

Supplemental Digital Content is available in the text
Keywords: absenteeism, longitudinal study, managerial quality, occupational health, psychosocial work factors, stress
Abstract
Objective:
To examine whether low leadership quality predicts long-term sickness absence (LTSA) in Denmark.
Methods:
Using Cox models, we estimated the association between exposure to low leadership quality and onset of register based LTSA (more than or equal to 6 weeks) during 12-months follow-up among 53,157 employees without previous LTSA.
Results:
During 51,155 person-years, we identified 2270 cases of LTSA. Low leadership quality predicted LTSA with a dose–respone pattern after adjustment for confounders. The hazard ratio (HR) of LTSA in the lowest compared with the highest quartile of leadership quality was 1.61 (95% CI: 1.43 to 1.82). Further, change from high to low leadership quality over time predicted risk of LTSA (HR = 1.42, 95% CI: 1.02 to 1.97) compared with persistent high leadership quality.
Conclusions:
Exposure to low leadership quality is a risk factor of LTSA in the Danish workforce.
Learning Objectives
Discuss the rationale for studying the association between quality of leadership and the physical and mental health of employees.
Summarize the findings on the impact of leadership quality on risk of long-term sickness absence (LTSA) in the Danish workforce.
Discuss the implications for efforts to improve leadership quality as a means of reducing LTSA among employees.
Leadership quality also denoted managerial quality or supervisory quality, relates to specific behaviors or actions of a leader toward their subordinates. This includes, for example the leader's ability to provide guidance, solve conflicts, or support employees in their professional development.1 High leadership quality may be a job resource with the potential of buffering health-hazardous exposures at work. According to Schaufeli and Bakker2 job resources are aspects of work that reduce job demands, are functional in achieving work goals, and/or stimulate personal growth, learning, and development. Low leadership quality may also cause adverse working conditions, for example negative behaviors at work such as workplace bullying.3 Further, in accordance with the “Stress-as-Offense-to-Self” theory by Semmer et al,4 low leadership quality may be considered as a stressor in itself, as lack of appreciation, acknowledgment, and the breach of the social contract of what can be reasonably expected from a leader may directly affect employees’ well-being.
Long-term sickness absence (LTSA) may be considered an important indicator of both somatic and mental ill-health as it is strongly associated with risk of both disability pension and mortality.5,6 Although leadership quality is a major topic in work and organizational psychology,7 it is uncertain whether low leadership quality is associated with risk of LTSA. So far, prospective cohort studies on the association between leadership quality and risk of LTSA have shown inconsistent results, with studies both demonstrating associations, absence of associations and associations only in subgroups.8–13 In general, this literature is characterized by studies that are either based on relatively small samples or samples limited to specific occupational groups. Further, to our knowledge, no studies have yet investigated associations between changes in leadership quality over time and risk of LTSA. Examining such associations would be important for guiding future interventions.
In this article, we report results from a large prospective study linking survey data of more than 53,000 Danish employees from a wide range of job types and industries with register data on LTSA, defined as 6 or more consecutive weeks of sickness absence. In order to examine the potential effects of intervening on leadership quality among employees in Denmark we investigated (i) if low leadership quality predicted risk of LTSA and (ii) if low leadership quality predicted risk of LTSA differently among men and women, age groups, educational groups, and sector of employment (private or public). We further investigated in a subsample of more than 7000 employees with repeated measurement on leadership quality, (iii) if a change from high to low leadership quality predicted risk of LTSA compared with persistent high level of leadership quality.
METHODS
Study Design and Population
We used data from the 2012, 2014, and 2016 waves of the Work Environment and Health in Denmark study (WEHD), a biennial survey data on working conditions and health. The design of WEHD is described in more detail elsewhere.14 Briefly, WEHD consists of a stratified workplace sample conducted in 2012 and 2016, a nationwide sample conducted in 2012, 2014, and 2016, and a cohort that consists of all responders from the 2012 wave of the nationwide sample who also received a questionnaire in 2014 and 2016. We included first-time respondents from the stratified workplace sample and the nationwide sample (study population 1) and respondents from the cohort responding in 2012 and 2014 (study population 2). Inclusion criteria for all participants were being (i) liable to pay taxes in Denmark, (ii) aged 18 to 64 years, (iii) employed with at least 35 hours monthly and with a monthly income of at least 3000 DKK (460 US Dollar, 400 Euro as of December 31, 2012), and (iv) not having a “research protected” address.
Figure 1 presents data source and flowcharts for study population 1 and 2. Study population 1 included all first time respondents from the 2012, 2014, and 2016 waves, a total of 67,402 individuals. The average response rate was 50%. We excluded 5116 respondents reporting non-employment at baseline (i.e., the date individuals filled in the questionnaire), 5242 respondents with LTSA during the 2 years before or at baseline, 989 respondents who received either retirement benefits or disability pension or emigrated during the 2 years before baseline, 1633 respondents without a leader, and 1268 respondents with missing data on key variables including leadership quality (n = 631), yielding a final sample of 53,157 participants in study population 1.
