

Abstract
Introduction
Various atraumatic tooth extraction techniques have gained popularity over the last few decades, and numerous instruments have been devised for the same. A pair of physics forceps is one such instrument that maintains the integrity of the gingival and surrounding periodontium while delivering the tooth out of the socket atraumatically. Extractions using these forceps are less invasive over conventional forceps using less intraoperative time but are technique sensitive and have a definitive learning curve.
Aim
To compare the efficacy of physics forceps with conventional forceps in the orthodontic extraction of bilateral premolars and to compare the clinical outcome and complications of each.
Material and Methods
In this prospective randomized split-mouth study, all the patients (n = 50) and total premolars (n = 200) were divided into two groups, in which first premolars in maxillary and mandibular quadrant on one side were extracted with physics forceps (n = 100), whereas those in the other 2 quadrants was done with conventional forceps (n = 100). Clinical outcomes in the form of time taken for extraction, postoperative pain, total number of analgesics taken, buccal cortical plate fracture, soft tissue healing after extraction and other complications were recorded and compared.
Results
The mean time for extraction of premolars with physics forceps was significantly less as compared to the conventional forceps (P 0.001). There was no statistically significant difference in the postoperative pain on any of the postoperative days, between both the groups. No major complication except root fracture was seen in 3 teeth in physics forceps group. Soft tissue healing was similar in both the groups.
Conclusion
Physics forceps are an effective method of atraumatic extraction of premolars as it reduce the intraoperative time significantly and have comparable clinical outcomes as the conventional forceps and are associated with few complications.
Keywords: Physics forceps, Atraumatic extractions, Orthodontic extractions
Introduction
Tooth extraction is one of the most common procedures performed in the general practice. Traditional extraction techniques use a combination of severing the periodontal attachment, luxation with an elevator and removal with forceps. If the tooth is already weakened by endodontic treatment or if both the roots are long and/or dilacerated, traditional extraction forceps often cause fracture of the tooth [1], surrounding bone or both which can lead to more extensive surgical approach, leading to corresponding undesirable postoperative sequelae.
In the past decade, there has also been an increased interest in atraumatic tooth extractions in order to maintain bone for implant insertion. Techniques for atraumatic extraction and techniques such as powered periotomes, piezosurgery, lasers, physics forceps, orthodontic extrusion of third molar and the Benex vertical extraction system are being widely used and reported [2–6].
A revolutionary new instrument in exodontia, the physics forceps introduced by Dr. Richard Golden [6], is dental extractor rather than a forcep and uses the biomechanical advantage of a first-class lever and distributes stress without the squeezing, grasping, twisting and pulling force. The physics forceps implement a first-class lever, creep and the type of force that provides a mechanical advantage making it more efficient. It has two handles one of which is connected to a bumper that functions as the fulcrum during extraction. The bumper is most often placed on facial aspect of the dental alveolus typically at the mucogingival junction. The other beak is applied to the palatogingival aspect of the tooth into the gingival sulcus, at a lower level than the bumper. The force applied by the bumper onto the gingival and the bone is distributed over the larger surface area and is compressive force, so the tooth and the alveolus do not fracture. Once the tooth is subluxated, it can be delivered with conventional forcep. Once the instrument is properly placed, pressure is slowly applied using wrist movement only [7].
The physics forceps technique applies a steady rotational torque to the periodontal ligament quantitatively creating the release of hyaluronidase in a shorter period of time than traditional forceps. It not only reduces patient’s postoperative discomfort but also maintains the socket integrity by not disturbing the soft tissue and hard tissue architecture, thus making future prosthesis replacement easier.
The aim of this study was to evaluate the efficacy of physics forceps versus conventional forceps in non-surgical orthodontic extractions of bilateral premolars and to compare the outcome variables between the two techniques (Figs. 1, 2, 3).
Fig. 1.

Physics forceps
Fig. 2.
