

Abstract
Background and Aim
Celiac disease (CD) is a chronic autoimmune enteropathy triggered by ingested gluten in genetically predisposed individuals. Although common in Europe and the United States, cases of CD are rarely encountered in East Asia, including Japan, and its prevalence remains to be fully evaluated in a large‐scale study. We previously investigated the presence of CD in adults in Japan, which revealed a low prevalence of 1 (0.05%) of 2008 nonclinical subjects, while 1 (2.1%) of 47 symptomatic patients was diagnosed based on serology and duodenal histopathology results. To confirm those results, we conducted an additional retrospective serological screening study of adults in Japan.
Methods
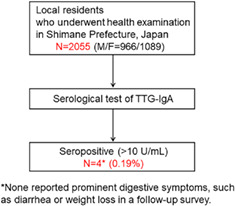
Serum samples were collected from 2055 adults who underwent a health examination in four local areas of Shimane prefecture in Japan from July 2008 to August 2013. As a screening test for CD, the antitissue transglutaminase IgA antibody (TTG) titer was determined in all subjects, and a value greater than 10 U/mL was considered to be evidence of CD.
Results
Of the 2055 subjects, 4 (0.19%) showed a high concentration of TTG. Although two of the four who were seropositive had died at the time of this retrospective study, none reported prominent digestive symptoms such as diarrhea or weight loss in a follow‐up survey.
Conclusions
Among a general population in Japan, a positive rate of serological tests for CD was noted in 0.19%, indicating quite a low presence, consistent with our previous results.
Keywords: antitissue transglutaminase IgA, celiac disease, Human leukocyte antigen, prevalence
Previous studies suggested that the prevalence of celiac disease (CD) in Japan is still quite low as compared to Western countries. To confirm the findings, in the present investigation we conducted an additional retrospective serological screening study of 2055 adults different from those in the previous cohort. Among a general population in Japan, positive rate of serological test for CD was noted in 0.19%, indicating a quite low presence and consistent with our previous results.
Introduction
Celiac disease (CD), an immune‐mediated disorder induced by ingestion of gluten in genetically susceptible individuals, is common in Europe and the United States, with a prevalence rate estimated to be as high as 1%.1, 2, 3 On the other hand, CD is still considered to be rare or nonexistent in East Asian countries, including China, Mongolia, Korea, and Japan, likely due to limited consumption of a gluten‐containing diet, as well as lower prevalence of the CD‐susceptible HLA types HLA‐DQ2 and DQ8.1, 4 We previously investigated the presence of CD in 2008 nonclinical adults and 47 symptomatic patients in Japan and found that 4 (0.2%) of the nonclinical adult population were positive for the serum antitissue transglutaminase IgA antibody (TTG), a CD‐specific autoantibody known to be highly sensitive and specific for diagnosis.5 Of those four subjects, one had HLA‐DQ8 but no histological changes in duodenal mucosal biopsy results, while another who did not possess a susceptible HLA type was finally diagnosed with CD based on histopathological findings of the duodenum. Furthermore, 2 (4.3%) of 47 symptomatic patients with unexplained abdominal symptoms were seropositive, of whom 1 (2.1%) was finally diagnosed with CD based on duodenum histopathological findings.
Those previous results suggested that the incidence of CD in Japan is still quite low compared to Western countries. To confirm the findings, in the present investigation, we conducted an additional retrospective serological screening study of 2055 adults different from those in the previous cohort.
Methods
A total of 2055 local residents who underwent health examinations from July 2008 to August 2013 in four local areas of Shimane Prefecture (Izumo City, Unnan City, Ohnan Town, and Okinoshima Town) in Japan were included. Serum samples were obtained from each of the subjects after fasting and were stored at −30°C until the assay. An assay to determine the presence of TTG was conducted using an ORG 540A Anti‐Tissue‐Transglutaminase IgA ELISA Kit (ORGENTEC Diagnostika GmbH, Germany) according to the instructions of the manufacturer. This test quantitatively determines the concentration of the antihuman tissue IgA antibody TTG.6 The cut‐off value is 10 U/mL, and individuals with a greater concentration are diagnosed as possible cases of CD. Thereafter, a follow‐up survey of subjects who had positive results in the serological test was performed by examining medical records and their general condition.