FIGURE 1.

Data sources and flowcharts for creating study population 1 and study population 2. LTSA, long-term sickness absence; RR, response rate; WEHD, Work Environment and Health in Denmark.
Study population 2 included 11,471 individuals who responded to both the 2012 and 2014 wave. We excluded respondents reporting non-employment in 2012 or 2014 (n = 1444), had LTSA (n = 1376) or received retirement benefits, disability pension or migrated (n = 268) in the 4-year time period ranging from 2 years before filling in the questionnaire in the 2012 wave until filling in the questionnaire in the 2014 wave, reported that they had no leader (n = 444), and had missing data on key variables (n = 316), yielding a final sample of 7623 respondents in study population 2.
Measurement of Leadership Quality
Leadership quality was measured with eight items developed for WEHD: How often … (Q1) “does your immediate manager explain the company's objectives so you understand what they mean for your work tasks?”; (Q2) “do you have sufficient authority in relation to your responsibilities at work?”; (Q3) “does your immediate manager take the time to engage in your professional development?”; (Q4) “does your immediate manager involve you in the planning of your work?”; (Q5) “does your immediate manager give you the necessary feedback (praise and criticism) for your work?”; (Q6) “is your work recognized and appreciated by the management?”; (Q7) “do you get the necessary help and support from your immediate manager?”; (Q8) “can you trust the information that comes from the management?”
Response categories for all items were “Never” (1), “Seldom” (2), “Sometimes” (3), “Often” (4), and “Always” (5). Scores were summed for all participants with non-missing values on four or more leadership quality items, resulting in a scale with a potential range from 8 to 40 points, with higher scores indicating better leadership quality. Participants with missing values on three or less leadership quality items were assigned the mean score of their non-missing items. In total 52,800 (99.3%) responded to all eight items.
In study population 1, we categorized the leadership quality score into four groups based on the quartiles within the study population (1st quartile = 23.0, 2nd quartile = 27.0, and 3rd quartile = 32.0) and labeled the groups: “Low leadership quality” (8.0 ≤ score < 23.0, mean = 18.6, standard deviation [SD] = 3.1); “Medium-low leadership quality” (23.0 ≤ score ≤ 27.0, mean = 25.1, SD = 1.4); “Medium-high leadership quality” (27 < score ≤ 32.0, mean = 30.0, SD = 1.4); and “High leadership quality” (32 < score ≤ 40.0, mean = 35.9, SD = 2.3).
In study population 2, we categorized the leadership quality score by median split as high (more than or equal to median) or low (less than median) leadership quality in 2012 (median = 28.0) and 2014 (median = 27.0), respectively. We then categorized the respondents into four groups based on the level of leadership quality (high or low) in 2012 and 2014: “Persistent high leadership quality”; “Change from high to low leadership quality”; “Change from low leadership to high leadership quality”; and “Persistent low leadership quality.”
In study population 2, we categorized the leadership quality score by median split as high or low leadership quality in 2012 (median = 28.0) and 2014 (median = 27.0), respectively. We then categorized the respondents into four groups based on the level of leadership quality (high or low) in 2012 and 2014: “Persistent high leadership quality”; “Change from high to low leadership quality”; “Change from low leadership to high leadership quality”; and “Persistent low leadership quality.”
The leadership quality items were developed for the WEHD questionnaire and its psychometric properties as a scale have not previously been tested. Therefore, we conducted a factor analysis (rotation method: varimax) in study population 1. The eight items loaded on one global factor with an eigenvalue of 4.57 and all rotated factor loadings ranged from 0.63 to 0.84, confirming the unidimensionality of the scale. The internal consistency of the scale was high with a Cronbach α of 0.89.
Measurement of LTSA
Using the respondents’ unique civil registration number, the WEHD questionnaire data was linked to the DREAM register (Danish Register-Based Evaluation of Marginalization). DREAM contains weekly information on all social transfer payments in Denmark since 1991, and retirement, maternity leave, emigration, death, and all compensation granted for sickness absence since 1996.15 The type of social transfer payment is reported per week for each person.
We defined LTSA as any sickness absence spell lasting 30 days or more (more than or equal to 6 weeks). The reason for this cut-off point was that of January 2012 only sickness absence spells of 30 days or more were reimbursed by the municipality and subsequently registered in DREAM. We assessed the first episode of 6 or more consecutive weeks of sickness absence for each individual during 12 month (52 weeks) follow-up after baseline. We used the same definition of LTSA for study population 1 and 2.
