <.001 |
| Current smoker | 99/1845 (5.4) | 1506/6788 (22.2) | 220/919 (23.9) | 945 (18.8) | 440/2686 (16.4) | <.001 |
| apoB level ≥90 mg/dL despite statin therapy | 115/1803 (6.4) | 1893/6668 (28.4) | 212/902 (23.5) | 1181/4929 (24.0) | 615/2640 (23.3) | .71 |
| Prior congestive heart failure | 32 (1.7) | 1300 (19.1) | 63 (6.8) | 610 (12.1) | 659 (24.5) | <.001 |
| Laboratory values | ||||||
| Estimated glomerular filtration rate <60 mL/min/1.73 m2 | 23/1828 (1.3) | 1973/6736 (29.3) | 105/909 (11.6) | 1007/4985 (20.2) | 884/2670 (33.1) | <.001 |
| hsTnI level, median (IQR), ng/L | 4 (2-6) | 4 (3-8) | <2b | 4 (3-5) | 10 (8-17) | NA |
Abbreviations: apoB, apolipoprotein B; ASCVD, atherosclerotic cardiovascular disease; hsTnI, high-sensitivity troponin I; IQR, interquartile range; MI, myocardial infarction; NA, not applicable.
SI conversion factor: To convert apoB level to grams per liter, multiply by 0.01.
The hsTnI levels for 8340 White individuals (1795 lower-risk ASCVD and 6545 very high-risk ASCVD) were less than 2 ng/L in 892 individuals (97.0%), 2 to 6 ng/L in 4877 individuals (97.0%), and greater than 6 ng/L in 2571 individuals (95.7%) (P = .008). The hsTnI levels for 176 Black individuals (26 lower-risk ASCVD and 150 very high-risk ASCVD) were less than 2 ng/L in 11 individuals (1.2%), 2 to 6 ng/L in 91 individuals (1.8%), and greater than 6 ng/L in 74 individuals (2.8%) (P = .001).
Presented without IQR because values less than 2 ng/L are below the level of detection for the assay.
Results
Patients
Of the 8635 patients in this biomarker substudy (eTable 1 in the Supplement), the median age was 65 years (interquartile range, 58-71 years), and 6614 (76.6%) were men; 8340 (96.6%) were White individuals and 176 (2.0%) were Black individuals. Based on clinical criteria, 6789 patients (78.6%) were in the very high-risk ASCVD group, with most (6342 of 6789 [93.4%]) qualifying based on 1 major event and multiple high-risk conditions and fewer (447 of 6789 [6.6%]) qualifying with at least 2 major adverse events. The remaining 1846 patients (21.4%) were in the lower-risk ASCVD group, in which all patients had 1 major event, 1511 had 1 additional high-risk feature, and 335 had none. Overall, 8199 of 8635 patients (95.0%) were receiving statin therapy. Baseline characteristics for the 2 ASCVD groups are listed in the Table.
The median hsTnI level was 4 ng/L (interquartile range, 3-7 ng/L). Overall, 7715 of 8635 patients (89.3%) had a detectable hsTnI level (≥2 ng/L). Of those with a detectable hsTnI level, 5028 of 7715 (65.2%) had levels between 2 and 6 ng/L, and 2687 of 7715 (34.8%) had levels exceeding 6 ng/L. Patients with baseline hsTnI level exceeding 6 ng/L were more likely to be older, to be male, and to have comorbidities, including prior coronary revascularization, diabetes, hypertension, prior congestive heart failure, and chronic kidney disease (Table).
Very High-Risk ASCVD vs Lower-Risk ASCVD
Of the 8635 patients in this analysis, 610 (7.1%) experienced a primary end point event (CV death, MI, or stroke). Patients meeting clinical criteria for the very high-risk ASCVD group had a statistically significantly higher rate of CV death, MI, or stroke, with a 3-year Kaplan-Meier event rate of 8.8% compared with 5.0% in the lower-risk ASCVD group (HR, 2.01; 95% CI, 1.58-2.57; P < .001) (Figure 1A). Statistically significant differences were also seen for each of the individual components, including CV death, MI, or stroke (eTable 2A in the Supplement).