This study was a part of a cohort study conducted by the Center for the Community‐based Healthcare Research and Education, Shimane University (Shimane CoHRE Study).7, 8 Written informed consent was obtained from each participant. The protocol was approved by the Ethical Committee of Shimane University School of Medicine, and the study was carried out in accordance with the principles of the Helsinki Declaration.
Results
Of the 2055 enrolled subjects, 966 were male, and 1089 were female, while their median age was 67.0 years (range 20–94 years) (Table 1). Four subjects showed a high TTG titer (>10 U/mL), indicating that the presence of CD based on serologic test findings among the local population was 0.19%. Three of four seropositive subjects were male, and their median age was 66.5 years (range 38–90 years). Two of the seropositive patients had died by the time this study was conducted. None of the four had prominent digestive symptoms, such as diarrhea or weight loss, noted in a follow‐up survey (Table 2). Cases 1, 3, and 4 had no significant abnormal serological findings, including albumin and C‐reactive protein (CRP), while hypoalbuminemia with an elevated level of serum gamma‐glutamyltranspeptidase was noted in Case 2, who had been treated for alcoholic liver disease. Because this was a retrospective serological screening study, no histological examinations of duodenal mucosa or HLA typing were conducted; thus, we could not confirm a CD diagnosis in any of the subjects. Nevertheless, the findings indicate that the presence of CD remains quite low among the general adult population in Japan.
Table 1.
Clinical characteristics of enrolled subjects
| Seronegative | Seropositive | |
|---|---|---|
| Number | 2051 | 4 |
| Gender (male/female) | 963/1088 | 3/1 |
| Median age (years) (range) | 67 (20–94) | 66.5 (38–90) |
| TTG test (U/mL), mean ± SD | 1.16 ± 0.97 | 12.99 ± 0.85 |
TTG, tissue transglutaminase.
Table 2.
Demographic and clinical characteristics of four subjects positive for tissue transglutaminase
| Case 1 | Case 2 | Case 3 | Case 4 | |
|---|---|---|---|---|
| Age (years) | 38 | 56 | 90 | 77 |
| Gender | Male | Male | Male | Female |
| TTG IgA titer (U/mL) | 13.4 | 11.3 | 13.2 | 12.8 |
| Status at time of study | Alive | Dead | Dead | Alive |
| BMI (kg/m2) | 21.5 | 17.3 | 21.9 | 19.2 |
| Albumin (g/dL) | 4.3 | 2.8 | 3.6 | 3.9 |
| CRP (mg/dL) | 0.02 | 0.12 | 0.09 | 0.08 |
BMI, body mass index; CRP, C‐reactive protein; TTG, tissue transglutaminase.
Discussion
The prevalence of CD has been increasing recently, especially in Western countries, due to recognition of characteristics of the disease and increased reliability of serological testing,2, 9, 10 although the disease is considered to be extremely rare in Japanese populations. To date, only a few case reports from Japan have been presented,11, 12 while only three studies have been published regarding the prevalence of CD in Japanese general populations.5, 13, 14 The first study, reported by Nakazawa, et al., showed a seropositive rate assessed by the presence of TTG of 2.8% and a histological prevalence of CD of 0.98% in 710 patients, including malignant lymphoma, gastroduodenal ulcer, and leukemia cases, whereas none of the 239 healthy subjects were found to be seropositive.13 The next study, performed by Watanabe et al., found a seropositive rate as assessed by TTG of 12.8% in 172 patients with inflammatory bowel diseases and of 1.6% in 190 healthy subjects, although none in that latter group were finally diagnosed with CD based on duodenal mucosa histological examination findings.14 In our previous study, the seropositive rate for TTG was shown to be 0.2% in 2008 nonclinical subjects, and only a single case (0.05%) was finally diagnosed with CD based on histological examination findings of duodenal mucosa.5 Consistent with those results, the present study showed that a seropositive rate for TTG was 0.19% in 2055 local residents, suggesting that its presence in healthy subjects in Japan ranges from 0 to 1.6%, and the histological prevalence is as low as 0.05%.
