

Suspension of elective surgical care during COVID-19 will result in a large backlog of cataract surgeries in Medicare beneficiaries. It is necessary to start planning proactively to reduce the backlog.
Abstract
Purpose:
To forecast the volume of cataract surgery in Medicare beneficiaries in the United States in 2020 and to estimate the surgical backlog that may be created due to COVID-19.
Design:
Epidemiologic modeling.
Methods:
Baseline trends in cataract surgery among Medicare beneficiaries were assessed by querying the Medicare Part B Provider Utilization National Summary data. It was assumed that once the surgical deferment is over, there will be a ramp-up period; this was modeled using a stochastic Monte Carlo simulation. Total surgical backlog 2 years postsuspension was estimated. Sensitivity analyses were used to test model assumptions.
Results:
Assuming cataract surgeries were to resume in May 2020, it would take 4 months under an optimistic scenario to revert to 90% of the expected pre-COVID forecasted volume. At 2-year postsuspension, the resulting backlog would be between 1.1 and 1.6 million cases. Sensitivity analyses revealed that a substantial surgical backlog would remain despite potentially lower surgical demand in the future.
Conclusions:
Suspension of elective cataract surgical care during the COVID-19 surge might have a lasting impact on ophthalmology and will likely result in a cataract surgical patient backlog. These data may aid physicians, payers, and policymakers in planning for postpandemic recovery.
The volume of cataract surgeries performed per year has increased steadily over the past few decades in the United States.1–3 Advancements in technology have resulted in enhanced safety and improved visual outcomes, resulting in more second-eye surgeries being performed, and a lower visual threshold for performing vision correction cataract surgery in younger patients.4 Furthermore, increased utilization of ambulatory surgical centers in the past few years has improved efficiency and contributed to greater cataract surgical volume.5
The ongoing COVID-19 pandemic resulted in a temporary halt in all elective ophthalmic surgeries. Although an important step, the impact of this suspension on current and future volume of cataract surgery is unknown. In this investigation, our goals were (1) to model the volume of cataract surgery in Medicare beneficiaries in 2020 in light of COVID-19 and (2) to estimate the surgical backlog that might have been created due to elective surgery suspension and subsequent ramp-up. Backlog in this context refers to surgical cases that have been indicated and the patient has consented to surgery, however, the surgical case has not yet been performed.
METHODS
Patient Population
Medicare Part B Provider Utilization National Summary from 2008 to 2018, which contains summary statistics of the 100% sample of the Medicare Part B claims data, was queried.6 The total volume of cataract surgeries for a given year was calculated by adding the number of surgical claims for Current Procedure Terminology (CPT) code 66984, extracapsular cataract removal with insertion of intraocular lens (IOL) prosthesis, and claims for CPT code 66982, extracapsular cataract removal with insertion of IOL–prosthesis complex. These data were used for subsequent analyses. The study adhered to the tenets of Declaration of Helsinki; institutional review board approval was not required as the data was derived from a free, publicly available resource that did not contain any patient-level data.
Prepandemic Forecast of Cataract Surgeries
The cataract surgery volume that might have been performed in the year 2020 based on pre-COVID trends from 2008 to 2018 was forecasted with linear regression model.
Cataract Surgeries From January to May 2020
It was assumed that 100% of the prepandemic forecasted volume was performed in January and February 2020. For the number of cases performed between March and May 2020, estimates based on the practice patterns of the first author (S.A.) were used, which is a busy multisurgeon ophthalmology community practice. Based on the practice patterns, it was assumed that 50% of the volume was performed in March 2020 and 3% in April 2020 (at the peak of the suspension). In most states in the United States, the mandated suspension on elective surgeries ended early in May. For example, in the state of Maryland, they ended on May 6, and in the first author's practice, they performed 50% of the previous year's surgical volume for the month of May. However, other practices in the community lagged due to operational considerations. In another practice in the same state, only 30% of the previous year's volume was performed in May. Furthermore, nationally, not all states allowed resumption of elective surgery in early May, and some states did not allow this until mid-May. Thus, it was assumed that the national volume of cataract performed in May 2020 would be 40% of expected.