Figure 1. Kaplan-Meier Rates for the Primary End Point (a Composite of Cardiovascular [CV] Death, Myocardial Infarction [MI], or Stroke) by Guideline-Derived Atherosclerotic Cardiovascular Disease (ASCVD) Risk Group and High-Sensitivity Troponin I (hsTnI) Level.
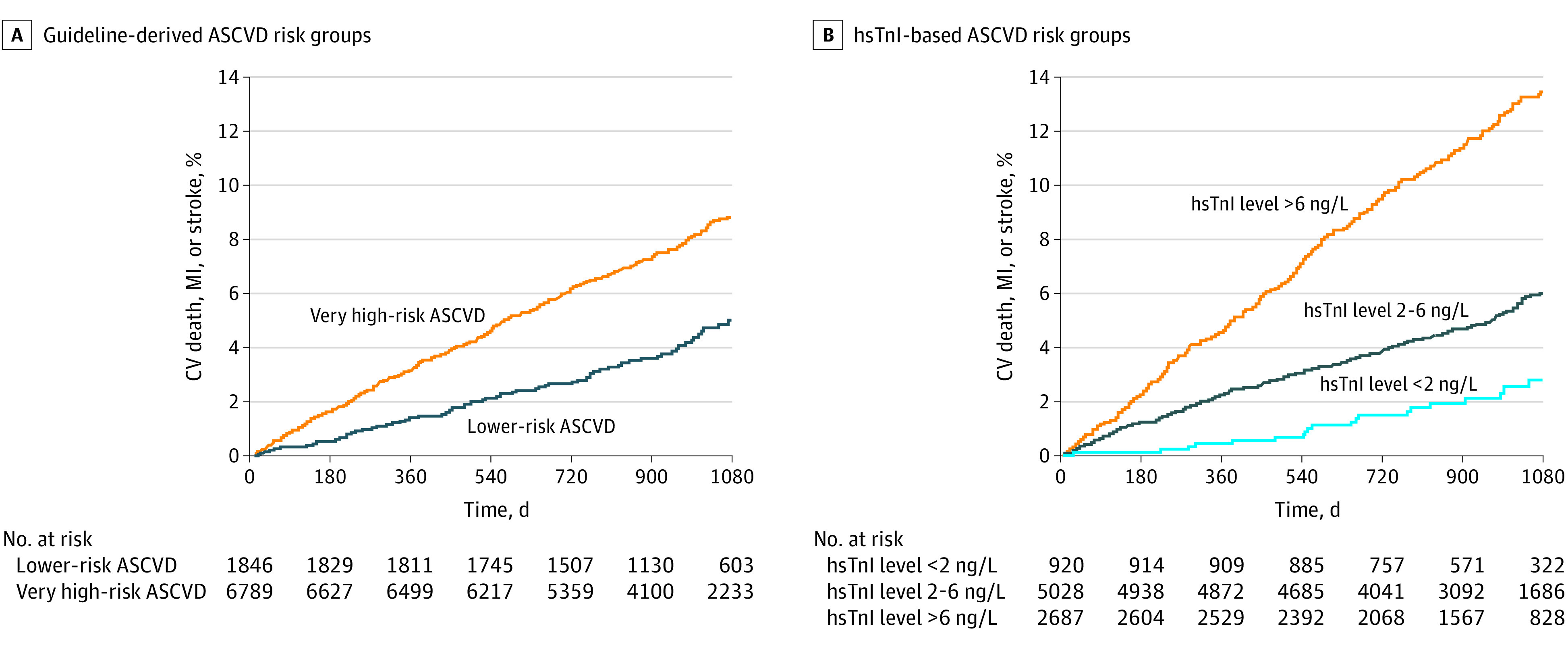
A, Patients meeting clinical criteria for the very high-risk ASCVD group had a statistically significantly higher rate of CV death, MI, or stroke, with a 3-year Kaplan-Meier event rate of 8.8% compared with 5.0% in the lower-risk ASCVD group (hazard ratio [HR], 2.01; 95% CI, 1.58-2.57; P < .001). B, Stratifying those with hsTnI levels of 6 ng/L or less into undetectable (<2 ng/L) and low (2-6 ng/L) levels identified patients with 3-year event rates of 2.8% and 6.0%, respectively, with a 3-year event rate of 13.5% in patients with hsTnI levels exceeding 6 ng/L. In the adjusted regression model, compared with patients with undetectable hsTnI levels, those with hsTnI levels of 2 to 6 ng/L were at a more than 2-fold higher risk (adjusted HR, 2.38; 95% CI, 1.47-3.85; P < .001) of adverse events, and those with hsTnI levels exceeding 6 ng/L were at an almost 5-fold higher risk (adjusted HR, 4.83; 95% CI, 2.98-7.84; P < .001).
