

Supplemental Digital Content is available in the text.
Keywords: acute respiratory distress syndrome, coronavirus disease 2019, critical care, prone, transthoracic echocardiography, ultrasound
Abstract
Objectives:
Patients with acute respiratory distress syndrome are at risk for developing cardiac dysfunction which is independently associated with worse outcomes. Transthoracic echocardiography is an ideal imaging modality for goal-directed assessment and optimization of cardiac function and volume status. Prone positioning, while demonstrated to improve oxygenation, offload the right ventricle, and reduce short-term mortality in acute respiratory distress syndrome, has previously precluded transthoracic echocardiography on these patients. The purpose of this study was to assess the ability to perform focused transthoracic echocardiography examinations on acute respiratory distress syndrome patients in the prone position.
Design:
We performed a cross-sectional study of critically ill patients hospitalized for acute respiratory distress syndrome due to coronavirus disease 2019.
Setting:
This study was conducted in medical and surgical intensive units in a tertiary hospital.
Patients:
We examined 27 mechanically ventilated and prone patients with acute respiratory distress syndrome due to coronavirus disease 2019. Participants were examined at the time of enrollment in an ongoing clinical trial (NCT04306393), and no patients were excluded from echocardiographic analysis.
Interventions:
None.
Measurements and Main Results:
We were able to perform transthoracic echocardiography and obtain satisfactory images for quantitative assessment of right ventricular function in 24 out of 27 (88.9%) and left ventricular function in 26 out of 27 (96.3%) of patients in the prone position, including many who were obese and on high levels of positive end-expiratory pressure (≥ 15 cm H2O).
Conclusions:
Transthoracic echocardiography can be performed at the prone patient’s bedside by critical care intensivists. These findings encourage the use of focused transthoracic echocardiography for goal-directed cardiac assessment in acute respiratory distress syndrome patients undergoing prone positioning.
The coronavirus disease 2019 (COVID-19) pandemic has resulted in a drastic increase in the number of patients with acute respiratory distress syndrome (ARDS), many of whom will require prone positioning to improve oxygenation. Transthoracic echocardiography (TTE) is a noninvasive tool that can provide a rapid assessment of cardiac function and volume status. It is often used to guide management by assessing response to interventions or to perform serial monitoring. Focused TTE assessment in ARDS patients may offer clinical benefits from hemodynamic monitoring and optimization of cardiac function and volume status to facilitate weaning from mechanical ventilation (1, 2). Prone positioning, while demonstrated to increase oxygenation and reduce mortality in ARDS (1), has previously precluded TTE examinations due to the perception that transthoracic windows cannot be obtained in the prone position. In this study, we describe a technique and demonstrate the feasibility of performing focused TTE examinations on mechanically ventilated patients with COVID-19 ARDS in the prone position.
MATERIALS AND METHODS
We performed TTE on critically ill adults with ARDS secondary to COVID-19 infection admitted to the medical and surgical ICUs at a tertiary hospital. Patients were examined at the time of enrollment in an institutional review board-approved randomized clinical trial of nitric oxide versus placebo for the treatment of COVID-19 (NCT04306393). All patients were intubated and receiving mechanical ventilation at the time of examination. Our study population was subject to the exclusion criteria of the trial which included a history of lung malignancy or lung transplant, the presence of severe burns (> 40% body surface area), the presence or presumed presence of severe neurologic deficit, those receiving renal replacement therapy, or the presence of an irreversible condition with 6-month mortality greater than 50%. No patients were excluded from echocardiographic analysis once enrolled in the trial.
Image Acquisition and Review
TTE images were obtained using the Philips CX50 portable ultrasound machine (Philips Healthcare, Andover, MA) and a phased array transducer. A three-lead electrocardiogram was recorded throughout each examination, with lead placement as follows: right arm lead on the patient’s right shoulder, left arm lead on the patient’s left shoulder, and left leg lead on the patient’s left flank. All examinations were performed by Dr. Gibson. All images, including quantitative assessments, were reviewed for adequacy through visual inspection by an intensivist (M.G.C.) certified in critical care echocardiography by the National Board of Echocardiography. Studies were interpreted by discussion between the examiner (L.E.G.) and the certified intensivist (M.G.C.).
Patient Positioning
We used the “swimmer position” to perform TTE on prone patients (3). To achieve this, the patient’s left arm was extended overhead at the shoulder with the elbow bent. A pillow was placed under the left shoulder to slightly elevate the lateral chest from the bed, allowing space for the ultrasound transducer. In order to prevent disruption of the endotracheal tube from the extended left arm, the patient’s head was turned to the right (Fig. 1).
Figure 1.
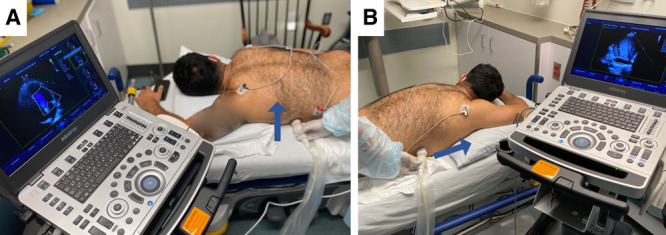
Patient positioning for prone transthoracic echocardiography, with the left shoulder slightly elevated by a pillow support. To obtain the apical four-chamber view, the transducer is placed along the left anterior axillary line at the fourth to fifth intercostal space with the indicator directed posteriorly (A; blue arrow). To obtain a lateral inferior vena cava view, the transducer is placed between the right anterior and midaxillary lines at the fifth to sixth intercostal space with the indicator directed toward the patient’s head (B; blue arrow).
