

Abstract
This study tested the skin-deep resilience hypothesis - that low socioeconomic status (SES) youth who are working hard to succeed in life experience good psychological and educational outcomes but at a cost to their physical health - in a sample of monozygotic (MZ) twins. The National Longitudinal Study of Adolescent Health (Add Health) contained a sample of 226 MZ twin pairs at Wave 1 (M age=16 years), of whom 141 pairs completed the Wave 4 assessment 13 years later (M age=29 years). Family SES was measured at Wave 1 via income, education, and occupation. Conscientiousness was measured at Wave 4 as an indicator of those who were working hard to succeed in life. Outcomes measured at Wave 4 included low-grade inflammation (C-reactive protein, CRP), mental health (depression, problematic alcohol use), and academic success (educational attainment). A co-twin control design was utilized which directly compared within-twin differences in the association between conscientiousness and life outcomes. Main effects of between-twin conscientiousness were found such that higher levels of conscientiousness were associated with higher educational attainment, fewer symptoms of depression, and less problematic alcohol use, across all SES groups. An interaction between family SES and within-twin difference in conscientiousness was found for CRP, such that, among twins growing up in lower SES households, the twin with higher levels of conscientiousness had higher levels of CRP. These patterns provide support for the phenomenon of skin-deep resilience using a twin methodology that reduces the possibility of confounding by shared genetic and environmental factors.
Keywords: conscientiousness, inflammation, socioeconomic status, twin study
INTRODUCTION
A substantial minority of youth who grow up under economic hardship achieve good outcomes in life, such as high levels of psychological well-being, occupational success, and high educational attainment, a phenomenon that has been termed resilience (Luthar, 2006; Masten, 2018). When youth attain such outcomes, they are generally thought to have successfully avoided the adverse consequences of poverty.
However, recent evidence suggests that some youth who are characterized as doing well by virtue of achieving academic success and good mental health, may actually be accruing costs of this success in terms of their physical health. For example, among youth of color from low-income neighborhoods, those who made it to college showed lower levels of substance use, but at the same time, higher levels of allostatic load (a multi-system indicator of physiological risk) compared to youth from low-income neighborhoods who did not make it to college (and compared to youth from high income neighborhoods in college) (Chen, Miller, Brody, & Lei, 2015). Similarly, low socioeconomic status (SES) youth of color who finished college reported lower levels of depression in their late 20s, but had a higher likelihood of metabolic syndrome, compared to low SES youth who did not go to college (and also compared to high SES youth who finished college) (Gaydosh, Schorpp, Chen, Miller, & Harris, 2018). This pattern has been termed ‘skin-deep resilience,’ reflecting the notion that above the skin, these youth appear to be doing well and achieving successes by external metrics, but below the skin, they are struggling physiologically in terms of their health.
One explanation for this phenomenon is that these low SES youth are attempting to overcome the obstacles and adversities they face in life by working hard to succeed academically. Their hard-driving work ethic is reflected in high levels of striving and self-control that help them achieve successes, but that also exact a toll on them physically, taxing physiological systems. In support of this idea, previous research has found interaction effects between SES and striving or self-control predicting health outcomes. For example, low-income youth of color who engaged in high levels of striving during adolescence were more likely to finish college, to earn higher incomes, and to have lower levels of depression in young adulthood compared to those with low levels of striving. However, these same youth were also more likely to develop diabetes by age 29, a pattern not evident in high-income youth (Brody, Yu, Miller, & Chen, 2016). Similarly, low-income youth of color who show high levels of self-control had lower levels of internalizing and externalizing problems, but higher levels of allostatic load and faster epigenetic aging (a measure of leukocyte DNA methylation profiles that reflects the discrepancy between a person’s biological and chronological age) compared to those with low levels of self-control (Brody et al., 2013; Miller, Yu, Chen, & Brody, 2015). In chronically ill populations, youth of color with asthma who exhibit high levels of self-control under stressful school conditions have better mental health but worse asthma inflammatory profiles compared to those with low levels of self-control (Chen et al., 2019).
Studies that have investigated related constructs have found similar patterns. For example, conscientiousness is a personality trait that encompasses being hard working, planful, careful, and self-controlled, with overlaps with the above constructs of self-control and striving. Interactions between SES and conscientiousness in previous research indicate that low SES adults of color who were high in conscientiousness had higher educational attainment and fewer symptoms of depression, but were more likely to develop a verified respiratory infection following viral challenge compared to those low on conscientiousness, with an opposite pattern for infection present in high SES adults (Miller, Cohen, Janicki-Deverts, Brody, & Chen, 2016). Similarly, low SES men of color who were high in conscientiousness had higher metabolic syndrome scores than those who were low in conscientiousness (Duggan, Jennings, & Matthews, 2019). Additionally, low SES adults of color who show high levels of high-effort coping, hard work, and a single-minded determination to succeed (John Henryism) evinced higher blood pressure and a greater risk of hypertension compared to those with low levels of John Henryism (James, Strogatz, Wing, & Ramsey, 1987; James, Keenan, Strogatz, Browning, & Garrett, 1992).