hsTnI Level and the Primary End Point
When stratifying patients by baseline hsTnI level, the 3-year rates for the primary end point for hsTnI levels of 6 ng/L or less and greater than 6 ng/L were 5.5% and 13.5%, respectively (eTable 2B and eFigure 1 in the Supplement). Patients with lower hsTnI levels were at similar risk of the primary end point compared with the guideline-derived lower-risk ASCVD group; however, hsTnI levels exceeding 6 ng/L identified patients with higher event rates than the very high-risk ASCVD group. Further stratifying those with hsTnI levels of 6 ng/L or less into undetectable (<2 ng/L) and low (2-6 ng/L) levels identified patients with 3-year event rates of 2.8% and 6.0%, respectively (Figure 1B). In the adjusted regression model, compared with patients with undetectable hsTnI levels, those with hsTnI levels of 2 to 6 ng/L were at a more than 2-fold higher risk (adjusted HR, 2.38; 95% CI, 1.47-3.85; P < .001) for the primary end point, and those with hsTnI levels exceeding 6 ng/L were at an almost 5-fold higher risk (adjusted HR, 4.83; 95% CI, 2.98-7.84; P < .001) (eFigure 2 in the Supplement).
Considering the 58.2% (5028 of 8635) of patients with hsTnI levels between 2 and 6 ng/L to be at average risk for this ASCVD population, then patients with undetectable hsTnI levels (<2 ng/L) were at statistically significantly lower risk (adjusted HR, 0.42; 95% CI, 0.26-0.68; P < .001) of the primary end point, and patients with hsTnI levels exceeding 6 ng/L were at 2-fold higher risk (adjusted HR, 2.03; 95% CI, 1.71-2.41; P < .001) (Figure 2). In addition, no CV deaths occurred in patients with an undetectable hsTnI level (eFigure 3 in the Supplement).
Figure 2. Adjusted Hazard Ratio (HR) for the Primary End Point, Myocardial Infarction (MI), Stroke, and All-Cause Mortality Stratified by High-Sensitivity Troponin I (hsTnI) Level.

Patients with undetectable hsTnI levels (<2 ng/L) were at statistically significantly lower risk (adjusted HR, 0.42; 95% CI, 0.26-0.68; P < .001) of the primary end point, and patients with hsTnI levels exceeding 6 ng/L were at 2-fold higher risk (adjusted HR, 2.03; 95% CI, 1.71-2.41; P < .001). All-cause mortality is shown rather than CV death because there were no CV deaths in patients with hsTnI levels less than 2 ng/L, precluding calculation of an HR.
Integrating hsTnI Level Into the Cholesterol Guidelines Risk Schema
When patients in the guideline-derived very high-risk ASCVD group (overall 3-year event rate of 8.8%) were further risk stratified by hsTnI level, 9.0% (614 of 6789), 57.5% (3905 of 6789), and 33.4% (2270 of 6789) had an hsTnI level less than 2 ng/L, 2 to 6 ng/L, and greater than 6 ng/L, respectively. The 3-year event rates for CV death, MI, or stroke were 2.7% in patients with an hsTnI level less than 2 ng/L, 6.5% in patients with an hsTnI level of 2 to 6 ng/L, and 14.3% in patients with an hsTnI level exceeding 6 ng/L (P for trend <.001) (Figure 3). Of 6789 patients, 614 (9.0%) had discordant ASCVD risk and hsTnI level (very high clinical risk and undetectable hsTnI level), a 3-year event rate of 2.7% (<1% per year), and risk that was less than that of the overall rate in the guideline-derived lower-risk ASCVD group (Figure 4 and eTable 3 in the Supplement).
Figure 3. Three-Year Kaplan-Meier Rates for the Primary End Point (a Composite of Cardiovascular [CV] Death, Myocardial Infarction [MI], or Stroke) by Atherosclerotic Cardiovascular Disease (ASCVD) Risk and High-Sensitivity Troponin I (hsTnI) Level.