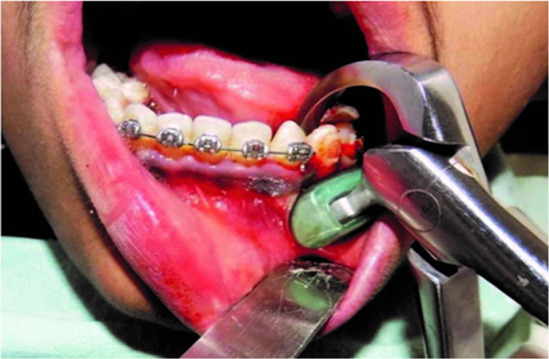
Use of physics forceps in the mandibular arch
Fig. 3.

Use of physics forceps in the maxillary arch
Material and Methods
The present study included 50 patients who reported to the Department of Oral and Maxillofacial Surgery for the bilateral removal of upper and lower premolars. Patients were selected irrespective of gender, cast, creed and socioeconomic status. All subjects were informed about the procedure and the possible complications associated with the same. Informed consent was obtained from each patient, and the study received ethical clearance from the institution’s selection committee.
Inclusion Criteria
Patients belonging to age group between 14 and 25 years and patients requiring bilateral extraction of upper and lower premolars for orthodontic reasons are included.
Exclusion Criteria
Patients with history of systemic disease, periodontally weak teeth and carious premolars and teeth requiring transalveolar extractions were excluded from the study.
Methodology
The sample size was calculated using results of the pilot study on 10 upper premolars and 6 lower premolar teeth by the means of student t test paired using G Power (3.1 version). All the patients (n = 50) and total teeth (n = 200) were divided into two groups. Group I included teeth (n = 100) where extractions were carried out using physics forceps and Group II (n = 100) where extractions were carried out using conventional extraction forceps. Preoperative assessment included detailed case history and radiographic examination. (orthopantomogram or intraoral periapical x-ray of the tooth).
The extractions were carried out under strict aseptic conditions. In every patient, decision of extraction of tooth with particular forcep system (physics or conventional) was done by tossing a coin for the first extraction followed by alternate use of another system. Both the upper and lower premolars were extracted simultaneously as atraumatically as possible according to randomization, using physics forceps in both quadrants on one side and conventional extraction forceps in the other two quadrants of the opposite side. However, all extractions were done by same operator, using 1.8 ml of 2% lignocaine hydrochloride with 1:200,000 adrenaline solution {LOX × 2%( Neon Ltd)} for each extraction to provide anesthesia. Additional amount of local anesthesia if required was recorded. In case of physics forceps, beaks were placed on lingual/palatal aspect of tooth at or below cementoenamel junction, and bumper was placed on buccal alveolar ridge at mucogingival junction, and then a constant controlled traction force was given till the tooth was displaced out of the socket. In case of conventional extraction forceps after cutting the fibers that attach the gingival margin to neck of the tooth, the extraction forceps were placed as apically as possible and parallel to the long axis of the tooth. Then, the tooth was removed out of the socket by giving torsional movements combined with buccolingual rocking, for mandibular premolar and by gently wiggling the tooth in a buccopalatal direction while pulling maxillary premolar. The socket was compressed manually, and a gauze roll was placed. Patients were asked to bite on it for 45 min. All patients received Cap. Amoxicillin Trihydrate 500 mg t.d.s{Cipmox 500 mg (Cipla Ltd)} for 3 days and one tab Paracetamol {Dolo 650 mg (Micro Labs Ltd)} immediate postoperatively. They were asked to record the number of additional analgesic tablets taken to relieve pain on each day for 7 postoperative days. Identical postextraction instructions were given to all patients.
Intraoperative Assessment
Intraoperatively, the following parameters were evaluated:
Volume of anesthetic solution used (in ml). Alignment of premolar: well aligned or rotated premolars. The time taken was calculated after the injection of local anesthetic from the point of application of beaks on the tooth to the completion of extraction, in seconds using stopwatch. Any damage to the adjacent tooth/luxation of tooth or any fracture of the root/crown or cortical plate was noted.
