

Abstract
Objective The health care system has been struggling to find the optimal way to protect patients and staff from coronavirus disease 2019 (COVID-19). Our objective was to evaluate the impact of two strategies on transmission of COVID-19 to health care workers (HCW) on labor and delivery (L&D).
Study Design We developed a decision analytic model comparing universal COVID-19 screening and universal PPE on L&D. Probabilities and costs were derived from the literature. We used individual models to evaluate different scenarios including spontaneous labor, induced labor, and planned cesarean delivery (CD). The primary outcome was the cost to prevent COVID-19 infection in one HCW. A cost-effectiveness threshold was set at $25,000 to prevent a single infection in an HCW.
Results In the base case using a COVID-19 prevalence of 0.36% (the rate in the United States at the time), universal screening is the preferred strategy because while universal PPE is more effective at preventing COVID-19 transmission, it is also more costly, costing $4,175,229 and $3,413,251 to prevent one infection in the setting of spontaneous and induced labor, respectively. For planned CD, universal PPE is cost saving. The model is sensitive to variations in the prevalence of COVID-19 and the cost of PPE. Universal PPE becomes cost-effective at a COVID-19 prevalence of 34.3 and 29.5% and at a PPE cost of $512.62 and $463.20 for spontaneous and induced labor, respectively. At a higher cost-effectiveness threshold, the prevalence of COVID-19 can be lower for universal PPE to become cost-effective.
Conclusion Universal COVID-19 screening is generally the preferred option. However, in locations with high COVID-19 prevalence or where the local societal cost of one HCW being unavailable is the highest such as in rural areas, universal PPE may be cost-effective and preferred. This model may help to provide guidance regarding allocation of resources on L&D during these current and future pandemics.
Key Points
Universal screening is the preferred strategy for labor.
With high prevalence, universal PPE is cost-effective.
For planned cesarean, universal PPE is cost saving.
Keywords: cost-effectiveness analysis, COVID-19, decision analysis, personal protective equipment, universal screening
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)—the virus that causes COVID-19—was first reported in December 2019 in Wuhan, in the Hubei province of China. 1 COVID-19 has now become a worldwide pandemic, and the United States (US) currently has the highest number of test-confirmed cases, with current estimates of 1,172,670 as of May 4, 2020. 2 These numbers are difficult to interpret because they likely underrepresent the true burden of disease as many people infected with COVID-19 are asymptomatic or only mildly symptomatic and have not undergone testing. 3
One approach to protecting pregnant patients and health care workers (HCW) on labor and delivery (L&D) is universal screening. In a report from New York City following implementation of universal COVID-19 screening on L&D, among 215 women who delivered between March 22 and April 4, 2020, a total of 33 patients (15.3%) tested positive and only 4 (12.1%) were symptomatic on presentation. 4 These findings highlight that COVID-19 may need to be considered for all patients presenting to L&D.
Universal COVID-19 screening clearly has value. It allows for timely initiation of infection control practices given that asymptomatic viral spread is possible, 5 it may allow for preservation of already-limited personal protective equipment (PPE) supplies, and it provides necessary information for well-baby and neonatal intensive care units. However, there are legitimate problems regarding universal screening. For example, there is continuing concern over the availability and turn-around time of tests as well as uncertainties about test characteristics. Universal PPE usage eliminates the issues related to testing; however, it may not be possibly given PPE shortages nationwide.
Our objective was to evaluate the impact of two different strategies—universal COVID-19 screening and universal PPE use—on COVID-19 transmission to an HCW on L&D. We hypothesized that universal PPE would be the optimal way to prevent transmission of COVID-19 to a HCW. However, given the impossibility of relying solely on universal PPE based on current supply, we additionally hypothesized that there would be a threshold prevalence of COVID-19 below which universal screening would be appropriate and above which universal PPE should be recommended.
Materials and Methods
We developed a decision analytic model to evaluate the costs and effects of these two potential policies on L&D during the COVID-19 pandemic ( Fig. 1 ). The cost analysis was designed to estimate and compare the direct expenditures related to COVID-19 screening and PPE usage. We individually ran models evaluating three different scenarios on L&D: (1) spontaneous labor, (2) planned induction, and (3) planned cesarean delivery (CD).