Patients in the guideline-derived very high-risk ASCVD group (overall 3-year event rate of 8.8%) were further risk stratified by hsTnI level. The 3-year event rates for CV death, MI, or stroke were 2.7% in patients with an hsTnI level less than 2 ng/L, 6.5% in patients with an hsTnI level of 2 to 6 ng/L, and 14.3% in patients with an hsTnI level exceeding 6 ng/L (P for trend <.001). Among patients in the lower-risk ASCVD group (overall 3-year event rate of 5.0%), hsTnI levels also provided a further gradient of risk. The 3-year event rates for CV death, MI, or stroke were 3.1% in patients with an hsTnI level less than 2 ng/L, 4.0% in patients with an hsTnI level of 2 to 6 ng/L, and 9.1% in patients with an hsTnI level exceeding 6 ng/L (P for trend <.001).
Figure 4. Reclassification of Cardiovascular Risk With the Addition of High-Sensitivity Troponin I (hsTnI) Level.

ASCVD indicates atherosclerotic cardiovascular disease; CV, cardiovascular; and MI, myocardial infarction.
Likewise, in the lower-risk ASCVD group (overall 3-year event rate of 5.0%), hsTnI levels also provided a further gradient of risk. In this group, 16.6% (306 of 1846), 60.8% (1123 of 1846), and 22.6% (417 of 1846) of patients had an hsTnI level less than 2 ng/L, 2 to 6 ng/L, and greater than 6 ng/L, respectively. The 3-year event rates for CV death, MI, or stroke were 3.1% in patients with an hsTnI level less than 2 ng/L, 4.0% in patients with an hsTnI level of 2 to 6 ng/L, and 9.1% in patients with an hsTnI level exceeding 6 ng/L (P for trend <.001) (Figure 3). Of 1846 patients, 417 (22.6%) had discordant ASCVD risk and hsTnI level (lower ASCVD risk and hsTnI level >6 ng/L) and had a 3-year event rate of 9.1%, comparable to the overall rate in the guideline-derived very high-risk ASCVD group (8.8%) (Figure 4).
The addition of hsTnI level to guideline-derived ASCVD risk led to a statistically significant improvement in the model for the primary end point (likelihood ratio test P < .001). Additional metrics of reclassification were also statistically significant and are listed in eTable 4 in the Supplement. The addition of hsTnI to guideline-derived ASCVD risk led to an improved net reclassification index at event rate of 0.15 (95% CI, 0.10-0.21) and integrated discrimination improvement index of 0.03 (95% CI, 0.03-0.04). Overall, use of hsTnI reclassified 1031 of 8635 patients (11.9%) (1 in 11 with very high-risk ASCVD and 1 in 4 with lower-risk ASCVD), whose guideline-derived clinical risk assignment would be altered (eTable 5 in the Supplement).
Discussion
This analysis highlights 3 key findings related to the current AHA/ACC cholesterol management guidelines9 risk stratification scheme and the potential for integration of hsTnI testing into risk stratification. First, the current guidelines’ approach to risk stratification in patients with ASCVD identifies 2 distinct groups at different risk for future major CV events. Second, hsTnI level alone stratifies risk, as well as the guideline-derived ASCVD risk groups. Third, hsTnI level provides CV risk stratification that is additive to the guideline-defined ASCVD groups and reclassifies risk appropriately.
Not all patients with ASCVD are at equivalent risk and, depending on their severity of disease and comorbidities, may have differing recommendations for certain therapies. For example, the very high-risk ASCVD group has a class IIa recommendation for both ezetimibe and PCSK9 inhibitors, whereas in lower-risk ASCVD patients there is only a class IIb recommendation for ezetimibe and no recommendation for a PCSK9 inhibitor.9 However, if one is preferentially recommending proven CV therapies to certain groups based on their perceived risk, it is critical to first demonstrate that the defined group is truly at higher risk, and second that each individual’s risk is classified as accurately as possible to ensure that the right patients are receiving the desired therapies.