Postoperative Assessment
Following parameters were assessed postoperatively:
Evaluation of postoperative pain—The patient rated postoperative pain on the day of extraction and subsequently at first, third and seventh postoperative day on a 10-cm long visual analog scale (VAS), and zero score on the VAS was recorded as ‘no pain,’ 1–3 as ‘mild pain,’ 4–6 as ‘moderate pain,’ 7–9 as ‘severe pain’ and 10 as ‘worst pain.’
-
(2)
Socket healing—Healing was evaluated postoperatively on third and seventh day on the basis of alveolar osteitis, acutely inflamed alveolus and acutely infected alveolus.
-
(3)
Soft tissue injury if any was examined and noted on third and seventh postoperative day.
-
(4)
Total consumption of analgesic tablets taken by the patient postoperatively for 7 days.
The data were statistically analyzed using SPSS version 20.0, and paired t test was applied to compare the mean time taken, pain score and analgesic consumption in both physics forceps and conventional extraction forceps groups for orthodontic extractions of bilateral maxillary and mandibular premolars.
Observations
Out of total 50 patients, 68% patients were below the age of 19 years. Thirty-two percent patients were in the age group of 20–25 years. The mean age of patients was 17.6 years with an age range of 14–25 years. Fourteen patients were male (28%) and 36 (68%) were female patients. The volume of local anesthetic solution used in both the groups was almost same, and no statistical significant difference was observed between Group I (physics forceps group) and Group II (conventional forceps group).
Regarding the alignment of teeth, 92 teeth in Group I and 94 teeth in Group II were well aligned in the arch. However, no difficulty was encountered while placing the bumper of physics forceps in cases of buccally placed teeth. The duration of extraction in 50 patients was noted at each appointment. The mean (SD) extraction time for both maxillary premolars and mandibular premolars in physics forceps group was less than conventional forceps group. This difference was found to be statistically significant (P = 0.001) (Table 1). The mean time taken for removal of maxillary premolars with fused roots/single root showed no statistically significant difference between the two groups (P = 0.151). However, the mean time taken for removal of maxillary premolars with flared roots and mandibular premolar with single root was significantly less in the physics forceps group as compared to those in the conventional group (Table 2).
Table 1.
Comparison of mean time taken for extraction
| Teeth | Group I (physics forceps group) Mean ± SD (in seconds) | Group II (conventional forceps group) Mean ± SD (in seconds) | P value |
|---|---|---|---|
| Maxillary premolars | 36.26 ± 16.13 | 43.46 ± 18.92 | 0.001* |
| Mandibular premolars | 24.34 ± 9.58 | 29.30 ± 10.49 | 0.001* |
SD standard deviation
NS: P > 0.05; Not Significant; *P < 0.05; Significant
Table 2.
Mean time taken for extraction of premolars with flared/fused roots
| Teeth | Morphology of roots | Number of teeth | Forceps | Time taken Mean ± SD (in seconds) | P value |
|---|---|---|---|---|---|
| Maxillary | Fused/single | 30 | Physics | 34.23 ± 14.73 | 0.151NS |
| 30 | Conventional | 38.97 ± 16.26 | |||
| Flared | 20 | Physics | 39.30 ± 17.99 | 0.006* | |
| 20 | Conventional | 49.00 ± 22.02 | |||
| Mandibular | Single | 50 | Physics | 24.34 ± 9.58 | 0.001* |
| 50 | Conventional | 29.30 ± 10.49 |
SD standard deviation
NS: P > 0.05; Not significant *P < 0.05; Significant
Three percent roots were fractured at the apical third in physics forceps group as compared to 2% roots in conventional forceps group. However, there were no complaints of fractured alveolus, dry socket, delayed healing or postoperative infection in both the groups.