Forecast of Cataract Surgeries
It was assumed that once the elective surgical suspension period is over, there would be a ramp-up period, and the volume of cataract surgeries performed would not immediately revert back to 100% of the prepandemic forecast. To model the ramp-up, a stochastic Monte Carlo simulation of a Gompertz function in a manner similar to that described for an elective orthopedic surgical population was used.7 A Gompertz function is a sigmoid curve with a rapid acceleration phase followed by a plateau phase.8 It has been previously used to describe a variety of biological growth and recovery phenomena.9 The rise in volume of cataract surgeries postpandemic was forecasted under an optimistic and a pessimistic scenario; we arbitrarily assumed growth velocities of 90% and 50% for the 2 scenarios, respectively. The growth velocities do not refer to a linear percentage change in surgical volume but are variables in the Gompertz function that affect the nonlinear slope of the ramp-up phase. The 90% and 50% were chosen as the bounds of the likely scenario. These assumptions were further tested with sensitivity analyses as described further. The primary outcome of interest was the number of months it would take until the number of cataract surgeries performed would reach 90% of the prepandemic forecasted volume.
Backlog Estimation
The total backlog of cataract surgeries was calculated by adding the fixed backlog (created from March to May 2020, when surgeries were deferred) with the new backlog (created from June 2020 onward during ramp-up, when the number of surgeries performed in a given month is less than 100% of the capacity). The outcome of interest was the total number of surgical cataract cases that would be backlogged 2-year postsuspension (May 2022).
Sensitivity Analyses
To model the uncertainty in our assumptions, one-way sensitivity analyses were conducted. Because the growth rates in the optimistic and pessimistic scenarios were chosen arbitrarily, first, the impact of ranging the growth rates from 30% to 95% was simulated. The minimum possible growth rate was assumed to be at least 30% because most centers would be able to be up and running, at least to some capacity, due to the ambulatory nature of our practice. It is possible that hospital-based practices might have a slower ramp-up phase due to lack of hospital operating room availability.
The second analysis investigated what would happen if the number of cases deferred during the pandemic was not as large as modeled. This was tested by varying the fixed backlog from −50% to +50%.
Third analysis investigated what would happen if the future demand for cataract surgery were to decline in response to the pandemic. The impact of decline in elective surgical demand was modeled to be from −10% to −30%.
A fourth analysis estimated the amount of time it would take to catch up on backlog under the ideal conditions. In this scenario, the growth rate was assumed to be 95%, fixed backlog to be −50%, and future demand to be −30%, and it would continue to grow at 10% per month after reaching the plateau phase.
Statistical Methods
Stata IC/15.0 (StataCorp) was used for all analyses. Monte Carlo simulations were run for 10 000 runs for each scenario. The number of cases were rounded to the nearest 10 000 throughout the manuscript for ease of read.
RESULTS
Forecast of Cataract Surgeries
Once elective surgical suspension is lifted and surgeries resume, the Monte Carlo simulation revealed that under the optimistic scenario, it would take 4 months to revert to 90% of the prepandemic forecasted volume (performing at least 280 000 cases per month). Under the pessimistic scenario, it would take 7 months (Figure 1). In both scenarios, the size of the surgical cataract case backlog at 2-year postsuspension (May 2022) would be tremendous: 1 080 000 cases in the optimistic scenario, and 1 550 000 cases in the pessimistic scenario (Figure 2).
Figure 1.
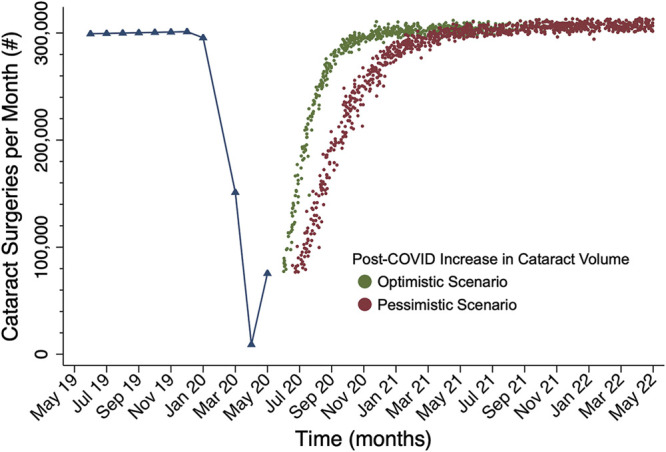
Monte Carlo simulation of elective cataract surgeries among Medicare beneficiaries in the United States post-COVID. Forecasted cataract surgery volume per month.
Figure 2.