Taken together, these studies suggest the plausibility of the skin-deep resilience scenario. However, all of the above studies are observational, meaning that there could easily be unobserved factors inflating or accounting for the observed patterns. Twin designs represent one approach to minimizing the influence of such confounds, particularly ones that involve heritable genetic and shared familial influences. The discordant twin design is an especially useful method in this regard (McGue, Osler, & Christensen, 2010). This design examines whether, within twin pairs, differences in an independent variable of interest are associated with the outcome of interest. When using monozygotic twins, this design controls for both shared genetic and shared environmental confounds. In the present study, we used monozygotic twins from a large, national study of adolescents to test skin-deep resilience hypotheses. As an outcome, we focused on a common biomarker of low-grade inflammation, C-reactive protein (CRP). Inflammation is thought to be one key pathway connecting childhood adversity to the development of multiple chronic diseases later in life (Miller, Chen, & Parker, 2011), and it plays an important role in the pathogenesis of cardiometabolic health problems including obesity, diabetes, and myocardial infarction (Hotamisligil, 2006; Ridker, 2007). CRP in particular has been prospectively associated with risk for Type 2 diabetes, coronary heart disease, and myocardial infarctions and strokes (Ridker, 2003; Ridker, Rifai, Cook, Bradwin, & Buring, 2005; Ridker, Hennekens, Buring, & Rifai, 2000; Pradhan, Manson, Rifai, Buring, & Ridker, 2001; Pradhan et al., 2002), and in children, CRP has been associated with adiposity, blood pressure, metabolic syndrome, carotid intima-media thickness, and lesions in the coronary artery (see (Balagopal et al., 2011) for an overview). Mirroring the findings in previous research (Miller et al., 2016; Brody et al., 2013; Brody et al., 2016), we hypothesized that there would be an interaction between family SES and within-twin conscientiousness. That is, among low SES twins, we expected the more conscientious one to evince higher CRP, whereas we hypothesized that this pattern would not be evident among high SES twins. Also mirroring previous research (Chen et al., 2019; Miller et al., 2015), we hypothesized there would be a divergence in physical versus mental health/academic outcomes, such that (unlike CRP) conscientiousness would be associated with better mental health (less depression, less substance use) and better educational attainment across all groups.
MATERIAL AND METHODS
Sample
The data were drawn from Waves 1 and 4 of the National Longitudinal Study of Adolescent Health (Add Health), a nationally representative sample of adolescents in grades 7 through 12 in the United States in 1995. Wave 1 (1994–1995) included 20,745 adolescents ages 11 to 20 years. The most recent wave of data collection (Wave 4, 2008) included 14,800 participants (71% of the original sample), when respondents were 24 to 32 years of age. The Add Health data include a subsample of 3,139 sibling pairs at Wave 1, including twins, full- or half-siblings, and adopted siblings (Harris, Halpern, Smolen, & Haberstick, 2006; Harris et al., 2009). For this study, we focus exclusively on monozygotic (MZ) twins (as the most stringent test of hypotheses, controlling for virtually all shared genetic and environmental factors). There were 226 MZ twin pairs enrolled in the study at Wave 1. In 85 of the original pairs, at least one twin was lost to attrition between Waves 1 and 4. The final sample consisted of 282 twins from 141 complete twin pairs. This sample included 176 (62.4%) individuals who self-identified as White with no Hispanic heritage, 52 (18.4%) as Black, 44 (15.6%) as Hispanic, and 10 (3.5%) as other race/ethnicities. The mean ages of the target twins were 16.3 years (SD = 1.48) at Wave 1 and 29.1 years (SD = 1.52) at Wave 4. This sample included 46.8% male, 53.2% female.
Measures
Family SES
At Wave 1, family SES was measured by a combination of parent education, parent occupation and total household income (Goodman, Slap, & Huang, 2003; Schwartz & Beaver, 2013). Parent education (of both parents if it was a two parent household) was reported by a parent and coded from 0 (no formal education) to 7 (professional training beyond 4 years in college). Codes were averaged for two parent households. Parents also reported their total household income before taxes. This measure was coded continuously in dollars (thousand). Youths were asked to identify their parents’ occupation from a list of 14 possible groupings ranging from 1 (farm/fishery worker) to 14 (professional/doctor/lawyer/scientist). Codes were averaged for two parent households. These three components were standardized and then summed to form the family SES composite.
Conscientiousness
Wave 4 of Add Health included a 20-item short-form version of the International Personality Item Pool (IPIP) (Donnellan, Oswald, Baird, & Lucas, 2006) designed to measure the Big Five factors of personality (not measured at Wave 1). The conscientiousness subscale included four items rated on a scale ranging from 1 (strongly agree) to 5 (strongly disagree), and was recoded such that higher scores indicated higher levels of conscientiousness.
Young Adult Academic and Mental Health Outcomes
Educational attainment.
At Wave 4 (~29 years old), participants reported their own educational attainment ranging from 1 (8th grade or less) to 13 (completed post baccalaureate professional education).
Depression.
At Wave 4, participants reported on depressive symptoms experienced in the past week on a 5-item version of the Center for Epidemiologic Studies - Depression (CES-D), with responses ranging from 0 (‘never or rarely’) to 3 (‘most of the time or all of the time’) (Perreira, Deeb-Sossa, Harris, & Bollen, 2005; Radloff, 1977). Higher scores indicated greater symptoms of depression.
Substance use (alcohol).
At Wave 4, participants were asked about lifetime history of alcohol use, binge drinking, and related problems, such as physical withdrawal when attempting to quit, and problems with family and friends, or at work, or within the legal system related to alcohol use (Hingson, Heeren, & Winter, 2006). Scores represented a count of problems, and ranged from 0 to 7.
Young Adult Low-Grade Inflammation
C-Reactive Protein (CRP).
At Wave 4, field researchers collected whole blood spots from a finger capillary prick onto filter paper that was dried, frozen, and assayed using an adapted sandwich ELISA method (for detailed documentation, see (Whitsel et al., 2012)). The sensitivity of the CRP assay was 0.035 mg/L, the within-assay coefficient of variation was 8.1%, and between-assay coefficient of variation was 11.0%. Because CRP’s distribution was skewed (skewness = 3.211, Kurtosis = 12.630), we used log-transformation to normalize the data (skewness = 0.735, Kurtosis = −0.047).
Covariates
Race:
At Wave 1, youth reported their race/ethnicity. Three dummy variables were created to reflect self-identification as (a) Black, non-Hispanic; (b) Hispanic, any race; and (c) any other race, non-Hispanic. The reference category included participants who self-identified as White, non-Hispanic. Multiracial participants were classified by their first choice of racial/ethnic category.
Gender:
Gender was coded as male (1) or female (0).
Age:
Participant age at Wave 1 was used as a covariate.