There was no statistically significant difference in the mean pain score as evaluated on visual analog scale (VAS) between the two groups on day of extraction, first, third and seventh postoperative day. However, on the first postoperative day, pain score was slightly higher in physics forceps group (3.04 ± 1.476), as compared to conventional forceps group (2.89 ± 1.210) (Table 3). Regarding the soft tissue injury, ulcer formation was observed on third postoperative day in two cases of Group I due to the excessive pressure applied by the bumper on the buccal aspect. These ulcers were healed as observed on seventh postoperative day.
Table 3.
Comparison of mean pain score
| VAS score | Group I (physics forceps group) Mean ± SD | Group II (conventional forceps group) Mean ± SD | P value |
|---|---|---|---|
| Day of extraction | 4.33 ± 1.719 | 4.31 ± 1.505 | 0.927NS |
| First postoperative day | 3.04 ± 1.476 | 2.89 ± 1.210 | 0.513NS |
| Third postoperative day | 1.11 ± 1.071 | 1.24 ± .957 | 0.349NS |
| Seventh postoperative day | 0.29 ± 0.506 | .22 ± .471 | 0.445NS |
SD: standard deviation
NS: P > 0.05; Not significant *P < 0.05; Significant
Statistically, there was no significant difference between the two groups regarding the number of analgesic tablets taken over a period of 7 days (P = 0.522).
The total volume of anesthetic solution used in both groups and the total number of analgesic tablets taken in each group are given in Table 4.
Table 4.
Comparison of volume of local anesthesia (in ml)
| Teeth | Group I (physics forceps group) Mean ± SD (in ml) | Group II (conventional forceps group) Mean ± SD (in ml) | P value |
|---|---|---|---|
| Maxillary premolars | 1.87 ± 0.14 | 1.86 ± 0.09 | 0.704NS |
| Mandibular premolars | 1.88 ± 0.14 | 1.84 ± 0.08 | 0.056NS |
SD: standard deviation
NS: P > 0.05; Not Significant; *P < 0.05; Significant
Discussion
Tooth extraction requires controlled forces for atraumatic extractions, which helps in preserving bone, gingival architecture and allows for option of future or immediate dental implant placement.
According to the basic principle of extractions, the forces applied to the handles are the long side of the lever, the beaks on the tooth are short side of the lever, and the hinge acts as a fulcrum. Hence, the force on the handles is magnified to allow the forceps to grasp the tooth with a great force. The second principle involves placement of the beaks of the forceps as parallel as possible to long axis of the tooth Misch and Perez [6]. Conventional forceps work by forces placed equally on the facial and lingual portion of the tooth and elevating it out of the socket by movement of the operators arm and wrist. Traditional extraction methods may result in gingival tissue laceration to complete loss of buccal bony plate and interdental bone crest Madathanpalli et al. [8]. Other complications involve trismus, dry socket, postoperative pain and if the bony dehiscence exists apical to the free gingival margin or the labial bone is very thin, then it may undergo significant resorption during natural healing process of socket Mandal et al. [9].
‘Physics forceps’ were developed by Dr. Richard Golden in 2004. The extraction technique differs from any other extraction technique in that the buccal portion of the forceps is not a beak, but rather a plastic-covered bumper which is placed apically in the vestibule, creating a more efficient class I lever system Madathanpalli et al. [8].
The length of the forceps handle to the bumper is 8 cm and the torque force that is generated on the tooth, periodontal ligament and bone is related to this, divided by the distance from the bumper to the beak of the forceps (1 cm). The force that is applied on the handle attached to the bumper increases the force on the tooth, periodontal ligament and bone by about 8 times. It is a compressive force, so the tooth and alveolus do not fracture Hariharan et al. [10]. When the periodontal ligament is traumatized with forceps, hyaluronidase is released. Hence, Physics forceps with its steady unrelenting of trauma to the periodontal ligament create a greater release of hyaluronidase than traditional forceps or elevator extraction because trauma from those techniques is intermittent Misch and Perez [6]. Once the tooth is subluxated, it can be delivered with the help of conventional forceps or a rongeur.