Fig. 1.
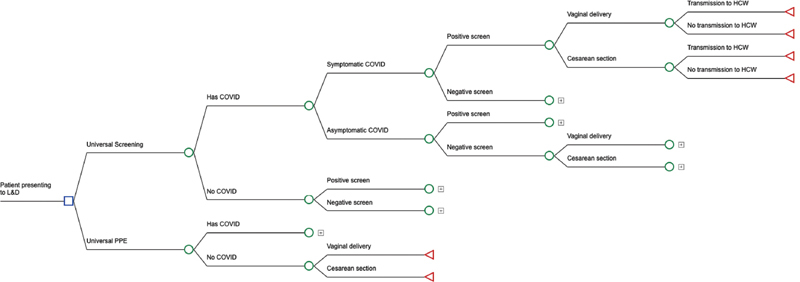
Decision-analytic model. All branches not terminating in a triangle are collapsed to facilitate display and are the same as branches already open.
To obtain base case probability point estimates and confidence intervals, we conducted an English language search of PubMed to identify relevant publications. The search was not limited by publication date or country of origin. All identified documents were examined and those that were relevant were retrieved. Reference lists of retrieved documents were manually reviewed to identify additional publications. We additionally utilized online tools created specifically for the COVID-19 pandemic, such as the Johns Hopkins Coronavirus Resource Center. 6 We calculated base case point estimates as the unweighted mean or median of the available databased on their distributions and confidence intervals ( Table 1 ). Importantly, we also used data from prior viral pandemics, given the paucity of data regarding COVID-19.
Table 1. Probabilities and costs.
| Variable | Base case | Range considered in sensitivity analysis | Reference |
|---|---|---|---|
| Probabilities | |||
| Probability of COVID | 0.0036 | 0.0001–1 | 6 20 |
| Probability a patient is symptomatic with COVID | 0.121 | 0–1 | 4 |
| Probability of transmission with standard precautions | All varied 0–1 | 9 10 11 12 | |
| VD (spontaneous) | 0.13 | ||
| VD IOL | 0.15 | ||
| CD (unplanned) spontaneous labor | 0.33 | ||
| CD (unplanned) IOL | 0.35 | ||
| CD (planned) | 0.27 | ||
| Probability of transmission wearing PPE | 0.07 | 0–1 | 14 |
| Sensitivity of rapid rest | 0.897 | 0.5–1 | 21 22 |
| Specificity of rapid test | 0.983 | 0.5–1 | 21 22 |
| Probability of a CD for COVID-19 negative women | All varied 0–1 | 8 | |
| IOL | 0.186 | ||
| Spontaneous labor | 0.222 | ||
| Probability of a CD with PPE (multiplier) | 1.25 | 1–2 | Assumed |
| Probability of a CD with COVID (multiplier) | 2 | 1–4 | Assumed |
| Costs | |||
| Cost of rapid test | $200 | $50–500 | UW laboratory |
| Cost of PPE for planned CD | $95.71 | $40-$500 | UW costs, 13 15 |
| Cost of PPE for unplanned CD | $147.21 | $40–500 | UW costs 13 15 |
| Cost of PPE for spontaneous VD | $90.43 | $40–500 | UW costs 13 |
| Cost of PPE for induced VD | $115.15 | $40–500 | UW costs 13 |
| Cost of CD | $16,216 | $12,000-$21000 | 16 |
| Cost of a VD | $8,749 | $6,000–11,000 | 16 |
Abbreviations: CD, cesarean delivery; IOL, induction of labor; PPE, personal protective equipment; UW, University of Washington in-house costs; VD, vaginal delivery.