Plan of Analyses
This study used a co-twin control (CTC) design that has been previously employed to strengthen causal inference in observational twin research (Hamdi, South, & Krueger, 2016; Schwartz, 2017; Turkheimer & Harden, 2014). This design examines whether differences in an exposure variable (conscientiousness in this study) within twin pairs are associated with an outcome of interest (CRP and psychosocial outcomes). Briefly, this design provides estimates of both “between-family” and “within-family” effects. The “between-family” effects are similar to the effects estimated using traditional regression based techniques and provides an approximation of individual-level effects. The “within-family” effects estimates directly the effect on an outcome within twin pairs and hence controls for genetic and familial confounding. The rationale of the CTC design is that if conscientiousness causally influences CRP, then among MZ twin pairs who are discordant in levels of conscientiousness, the more conscientious twin should have higher CRP than his/her co-twin. In technical terms, the CTC design models the exposure variable (X) in terms of a “within-twin pair” regression coefficient (βw) and a “between-twin pair” regression coefficient . The Yij is the outcome for individual j within the twin pair i, Xij is the exposure variable for individual j within the twin pair i, and . is the mean of exposure variable for the twin pair i. All the analyses were run in SPSS (version 25), using generalized estimating equation (GEE) with robust standard errors and family was specified as a clustering variable to account for nonindependence of observations among twin pairs nested within families.
To examine the skin-deep resilience hypothesis, the GEE models included main effects of family SES (as a continuous variable), the mean levels of conscientiousness per twin pair (between-family effects), and each twin’s deviation from the pair’s mean (within-family effects or twin difference effects); as well as the two-way interaction terms of family SES × mean levels of conscientiousness and family SES × deviation of conscientiousness, with the family SES × deviation of conscientiousness term being the primary variable of interest. Gender, age, and race/ethnicity were included as covariates. We specified linear models for continuous outcomes of education attainment, depressive symptoms, and log-transformed CRP, and a Poisson model for the alcohol use outcome.
RESULTS
Preliminary Analyses
Table 1 presents descriptive statistics and Table 2 presents correlations among study variables for the entire sample. Family SES was negatively correlated with CRP and positively correlated with youths’ own educational attainment. In the sample as a whole, between-twin pair mean levels of conscientiousness were negatively correlated with young adult depressive symptoms and alcohol use, positively correlated with educational attainment, but not significantly correlated with CRP. In the sample as a whole, within-twin pair differences in conscientiousness were not associated with either CRP or psychosocial variables.
Table 1.
Sample characteristics (N = 282)
| Variables (wave) | n (%) or Mean (SD) | range |
|---|---|---|
| Gender (male) | 132 (46.8%) | - |
| Age (Wave 1) | 16.27 (1.48) | 13 – 19 |
| Age (Wave 4) | 29.14 (1.52) | 26 – 32 |
| Race/ethnicity | ||
| White, non-Hispanic | 176 (62.4%) | - |
| Black, non-Hispanic | 52 (18.4%) | - |
| Hispanic, any race | 44 (15.6%) | - |
| Other race | 10 (3.5%) | - |
| Family SES (Wave 1) | 0.087 (1.83) | −3.13 – 14.25 |
| Parent education | 4.08 (1.66) | 0 – 7 |
| Parent occupation | 9.20 (3.24) | 1 – 14 |
| Family income | 54.48 (81.17) | 0 – 800 |
| Mean conscientiousness (Wave 4) | 14.88 (2.17) | 8 – 20 |
| Deviation of conscientiousness (Wave 4) | 0 (1.58) | −5.5 – 5.5 |
| C-reactive protein (log-transformed) (Wave 4) | 0.55 (0.36) | 0.04 – 1.66 |
| Depressive symptoms (Wave 4) | 2.51 (2.39) | 0 – 13 |
| Young adult educational attainment (Wave 4) | 5.88 (2.31) | 1 – 13 |
| Alcohol use (Wave 4) | 0.63 (1.21) | 0 – 6 |
Table 2.
Correlations among study variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender, male | — | ||||||||||
| 2. Age | .077 | — | |||||||||
| 3. Ethnicity, Hispanic | −.012 | −.060 | — | ||||||||
| 4. Race, Black | −.006 | −.039 | −.204** | — | |||||||
| 5. Race, others | −.026 | .104 | −.082 | −.091 | — | ||||||
| 6. Family SES | .024 | .088 | −.235*** | −.035 | −.017 | — | |||||
| 7. Mean conscientiousness | −.048 | .109 | .096 | −.059 | −.052 | −.049 | — | ||||
| 8. Deviation of conscientiousness | .000 | .000 | .000 | .000 | .000 | .000 | .000 | — | |||
| 9. C-reactive protein | −.163** | −.089 | .189** | −.015 | .051 | −.160** | −.029 | −.003 | — | ||
| 10. Depressive symptoms | −.042 | −.007 | −.030 | .002 | .016 | −.050 | −.152* | −.069 | −.036 | ||
| 11. Education attainment | .034 | .125* | −.084 | −.102 | .052 | .234*** | .144* | .024 | −.018 | −.190** | |
| 12. Alcohol use | .045 | .002 | −.039 | −.089 | .106 | .061 | −.214*** | −.047 | −.033 | .124* | −.091 |
N = 282.
p < .05.
p < .01.
p < .001.
Family SES, Conscientiousness, and Young Adult Academic/Mental Health Outcomes
Table 3 presents the associations of family SES and conscientiousness with educational attainment, depressive symptoms, and alcohol use. Overall, main effect analyses indicated that higher family SES at age 16 was associated with participants’ attaining a higher education by age 29. Main effects for between-pair mean conscientiousness also emerged for all young adult academic and mental health outcomes. The between-family effects indicated that twins with higher mean conscientiousness had higher educational attainment, lower levels of depressive symptoms, and less problematic alcohol use. No significant within-family effects of conscientiousness or SES × conscientiousness interactions emerged for academic/mental health outcomes.