Physics forceps require constant traction force involving only unidirectional force for extraction, while conventional forceps involve buccal and lingual directing force to luxate the tooth followed by twisting or rotating force depending on the tooth to be removed which can increase the intraoperative time Patel et al. [11]. The biomechanics of the instrument reduces stress placed on fragile root structure, which helps in maintaining the facial plate of bone. When interseptal bone and the facial plate are maintained, the entire process of grafting and placing an immediate dental implant becomes more predictable.
According to Dym and Weiss, there is no need to raise a mucoperiosteal flap or use an elevator before attempting extraction with the physics forceps. This is a major advantage, particularly in cases that require atraumatic extraction Hariharan et al. [10].
We chose a split-mouth study design, because it has fewer chances of bias, as so many variables (such as nutritional status, oral hygiene and quality of bone) were same on both sides, and the patient’s compliance was constant. There was no operator bias as the same surgeon operated on both sides of each patient.
The mean age of patients taken in present study was 17.6 years (range 14–25 years). Out of which 14 were male patients and 36 female patients. Similarly, Hariharan et al. [10] in their study on orthodontic extractions of maxillary premolars had mean age of patients as 16 years with the range 11–23 years, of which 15 were female patients and 12 male patients. Madathanpalli et al. [8] in their study on 30 patients for removal of maxillary first molar had a mean age of patients as 36.53 years in physics forceps group and 38.35 years in conventional forceps group which was quite high as compared to the present study (mean age 17.6 years).
Volume of anesthetic solution used in the present study was 1.8 ml in all patients for extraction of maxillary and mandibular premolars, similar to that reported by Hariharan et al. [10].
The mean time taken in present study for extraction of maxillary and mandibular premolars was 36.26 ± 16.13 s and 24.34 ± 9.58 s, respectively, in Group I and 43.46 ± 18.92 s and 29.30 ± 10.49 s in Group II. Statistically, there was significant difference between the two groups. This is due to the steep learning curve of physics forceps which requires accurate placement of the forceps and the bumper on the buccal aspect of alveolus. Once the operator is familiar with the placement of the forceps, movement of the wrist and direction of force applied, the process of extraction becomes easier and faster. Lingaraj et al. [12] who in their study on 12 patients for extraction of bilateral upper premolars reported significant difference in the mean time taken for tooth extraction using physics forceps (131.75 s) as compared to conventional forceps (295.71 s). Patel et al. [11] in their study on orthodontic extractions of bilateral upper and lower premolars (n = 42) recorded less operating time in case of physics forceps which was 58.8 (± 48.13) seconds as compared to conventional forceps 88.33 (± 35.59) seconds.
The mean time taken for removal of maxillary premolars with flared roots and mandibular premolars with single root was found to be less in physics forceps group than conventional forceps group.
Postoperative pain was recorded which was slightly higher in physics forceps group (3.04 ± 1.476), as compared to conventional forceps group (2.89 ± 1.210) on first postoperative day. However, there was no statistically significant difference in the mean pain score as evaluated on visual analog scale (VAS) [13] between the two groups on day of extraction, first, third and seventh postoperative day.
Similarly, Patel et al. [11] reported no statistically significant difference between physics and conventional forceps in the VAS score on the first and third postoperative days. Lingaraj et al. [12] and Mandal et al. [9] also found significantly less pain with the use of physics forceps on first and third postoperative days. Hariharan et al. [10] recorded lower pain on first day postoperatively, whereas Madathanpalli et al. [8] reported lesser pain on third postoperative day with the use of physics forceps. The authors attributed this to the working mechanism of physics forceps, which allows the tooth to be removed atraumatically unlike conventional forceps, thus reducing trauma at surgical site and pain in the early postoperative period.