We estimated the prevalence of COVID-19 in the community by using the total diagnosed cases from the Johns Hopkins Coronavirus Resource Center as well as the estimated population of the United States (the former from April 5, 2020 and the latter an estimate from the U.S. census bureau in July 2019). This likely represents the minimum overall prevalence given that only a small percentage of the U.S. population has been tested. Experience from New York informed the likelihood that a pregnant patient would be symptomatic with a COVID-19 infection, 4 as well as the likelihood of a CD in the setting of COVID-19. 7 Our initial assumption was that the likelihood of a CD should be based on whether the delivery was spontaneous or induced labor. 8 We then added two modifiers: one for the possibility that patients infected with COVID-19 have an increased risk of CD due to physiologic changes related to infection, and a second for the increased likelihood of CD while wearing PPE given the difficulty in performing an emergent CD while properly donning PPE.
The reproduction number of an infection (R0) is defined as the expected number of cases directly generated by one case in a population where all individuals are susceptible to infection and is a measure of how contagious the disease is. COVID-19 is believed to have an R0 between 1.4 and 6.5 and therefore likely higher than both the 2009 H1N1 outbreak (R0 = 1.5) and the 1918 influenza pandemic (R0 = 1.8). 9 10 11 The likelihood of transmission without wearing PPE was therefore estimated from the likelihood of transmission of the 1918 influenza pandemic. We calculated the risk of transmission based on person-hours of contact on L&D and postpartum. 12 13 The amount of time a patient spent on L&D as well as postpartum was varied depending on the mode of delivery.
Regarding the risk of transmission with PPE, we used data from the SARS coronavirus (SARS-CoV) epidemic. Given similar methods of transmission, the reduction in transmission risk with PPE use for COVID-19 is likely similar to SARS-CoV. A study from the SARS-CoV epidemic showed that handwashing and N-95 masks were both highly effective at reducing transmission (relative risk = 0.07 and 0.1, respectively). 14 In creating our model for universal PPE, we considered whether patients should wear a surgical mask to decrease the likelihood of transmission. In the base case, we did not assume that patients would wear a surgical mask given that in our experience on L&D, appropriate mask use varies widely. However, both the cost of a patient mask and the reduction of transmission while the patient is wearing a mask were built into the model to examine these effects during sensitivity analysis.
Finally, the sensitivity and specificity of a rapid COVID-19 test were derived from an average of 10 different tests currently on the market.
We derived cost estimates in a similar fashion to the probability estimates but additionally queried local hospital data ( Table 1 ). The costs of the rapid COVID-19 test, goggles, gown, gloves, a surgical mask, an N-95 mask, and a powered air-purifying respirator were taken from local hospital data. The cost of hand sanitizer and antiviral wipes were not accounted for in our estimates. Cost profiles were set up for induced labor, spontaneous labor, and planned CD with the possible obstetric outcomes, vaginal delivery (VD), unplanned CD, and planned CD—within each profile—as appropriate. These cost profiles took into account the average number of hours on L&D and on a postpartum floor, the number of room entries during those times, the PPE required during each of those room entries, and the costs of the procedures themselves. 13 15 16 Vaginal deliveries were assumed to have a 1.5-day postpartum stay, and CD had a 2- and 2.5-day postpartum stay for planned and unplanned CD, respectively. 15 Postoperative patients were assumed to have higher nursing needs postpartum with an additional two interactions per day with nursing staff. The number of personnel in the operating room during a CD was assumed to be a minimum number for a teaching hospital and included presence by pediatrics. We did not account for long-term costs related to COVID-19 acquisition by an HCW. We adjusted all costs to reflect 2020 US dollars.
The model assumed that all HCWs were susceptible to COVID-19. It did not take into account the costs of downstream effects of an HCW being infected. Finally, it did not take visitors into account, either intrapartum or postpartum.
The primary outcome was the cost to prevent one COVID-19 infection in an HCW. We used a cost-effectiveness (willingness-to-pay) threshold of $25,000, which was an estimate of the immediate costs of a COVID-19 infection in an HCW. To calculate this cost, we used data regarding the costs of hospitalization and ICU care for influenza patients, as well as the median wage of a HCW. 17 18 We accounted for the probability of different outcomes of COVID-19 (homecare, hospitalization, ICU admission, and fatality), as well as the immediate lost wages while the HCW was out of work. 19
In addition to the base case analysis, we performed one- and two-way sensitivity analyses. In particular, this allowed us to assess whether there was a threshold COVID-19 prevalence where universal PPE was the preferred strategy and how varying the willingness-to-pay changed this threshold. Finally, Monte Carlo simulation (a computational algorithm that relies on repeated random sampling of all variables across their confidence intervals based on their distributions) was utilized given the uncertainty of many of the point estimates. In the Monte Carlo simulation, β distributions were used for probability estimates, log normal distributions were used for relative risks, and γ distributions were used for cost variables. Given the plausible variation in all of the probabilities and cost estimates included in the model, no variable was excluded from the Monte Carlo analysis. Each obstetrician scenario was run with 100,000 samples.