Table 3.
Family SES and conscientiousness as predictors of academic and psychological outcomes (N = 282)
| Educational Attainment | Alcohol Use | Depressive Symptoms | ||||
|---|---|---|---|---|---|---|
| Predictors | b | [95% CI] | b | [95% CI] | b | [95% CI] |
| 1. Gender, male | .078 | [−.182, .339] | .063 | [−.155, .282] | −.128 | [−.401, .146] |
| 2. Age | .165 | [−.095, .425] | .031 | [−.198, .259] | .052 | [−.191, .296] |
| 3. Ethnicity, Hispanic | −.139 | [−.409, .131] | −.045 | [−.328, .237] | −.070 | [−.320, .180] |
| 4. Race, Black | −.226 | [−.469, .017] | −.202 | [−.499, .095] | −.016 | [−.309, .276] |
| 5. Race, others | .091 | [−.175, .358] | .116 | [−.011, .243] | .008 | [−.275, .290] |
| 6. Family SES | .456*** | [.202, .710] | .065 | [−.120, .250] | −.104 | [−.407, .198] |
| 7. Mean conscientiousness | .330** | [.091, .568] | −.373*** | [−.540, −.205] | −.357** | [−.616,−.099] |
| 8. Deviation of conscientiousness | .049 | [−.206, .304] | −.085 | [−.296, .126] | −.168 | [−.479, .144] |
| 9. Family SES × Mean conscientiousness | .123 | [−.132, .378] | .024 | [−.141, .190] | −.134 | [−.421, .153] |
| 10. Family SES × Deviation of conscientiousness | .203 | [−.133, .539] | .013 | [−.254, .280] | −.283 | [−.613, .047] |
p < .05.
p < .01.
p < .001.
Family SES, Conscientiousness, and Young Adult Low-Grade Inflammation
Table 4 presents the associations between family SES, conscientiousness, and CRP. There was a main effect such that higher family SES was associated with lower CRP. There was also a significant two-way interaction of family SES × within-twin deviation of conscientiousness (b = −.057, 95% CI [−.105, −.009], p = .020). Although this interaction emerged in analyses treating SES as a continuous variable, we followed standard guidelines for interpreting its form (Hayes, 2018). Those guidelines involve plotting estimated CRP levels at lower (−1.5 SD below the mean) and higher (+1.5 SD above the mean) values of the distributions of predictor variables (which in this case are family SES and within-twin conscientiousness). These results, depicted in Figure 1, show that for twins who came from low SES families, the more conscientious twin had higher CRP at age 29 compared to their co-twin (simple slope b = .085, 95% CI [.006, .163], standardized beta = .23, p = .036), even after controlling for covariates. This association went in the opposite direction for twins raised in high SES families. In these families, the more conscientious twin had lower CRP compared to their co-twin (simple slope = −.087, 95% CI [−.171, −.002], standardized beta = −.24, p = .046). The standardized betas in the above two simple slopes represent an effect size, and for low SES twins, can be interpreted as meaning that for every 1 standard deviation increase in the conscientiousness gap between twin pairs, there is a concomitant .23 SD increase in CRP (for the higher conscientious twin compared to the lower conscientious twin). The Johnson Neyman technique indicates that the simple slope of the association between deviation of conscientiousness and CRP is significant both when family SES is <= −1.32 SD below the mean and when family SES is >= 1.24 SD above the mean.
Table 4.
Family SES and conscientiousness as predictors of low-grade inflammation (N = 282)
| C-reactive protein | ||
|---|---|---|
| Predictors | b | [95% CI] |
| 1. Gender, male | −.051* | [−.090,−.011] |
| 2. Age | −.022 | [−.066, .022] |
| 3. Ethnicity, Hispanic | .059** | [.015, .104] |
| 4. Race, Black | .002 | [−.043, .047] |
| 5. Race, others | .023 | [−.026, .072] |
| 6. Family SES | −.055* | [−100,−011] |
| 7. Mean conscientiousness | −.022 | [−.060, .015] |
| 8. Deviation of conscientiousness | −.001 | [−.040, .038] |
| 9. Family SES × Mean conscientiousness | .038 | [−.004, .079] |
| 10. Family SES × Deviation of conscientiousness | −.057* | [−.105,−.009] |
p < .05.
p < .01.
p < .001. C-reactive protein was log-transformed.
Figure 1.