Measurement of Covariates
As covariates we included sex (men or women), age (continuous), highest completed education in four categories (high; middle-high; middle-low; or low), according to the International Standard Classification of Education (ISCED),16 cohabitation (yes/no), number of children living at home (no children; at least one child younger than 8 years old; or at least one child aged 8 to 17 while no children younger than 8 years old in the household), and sector of employment (private or public). We selected these covariates, as they are associated with risk of LTSA in Denmark.10,11,17 Information on sex, age, education, cohabitation, and children was retrieved from population based registers.18–21 Information on sector of employment was retrieved from the Integrated Database for Labor Market Research.22 We further included job type defined by one-digit DISCO-08 number, the Danish version of the International Standard Classification of Occupations’ (ISCO-08) system,23 and industry by using the codes of the Danish version of the EU's nomenclature (NACE, Statistical classification of economic activities in the European Community) from Statistics Denmark.24 We used “the standard industrial grouping for publishing purposes” that aggregates the 726 possible industries into 10 groups. We included job type and industry as previous research suggest that job type is associated with participation in WEHD14 and we expected that reported leadership quality might differ between employees in different industries.
Statistical Analysis
Using Cox proportional regression models, we estimated hazard ratios (HR) and 95% confidence intervals (95% CI) for the association between exposure to different levels of leadership quality reported at baseline and risk of LTSA during a 12 months follow-up period with calendar time as the underlying time axis. Participants were followed from the date of first time questionnaire completion (study population 1) and the second time questionnaire completion (study population 2), respectively, until first episode of LTSA or censoring due to statutory retirement, voluntary early retirement, disability pension, emigration, death or end of follow-up, whichever came first. We calculated cases per 1000 person years, crude estimates and estimates adjusted for sex, age, education, cohabitation and children living at home, sector of employment, job type, industry, and type of sample (stratified workplace sample or nationwide sample). Because we used calendar time as the underlying time axis in the analyses, estimates were also adjusted for the year participants filled in the questionnaire accounting for trends in sickness absence over time and design differences between the three WEHD waves.
Proportional hazard assumptions for leadership quality and covariates were visually inspected using Log–Log curves. We found no indication of violation of the proportional hazard assumption.
In study population 1 we tested for a dose–response relationship between lower levels of leadership quality and risk of LTSA by estimating the fully adjusted HR (95% CI) for one unit decrease in the categorized leadership quality groups. Further, we tested if low leadership quality predicted risk of LTSA differently depending on sex, age, educational attainment, and sector of employment by repeating the analyses separately for men and women, age groups (18 to 29, 30 to 44, 45 to 54, 55 to 64 years), the four educational groups (low, middle-low, middle-high, high), and labor market sector (employment in private or public sector).
In study population 2, we examined the association between changes in leadership quality from the 2012 to the 2014 survey and risk of LTSA in the 12 months after the 2014 survey. We estimated adjusted HRs (95% CI) for subsequent risk of LTSA among respondents experiencing persistent low leadership quality, a change from low to high leadership quality, and change from high to low leadership quality between 2012 and 2014 compared with respondents with persistent high leadership quality between 2012 and 2014. We used the same covariates as in the analysis on study population 1.
Sensitivity Analysis
We conducted two sensitivity analyses among the respondents from study population 1. First, to test for reversed causation we excluded cases of LTSA during the first 6 months of follow-up (n = 1823). We then estimated HR and 95% CI for the association between low leadership quality at baseline and risk of LTSA from 6 months after baseline until 12 months after baseline.
Second, we examined the association between the eight leadership quality items separately and risk of LTSA. We standardized the eight items and the leadership quality score with a mean of zero and a standard deviation of one and estimated HR and 95% CI for LTSA per one standard deviation decrease in the leadership quality item, that is from higher to lower leadership quality score during 12 months of follow-up. Estimates were adjusted for the same covariates as in the analysis on study population 1. This analysis was limited to respondents from study population 1 without missing values on any of the eight leadership quality items (n: 52,800).