We performed all analyses using TreeAge Pro 2020Suite (TreeAge Software, Inc., Williamstown, MA). The study did not involve human subjects and was exempt from institutional review board approval.
Results
In the base case assuming a COVID-19 prevalence of 0.36%, universal PPE is more costly but also more effective at preventing COVID-19 transmission than universal screening for spontaneous and induced labor, with a cost to prevent transmission to one HCW of $4,175,229 and $3,413,251, respectively ( Table 2 ). Therefore, for spontaneous and induced labor, universal screening is the preferred strategy given the high cost of universal PPE in the base case. However, for a planned CD, universal PPE is cost saving (less costly and more effective) compared with universal screening.
Table 2. Cost to prevent infection in one health care worker using universal personal protective equipment at different prevalence rates of COVID-19.
| Location/prevalence rate a | Spontaneous labor | Induced labor |
|---|---|---|
| Los Angeles County, CA Rate = 0.26% |
$5,830,270 | $4,766,801 |
| King County, WA Rate = 0.29% |
$5,216,552 | $4,264,792 |
| United States Rate = 0.36% |
$4,175,229 | $3,413,251 |
| Cook County, IL Rate = 0.82% |
$1,802,710 | $1,473,017 |
| New York City, NY Rate = 1.99% |
$732,912 | $598,174 |
| Westchester County, NY Rate = 3.09% |
$465,986 | $379,897 |
| Rate = 5% | $280,742 | $228,391 |
| Rate = 10% | $131,019 | $105,949 |
| Rate = 15% | $81,111 | $65,139 |
| Rate = 20% | $56,157 | $44,733 |
Prevalence rates from May 4, 2020 with data from Johns Hopkins Coronavirus Resource Center and population estimates from the U.S. Census Bureau (July 2019 population estimate).
Note: Universal personal protective equipment use remained cost saving for planned cesarean sections, regardless of the prevalence of COVID-19.
In sensitivity analysis, the model is most sensitive to the prevalence of COVID-19, the cost of the COVID-19 test, and the cost of PPE. Assuming a willingness to pay (cost-effectiveness threshold) of $25,000, universal PPE becomes cost-effective at a COVID-19 prevalence of 34.27 and 29.54% for spontaneous and induced labor, respectively. Below those prevalence thresholds, universal screening is the preferred strategy. We varied the prevalence of COVID-19 to reflect reported estimates in different regions of the United States ( Table 2 ). We additionally evaluated prevalence thresholds by willingness to pay ( Fig. 2 ). Notably, if we are instead willing to pay $100,000 to prevent transmission to a HCW (the amount typically assumed would be paid for one quality adjusted life year), universal PPE is cost-effective at a COVID-19 prevalence of 12.7 and 10.6% for spontaneous and induced labor, respectively. For a planned CD, universal PPE is cost saving regardless of COVID-19 prevalence.
Fig. 2.
