

Abstract
Background
Vertical maxillary excess, a dentofacial deformity present in a large proportion of population impute an increased lower facial height due to increased maxillary height. This results in a clockwise rotation in the mandible, and the chin advances posteriorly and inferiorly. Le Fort I superior repositioning of the maxilla begets movement of pogonion point anteriorly and cranially. Cephalometric analysis helps to access change in position of chin following Le Fort I impaction. In our study, from this analysis a formula was defined to perceive the exact amount of this change in chin position along the vertical and sagittal plane as a result of autorotation.
Materials and Methods
This experimental study assessed 45 patients with vertical maxillary excess over a period of 2 years and 6 months (January 2016–May 2018) in Government Medical College Hospital, Kottayam, Kerala, India. The planned procedure was Le Fort I superior impaction for correction of vertical maxillary excess. Pre-operative cephalograph was taken initially. Post-operative cephalograph after 3 months was then compared with initial pre-operative cephalograph to assess the change in position of the pogonion and menton.
Results
Forty-five participants were studied. The multiple regression model was applied to predict the changes in the chin (dependent factor) according to the vertical change in the maxilla (predictive factor). For every 1 mm change in the maxilla vertically, the chin was estimated to move 0.59 vertically. For a standard deviation increase of 1 in the position of the maxilla, the chin moved superiorly by 0.744 of the standard deviation. For every 1 mm of vertical change in the maxilla, the chin could be expected to move 0.22 mm horizontally. For a standard deviation increase of 1 in the maxillary position, the chin advanced by 0.273 of the standard deviation.
Conclusion
This study draws to a conclusive finding that the movement of maxilla in the superior direction has an effect on the repositioning of the chin in the anterior and cranial directions. This has led to a formulation that 1 mm of superior impaction of maxilla results in 0.6 mm of vertical and 0.2 mm of sagittal movement of chin. This might help to have a glance of future chin position and aid in deciding the need for mandibular surgery.
Keywords: Autorotation, Le Fort I impaction, Chin, Maxillary osteotomy
Introduction
A smile is the prettiest thing you ever wear. But some individuals hide it because they have a “gummy smile”. Vertical maxillary excess is prevalent in approximately 22.2% of population [1]. The correction of vertical maxillary excess usually includes maxillary Le Fort I superior impaction. After maxillary superior impaction, one of the effects on mandible is the anterosuperior displacement of bony chin position. The mandible rotates from the patient’s original occlusion to a more superior position.
The chin is defined by a graceful transition of the mandibular angles towards the midline [2]. Hence, it is of prime importance to predict the amount of autorotation in maxillary superior impaction and pogonion displacement in vertical and sagittal planes as it causes significant changes in the lower third of the face. In the surgical orthodontic treatment of dentofacial deformities, cephalometric prediction tracings are important to assess the bony and soft tissue changes. Cephalometric analysis enables one to make a quantitative assessment of the location and magnitude of the dentofacial deformity (Fig. 1).
Fig. 1.
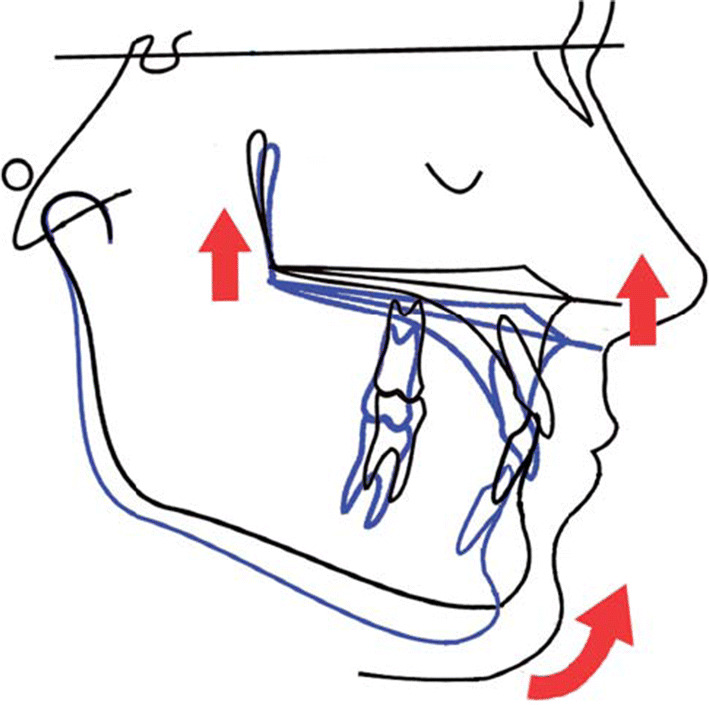
In VME patients, the increased maxillary height causes a clockwise rotation in the mandible and the chin moves posteriorly and inferiorly. After the Le Fort I superior impaction surgery, the pogonion will rotate anteriorly and superiorly [3]
In our study, we evaluate the extent of change in chin position in sagittal and vertical planes following Le Fort I superior impaction using cephalometric analysis.