The mean analgesic consumption during the 7 postoperative days indicated no statistically significant difference between the two groups, in accordance with the studies of Patel et al. [11] and Madathanpalli et al. [8] who showed minimal postoperative analgesic requirement.
Reported post-operative complications range from acutely inflamed sockets, dry socket formation, buccal cortical plate fractures crown fractures, luxation or damage to adjacent teeth [14, 15]. Socket healing was assessed on the basis of alveolar osteitis, acutely inflamed alveolus and acutely infected alveolus in all the patients in the present study. However, it remained uneventful in both the groups as observed on third and seventh postoperative day. No patient reported with dry socket, crown fracture, and bleeding with either of the techniques.
In our study 3 patients (6%) in physics group and 2 patients (4%) in conventional forceps group had root fracture at apical third because of sudden curvature at the root tip. The fractured root fragments were removed using bur window technique. Hariharan et al. [10] reported fracture of buccal root above the middle third with the use of conventional extraction forceps, whereas Patel et al. [11] also reported root tip fractures in two teeth using conventional forceps which was not seen in any case of Physics forceps. El-Kenawy et al. [16] also reported (8.5%) root fractures in physics forceps group and (16.6%) in conventional forceps group.
The buccal cortical plate is comparatively weaker and usually fractures due to inadvertent forces applied by operator or by application of excessive forces. However, in the present study there was no case of buccal cortical plate fracture. Lingaraj et al. [12] in their study on 12 patients reported cortical plate fracture in 5 cases of conventional forceps group only. Patel et al. [11] found fracture of buccal cortical plate in 2 cases of physics forceps group. El-Kenawy et al. [16] in their study on 200 patients reported bone plate fracture in 3 cases in physics forceps group and 7 cases in conventional forceps group.
Design of physics forceps is such that forces are applied on buccal gingiva through bumper which contributes to the crushing injury. In this study regarding the soft tissue injury, ulcer formation was observed on third postoperative day in two cases of Group I due to the excessive pressure applied by the bumper on the buccal aspect. These ulcers healed as observed on seventh postoperative day, while in Group II none of the cases reported with ulcer formation postoperatively. Lingaraj et al. [12] also reported gingival laceration in one patient of physics forceps group and eleven patients of conventional forceps group. The authors reported lacerations on buccal mucosa where bumper of Physics forceps was placed for extraction of teeth in the upper arch.
Conclusion
A pair of physics forceps has been devised for the atraumatic extraction of teeth especially those which need implant placement. Although it has a definite learning curve, but once the operator becomes familiar with its functioning, the process becomes simple. This study concluded that the physics forceps take less time for extraction with minimal or no damage to soft tissue while maintaining the integrity of the socket. The present study was limited to orthodontic extraction, and hence more multicentric prospective trials with a larger sample size including multirooted teeth, root stumps and grossly decayed teeth need to be carried out.
Compliance with Ethical Standards
Conflict of interest
All authors have declared that they have no conflict of interest.
Human and Animal Rights
Research involving human participants and/or animals—yes.
Informed Consent
Yes.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Sarika Kapila, Email: sarikakapila@yahoo.com.
Tejinder Kaur, Email: tkgumber@gmail.com.
Ramandeep Singh Bhullar, Email: ramandeepbhullar@rediffmail.com.
Amneet Sandhu, Email: sandhuamneet@yahoo.com.
Amit Dhawan, Email: surg.amit@gmail.com.