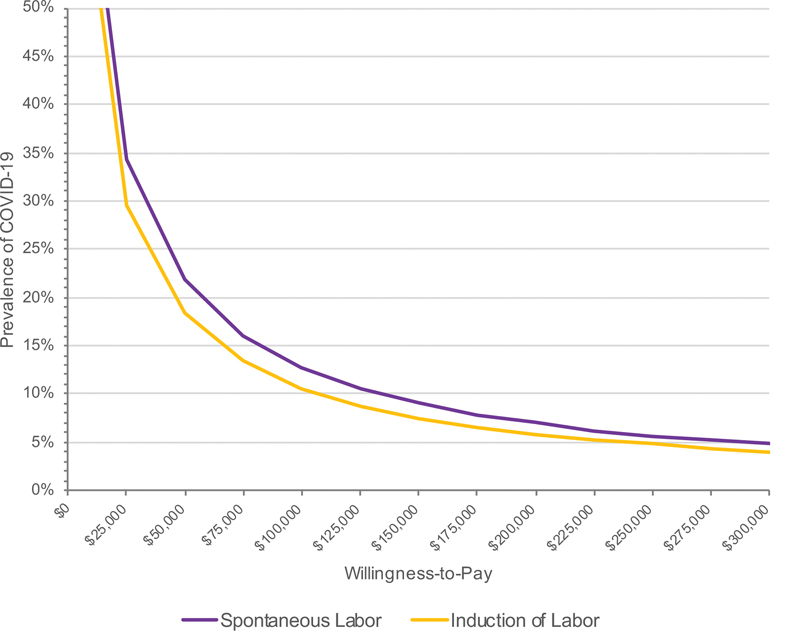
Prevalence of coronavirus disease 2019 versus willingness to pay to prevent transmission to one health care worker for spontaneous and induced labor. Each line shows the prevalence threshold at which the cost to prevent one health care worker infection is equal to that willingness to pay.
Varying the cost of the COVID-19 test (base case $200) changes the outcome for all modes of delivery. Universal PPE becomes cost-effective when the cost of the test exceeds $512.62 and $463.20 for spontaneous and induced labor, respectively. For planned CD, universal PPE is the cost-effective option starting at a cost of $93.18 per test. Finally, varying the cost of PPE for a VD and unplanned CD do not change the outcome of the model. However, for a planned CD, universal PPE is only cost-effective when the cost of PPE for the hospitalization is less than $201.81 (base case $95.71).
In additional one-way sensitivity analyses, the COVID-19 test characteristics, the likelihood of transmission without PPE, the reduction in transmission risk with PPE, requiring that all symptomatic and COVID-19 positive patients wear a mask, and universal patient masking have minimal effect on the model at clinically relevant values.
In two-way sensitivity analyses, we further examined the scenario of a planned CD. Evaluating the cost of PPE and the prevalence of COVID-19 in the setting of a planned CD, universal screening is the cost-effective option at higher PPE costs and lower prevalence rates. Similarly, in three-way sensitivity analysis evaluating the cost of PPE, the prevalence of COVID-19, and the probability of transmission to an HCW as the probability of transmission to an HCW decreases, universal screening becomes cost-effective at lower prevalence rates ( Fig. 3 ).
Fig. 3.
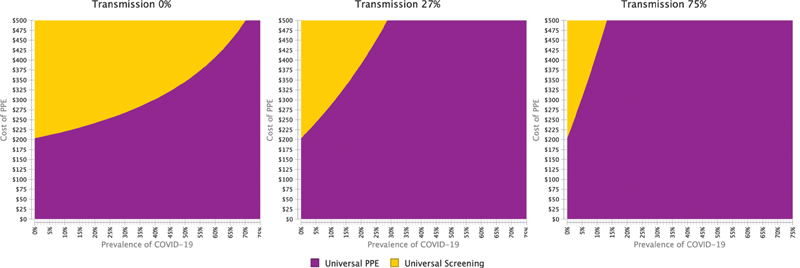
Two-way sensitivity analysis of the prevalence of coronavirus disease 2019 and the cost of personal protective equipment for a cesarean delivery. The colors represent when that strategy is cost-effective at a willingness to pay of $25,000. The first graph shows the relationship if the likelihood of transmission to a health care worker is 0%, the second shows the relationship if the likelihood of transmission is 27% (base case), and the third shows the relationship if the likelihood of transmission is 75%.
A Monte Carlo simulation was performed to simulate the outcome of 100,000 women who were randomized to the two strategies. Universal screening was the preferred strategy at a willingness to pay of $25,000 in 60.1, 57.4, and 17.2% of simulation for spontaneous labor, induced labor, and planned CD, respectively. At a willingness to pay of $100,000, universal screening was the preferred strategy in 59.5, 56.8, and 14.4% of simulation for spontaneous labor, induced labor, and planned CD, respectively.