A few studies regarding the prevalence of CD in other East Asian countries, including Mongolia and Korea, have been presented.4, 15, 16 It is possible that CD is more common than previously recognized in China.17 In 2015, Wang et al. reported a seropositive rate of 1.77% and five cases (1.01%) diagnosed with CD among 395 adult Chinese patients with diarrhea‐predominant irritable bowel syndrome (IBS), while a seropositive rate of 0.55% was noted in 363 healthy control subjects, including 2 (0.28%) diagnosed with CD.18 More recently, Kou et al. found a prevalence of CD of 2.85% in 246 patients with IBS,19 suggesting that CD is not rare in Chinese populations. The reasons for the prevalence differences between China and other East Asian countries remain obscure, although it has been reported that the frequency of HLA‐DQ2 in China is higher at 5–20% compared to that in Japan and Korea at less than 1%.20 Moreover, the haplotype HLA‐DQA1*03‐ DQB1*03:03 (HLA‐DQ9.3), which is common in Chinese populations but has a low frequency in Caucasians, is thought to be a factor related to CD susceptibility in China.18
In addition to the low prevalence of HLA‐DQ genotypes leading to susceptibility for CD, the dietary intake of wheat in Japan is still half of what has been observed in China, although the consumption of these products has been increasing along with a more Western diet in the past few decades.4 However, larger screening and genetic studies conducted in different regions in Japan are needed to confirm the precise prevalence of CD in symptomatic, as well as healthy, individuals.
Grain food consumption is a known trigger of gluten‐related disorders such as CD, as well as nonceliac gluten sensitivity (NCGS) and wheat allergy.21, 22 A typical clinical presentation of NCGS includes intestinal and/or extraintestinal symptoms related to the ingestion of gluten‐containing grains, similar to IBS and CD, although with symptomatic improvement upon their withdrawal. NCGS is considered to be mainly determined based on a “diagnosis of exclusion” due to the lack of validated biomarkers and histopathological criteria for confirmation of the condition. Although antigliadin IgG has been reported to be positive in 50% of NCGS patients,23 that antibody is not specific for NCGS. Unfortunately, no informative studies are known to have been conducted in East Asia, including Japan, regarding NCGS prevalence. There is a possibility of increased numbers of patients of NGCS along with increasing wheat consumption in Japan, and a nationwide study is needed to investigate the precise prevalence and clinical presentation of gluten sensitivity in Japanese populations.
This study has some limitations. Serological testing targeted TTG only and cases with a high TTG level were not confirmed by a histological examination of duodenal mucosa or HLA typing. We contacted two alive individuals who were positive for TTG and recommended endoscopy and HLA typing, but consent was not obtained.
In conclusion, the positive rate of serological tests for CD was 0.19% in nonclinical adults, indicating that the presence of CD in Japan remains quite low, consistent with the results of our previous study.
Acknowledgments
The authors thank Keiko Masuzaki of the Shimane University School of Medicine for excellent technical assistance.
Declaration of conflict of interest: None
References
- 1. Kang JY, Kang AH, Green A, Gwee KA, Ho KY. Systematic review: worldwide variation in the frequency of coeliac disease and change over time. Aliment. Pharmacol. Ther. 2013; 38: 226–45. [DOI] [PubMed] [Google Scholar]
- 2. Lionetti E, Gatti S, Pulvirenti A, Catassi C. Celiac disease from a global perspective. Best Pract. Res. Clin. Gastroenterol. 2015; 29: 365–79. [DOI] [PubMed] [Google Scholar]
- 3. Al‐Bawardy B, Codipilly DC, Rubio‐Tapia A, Bruining DH, Hansel SL, Murray JA. Celiac disease: a clinical review. Abdom Radiol. 2017; 42: 351–60. [DOI] [PubMed] [Google Scholar]
- 4. Cummins AG, Roberts‐Thomson IC. Prevalence of celiac disease in the Asia‐Pacific region. J. Gastroenterol. Hepatol. 2009; 24: 1347–51. [DOI] [PubMed] [Google Scholar]