Materials and Methodology
This clinical study was conducted in the Department of Oral and Maxillofacial Surgery, Government Medical College, Kottayam. Forty-five patients with vertical maxillary excess were selected. The planned procedure was Le Fort I impaction for correction of vertical maxillary excess. Out of 45 patients operated, 26 were females and rest were males, and their age ranged from 19 to 28 years.
Pre-operative cephalograph was taken initially. Post-operative cephalograph after 3 months was then taken to assess the change in position of the pogonion and menton. All patients underwent post-operative orthodontic treatment.
Duration of Study
The study was conducted over a period of 2 years and 6 months (January 2016–May 2018)
Inclusion Criteria
All patients who attained completion of skeletal maturity having vertical maxillary excess planned for superior impaction by Le Fort I osteotomy.
Exclusion Criteria
Patients with syndrome/cleft palate
Patients who underwent mandibular advancement/setback procedures.
Medically compromised patients.
Patients with history of trauma.
Use of distraction techniques in mandible
Cephalometric Analysis
Lateral cephalograms taken were used to assess the change in chin position and the amount of maxillary superior repositioning. Hard tissue cephalometric analysis undertaken was based on COGS analysis.
Tracing Technique
All the cephalograms were traced by a single operator. Cephalometric landmarks were located, identified, and marked. Pre-operative and post-operative cephalometric analyses were used to determine the amount of the maxillary superior repositioning.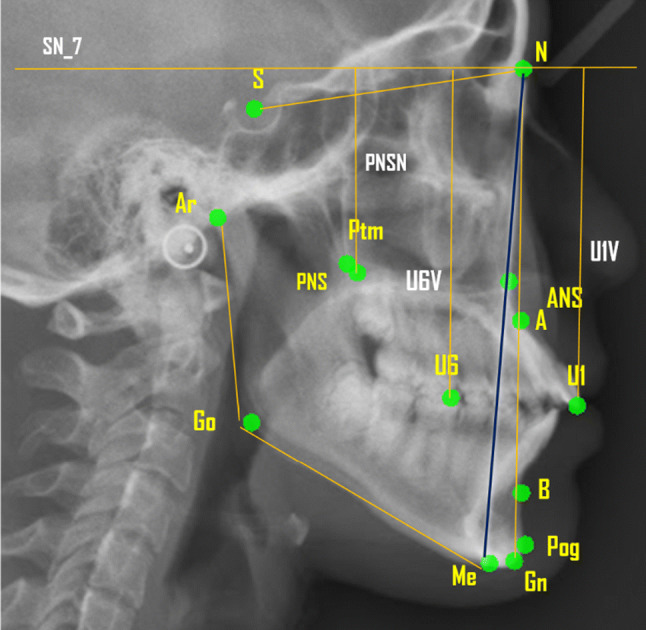
The distance from nasion to menton was taken to assess the vertical change in chin position, and the distance from true horizontal plane to pogonion was used to assess the sagittal change in chin position.
SN_7 plane A 7 degree line is drawn from line connecting sella (S) to nasion (N) which is the true horizontal plane (SN_7). All the vertical measurements are taken perpendicular to this plane, and all the horizontal measurements are measured parallel to this plane.
U6V and U1V plane The analysis measured the linear distances (in millimetres) from the maxillary landmarks at upper molar (U6) and upper central incisor (U1) to vertical reference lines that dropped perpendicular to the true horizontal plane passing through sella point. The difference in the vertical distance provides the amount of superior impaction of maxilla post-operatively.
N-Me line The distance from the nasion to menton point was applied to assess the vertical changes of the chin before and after the operation.