The first of these 2 key goals was achieved by the recent AHA/ACC cholesterol management guidelines,9 consistent with other recent work.24 The clinical framework did in fact identify patients at higher clinical risk, with a 2-fold higher event rate in our prospective cohort biomarker substudy population. This relative risk may be an underestimate in this prior MI population given the absence of patients without a history of any major events. Therefore, the difference in risk between our 2 study groups may actually be greater among all ASCVD populations. However, our observed annualized CV event rate of approximately 3% (8.8% divided by 3) per year is likely a reasonable estimate for very high-risk ASCVD.
hsTnI Level and Lipid Therapy
Measurement of hsTnI might easily and affordably identify patients who are at low, intermediate, and high CV risk using hsTnI cut points of 2 and 6 ng/L to stratify patients with stable ischemic heart disease into low-risk (<1% per year), intermediate-risk (1%-3% per year), and high-risk (>3% per year) cohorts. Compared with patients at intermediate (average) risk, hsTnI level identifies not only patients who are at 2-fold higher risk when exceeding 6 ng/L but also those with a statistically significantly lower risk when less than 2 ng/L. Furthermore, among the 10.7% (920 of 8635) of patients with an undetectable hsTnI level, there were no CV deaths during the approximate 3-year follow-up in this study.
A key finding of this study is that risk stratification using hsTnI appears to be complementary to the 13 clinical risk factors in the guideline-based ASCVD framework. Indeed, the addition of hsTnI level gives a more granular estimate of CV risk. For example, the very high-risk patients with ASCVD and an undetectable hsTnI level have an annualized CV event rate of less than 1% (2.7% divided by 3) per year, reclassifying them as very low risk. In contrast, lower-risk patients with ASCVD and hsTnI level exceeding 6 ng/L carry an annualized CV event risk similar to that of the very high-risk ASCVD group. This approach identifies 20% to 25% of lower-risk patients with ASCVD who might be considered for ezetimibe or PCSK9 inhibition in the same way as very high-risk patients with ASCVD. In addition, clinically very high-risk patients with ASCVD and undetectable hsTnI levels may warrant management with similar strategies as those recommended for lower-risk (ie, not very high-risk) patients with ASCVD. These analyses suggest that incorporating an inexpensive and widely available biomarker into ASCVD risk assessment could both improve risk stratification and ensure that patients are offered risk-appropriate medical therapies.
Our findings relative to the current AHA/ACC cholesterol management guidelines9 are consistent with the application of hsTnI to the 2017 AHA/ACC high blood pressure guidelines.8 Both studies found that the incorporation of hsTnI improves risk stratification and identifies patients who may warrant more aggressive preventive therapies. In conjunction with the accumulated strong and consistent evidence for the predictive value of hsTnI level in stable patients with ASCVD,1,2,3,4,5,6,7 these findings support consideration of its implementation for risk-based therapeutic selection in clinical practice.
Limitations
The results of this study must be interpreted in the context of the study design. All patients in the analysis had a history of MI; therefore, the findings may not be generalizable to all ASCVD populations. The analyses were based on a prospective cohort biomarker substudy of patients with different hsTnI levels, as opposed to continuous data, which leads to a loss in power. However, use of cut points is often helpful for clinical decision-making and structured risk stratification, as in the cholesterol guidelines risk schema. In addition, these results are based on a particular hsTnI assay, and we cannot extrapolate to similar cut points for other troponin assays. This study was an exploratory analysis of the 2018 AHA/ACC cholesterol management guidelines9 risk groups, published after the prospective cohort biomarker substudy was designed. Some components of the guidelines’ risk stratification approach were not available, such as LDL-C level, and apoB level was used as a surrogate.11
Conclusions
The findings of this cohort substudy suggest that a strategy incorporating hsTn testing into a guideline-derived ASCVD risk algorithm provides enhanced risk stratification and reclassifies patients into more appropriate risk groups. This application of hsTn might be used to optimize the care of patients with ASCVD.