- 5. Fukunaga M, Ishimura N, Fukuyama C et al Celiac disease in non‐clinical populations of Japan. J. Gastroenterol. 2018; 53: 208–14. [DOI] [PubMed] [Google Scholar]
- 6. Fernandez E, Riestra S, Rodrigo L et al Comparison of six human anti‐transglutaminase ELISA‐tests in the diagnosis of celiac disease in the Saharawi population. World J. Gastroenterol. 2005; 11: 3762–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hamano T, Kimura Y, Takeda M et al Effect of Environmental and Lifestyle Factors on Hypertension: Shimane COHRE Study. PLoS One. 2012; 7: e49122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kohno K, Niihara H, Hamano T et al J‐curve association between alcohol intake and varicose vein in Japan: the Shimane CoHRE Study. J. Dermatol. 2019; 46: 902–6. [DOI] [PubMed] [Google Scholar]
- 9. Murray JA, Van Dyke C, Plevak MF, Dierkhising RA, Zinsmeister AR, Melton LJ III. Trends in the identification and clinical features of celiac disease in a north American community, 1950‐2001. Clin. Gastroenterol. Hepatol. 2003; 1: 19–27. [DOI] [PubMed] [Google Scholar]
- 10. West J, Fleming KM, Tata LJ, Card TR, Crooks CJ. Incidence and prevalence of celiac disease and dermatitis herpetiformis in the UKover two decades: population‐based study. Am. J. Gastroenterol. 2014; 109: 757–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Makishima H, Ito T, Kodama R et al Intestinal diffuse large B‐cell lymphoma associated with celiac disease: a Japanese case. Int. J. Hematol. 2006; 83: 63–5. [DOI] [PubMed] [Google Scholar]
- 12. Freeman HJ. Biopsy‐defined adult celiac disease in Asian‐Canadians. Can. J. Gastroenterol. 2003; 17: 433–6. [DOI] [PubMed] [Google Scholar]
- 13. Nakazawa H, Makishima H, Ito T et al Screening tests using serum tissue transglutaminase IgA may facilitate the identification of undiagnosed celiac disease among Japanese population. Int. J. Med. Sci. 2014; 11: 819–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Watanabe C, Komoto S, Hokari R et al Prevalence of serum celiac antibody in patients with IBD in Japan. J. Gastroenterol. 2014; 49: 825–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Poddighe D, Rakhimzhanova M, Marchenko Y, Catassi C. Pediatric celiac disease in central and east asia: current knowledge and prevalence. Medicina (Kaunas). 2019; 55: E11. 10.3390/medicina55010011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Makharia GK. Celiac disease screening in southern and East Asia. Dig. Dis. 2015; 33: 167–74. [DOI] [PubMed] [Google Scholar]
- 17. Yuan J, Gao J, Li X et al The tip of the "celiac iceberg" in China: a systematic review and meta‐analysis. PLoS One. 2013; 8: e81151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Wang H, Zhou G, Luo L et al Serological screening for celiac disease in adult Chinese patients with diarrhea predominant irritable bowel syndrome. Medicine (Baltimore). 2015; 94: e1779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Kou GJ, Guo J, Zuo XL et al Prevalence of celiac disease in adult Chinese patients with diarrhea‐predominant irritable bowel syndrome: A prospective, controlled, cohort study. J. Dig. Dis. 2018; 19: 136–43. [DOI] [PubMed] [Google Scholar]
- 20. Saito S, Ota S, Yamada E, Inoko H, Ota M. Allele frequencies and haplotypic associations defined by allelic DNA typing at HLA class I and class II loci in the Japanese population. Tissue Antigens. 2000; 56: 522–9. [DOI] [PubMed] [Google Scholar]
- 21. Leonard MM, Sapone A, Catassi C, Fassano A. Celiac disease and nonceliac gluten sensitivity: a review. JAMA. 2017; 318: 647–56. [DOI] [PubMed] [Google Scholar]
- 22. Elli L, Branchi F, Tomba C et al Diagnosis of gluten related disorders: Celiac disease, wheat allergy and non‐celiac gluten sensitivity. World J. Gastroenterol. 2015; 21: 7110–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Volta U, Tovoli F, Cicola R et al Serological tests in gluten sensitivity (nonceliac gluten intolerance). J. Clin. Gastroenterol. 2012; 46: 680–5. [DOI] [PubMed] [Google Scholar]