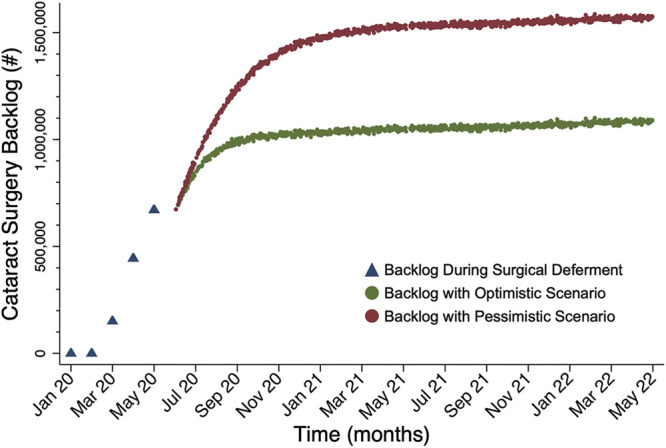
Backlog of cataract surgeries post-COVID. Forecasted cumulative backlog of cataract surgeries over time.
Sensitivity Analyses
Varying the growth velocity from 30% to 95% resulted in significant variation in the time to revert to 90% of the prepandemic forecasted volume. With a 30% growth rate, it would take 12 months, whereas with a 95% growth rate, it would take 3.5 months to recover. Varying the fixed backlog from −50% to +50% resulted in the total backlog at 2-year post-suspension ranging from: 740 000 to 1 420 000 cases, respectively, assuming the optimistic scenario growth (90%) rate.
Of interest, the backlog persisted despite varying surgical demand in the sensitivity analysis. Under the optimistic recovery model, if surgical demand decreased by 10%, the backlog would be 990 000 cases at 2 years, and if demand decreased by 30%, there would be a backlog of 850 000 cases at 2 years. Under the backlog minimization scenario where growth rate was assumed to be 95%, fixed backlog was assumed to be −50%, and future demand was assumed to be −30%, with a compounded 10% per month growth rate, it would still take 9 months to catch-up on the backlog.
DISCUSSION
Based on the trends in surgical volume of cataract surgery over the past decade, 3.7 million cataract cases would have been performed in 2020 in the United States among Medicare beneficiaries. However, the COVID-19 pandemic has resulted in a large-scale disruption of healthcare. Although many centers are restarting surgery, because of safety concerns and operational and supply chain considerations, the ramp-up is restrained. There is significant uncertainty about volume of elective surgeries. In this article, we explored these issues. Our analysis indicates that suspension of elective cataract surgical care will have a lasting impact on ophthalmology and will likely result in a sizeable backlog.
The suspension of elective cases during COVID surge was an important step for safety of both patients and surgical teams. Viral transmission through aerosols and fomites and prolonged infectivity of virions in aerosols are a threat. A case series from China found that of 34 asymptomatic patients who underwent elective surgery during the incubation period of COVID-19, the mortality rate was an alarming 20%.10
Now that the suspension is over, the surgical volume might not revert to pre-COVID forecasts immediately for a variety of reasons. Because this event is unprecedented in modern medicine, the growth velocity at which the volume of cataract surgery would ramp-up is unknown. Using simulation techniques, we modeled a range of scenarios and found that it would take a minimum of 4 months to revert to near prepandemic forecasted volume even under optimistic conditions with high (90%) growth velocity. Unlike other surgical disciplines that might be more reliant on expansive resources such as intensive care and inpatient hospitalization, it might be possible to reach high ramp-up velocities in ophthalmology due to outpatient nature of surgeries and relatively limited resource footprint. However, this ramp-up might vary based on different states. For example, in the first author's practice, in the state of Maryland, it was possible to go from 4% of the previous year's volume performed in April 2020 to 50% of the previous year's volume performed in May 2020 at the author's practice. By contrast, in California, because of regulations, many ambulatory surgical centers had slower opening, and the surgical volume at most centers for May did not reach that level. It is difficult to predict how the regulator decisions in each state would affect ramp-up. Furthermore, patient care logistics, such as surgical consultation, consent, and preoperative medical and financial clearance, will contribute to the ramp-up time. In the future, we will be able to ascertain the real growth velocities based on retrospective review of actual surgical volume. The estimated forecasts in our study provide a benchmark to compare actual future volume against.
Regardless of the growth velocity during the ramp-up period, a substantial backlog is likely. The source of the backlog is both the cases that are deferred during the suspension period and the additional cases that are not being performed while the production is not at 100% capacity during the ramp-up phase. Our analysis reveals that even under optimistic conditions, the backlog would be greater than 1 million surgical cataract cases at 2 years postsuspension. Even in the backlog minimization sensitivity analysis with all ideal conditions, it would take 9 months to catch up on the backlog.