N-Pog Line The most prominent point of the chin, pogonion, was used to determine the sagittal changes of the chin before and after surgery. The measurement was made parallel to the true horizontal plane from a perpendicular dropped through N of the true horizontal plane.
SNA Plane The changes in A point in the anterior–posterior direction were measured parallel to the true horizontal plane from a perpendicular that dropped through N of the SN _7.
PNSN line A perpendicular dropped from the true horizontal plane to the posterior nasal spine (PNS) provides the posterior maxillary height.
Assessment of the Patients
Assessment of the patients was done daily following surgery for 5 days and after that every week till 1 month. Then, a monthly review for 3 months followed by a half yearly assessment of the patient was performed.
Post-operative Lateral Cephalogram
Lateral cephalogram was taken at three months following surgery to assess the change in chin position vertically and sagittally.
Vertical change in chin position was obtained from the distance from the nasion to menton, and the horizontal change in position of chin was assessed from the distance from the perpendicular line that dropped from the true horizontal plane (SN_7) to the most prominent point on chin, pogonion.
Results
The assessment of the data using a multiple regression model demonstrated that approximately 89.1% of the vertical change in the chin could be predicted by knowing the amount of the maxillary superior repositioning (R2 = 0.891). For every 1-mm change in the maxilla vertically, the chin was estimated to move 0.59 vertically. For a standard deviation increase of 1 in the position of the maxilla, the chin moved superiorly by 0.744 of the standard deviation (β = 0.744).
The multiple regression model showed that approximately 59.8% of the horizontal change in the chin could be accounted for by the amount of maxillary superior repositioning (R2 = 0. 598). For every 1 mm of vertical change in the maxilla, the chin could be expected to move 0.22 mm horizontally. For a standard deviation increase of 1 in the maxillary position, the chin advanced by 0.273 of the standard deviation (β = 0.273).
The equation thus obtained for prediction of the change in chin position vertically following Le Fort I superior impaction is
YMe is the difference of vertical change in chin N-Me after 3 months (NMe pre–NMe 3 Mon), V1 is difference of vertical distance at U6 from SN (i.e. amount of superior impaction to be obtained), V2 is difference of vertical distance at U1 from SN (i.e. amount of superior impaction to be obtained).
The equation thus obtained for prediction of the change in chin position horizontally following Le Fort I superior impaction is
YPog is the difference of horizontal distance in chin N-MePog after 3 months (N-Pog pre–N-Pog3 Mon), V1 is difference of vertical distance at U6 from SN (i.e. amount of superior impaction to be obtained), V2 is difference of vertical distance at U1 from SN (i.e. amount of superior impaction to be obtained).
Discussion
This study pointed out the high predictability of the chin position based on the amount of maxillary superior repositioning.
Sagittal Changes After Autorotation
Wang et al. [4] concluded in their study that the horizontal movement of the Pog point demonstrated high correlation with the vertical movement of the ANS point and the upper first molar, but not affected by the vertical movement of the PNS point. The horizontal movement of the Pog point was almost in 1:1 ratio to the vertical movement of the ANS point and the U6 point suggesting that the ratio could be used to predict horizontal chin position.
In our study, we obtained a 5:1 ratio of the horizontal movement of Pog point to the vertical movement of U6 point.
This difference in ratio may be due to the change in centre of condylar rotation after surgery and prior to surgery. Mandibular movement may be a simple rotation or translation or a combination of these; this might be the other reason for the difference observed. This could be also due to difference in techniques used for mandibular splint fabrication.
The above study also states that there is a large individual variation in finding the centre of rotation. It could overestimate the horizontal position of chin by 2 mm in 5 mm of surgical maxillary impaction [4]. A further study to determine the condylar centre along with the dimensional change of chin position would give more light to this discrepancy.
Vertical Changes After Autorotation
The vertical dimensions of the lower-face change via maxillary impaction followed by mandibular autorotation. There are many reports in the literature on the extent of reduction in lower facial height in relation to maxillary impaction.
Schendel et al. [5], Bell et al. and Fish et al. who dealt with the question of impaction of the maxilla and autorotation of the mandible at an early stage recommended a simulation of the outcome using templates on the lateral cephalogram.
Lee et al. [6] observed that the soft tissue structures followed the skeletal structures to almost the same extent after maxillary impaction [3, 7].