Discussion
This analysis demonstrates that the preferred strategy for screening and PPE usage on L&D in the setting of the COVID-19 pandemic varies by the type of admission and is highly related to the underlying prevalence of COVID-19 in the community. At relatively low prevalence of disease (<10%) as is thought to be the case at this time throughout most of the United States, universal screening is the preferred strategy for women presenting in spontaneous labor and for labor induction. Interestingly for planned CD, universal PPE was more often cost-effective, and therefore, the preferred strategy as long as the cost of said PPE remains stable. For all scenarios, we argue that the cheaper strategy should be preferred until the cost-effectiveness threshold.
At high-disease prevalence, universal PPE is how best to protect HCW. While not feasible in our current system, this result argues for enhanced preparedness in the future to allow for increased supply of PPE or for rapid enhancement of production capabilities. This is additionally important because testing will necessarily lag, at least slightly, behind any novel outbreak. Even if universal PPE is not recommended in the long term, it may be beneficial to implement it as the preferred strategy in the short term, or at the peak of the outbreak in a given area.
This model relies on the ability to screen all women on L&D for COVID-19, by using a standard test prior to a planned admission or a rapid test upon arrival to L&D for unplanned admissions. We understand that in some hospitals universal testing is not feasible given limited test supplies in general or where a rapid test is entirely unavailable. Unfortunately, a test result that takes 8, 12, or 24 hours to result will likely not be helpful for unplanned admissions on L&D when decisions usually have to be made more rapidly than that. This model also assumes that no additional PPE is used nor HCWs exposed prior to knowing the results of the test.
Our model is highly sensitive on our chosen willingness-to-pay to prevent one COVID-19 infection in an HCW. The chosen threshold of $25,000 is based purely on direct costs and lost wages. In locations with, for example, many critical care specialists, one HCW infection is likely not to be hard on that community. However, in locations especially rural areas, where there is one critical care specialist; if that person becomes sick, it could severely impact the community. In this setting, the willingness to pay to prevent that one HCW infection is likely to be significantly higher than $25,000. In these places, universal PPE might be preferred. Because different hospitals and locations can implement different policies, locations with the highest COVID-19 prevalence or with the fewest HCWs may want to implement universal PPE, and PPE could be preferentially routed to those locations. In locations where the prevalence is lower, or the number of available HCWs is higher, universal screening is likely preferred and could help to preserve PPE.
The strengths of this study are the ability to evaluate large ranges of possible probabilities given the current limited data. Additionally, this is the only decision analysis we are aware of that has evaluated strategies for PPE use to prevent disease spread on L&D.
The major limitation is the paucity of data surrounding the current COVID-19 pandemic, and a model is only as good as the data that is available to be used. Additionally, given that there is new information about COVID-19 on a daily basis, the information in this analysis may prove to be incorrect. To overcome this limitation, we varied our base case estimates widely. Additionally, we did not consider visitors or support people in our model. Many hospitals have implemented restrictive visitor policies with some requiring that visitors wear masks. Both restrictive visitor policies as well as masking will likely help to limit spread to HCW. Finally, we did not account for the long-term consequences of COVID-19 infection, as many of those consequences are not yet known.
There is limited information surrounding the current COVID-19 pandemic. This model uses data from prior pandemics to determine the likelihood of transmission, but further research should be performed to determine the specific risks of transmission with COVID-19. Furthermore, once available, updated costs regarding the long-term consequences of COVID-19 infection could be included in a future model.
Universal PPE is the best method to prevent infection in HCW; however, it is not necessarily feasible based on both availability and cost. Therefore, efforts to increase screening capability should continue to be a public health focus. Overall, we believe that this model applies a different lens to the current pandemic and will allow us to make decisions about hospital policy and allocation of resources, keeping in mind both cost and effect, as we face the next phase of the COVID-19 pandemic and as we inevitably face the next pandemic.
Funding Statement
Funding None.
Footnotes
Conflict of Interest None declared.