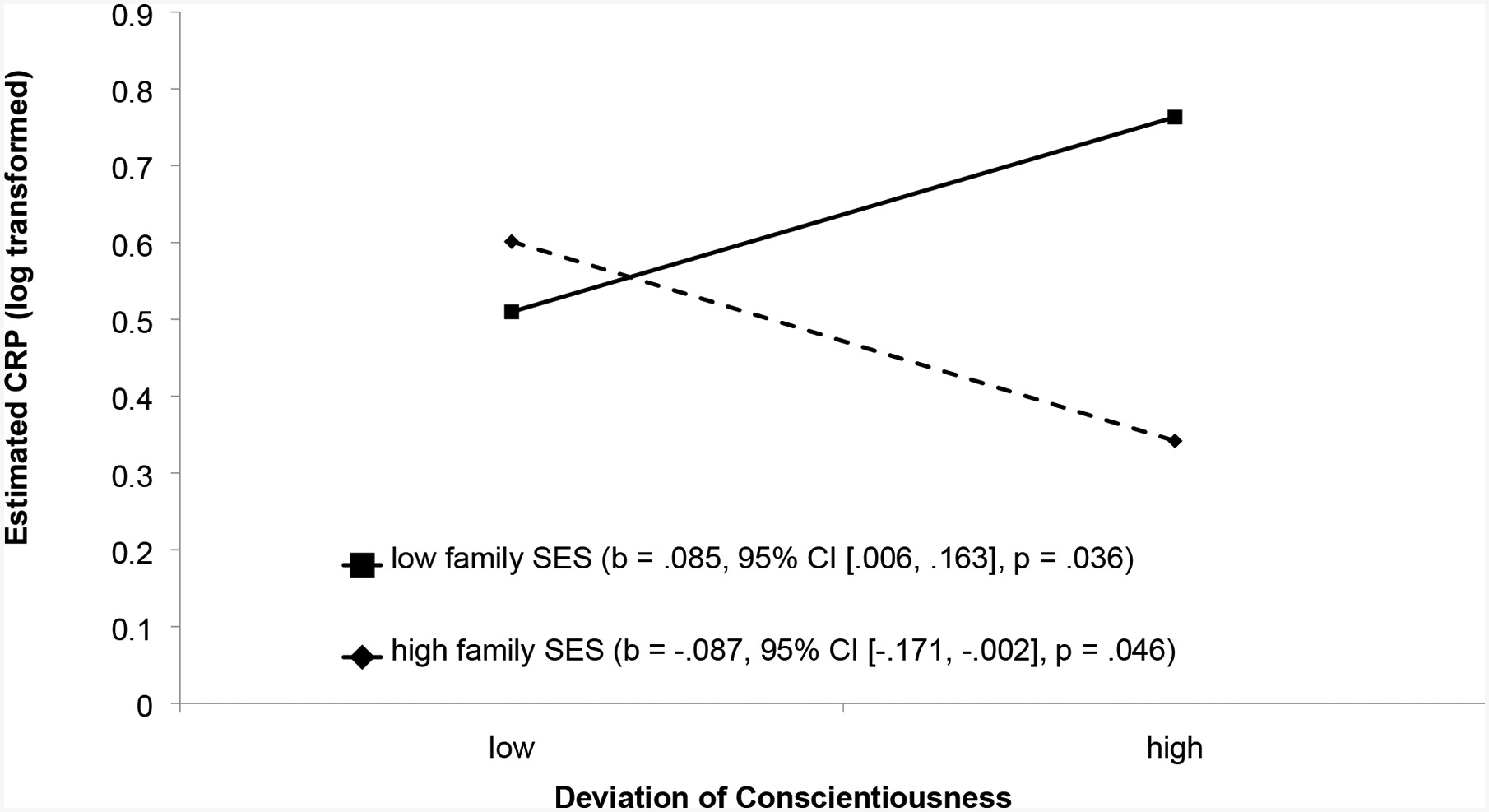
Levels of CRP at age 29 as a function of family SES and the deviation of conscientiousness among twin pairs. The lines represent the regression lines for different levels of family socioeconomic status (SES). Low refers to 1.5 SD below the mean; high refers to 1.5 SD above the mean for both variables. Numbers in parentheses refer to simple slopes.
Supplemental analyses were conducted to determine whether participants’ gender or race/ethnicity would moderate the findings reported above. None of the interactions with gender or race/ethnicity were significant.
Additional Analyses
We conducted additional analyses to probe the robustness of the CRP findings. The above analyses were conducted on all CRP samples. We also re-ran analyses excluding samples >10mg/L (n=26), which could reflect acute infection or trauma as opposed to chronic inflammation. The interaction term for family SES × deviation of conscientiousness predicting CRP remained significant: b=−.056, 95% CI [−.092, −.021], p=.002.
Second, we re-ran analyses controlling for body mass index (BMI), self-report of infectious or inflammatory diseases (yes/no), and self-report of anti-inflammatory medication usage (yes/no). After controlling for these additional covariates, the interaction term between family SES × deviation of conscientiousness predicting CRP remained significant: b=−.059, 95% CI [−.10, −.02], p=.005
DISCUSSION
The results of this study demonstrated support for the skin-deep resilience phenomenon using a co-twin control design. In a sample of MZ twins, we found that among twins growing up in lower SES households, the twin with higher levels of conscientiousness also had higher CRP in young adulthood. In contrast, there were main effects of conscientiousness on academic and mental health outcomes in young adulthood, such that higher levels of between-twin conscientiousness were associated with higher educational attainment, fewer symptoms of depression, and less problematic alcohol use, across all SES groups. This divergence between outcomes suggests the possibility that conscientiousness is generally beneficial for academic and psychological outcomes, but might have costs in the form of low-grade inflammation that are specific for individuals from low SES households.
These patterns are consistent with a growing literature documenting interactions between SES and conscientiousness/self-control/striving in predicting physical health outcomes (Miller et al., 2016; Duggan et al., 2019; Brody et al., 2016; Miller et al., 2015). However, here we extend this research through the use of a twin design that mitigates the risks posed by shared genetic and environmental confounds. These findings are also consistent with quasi-experimental data that utilized a natural experiment design testing the effects of an increase in the required years of schooling in France. That study documented that an increase in schooling led to an increase in blood pressure among those from lower social classes (but not for those from higher social classes) (Courtin et al., 2019). Taken together, these findings suggest that high levels of prolonged striving in school among low SES students may come at a physical health cost.
In contrast, among MZ twins from higher SES households, the opposite was true: the twin with higher levels of conscientiousness had lower levels of CRP. These findings fit with a large literature and theory about the benefits of conscientiousness generally for numerous health outcomes including mortality, risk for chronic illnesses, and cardiovascular risk factors (for reviews, see: (Bogg & Roberts, 2013; Bogg & Roberts, 2004; Kern & Friedman, 2008)). It is thought that conscientiousness is generally beneficial to health because more conscientious individuals will engage in healthier behaviors as well as be more planful about their future health (Bogg & Roberts, 2004). Our finding with CRP amongst higher SES participants is consistent with this broader literature, and this may be because many previous studies on conscientiousness and health have traditionally been conducted among predominantly middle to upper middle class participants.