eTable 1. Baseline Characteristics in the Biomarker Cohort Compared to the Overall Trial Population
eTable 2A. Cardiovascular End Points Stratified by Baseline ASCVD Group
eTable 2B. Cardiovascular End Points Stratified by Baseline hsTnI
eTable 3. Cardiovascular End Points Stratified by Baseline ASCVD Group and hsTnI Level (ng/L)
eTable 4. Measures of Reclassification and Discrimination Improvement
eTable 5. Reclassification and Event Rates With hsTnI
eFigure 1. KM Rates for Primary End Point by hsTnI Category (>6 and ≤6 ng/L)
eFigure 2. Adjusted HR for the Primary End Point, MI, All-Cause Mortality, and Stroke Stratified by hsTnI Level
eFigure 3. Cardiovascular and Coronary Heart Death, MI, and Stroke by hsTnI Level (ng/L)
References
- 1.de Lemos JA, Drazner MH, Omland T, et al. Association of troponin T detected with a highly sensitive assay and cardiac structure and mortality risk in the general population. JAMA. 2010;304(22):2503-2512. doi: 10.1001/jama.2010.1768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Omland T, de Lemos JA, Sabatine MS, et al. ; Prevention of Events With Angiotensin Converting Enzyme Inhibition (PEACE) Trial Investigators . A sensitive cardiac troponin T assay in stable coronary artery disease. N Engl J Med. 2009;361(26):2538-2547. doi: 10.1056/NEJMoa0805299 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.White HD, Tonkin A, Simes J, et al. ; LIPID Study Investigators . Association of contemporary sensitive troponin I levels at baseline and change at 1 year with long-term coronary events following myocardial infarction or unstable angina: results from the LIPID Study (Long-term Intervention With Pravastatin in Ischaemic Disease). J Am Coll Cardiol. 2014;63(4):345-354. doi: 10.1016/j.jacc.2013.08.1643 [DOI] [PubMed] [Google Scholar]
- 4.Omland T, Pfeffer MA, Solomon SD, et al. ; PEACE Investigators . Prognostic value of cardiac troponin I measured with a highly sensitive assay in patients with stable coronary artery disease. J Am Coll Cardiol. 2013;61(12):1240-1249. doi: 10.1016/j.jacc.2012.12.026 [DOI] [PubMed] [Google Scholar]
- 5.Everett BM, Brooks MM, Vlachos HE, Chaitman BR, Frye RL, Bhatt DL; BARI 2D Study Group . Troponin and cardiac events in stable ischemic heart disease and diabetes. N Engl J Med. 2015;373(7):610-620. doi: 10.1056/NEJMoa1415921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cavender MA, White WB, Jarolim P, et al. Serial measurement of high-sensitivity troponin I and cardiovascular outcomes in patients with type 2 diabetes mellitus in the EXAMINE Trial (Examination of Cardiovascular Outcomes With Alogliptin Versus Standard of Care). Circulation. 2017;135(20):1911-1921. doi: 10.1161/CIRCULATIONAHA.116.024632 [DOI] [PubMed] [Google Scholar]
- 7.Bonaca MP, O’Malley RG, Jarolim P, et al. Serial cardiac troponin measured using a high-sensitivity assay in stable patients with ischemic heart disease. J Am Coll Cardiol. 2016;68(3):322-323. doi: 10.1016/j.jacc.2016.04.046 [DOI] [PubMed] [Google Scholar]
- 8.Pandey A, Patel KV, Vongpatanasin W, et al. Incorporation of biomarkers into risk assessment for allocation of antihypertensive medication according to the 2017 ACC/AHA high blood pressure guideline: a pooled cohort analysis. Circulation. 2019;140(25):2076-2088. doi: 10.1161/CIRCULATIONAHA.119.043337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. doi: 10.1161/CIR.0000000000000625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bonaca MP, Bhatt DL, Cohen M, et al. ; PEGASUS-TIMI 54 Steering Committee and Investigators . Long-term Use of Ticagrelor in Patients With Prior Myocardial Infarction. N Engl J Med. 2015;372(19):1791-1800. doi: 10.1056/NEJMoa1500857 [DOI] [PubMed] [Google Scholar]
- 11.Tani S, Yagi T, Atsumi W, Kawauchi K, Matsuo R, Hirayama A. Relation between low-density lipoprotein cholesterol/apolipoprotein B ratio and triglyceride-rich lipoproteins in patients with coronary artery disease and type 2 diabetes mellitus: a cross-sectional study. Cardiovasc Diabetol. 2017;16(1):123. doi: 10.1186/s12933-017-0606-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jacobson TA, Ito MK, Maki KC, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia, part 1: full report. J Clin Lipidol. 2015;9(2):129-169. doi: 10.1016/j.jacl.2015.02.003 [DOI] [PubMed] [Google Scholar]