RESULTS
Characteristics of the Study Populations
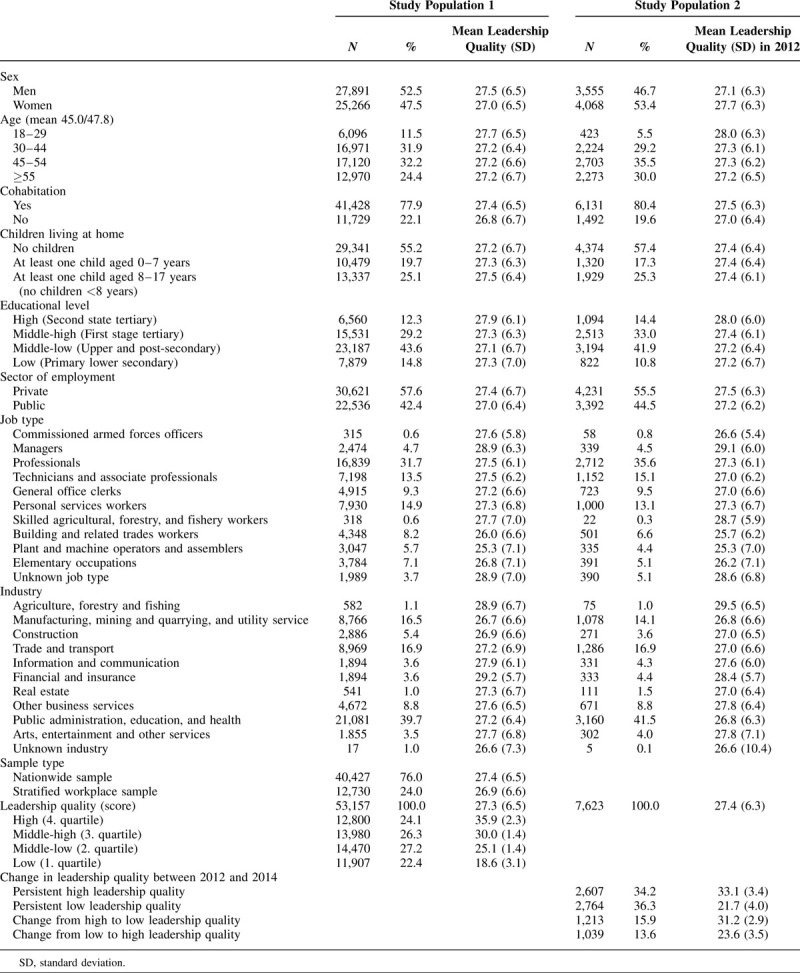
Table 1 shows the baseline characteristics of the two study populations. In study population 1 slightly more than half were men (52.5%), mean age was 45.0 years (SD = 11.3), and the majority was employed in the private sector (57.6%). Most participants had middle-low education (upper and post-secondary education, 43.6%), were cohabiting (77.9%), had no children living at home (55.2%), where professionals (31.7%), and were working with public administration, education, and health (39.7%). The mean leadership quality score was 27.3 (SD = 6.5) and similar across the study participants’ characteristics. In comparison with study population 1, participants in study population 2 were more often women (53.4%) and had a higher mean age of 47.8 (SD = 10.0).
TABLE 1.
Characteristics of the Study Population at Baseline and Average Leadership Quality in Study Population 1 (n = 53,157) and Study Population 2 (n = 7,623)
Leadership Quality and Predicted Risk of LTSA in Study Population 1
During 51,155 person years, we identified 2270 cases of LTSA (44 cases per 1000 person-years). Among LTSA cases, the mean time from baseline to LTSA was 26.7 weeks (0.51 years). Participants were censored during follow-up due to statutory retirement pension (n: 734), voluntary early retirement (n: 933), disability pension (n: 80), emigration (n: 216), or death (n: 282).
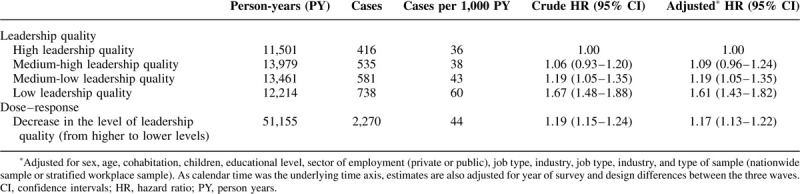
Table 2 shows LTSA cases per 1000 person-years and the crude and adjusted hazard ratios of the association between exposure to levels of leadership quality at baseline and onset of LTSA during follow-up. The number of LTSA cases per 1000 person-years was 36, 38, 43, and 60 for high, medium-high, medium-low, and low leadership quality, respectively. The corresponding adjusted hazard ratios were 1.09 (95% CI: 0.96 to 1.24), 1.19 (95% CI: 1.05 to 1.35), and 1.61 (95% CI: 1.43 to 1.82), respectively. There was a dose–response association between lower leadership quality scores and higher risk of LTSA. For each one unit decrease in the level of leadership quality (from higher to lower levels), the adjusted HR for LTSA was 1.17 (95% CI: 1.13 to 1.22).
TABLE 2.