References
- 1.Ahel V, Ćabov T, Špalj S, Perić B, Jelušić D, Dmitrašinović M. Forces that fracture teeth during extraction with mandibular premolar and maxillary incisor forceps. Br J Oral Maxillofac Surg. 2015;53(10):982–987. doi: 10.1016/j.bjoms.2015.08.007. [DOI] [PubMed] [Google Scholar]
- 2.White J, Holtzclaw D, Toscano N. Powertome assisted atraumatic tooth extraction. J Implant Adv Clin Dent. 2009;6:35–44. [Google Scholar]
- 3.Weiss A, Stern A, Dym H. Technological advances in extraction techniques and outpatient oral surgery. Dent Clin N Am. 2011;55:501–513. doi: 10.1016/j.cden.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 4.Stübinger S, Kuttenberger J, Filippi A, Sader R, Zeilhofer HF. Intraoral piezosurgery: preliminary results of a new technique. J Oral Maxillofac Surg. 2005;63(9):1283–1287. doi: 10.1016/j.joms.2005.05.304. [DOI] [PubMed] [Google Scholar]
- 5.Muska E, Walter C, Knight A, Taneja P, Bulsara Y, Hah M, Desai M, Dietrich T. Atraumatic vertical tooth extraction: a proof of principle clinical study of a novel system. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116(5):e303–e310. doi: 10.1016/j.oooo.2011.11.037. [DOI] [PubMed] [Google Scholar]
- 6.Misch CE. Perez HM (1998) Atraumatic extraction: a biomechanical rationale. Dent Today. 2008;27(8):100–101. [PubMed] [Google Scholar]
- 7.Pilare K. Physics forceps-a new revolution in exodontia. Int J Curr Res. 2017;9(05):51218–51220. [Google Scholar]
- 8.Madathanapalli S, Surana S, Thakur D, Ramnani P, Kapse S. Physics forceps vs conventional forceps in extraction of maxillary first molar. Int J Oral Care Res. 2016;4(1):29–32. doi: 10.5005/jp-journals-10051-0008. [DOI] [Google Scholar]
- 9.Mandal S, Gupta S, Mittal A, Garg R. Collate on the ability of physics forceps v/s conventional forceps in multirooted mandibular tooth extractions: a randomized control trial. J Dent Med Sci. 2015;14(3):63–66. [Google Scholar]
- 10.Hariharan S, Narayanan V, Soh CL. Split-mouth comparison of Physics forceps and extraction forceps in orthodontic extraction of upper premolars. Br J Oral Maxillofac Surg. 2014;52:137–140. doi: 10.1016/j.bjoms.2014.06.013. [DOI] [PubMed] [Google Scholar]
- 11.Patel HS, Managutti AM, Menat S, Agarwal A, Shah D, Patel J. Comparative evaluation of efficacy of Physics forceps versus Conventional Forceps in orthodontic extractions: A prospective randomized split mouth study. J Clin Diagn Res. 2016;10(7):ZC41–ZC45. doi: 10.7860/JCDR/2016/17724.8160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lingaraj J, Balihallimathm DS, Inamdar A. Comparison of physics forceps and conventional extraction forceps in orthodontic extraction of upper premolars. Int J Recent Sci Res. 2017;8(8):19149–19152. [Google Scholar]
- 13.Bijur PE, Silver W, Gallagher EJ. Reliability of the Visual Analog Scale for measurement of acute pain. Acad Emerg Med. 2001;8(12):1153–1157. doi: 10.1111/j.1553-2712.2001.tb01132.x. [DOI] [PubMed] [Google Scholar]
- 14.Blum IR. Contemporary views on dry socket (alveolar osteitis): a clinical appraisal of standardization, aetiopathogenesis and management: a critical review. Int J Oral and Maxillofac Surg. 2002;31(3):309–317. doi: 10.1054/ijom.2002.0263. [DOI] [PubMed] [Google Scholar]
- 15.Oginni FO, Fatusi OA, Alagbe AO. A clinical evaluation of dry socket in a Nigerian teaching hospital. J Oral Maxillofac Surg. 2003;61(8):871–879. doi: 10.1016/S0278-2391(03)00248-9. [DOI] [PubMed] [Google Scholar]
- 16.El-Kenawy MH, Ahmed WM. Comparison between physics and conventional forceps in simple dental extractions. J Maxillofac Oral Surg. 2015;14(4):949–955. doi: 10.1007/s12663-015-0765-6. [DOI] [PMC free article] [PubMed] [Google Scholar]