The impact of COVID on elective surgery demand is also unclear. With the aging of the population and innovations in treatment, the demand for cataract surgery has been steadily increasing over the past 2 decades.4 The sensitivity analysis reveals that even if demand fell by 30%, a substantial surgical backlog would remain. Furthermore, there have been several studies that document adverse events arising from delay in cataract treatment, such as depression, falls, and traffic accidents.11–13 It is possible that we might see a rise in these events in the Medicare population. For instance, a systematic review of 27 studies found that patients who waited more than 6 months for surgery had worse outcomes compared with patients who waited <6 weeks, such as worse vision and poor quality of life.14
Addressing the backlog would require eventually increasing production beyond the prepandemic levels. This necessitates proactive planning. Greater efficiency is required in preoperative components such as: measurements for IOLs, presurgical imaging, and medical and financial clearance. Establishing collaborative and cohesive relationships with our optometry colleagues will be critical to expand access to care and triage. Increasing available operative time and space per surgeon might help increase throughput. When appropriate, using topical anesthesia for cataract surgery might aid in the efficiency.15 For surgeons who prefer femtosecond laser–assisted cataract surgery, strategies to improve workflow and reduce time such as moving the laser to the operating room or alternatives to laser-assisted capsulotomy such as zepto and miLoop for dense lenses might be of consideration.16–19 Furthermore, same-day sequential cataract surgery might be considered for patients needing bilateral surgery owing to considerations of anisometropia and intended monovision.20 It might be possible to covert some postoperative visits to telemedicine or to defer them altogether without compromising patient safety.21,22 There are insufficient real-world data to assess how the aforementioned various strategies might increase throughput and potentially help diminish the backlog. Production would have to increase beyond previous throughput levels to catch up on the backlog. This might be a potential direction for future health services research in ophthalmology.
Another important point is that keeping ophthalmology practices solvent through governmental and private aid would be critical to preserving the workforce and taking care of the population. A secondary analysis we performed indicates that once we reach prepandemic surgical volume, we would have to keep growing at a compounded rate of 10% per month to start reducing the backlog and go beyond the 100% throughput compared with what was being performed previously. However, despite best efforts and surgeon's desires to increase throughput, it might not be possible to increase throughput at this extreme rate owing to a variety of health system constraints. One such constraint in the foreseeable future is that surgical centers are limiting the number of cases to maintain social distancing guidelines and reduce infection spread.
Our study has multiple limitations. First, we do not account for second or other future waves of the pandemic. This adds significant uncertainty that might influence the backlog estimations. Second, we focused on Medicare beneficiaries, which underestimate the total volume of cataract surgeries in the United States. However, according to the Centers of Disease Control Vision and Eye Health Surveillance System, approximately 80% of the patients who underwent cataract surgery in the United States in 2016 were Medicare beneficiaries.23 Furthermore, we did not take into account the potential seasonality of cataract surgery because the number of surgeries performed each month might potentially vary depending on the geographical region of the country. Despite these assumptions, our sensitivity analyses revealed that although the magnitude might vary, there inevitably will be a surgical cataract backlog, even in the face of potential reduced demand.
In conclusions, suspension of elective cataract surgical care during the COVID surge will have a significant and lasting impact on Ophthalmology and will likely result in a large surgical backlog. Addressing the backlog through proactive planning would be vital to success. Our data might aid physicians, payers, and policymakers in planning for postpandemic recovery.
WHAT WAS KNOWN
Suspension of elective surgery during COVID-19 has impacted surgical cataract volumes.
WHAT THIS STUDY ADDS
This study provides a numerical estimate of how long it will take to revert to near prepandemic levels and much surgical cataract backlog will be created over time.
Footnotes
Disclosures: None of the authors has a financial or proprietary interest in any material or method mentioned.