Association Between Exposure to Different Levels of Leadership Quality at Baseline and Onset of Long-term Sickness Absence During 12-months Follow-up Among 53,157 Employees (Study Population 1)
Leadership Quality and LTSA Separately for Men and Women, Age Groups, Educational Level, and Sector of Employment in Study Population 1
Figure 2 shows the association between leadership quality and risk of LTSA separately for men and women, age groups, educational level, and sector of employment. Low leadership quality predicted risk of LTSA in both men and women, in all age groups, at all educational levels and among employees in the private and public sector. We found no indication of interactions between leadership quality and sex (P-value: 0.37), age groups (P-value: 0.55), educational level (P-value: 0.86), or sector of employment (P-value: 0.48).
FIGURE 2.
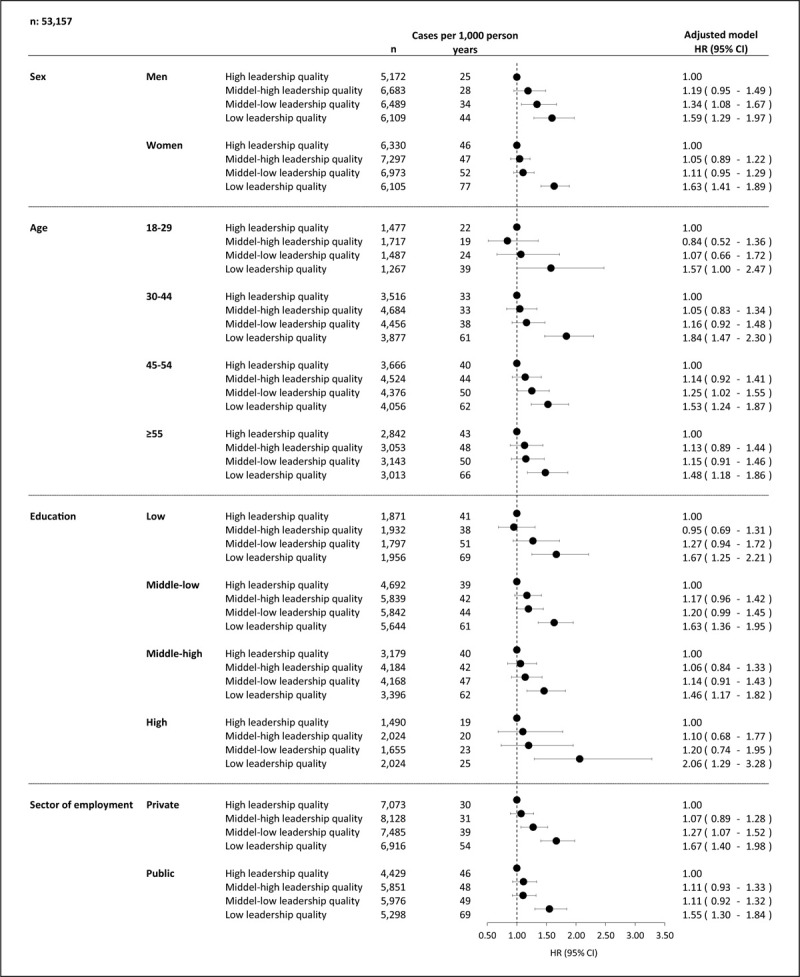
Association between leadership quality and long-term sickness absence during 12-months follow-up by sex, age groups, educational groups, and sector of employment among 53,157 employees (study population 1). Estimates are adjusted for sex, age, cohabitation, children, educational level, sector of employment (private or public), job type, industry, and type of sample (nationwide sample or stratified workplace sample). As calendar time was the underlying time axis, estimates are also adjusted for year of survey and design differences between the three waves. CI, confidence intervals; HR, hazard ratio; PY, person years.
Change in Leadership Quality and Predicted Risk of LTSA in Study Population 2
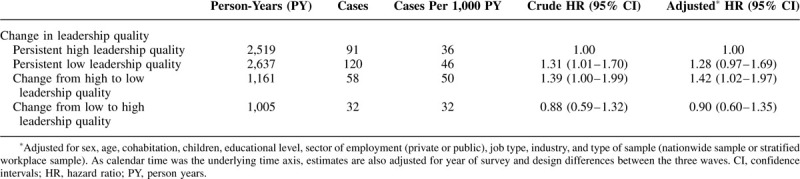
Table 3 shows for study population 2 LTSA cases per 1000 person-years and the crude and adjusted hazard ratios for the association between changes in leadership quality from the 2012 to the 2014 survey and onset of LTSA during 12 months follow-up after the 2014 survey. The number of LTSA cases per 1000 person-years was 36, 46, 50, and 32 for persistent high leadership quality, persistent low leadership quality, change from high to low leadership quality, and change from low to high leadership quality, respectively. Compared with persistent high leadership quality change from high leadership quality to low leadership quality predicted risk of LTSA with a HR of 1.42 (95% CI: 1.02 to 1.97). Persistent low compared with persistent high leadership quality was associated with risk of LTSA with a HR of 1.28 (95% CI: 0.97 to 1.69). The risk of LTSA in employees changing from low to high leadership quality was similar to that of employees with persistent high leadership quality (HR = 0.90, 95% CI: 0.71 to 1.47).