References
- 1.WHO. Novel coronavirus – China. WHO. Available at:http://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/. April 15, 2020
- 2.CDC. Coronavirus disease 2019 (COVID-19) in the U.S. Centers for Disease Control and Prevention. Available at:https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed May 4, 2020
- 3.Guan W-J, Ni Z-Y, Hu Y et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi: 10.1056/NEJMoa2002032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sutton D, Fuchs K, D'Alton M, Goffman D. Universal screening for SARS-CoV-2 in women admitted for delivery. N Engl J Med. 2020;382(22):2163–2164. doi: 10.1056/NEJMc2009316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zou L, Ruan F, Huang M et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177–1179. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.COVID-19 Map. Johns hopkins coronavirus resource center. Available at:https://coronavirus.jhu.edu/map.html. Accessed May 4, 2020
- 7.Breslin N, Baptiste C, Gyamfi-Bannerman C et al. COVID-19 infection among asymptomatic and symptomatic pregnant women: two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am J Obstet Gynecol MFM. doi: 10.1016/j.ajogmf.2020.100118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Grobman W A, Rice M M, Reddy U M et al. Labor induction versus expectant management in low-risk nulliparous women. N Engl J Med. 2018;379(06):513–523. doi: 10.1056/NEJMoa1800566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Liu Y, Gayle A A, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020;27(02):taaa021. doi: 10.1093/jtm/taaa021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhang S, Diao M, Yu W, Pei L, Lin Z, Chen D. Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: a data-driven analysis. Int J Infect Dis. 2020;93:201–204. doi: 10.1016/j.ijid.2020.02.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature. BMC Infect Dis. 2014;14:480. doi: 10.1186/1471-2334-14-480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haber M J, Shay D K, Davis X M et al. Effectiveness of interventions to reduce contact rates during a simulated influenza pandemic. Emerg Infect Dis. 2007;13(04):581–589. doi: 10.3201/eid1304.060828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhang J, Landy H J, Branch D W et al. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet Gynecol. 2010;116(06):1281–1287. doi: 10.1097/AOG.0b013e3181fdef6e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Teleman M D, Boudville I C, Heng B H, Zhu D, Leo Y S. Factors associated with transmission of severe acute respiratory syndrome among health-care workers in Singapore. Epidemiol Infect. 2004;132(05):797–803. doi: 10.1017/s0950268804002766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fay E E, Hitti J E, Delgado C M et al. An enhanced recovery after surgery pathway for cesarean delivery decreases hospital stay and cost. Am J Obstet Gynecol. 2019;221(04):3490–3.49E11. doi: 10.1016/j.ajog.2019.06.041. [DOI] [PubMed] [Google Scholar]
- 16.American Health Insurance PlansRecent Trends in Hospital Prices in California and OregonAvailable at:http://www.ahipresearch.org/pdfs/PricesCaliforniaOregon2010.pd. Accessed December 2010
- 17.Khazeni N, Hutton D W, Garber A M, Hupert N, Owens D K. Effectiveness and cost-effectiveness of vaccination against pandemic influenza (H1N1) 2009. Ann Intern Med. 2009;151(12):829–839. doi: 10.1059/0003-4819-151-12-200912150-00157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.US Department of Labor. Bureau of Labor Statistics. Occupational Outlook Handbook, Healthcare Occupations. Available at:https://www.bls.gov/ooh/healthcare/mobile/home.htm. Accessed April 16, 2020
- 19.CDCMMWR. Severe outcomes among patients with coronavirus disease 2019 (COVID-19) — United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep.202069. Doi: 10.15585/mmwr.mm6912e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.U.S. Census Bureau QuickFacts. United States. Available at:https://www.census.gov/quickfacts/fact/table/US/PST045219. Accessed May 4, 2020.
- 21.Administrator J website. Global Progress on COVID-19 Serology-Based Testing. Johns Hopkins Center for Health Security. Available at:https://www.centerforhealthsecurity.org/resources/COVID-19/serology/Serology-based-tests-for-COVID-19.html. Accessed April 15, 2020
- 22.Sheridan C. Fast, portable tests come online to curb coronavirus pandemic. Nat Biotechnol. 2020;38(05):515–518. doi: 10.1038/d41587-020-00010-2. [DOI] [PubMed] [Google Scholar]