However, why would the effects of conscientiousness on inflammation diverge amongst lower versus higher SES individuals? We theorize that in the particular group of low SES individuals who are high in conscientiousness, there is a unique and different set of factors driving health (skin-deep resilience). That is, for lower SES individuals, having lofty long-term goals may prove frustrating when structural conditions undermine one’s capacity to achieve those goals. For example, many of these low SES youth may be attending schools with limited resources that constrain their chances for academic success, or may come from families that are limited in their ability to provide academic support and resources to their children, or are balancing school and family/work demands that high-achieving high SES youth do not have to contend with. These conscientious low SES youth are then having to engage in prolonged levels of high effortful striving, without many resources, supports, or breaks, in order to achieve their goals, and this effortful striving takes its toll on physical health. In contrast, among high SES individuals, high levels of individual conscientiousness may complement the existing family and school support structures and enable individuals to achieve successful life outcomes that include good health.
Across all groups, we find that conscientiousness is associated with beneficial psychosocial outcomes, including higher educational attainment, less depression, and less substance use. These findings are consistent with a large literature that has documented the benefits of conscientiousness on various psychological and life outcomes, including academic achievement, occupational attainment, income, substance use, life satisfaction, and positive affect (Kotov, Gamez, Schmidt, & Watson, 2010; Poropat, 2009; Roberts, Kuncel, Shiner, Caspi, & Goldberg, 2007; Duckworth, Weir, Tsukayama, & Kwok, 2012; Ozer & Benet-Martinez, 2006). This may be because conscientious individuals are more likely to make their behaviors consistent with long-term goals, to think before acting, and to make choices with school, work, and family roles in mind (Duckworth et al., 2012; Jackson et al., 2010; Shanahan, Hill, Roberts, Eccles, & Friedman, 2014). However, we note that in the present study, only the main effect of between-twin (not within-twin) conscientiousness predicted psychosocial outcomes, weakening the strength of any causal conclusions that can be drawn about conscientiousness. It is uncertain why between and not within twin effects emerged here, but as noted above, there is a substantial existing literature that documents main effects of conscientiousness on many life outcomes, thus supporting the between-twin findings. It is likely that there are also genetic and family environment factors that contribute to both conscientiousness and life outcomes.
One question that might arise is why the challenges and struggles associated with growing up in a low SES environment for someone with high levels of conscientiousness would not lead to increases in depressive symptoms. We hypothesize that it is because many low SES youth who are high in conscientiousness are achieving a multitude of successes in their lives, in terms of educational attainment, jobs, and good incomes in adulthood. These successes make them and their families proud, because they have found ways to work hard and overcome numerous obstacles. We speculate that the praise from others and boosts to self-esteem that result from these successes may create positive (rather than depressed) mood. The idea that exposure to environmental adversities might not necessarily result in greater depression can also be seen in the literature, whereby Blacks have lower levels of major depression than Whites, despite the greater stress exposure, marginalized status, and fewer resources they typically experience (Barnes & Bates, 2017; Breslau et al., 2006). This may be because of protective factors, such as religiosity and self-esteem, that buffer individuals from environmental adversities (Barnes & Bates, 2017; Breslau et al., 2006). It may also be that individuals who confront frequent environmental adversities cope with these stressors through unhealthy behaviors (e.g., substance use, comfort eating) that alleviate psychological distress but have negative implications for physical health (Jackson, Knight, & Rafferty, 2010).
Strengths of the present study involve the testing of study hypotheses using a sample of MZ twins and a co-twin control design, the use of a biomarker of low-grade inflammation (rather than relying on self-reports of health), and the longitudinal design that allowed us to test effects on academic, mental, and physical health outcomes ~13 years after baseline assessment of family SES. The use of a co-twin control design with MZ twins allowed us to minimize potential confounding by shared genetic and environmental factors. However other non-shared factors unique to one twin and random error could still confound the observed associations. Limitations of the present study included the relatively small sample, which did not allow us to test for effects specific to certain racial/ethnic groups, the fact that this twin subsample is not population representative (thus limiting conclusions that can be drawn to the general population), and the lack of a conscientiousness measure or inflammation measures at earlier waves of the study. We also did not have measures of mental health that were not self-report, and in order to rule out common method variance, it would be important for future studies to include measures that do not rely solely on participant recall. We note as well that while it may initially seem counterintuitive that results with depressive symptoms and an inflammatory biomarker could go in opposite directions, there is both heterogeneity (variability by demographic group) and inconsistency in the depression-inflammation link (Howren, Lamkin, & Suls, 2009; Glassman & Miller, 2007). Finally, future studies would benefit from being able to test a broader range of inflammation markers (e.g., Add Health did not collect data on cytokines) and clinical health outcomes, from being able to follow participants further into adulthood when chronic conditions become more prevalent, and from designing experimental manipulations or interventions that test skin-deep resilience hypotheses. Future studies should also continue to test between- versus within-twin effects of conscientiousness on a variety of life outcomes.
CONCLUSIONS
In sum, the present study demonstrated further evidence for skin-deep resilience among MZ twins: that is, among lower SES twins, the twin with higher levels of conscientiousness also had higher CRP, whereas the opposite was true among higher SES twins. In addition, there was a divergence of mental health/academic outcomes with physical health outcomes, such that higher levels of conscientiousness were beneficial for educational attainment, depressive symptoms, and alcohol use, regardless of SES. These findings suggest that academic programs designed to support at-risk youth may benefit from incorporating a broader focus that includes physical health promotion efforts, so that achieving academic success does not end up coming at a cost to these youth.
Highlights.
Higher conscientiousness appears to have detrimental effects on inflammation in lower socioeconomic status (SES) youth.
Among monozygotic (MZ) twins from lower SES households, the one with higher conscientiousness evinced higher levels of C-reactive protein (CRP).
Among MZ twins from higher SES households, the opposite is true - the twin with higher conscientiousness had lower CRP.
Higher conscientiousness was associated with higher educational attainment, fewer depressive symptoms, and less problematic alcohol use across all participants.
These findings provide evidence for “skin-deep resilience” - the idea that low SES youth who work hard to succeed in life experience good life outcomes, but at a cost to their physical health.