TABLE 3.
Association Between Changes in Leadership Quality from 2012 to 2014 and Long-term Sickness Absence During 12-months Follow-up Among 7623 Employees (Study Population 2)
Sensitivity Analysis
When we excluded cases during the first 6 months of follow-up, results were similar to the main analyses (Online-table 1).
When we analyzed the eight leadership quality items, separately, we found that one standard deviation decrease in the score predicted risk of LTSA for all eight items with adjusted HRs ranging from 1.11 to 1.22 (Online-figure 1). We found the strongest associations for items concerning authority in relation to responsibility (Q2), recognition and appreciation by the management (Q6), help and support from the immediate manager (Q7), and trusting information from the management (Q8). One standard deviation decrease in the total leadership quality score predicted risk of LTSA with an adjusted HR of 1.23 (95% CI: 1.18 to 1.28) (Online-figure 1).
DISCUSSION
Summary of Results
This study of 53,157 employees from a wide range of job types and industries in Denmark showed that during 12 months of follow-up low leadership quality, compared with high leadership quality, was associated with higher risk of onset of LTSA, measured as 6 or more consecutive weeks of sickness absence. There was a clear dose–response association between lower levels of leadership quality and higher risk of LTSA. Low leadership quality predicted a higher risk of LTSA in both men and women, in all age groups, at all educational levels, and among employees in the private and public sector.
In a subsample of 7623 employees with repeated measurements of leadership quality, change from high to low leadership quality was associated with higher risk of onset of LTSA compared with persistent high leadership quality. The increased risk of LTSA among employees who had experienced a worsening in leadership quality suggests that the association between low leadership quality and risk of LTSA is mainly driven by workplace conditions and not by personality traits of the respondents.
Comparison With Previous Research
Previous research on leadership quality and risk of LTSA has shown inconsistent results, with some studies reporting associations and other studies not or only in subgroups.8–13 For example, a Danish study by Clausen et al8 reported that low compared with high leadership quality predicted risk of LTSA with a HR of 1.21 (95% CI: 1.12 to 1.31) among 39,408 employees from four occupational groups. The slightly stronger estimate in our study (HR: 1.61, 95% CI: 1.43 to 1.82) may be due to (i) differences in the items measuring leadership quality, (ii) higher exposure contrast in our study (categorization into tertiles by Clausen et al8 and into quartiles in our study), and (iii) different definitions of LTSA (more than or equal to 3 weeks and more than or equal to 6 weeks, respectively).
Another Danish study by Lund et al12 reported that a higher degree of leadership quality was associated with a lower risk of LTSA among women but not among for men. In our study, though, we found associations in both women and men. A reason for this difference may be the different sample sizes of the two studies. Our sample was 10 times larger (53,157 vs 5357) and the amount of LTSA cases was nearly six times larger (2270 vs 359) compared with the study by Lund et al.12 Consequently, our study had higher statistical power, increasing the chances to detect also small associations, and to estimate associations with a high level of precision.
Strengths and Limitations
The strengths of this study are the large dataset with 53,157 employees representing a wide range of job types and industries in the Danish workforce. The use of register-based LTSA ensured almost no loss to follow-up. To our knowledge, this is the largest study on the association between leadership quality and sickness absence to date. The large number of participants and cases allowed us to conduct subgroup analyses demonstrating that associations between leadership quality and LTSA was similar for men and women and across age groups, educational groups, and sector of employment.
The leadership quality score used in this study was a newly developed tool for WEHD and had not been tested previously. We therefore conducted a factor analysis of the scale before analyzing the association between leadership quality and LTSA. The items of the scale loaded on one global factor, the internal consistency of the scale was high, and a Cronbach α of 0.89 indicated a high degree of correlation between the items. A sensitivity analysis showed that all eight items predicted LTSA in the same direction and contributed to the ability of the leadership quality scale to predict LTSA. Thus, although the leadership quality scale was not tested previously, it turned out as a reliable scale with predictive validity regarding risk of LTSA.
To ensure that our results were not affected by reverse causation we conducted a sensitivity analysis excluding LTSA events during the first 6 months after baseline. The analysis showed similar estimates with an increased risk of LTSA among participants reporting low leadership quality, indicating that the association between leadership quality and risk of LTSA is not due to reverse causation.