Bell et al., Fish et al. and Epker and Fish [5, 8, 9] described a 1:1 ratio between lower-face shortening (cranial movement of the chin prominence) after maxillary impaction and mandibular autorotation.
In our study, the vertical distance was measured from nasion to menton, and we got a ratio of 1:0.8 which is approximately 1:1.
Pitfall in the Study
A study by Arabion [3] concluded when maxillary impaction was more than 8 mm, the regression model did not follow a linear correlation between the amount of maxillary superior repositioning and horizontal change in the pogonion. All the 45 cases of maxillary impaction performed were less than 8 mm; hence, our study could not confirm this finding.
The formula derived for prediction of vertical in chin is for cases with superior impaction less than 8 mm.
Wang et al. [4] in their study concluded that when the condyle acted a centre of rotation, the erroneous determination of the true rotatory axis of the mandible encompassed the overestimated horizontal position of the Pog point by 1.7 mm and underestimated vertical position of the Me point by 1.3 mm in the results. This might offer surgeons or orthodontists the wrong information in deciding the surgical plan and facial profile. In our study, centre of rotation and its correlation with the mandibular shift was not assessed.
Conclusion
From this study, we conclude that there is a change in chin position following Le Fort I impaction that could be predicted using a formula. Applying thus obtained formula, we found that with a 1-mm superior impaction of maxilla vertically, the position of chin moves 0.6 mm vertically and 0.2 mm horizontally. This derived formula has to be applied in a larger population to determine the accuracy of the model.
Funding
None.
Compliance with Ethical Standards
Conflict of interest
None.
Ethical approval
The institutional ethical committee approved this experimental study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Jayalakshmi Jayakumar, Email: jjsmilesalot@gmail.com.
N. Jayakumar, Email: drjkndct@gmail.com
Bobby John, Email: johnbobbyj@gmail.com.
P. G. Antony, Email: drpgantony@yahoo.com
References
- 1.Ming TC. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle Orthod. 2006;76(5):806–809. doi: 10.1043/0003-3219(2006)076[0806:SAMODD]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Naini FB, Gill DS. Facial aesthetics: 1. Concepts and canons. Dent Update. 2008;35(2):102–104. doi: 10.12968/denu.2008.35.2.102. [DOI] [PubMed] [Google Scholar]
- 3.Arabion H, Tabrizi R, Fattahi H, Khaghaninezhad M, Bahramnia F. Spatial changes of the chin in the vertical and sagittal planes after superior repositioning of the Maxilla. J Craniofac Surg. 2015;26(3):e249–e253. doi: 10.1097/SCS.0000000000001363. [DOI] [PubMed] [Google Scholar]
- 4.Wang Y, Ko EW, Huang C, Chen Y. The inter-relationship between mandibular autorotation and maxillary LeFort I impaction osteotomies. J Craniofac Surg. 2006;17(5):898–904. doi: 10.1097/01.scs.0000234985.99863.97. [DOI] [PubMed] [Google Scholar]
- 5.Schendel SA, Eisenfeld JH, Bell WH, Epker BN. Superior repositioning of the maxilla: stability and soft tissue osseous relations. Am J Orthod. 1976;70(6):663–674. doi: 10.1016/0002-9416(76)90226-8. [DOI] [PubMed] [Google Scholar]
- 6.Lee D, Bailey L, Proffit WR. Soft tissue changes after superior re- positioning of the maxilla with Le Fort I osteotomy: 5-year follow up. Int J Adult Orthod Orthognath Surg. 1996;11:301–311. [PubMed] [Google Scholar]
- 7.Steinhäuser S, Richter U, Richter F, Bill J, Rudzki-janson I. Profile changes following maxillary impaction and autorotation of the mandible. J Orofacial Orthoped. 2008;69(1):31–41. doi: 10.1007/s00056-008-0723-8. [DOI] [PubMed] [Google Scholar]
- 8.Fish LC, Epker BN. Surgical-orthodontic cephalometric prediction tracing. J Clin Orthod. 1980;8:119–125. [PubMed] [Google Scholar]
- 9.Stoker NG, Epker BN, Peter J, Hospital S, Worth F, et al. The posterior maxillary ostectomy: a retrospective study of treatment results. Int J Oral Surg. 1974;3:153–157. doi: 10.1016/S0300-9785(74)80019-0. [DOI] [PubMed] [Google Scholar]