Funding Source:
This research was supported by National Institutes of Health grant HD093718, and uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. No direct support was received from grant P01-HD31921 for this analysis.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
All authors declare no competing interests.
References
- Balagopal P, de Ferranti SD, Cook S, Daniels SR, Gidding SS, Hayman LL, … Steinberger J (2011). Nontraditional risk factors and biomarkers for cardiovascular diseases: Mechanistic, research, and clinical considerations for youth. A scientific statement from the American Heart Association. Circulation, 123, 2749–2769. [DOI] [PubMed] [Google Scholar]
- Barnes DM, & Bates LM (2017). Do racial patterns in psychological distress shed light on the Black-White depression paradox? A systematic review. Social Psychiatry and Psychiatric Epidemiology, 52, 913–928. [DOI] [PubMed] [Google Scholar]
- Bogg T, & Roberts BW (2013). The case for conscientiousness: evidence and implications for a personality trait marker of health and longevity. Ann Behav Med, 45(3), 278–288. doi: 10.1007/s12160-012-9454-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogg T, & Roberts BW (2004). Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin, 130, 887–919. [DOI] [PubMed] [Google Scholar]
- Breslau J, Aguilar-Gaxiola S, Kendler KS, Su M, Williams D, & Kessler RC (2006). Specifying race-ethnic differences in risk for psychiatric disorder in a USA national sample. Psychological Medicine, 36, 57–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, Yu T, Chen E, Miller GE, Kogan SM, & Beach SRH (2013). Is resilience only skin deep? Rural African Americans’ preadolescent socioeconomic status-related risk and competence and age 19 psychological adjustment and allostatic load. Psychological Science, 24, 1285–1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, Yu T, Miller GE, & Chen E (2016). Resilience in adolescence, health, and psychosocial outcomes. Pediatrics, 138, e20161042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen E, Miller GE, Brody GH, & Lei M (2015). Neighborhood Poverty, College Attendance, and Diverging Profiles of Substance Use and Allostatic Load in Rural African American Youth. Clin Psychol Sci, 3(5), 675–685. doi: 10.1177/2167702614546639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen E, Shalowitz MU, Story RE, Hayen R, Leigh AKK, Hoffer LC, … Miller GE (2019). The costs of high self-control in Black and Latino youth with asthma: Divergence of mental health and inflammatory profiles. Brain Behavior and Immunity, 80, 120–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtin E, Nafilyan V, Avendano M, Meneton P, Berkman LF, Goldberg M, … Dowd JB (2019). Longer schooling but not better off? A quasi-experimental study of the effect of compulsory schooling on biomarkers in France. Social Science & Medicine, 220, 379–386. [DOI] [PubMed] [Google Scholar]
- Donnellan MB, Oswald FL, Baird BM, & Lucas RE (2006). The mini-IPIP scales: tiny-yet-effective measures of the Big Five factors of personality. Psychol Assess, 18(2), 192–203. doi: 10.1037/1040-3590.18.2.192 [DOI] [PubMed] [Google Scholar]
- Duckworth AL, Weir D, Tsukayama E, & Kwok D (2012). Who does well in life? Conscientious adults excel in both objective and subjective success. Frontiers in Psychology, 3, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duggan KA, Jennings JR, & Matthews KA (2019). Prospective associations of adolescent conscientiousness with psychological resources and metabolic syndrome in Black and White men. Psychosomatic Medicine, 81, 341–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaydosh L, Schorpp K, Chen E, Miller G, & Harris KM (2018). College completion predicts lower depression but higher metabolic syndrome among disadvantaged minorities in young adulthood. Proceedings of the National Academy of Sciences, 115, 109–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glassman AH, & Miller GE (2007). Where there is depression, there is inflammation…sometimes! Biological Psychiatry, 62, 280–281. [DOI] [PubMed] [Google Scholar]
- Goodman E, Slap GB, & Huang B (2003). The public health impact of socioeconomic status on adolescent depression and obesity. American Journal of Public Health, 93, 1844–1850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamdi NR, South SC, & Krueger RF (2016). Does education lower allostatic load? A co-twin control study. Brain Behavior and Immunity, 56, 221–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris KM, Halpern CT, Smolen A, & Haberstick BC (2006). The national longitudinal study of Adolescent Health (Add Health) twin data. Twin Research and Human Genetics, 6, 988–997. [DOI] [PubMed] [Google Scholar]
- Harris KM, Halpern CT, Whitsel E, Hussey J, Tabor J, Entzel P, & Udry JR (2009). The National Longitudinal Study of Adolescent to Adult Health: Research design, Retrieved from. http://www.cpc.unc.edu/projects/addhealth/design.