- 13.Ford I, Shah AS, Zhang R, et al. High-sensitivity cardiac troponin, statin therapy, and risk of coronary heart disease. J Am Coll Cardiol. 2016;68(25):2719-2728. doi: 10.1016/j.jacc.2016.10.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Blankenberg S, Salomaa V, Makarova N, et al. ; BiomarCaRE Investigators . Troponin I and cardiovascular risk prediction in the general population: the BiomarCaRE Consortium. Eur Heart J. 2016;37(30):2428-2437. doi: 10.1093/eurheartj/ehw172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Everett BM, Zeller T, Glynn RJ, Ridker PM, Blankenberg S. High-sensitivity cardiac troponin I and B-type natriuretic peptide as predictors of vascular events in primary prevention: impact of statin therapy. Circulation. 2015;131(21):1851-1860. doi: 10.1161/CIRCULATIONAHA.114.014522 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Omland T, de Lemos JA, Holmen OL, et al. Impact of sex on the prognostic value of high-sensitivity cardiac troponin I in the general population: the HUNT Study. Clin Chem. 2015;61(4):646-656. doi: 10.1373/clinchem.2014.234369 [DOI] [PubMed] [Google Scholar]
- 17.Patterson CC, Blankenberg S, Ben-Shlomo Y, et al. Which biomarkers are predictive specifically for cardiovascular or for non-cardiovascular mortality in men? evidence from the Caerphilly Prospective Study (CaPS). Int J Cardiol. 2015;201:113-118. doi: 10.1016/j.ijcard.2015.07.106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Neumann JT, Havulinna AS, Zeller T, et al. Comparison of three troponins as predictors of future cardiovascular events: prospective results from the FINRISK and BiomaCaRE studies. PLoS One. 2014;9(3):e90063. doi: 10.1371/journal.pone.0090063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Apple FS, Simpson PA, Murakami MM. Defining the serum 99th percentile in a normal reference population measured by a high-sensitivity cardiac troponin I assay. Clin Biochem. 2010;43(12):1034-1036. doi: 10.1016/j.clinbiochem.2010.05.014 [DOI] [PubMed] [Google Scholar]
- 20.Apple FS, Collinson PO; IFCC Task Force on Clinical Applications of Cardiac Biomarkers . Analytical characteristics of high-sensitivity cardiac troponin assays. Clin Chem. 2012;58(1):54-61. doi: 10.1373/clinchem.2011.165795 [DOI] [PubMed] [Google Scholar]
- 21.Pencina MJ, Steyerberg EW, D’Agostino RB Sr. Net reclassification index at event rate: properties and relationships. Stat Med. 2017;36(28):4455-4467. doi: 10.1002/sim.7041 [DOI] [PubMed] [Google Scholar]
- 22.Pencina MJ, D’Agostino RB, Pencina KM, Janssens AC, Greenland P. Interpreting incremental value of markers added to risk prediction models. Am J Epidemiol. 2012;176(6):473-481. doi: 10.1093/aje/kws207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pepe MS, Kerr KF, Longton G, Wang Z. Testing for improvement in prediction model performance. Stat Med. 2013;32(9):1467-1482. doi: 10.1002/sim.5727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Roe MT, Li QH, Bhatt DL, et al. Risk categorization using new American College of Cardiology/American Heart Association guidelines for cholesterol management and its relation to alirocumab treatment following acute coronary syndromes. Circulation. 2019;140(19):1578-1589. doi: 10.1161/CIRCULATIONAHA.119.042551 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Baseline Characteristics in the Biomarker Cohort Compared to the Overall Trial Population
eTable 2A. Cardiovascular End Points Stratified by Baseline ASCVD Group
eTable 2B. Cardiovascular End Points Stratified by Baseline hsTnI
eTable 3. Cardiovascular End Points Stratified by Baseline ASCVD Group and hsTnI Level (ng/L)
eTable 4. Measures of Reclassification and Discrimination Improvement
eTable 5. Reclassification and Event Rates With hsTnI
eFigure 1. KM Rates for Primary End Point by hsTnI Category (>6 and ≤6 ng/L)
eFigure 2. Adjusted HR for the Primary End Point, MI, All-Cause Mortality, and Stroke Stratified by hsTnI Level
eFigure 3. Cardiovascular and Coronary Heart Death, MI, and Stroke by hsTnI Level (ng/L)