Several limitations of the study should be noted. First, the Danish registers do not include cause of LTSA and consequently we do not know whether a participant was sick due to a somatic disease or mental disorder. Consequently, we were not able to analyze whether low leadership quality predicted LTSA due to a somatic disease or mental disorder differently, which could be important to clarify as low leadership quality previously has been associated with an increased risk of both ischemic heart diseases and depressive disorder.25,26 Second, our study was limited to spells of sickness absence of 6 weeks or more as sickness absence in DREAM is registered when the employee's salary after 30 days is reimbursed by the municipalities. Long-term and short-term sickness absence may have different causes and therefore our results cannot be generalized to all types of sickness absence. Third, the baseline response rate in the three WEHD waves of 54%, 50%, and 50%, respectively may raise concerns about the representativeness of the results. A recent analysis conducted on the 2012 WEHD wave showed that sex, age, cohabitations, education, and job type were associated with the likelihood of responding to the questionnaire in 2012,14 and consequently we adjusted for these variables in the analyses. Finally, it is unclear whether our results are generalizable to employees in other countries with different sickness absence legislations. As our study, like most previous research on work environment and LTSA, has been conducted in a Nordic country, future prospective studies on leadership quality and LTSA in other than Nordic countries is encouraged.
We did not adjust the estimates for other psychosocial work conditions, even though previous research has shown associations between other psychosocial work environment factors and risk of LTSA,8,10,13,27 including a study using the WEHD data that found an association between high emotional demands and LTSA.27 We refrained from these adjustments, because we reasoned that low leadership quality may cause the occurrence of several potentially adverse psychosocial work environment factors, for example high quantitative demands, high emotional demands, low job control, or even workplace bullying.3 Thus, these other psychosocial work environment factors might not be confounders but mediators in the causal pathway linking low exposure to leadership quality with risk of LTSA, which would make statistical adjustment inappropriate. We suggest that future studies investigate how psychosocial working conditions may mediate the association between leadership quality and LTSA.
CONCLUSION
Low leadership quality predicted an increased risk of LTSA in a large nationwide sample of employees in Denmark. Associations were similar across men and women, age groups, educational levels, and sector of employment. Compared with persistent high leadership quality a change from high to low leadership quality 2 years apart predicted a higher risk of LTSA indicating that the increased risk of LTSA is likely related to workplace conditions rather than individual traits of the employees. As we found that low leadership quality predicted a 1.61 fold increased risk of LTSA, measured as 6 or more weeks of sickness absence, leadership quality may be considered an important social stressor at work with considerable consequences. Therefore, future intervention studies should examine if improving leadership quality can reduce LTSA among employees.
Supplementary Material
Supplementary Material
Footnotes
Clinical significance: Low leadership quality may be considered a stressor at work affecting employees’ well-being. Long-term sickness absence is an important indicator of somatic and mental health and is strongly associated with risk of disability pension. Improving leadership quality may reduce risk of long-term sickness absence.
Funding: The Danish Working Environment Research Fund (grant number 10-2016–03). The funding source had no further role in the study design; data collection, analysis and interpretation of data; in the writing of the paper, or in the decision to submit the paper for publication.
Sørensen, Framke, Clausen, Garde, Johnsen, Kristiansen, Madsen, Nordentoft, and Rugulies have no relationships/conditions/circumstances that present potential conflict of interest.
The JOEM editorial board and planners have no financial interest related to this research.
REFERENCES
- 1.Pejtersen JH, Kristensen TS, Borg V, Bjorner JB. The second version of the Copenhagen Psychosocial Questionnaire. Scand J Public Health 2010; 38:8–24. [DOI] [PubMed] [Google Scholar]
- 2.Schaufeli WB, Bakker AB. Job demands, job resources, and their relationship with burnout and engagement: a multi-sample study. J Organ Behav 2004; 25:293–315. [Google Scholar]
- 3.Hauge LJ, Einarsen S, Knardahl S, Lau B, Notelaers G, Skogstad A. Leadership and role stressors as departmental Level predictors of workplace bullying. Int J Stress Manag 2011; 18:305–323. [Google Scholar]
- 4.Semmer NK, Jacobshagen N, Meier LL, Elfering A. Houdmont J, Scott M. Occupational stress research: the “Stress-as-offense-to-self” perspective. Occupational Health Psychology: European Perspectives on Research Education and Practice. Nottingham:Nottingham University Press; 2007. 43–60. [Google Scholar]