REFERENCES
- 1.Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg 2013;39:1383–1389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hatch WV, Campbell Ede L, Bell CM, El-Defrawy SR, Campbell RJ. Projecting the growth of cataract surgery during the next 25 years. Arch Ophthalmol 2012;130:1479–1481 [DOI] [PubMed] [Google Scholar]
- 3.Klein BEK, Howard KP, Lee KE, Klein R. Changing incidence of lens extraction over 20 years: the Beaver Dam eye study. Ophthalmology 2014;121:5–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Erie JC. Rising cataract surgery rates: demand and supply. Ophthalmology 2014;121:2–4 [DOI] [PubMed] [Google Scholar]
- 5.Stagg BC, Talwar N, Mattox C, Lee PP, Stein JD. Trends in use of ambulatory surgery centers for cataract surgery in the United States, 2001-2014. JAMA Ophthalmol 2018;136:53–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Centers for Medicare and Medicaid Services. Part B National Summary Data File. 2008-2018. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/Part-B-National-Summary-Data-File/Overview. Accessed June 22, 2020 [Google Scholar]
- 7.Jain A, Jain P, Aggarwal S. SARS-CoV-2 impact on elective orthopaedic surgery: post-pandemic recovery implications. J Bone Joint Surg Am 2020. In Press [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gompertz B. On the nature of the function expressive of the law of human mortality, and on a new mode of determining the value of life contingencies. Philos Trans R Soc Lond B Biol Sci 1825;182:513–585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tjørve KMC, Tjørve E. The use of Gompertz models in growth analyses, and new Gompertz model approach: an addition to the Unified Richards family. PLoS One 2017;12:1–17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lei S, Jiang F, Su W, Chen C, Chen J, Mei W, Zhan LY, Jia Y, Zhang L, Liu D, Xia ZY, Xia Z. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 2020;21:100331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gimbel HV, Dardzhikova AA. Consequences of waiting for cataract surgery. Curr Opin Ophthalmol 2011;22:28–30 [DOI] [PubMed] [Google Scholar]
- 12.Palagyi A, Rogers K, Meuleners L, McCluskey P, White A, Ng JQ, Morlet N, Keay L. Depressive symptoms in older adults awaiting cataract surgery. Clin Exp Ophthalmol 2016;44:789–796 [DOI] [PubMed] [Google Scholar]
- 13.Schlenker MB, Thiruchelvam D, Redelmeier DA. Association of cataract surgery with traffic crashes. JAMA Ophthalmol 2018;136:998–1007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hodge W, Horsley T, Albiani D, Baryla J, Belliveau M, Buhrmann R, O'Connor M, Blair J, Lowcock E. The consequences of waiting for cataract surgery: a systematic review. CMAJ 2007;176:1285–1290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nderitu P, Ursell P. Factors affecting cataract surgery operating time among trainees and consultants. J Cataract Refract Surg 2019;45:816–822 [DOI] [PubMed] [Google Scholar]
- 16.Agarwal A, Jacob S. Current and effective advantages of femto phacoemulsification. Curr Opin Ophthalmol 2017;28:49–57 [DOI] [PubMed] [Google Scholar]
- 17.Gupta PC, Ram J. Femtosecond laser-assisted cataract surgery in complex cases. J Cataract Refract Surg 2016;42:1693. [DOI] [PubMed] [Google Scholar]
- 18.Hooshmand J, Abell RG, Allen P, Vote BJ. Thermal capsulotomy: initial clinical experience, intraoperative performance, safety, and early postoperative outcomes of precision pulse capsulotomy technology. J Cataract Refract Surg 2018;44:355–361 [DOI] [PubMed] [Google Scholar]
- 19.Ianchulev T, Chang DF, Koo E, MacDonald S, Calvo E, Tyson FT, Vasquez A, Ahmed IIK. Microinterventional endocapsular nucleus disassembly: novel technique and results of first-in-human randomised controlled study. Br J Ophthalmol 2019;103:176–180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Singh R, Dohlman TH, Sun G. Immediately sequential bilateral cataract surgery: advantages and disadvantages. Curr Opin Ophthalmol 2017;28:81–86 [DOI] [PubMed] [Google Scholar]
- 21.Kessel L, Andresen J, Erngaard D, Flesner P, Tendal B, Hjortdal J. Safety of deferring review after uneventful cataract surgery until 2 weeks postoperatively. J Cataract Refract Surg 2015;41:2755–2764 [DOI] [PubMed] [Google Scholar]
- 22.Saeed A, Guerin M, Khan I, Keane P, Stack J, Hayes P, Tormey P, Mullhern M, Beatty S. Deferral of first review after uneventful phacoemulsification cataract surgery until 2 weeks: randomized controlled study. J Cataract Refract Surg 2007;33:1591–1596 [DOI] [PubMed] [Google Scholar]
- 23.Centers for Disease Control and Prevention. Vision and Eye Health Surveillance System. Available at: https://www.cdc.gov/visionhealth/vehss/index.html. Accessed on June 22, 2020 [Google Scholar]