- Hayes AF (2018). Introduction to mediation, moderation, and conditional process analysis, Second Edition New York, NY: Guilford Press. [Google Scholar]
- Hingson RW, Heeren T, & Winter MR (2006). Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Archives of Pediatric Adolescent Medicine, 160, 739–746. [DOI] [PubMed] [Google Scholar]
- Hotamisligil GS (2006). Inflammation and metabolic disorders. Nature, 444(7121), 860–867. doi: 10.1038/nature05485 [DOI] [PubMed] [Google Scholar]
- Howren MB, Lamkin DM, & Suls J (2009). Associations of depression with C-reactive protein, IL-1, and IL-6: A meta-analysis. Psychosomatic Medicine, 71, 171–186. [DOI] [PubMed] [Google Scholar]
- Jackson JJ, Wood D, Bogg T, Walton KE, Harms PD, & Roberts BW (2010). What do conscientious people do? Development and validation of the Behavioral Indicators of Conscientiousness (BIC). Journal of Research in Personality, 44, 501–511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson JS, Knight KM, & Rafferty JA (2010). Race and unhealthy behaviors: chronic stress, the HPA axis, and physical and mental health disparities over the life course. Am J Public Health, 100(5), 933–939. doi: 10.2105/AJPH.2008.143446 [DOI] [PMC free article] [PubMed] [Google Scholar]
- James SA, Keenan NL, Strogatz DS, Browning SR, & Garrett JM (1992). Socioeconomic status, John Henryism, and blood pressure in black adults. The Pitt County Study. Am J Epidemiol, 135(1), 59–67. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1736661 [DOI] [PubMed] [Google Scholar]
- James SA, Strogatz DS, Wing SB, & Ramsey DL (1987). Socioeconomic status, John Henryism, and hypertension in blacks and whites. Am J Epidemiol, 126(4), 664–673. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=3631056 [DOI] [PubMed] [Google Scholar]
- Kern ML, & Friedman HS (2008). Do conscientious individuals live longer? A quantitative review. Health Psychology, 27, 505–512. [DOI] [PubMed] [Google Scholar]
- Kotov R, Gamez W, Schmidt F, & Watson D (2010). Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136, 768–821. [DOI] [PubMed] [Google Scholar]
- Luthar SS (2006). Resilience in development: A synthesis of research across five decades In Cicchetti D & Cohen DJ (Eds.), Developmental psychopathology, 2nd ed., Vol. 3. Risk, disorder, and adaptation (pp. 739–795). New York, NY: John Wiley & Sons. [Google Scholar]
- Masten AS (2018). Resilience theory and research on children and families: Past, present, and promise. Journal of Family Theory & Review, 10, 12–31. [Google Scholar]
- McGue M, Osler M, & Christensen K (2010). Causal inference and observational research: The utility of twins. Perspectives on Psychological Science, 5, 546–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller GE, Cohen S, Janicki-Deverts D, Brody GH, & Chen E (2016). Viral challenge reveals further evidence of skin-deep resilience in African Americans from disadvantaged backgrounds. Health Psychology, 35, 1225–1234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller GE, Chen E, & Parker KJ (2011). Psychological stress in childhood and susceptibility to the chronic diseases of aging: moving toward a model of behavioral and biological mechanisms. Psychol Bull, 137(6), 959–997. doi: 10.1037/a0024768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller GE, Yu T, Chen E, & Brody GH (2015). Self-control forecasts better psychosocial outcomes but faster epigenetic aging in low-SES youth. Proc Natl Acad Sci U S A, 112(33), 10325–10330. doi: 10.1073/pnas.1505063112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozer DJ, & Benet-Martinez V (2006). Personality and the prediction of consequential outcomes. Annual Review of Psychology, 57, 401–421. [DOI] [PubMed] [Google Scholar]
- Perreira KM, Deeb-Sossa N, Harris KM, & Bollen K (2005). What are we measuring? An evaluation of the CES-D across race/ethnicity and immigrant generation. Social Forces, 83, 1567–1601. [Google Scholar]
- Poropat AE (2009). A meta-analysis of the five-factor model of personality and academic performance. Psychological Bulletin, 135, 322–338. [DOI] [PubMed] [Google Scholar]
- Pradhan AD, Manson JE, Rifai N, Buring JE, & Ridker PM (2001). C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA, 286(3), 327–334. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=11466099 [DOI] [PubMed] [Google Scholar]
- Pradhan AD, Manson JE, Rossouw JE, Siscovick DS, Mouton CP, Rifai N, … Ridker PM (2002). Inflammatory biomarkers, hormone replacement therapy, and incident coronary heart disease: Prospective analysis from the Women’s Health Initiative observational study. Jama-Journal of the American Medical Association, 288(8), 980–987. Retrieved from ISI:000177656400023 [DOI] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population_. Journal of Applied Psychological Measurement, 1, 385–401. [Google Scholar]
- Ridker PM (2003). Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation, 107(3), 363–369. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12551853 [DOI] [PubMed] [Google Scholar]
- Ridker PM (2007). Inflammatory biomarkers and risks of myocardial infarction, stroke, diabetes, and total mortality: implications for longevity. Nutr Rev, 65(12 Pt 2), S253–9. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18240558 [DOI] [PubMed] [Google Scholar]
- Ridker PM, Rifai N, Cook NR, Bradwin G, & Buring JE (2005). Non-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in women. JAMA, 294(3), 326–333. doi: 10.1001/jama.294.3.326 [DOI] [PubMed] [Google Scholar]
- Ridker PM, Hennekens CH, Buring JE, & Rifai N (2000). C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. New England Journal of Medicine, 342(12), 836–843. Retrieved from ISI:000086014100002 [DOI] [PubMed] [Google Scholar]
- Roberts BW, Kuncel NR, Shiner R, Caspi A, & Goldberg LR (2007). The power of personality: The comparative validity of personality traits, socioeconomic status, and cognitive ability for predicting important life outcomes. Perspectives on Psychological Science, 2, 313–345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz JA (2017). Long-term physical health consequences of perceived inequality: Results from a twin comparison design. Social Science & Medicine, 187, 184–192. [DOI] [PubMed] [Google Scholar]
- Schwartz JA, & Beaver KM (2013). Serious fighting-related injuries produce a significant reduction in intelligence. Journal of Adolescent Health, 53, 520–525. [DOI] [PubMed] [Google Scholar]
- Shanahan MJ, Hill PL, Roberts BW, Eccles J, & Friedman HS (2014). Conscientiousness, health, and aging: The life course of personality model. Developmental Psychology, 50, 1407–1425. [DOI] [PubMed] [Google Scholar]
- Turkheimer E, & Harden KP (2014). Behavior genetic research methods: testing quasi-causal hypotheses using multivariate twin data In Reis HT & Judd CM (Eds.), Handbook of Research Methods in Social and Personality Psychology (p. 159e187). [Google Scholar]
- Whitsel EA, Cuthbertson CC, Tabor JW, Potter AJ, Wener MH, Kileya-Jones LA, & Harris KM (2012). Add Health Wave IV documentation: Measures of inflammation and immune function. Chapel Hill, NC: University of North Carolina at Chapel Hill. [Google Scholar]