- 5.Amiri S, Behnezhad S. Depression and risk of disability pension: A systematic review and meta-analysis. Int J Psychiatry Med 2019; doi: 10.1177/0091217419837412. [DOI] [PubMed] [Google Scholar]
- 6.Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry 2015; 72:334–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lovelace JB, Neely BH, Allen JB, Hunter ST. Charismatic, ideological, & pragmatic (CIP) model of leadership: a critical review and agenda for future research. Leadersh Q 2019; 30:96–110. [Google Scholar]
- 8.Clausen T, Burr H, Borg V. Do psychosocial job demands and job resources predict long-term sickness absence? An analysis of register-based outcomes using pooled data on 39,408 individuals in four occupational groups. Int Arch Occup Environ Health 2014; 87:909–917. [DOI] [PubMed] [Google Scholar]
- 9.Aagestad C, Johannessen HA, Tynes T, Gravseth HM, Sterud T. Work-related psychosocial risk factors for long-term sick leave: a prospective study of the general working population in Norway. J Occup Environ Med 2014; 56:787–793. [DOI] [PubMed] [Google Scholar]
- 10.Labriola M, Christensen KB, Lund T, Nielsen ML, Diderichsen F. Multilevel analysis of workplace and individual risk factors for long-term sickness absence. J Occup Environ Med 2006; 48:923–929. [DOI] [PubMed] [Google Scholar]
- 11.Rugulies R, Aust B, Pejtersen JH. Do psychosocial work environment factors measured with scales from the Copenhagen Psychosocial Questionnaire predict register-based sickness absence of 3 weeks or more in Denmark? Scand J Public Health 2010; 38: suppl: 42–50. [DOI] [PubMed] [Google Scholar]
- 12.Lund T, Labriola M, Christensen KB, Bültmann U, Villadsen E, Burr H. Psychosocial work environment exposures as risk factors for long-term sickness absence among Danish employees: results from DWECS/DREAM. J Occup Environ Med 2005; 47:1141–1147. [DOI] [PubMed] [Google Scholar]
- 13.Clausen T, Nielsen K, Carneiro IG, Borg V. Job demands, job resources and long-term sickness absence in the Danish eldercare services: a prospective analysis of register-based outcomes. J Adv Nurs 2012; 68:127–136. [DOI] [PubMed] [Google Scholar]
- 14.Johnsen NF, Thomsen BL, Hansen JV, Christensen BS, Rugulies R, Schlünssen V. Job type and other socio-demographic factors associated with participation in a national, cross-sectional study of Danish employees. BMJ Open 2019; 9:e027056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Burr H, Pedersen J, Hansen JV. Work environment as predictor of long-term sickness absence: Linkage of self-reported DWECS data with the DREAM register. Scand J Public Health 2011; 39: suppl: 147–152. [DOI] [PubMed] [Google Scholar]
- 16. United Nations Educational Scientific and Cultural Organization (UNESCO). International Standard Classification of Education (ISCED 1997); 1997. Available at: http://www.unesco.org/education/information/nfsunesco/doc/isced_1997.htm. Accessed May 22, 2019. [Google Scholar]
- 17.Nielsen ML, Rugulies R, Christensen KB, Smith-Hansen L, Kristensen TS. Psychosocial work environment predictors of short and long spells of sickness absence during a two-year follow-up. J Occup Environ Med 2006; 48:591–598. [DOI] [PubMed] [Google Scholar]
- 18.Pedersen CB. The Danish Civil Registration System. Scand J Public Health 2011; 39:22–25. [DOI] [PubMed] [Google Scholar]
- 19.Jensen VM, Rasmussen AW. Danish Education Registers. Scand J Public Health 2011; 39:91–94. [DOI] [PubMed] [Google Scholar]
- 20. Statistics Denmark. Documentation of Statistics: Population and Elections; 2019. Available at: https://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics?subject=02. Accessed May 22, 2019. [Google Scholar]
- 21. Statistics Denmark. Documentation of Statistics: Households, Families and Children; 2019. Available at: https://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics/households--families-and-children. Accessed May 22, 2019. [Google Scholar]
- 22.Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health 2011; 39:95–98. [DOI] [PubMed] [Google Scholar]
- 23. International Labour Organization. ISCO-08 Structure, Index Correspondence with ISCO-88; 2018. Available at: http://www.ilo.org/public/english/bureau/stat/isco/isco08/. Accessed November 20, 2018. [Google Scholar]
- 24. Torma K, Simbold CT, Sørensen AG, Madsen KK, Skjelbo K. Dansk Branchekode 2007, DB07 Copenhagen: Statistics Denmark; 2007. [Google Scholar]
- 25.Rugulies R, Jakobsen LM, Madsen IEH, Borg V, Carneiro IG, Aust B. Managerial quality and risk of depressive disorders among Danish eldercare workers: a multilevel cohort study. J Occup Environ Med 2018; 60:120–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nyberg A, Alfredsson L, Theorell T, Westerlund H, Vahtera J, Kivimäki M. Managerial leadership and ischaemic heart disease among employees: the Swedish WOLF study. Occup Environ Med 2009; 66:51–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Framke E, Sørensen JK, Nordentoft M, et al. Perceived and content-related emotional demands at work and risk of long-term sickness absence in the Danish workforce: a cohort study of 26 410 Danish employees. Occup Environ Med 2019; 76:895–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.