Obtaining the Apical Window
Exams began with the apical window. The ultrasound transducer was placed vertically on the left flank with the indicator directed posteriorly, as shown in Figure 1A. The window was obtained in the traditional apical position, at the point of maximal pulsation near the midclavicular line in the fourth or fifth intercostal space. Once the apical four-chamber view was achieved, an apical five-chamber was obtained by tilting the probe anteriorly. Views were considered adequate if all four chambers (apical four-chamber) and also addition of the left ventricular (LV) outflow tract (apical five-chamber) could be visualized.
Obtaining the Lateral Inferior Vena Cava Window
Next, a view of the inferior vena cava (IVC) was obtained by repositioning the transducer at the right flank. The transducer was placed horizontally with the indicator directed toward the patient’s head, as shown in Figure 1B. Once the IVC was found, a subcostal short-axis view or four-chamber view was obtained by tilting the probe toward the left shoulder and rotating the probe clockwise. The lateral IVC view was considered adequate if the IVC and right atrium could be visualized.
Assessing Cardiac Function
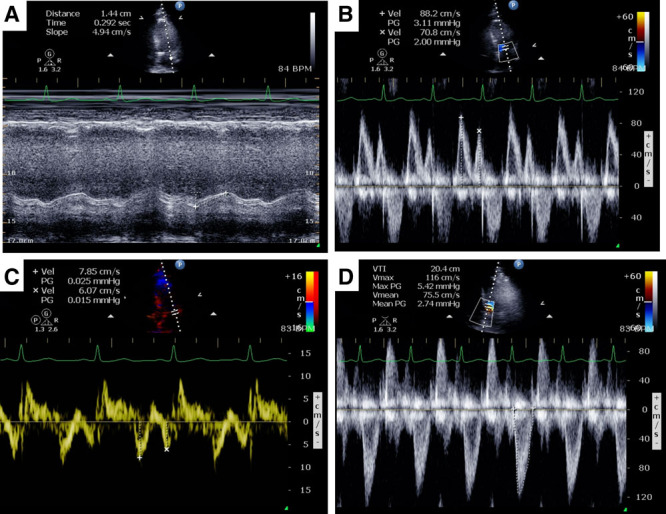
Quantitative assessments of cardiac function were performed according to the most recent recommendations from the American Society of Echocardiography (4, 5). Representative images of right ventricular (RV) assessment obtained on our patients are shown in Figure 2. From the apical four-chamber view, RV function was assessed by chamber size (Fig. 2A), tricuspid annular plane systolic excursion (TAPSE) in M-mode (Fig. 2B), and RV peak systolic tricuspid annulus velocity (RV S′) using tissue Doppler imaging (Fig. 2C). Pulmonary pressures were assessed by tricuspid regurgitation peak gradient (TR PG) using color (Fig. 2D) and continuous-wave Doppler (Fig. 2E). We also performed agitated saline bubble studies when requested by the clinical team to determine the presence of intracardiac shunting. From the lateral subcostal window, we estimated right atrial pressure by the size and collapsibility/distensibility of the IVC (Fig. 2F).
Figure 2.

Assessments of right ventricular (RV) function performed on a patient in the prone position including apical four-chamber view (A; Supplemental Video 1, Supplemental Digital Content 1, http://links.lww.com/CCX/A256; legend, Supplemental Digital Content 6, http://links.lww.com/CCX/A261) for comparison of chamber sizes (A), tricuspid annular plane systolic excursion (B), RV peak systolic tricuspid annulus velocity (C), color Doppler across the tricuspid valve showing a regurgitant jet (D; Supplemental Video 2, Supplemental Digital Content 2, http://links.lww.com/CCX/A257; legend, Supplemental Digital Content 6, http://links.lww.com/CCX/A261), continuous-wave Doppler of the same regurgitant jet to obtain the tricuspid regurgitant peak gradient (E), and lateral inferior vena cava (IVC) view for measurement of IVC diameter and distensibility/collapsibility index (F). BPM = beats per minute, PG = peak gradient, Vel = velocity.
Acknowledging that LV dysfunction may also contribute to elevated pulmonary pressures, we assessed variables of LV systolic and diastolic function. Representative images of LV assessment obtained on our patients are shown in Figure 3. From the apical four-chamber view, we assessed chamber size, mitral annular plane systolic excursion (MAPSE) (Fig. 3A), mitral inflow signal (E and A) by pulsed-wave Doppler (Fig. 3B), and motion of the mitral annulus (e′ and a′) using tissue Doppler imaging (Fig. 3C). From the apical five-chamber view, we measured the velocity time integral (VTI) of the LV outflow tract and its variation with positive pressure ventilation (Fig. 3D).
Figure 3.
Assessments of left ventricular (LV) function performed on a patient in the prone position including mitral annular plane systolic excursion (A), pulsed-wave Doppler of the mitral inflow (E and A waves) (B), pulsed-wave tissue Doppler of the mitral annular velocities (e′ and a′) (C), and pulsed-wave Doppler of the LV outflow tract velocity time integral (D). BPM = beats per minute, max PG = maximum peak gradient, mean PG = mean peak gradient, PG = peak gradient, Vel = velocity, Vmax = maximum velocity, Vmean = mean velocity, VTI = velocity time integral.
RESULTS
A total of 27 mechanically ventilated patients with COVID-19 ARDS were examined by TTE while in the prone position (Table 1). Patients were 37% female and 63% male, with a mean age of 55 ± 11 years, body mass index (BMI) 31 ± 5.1 kg/m2, and were on 13 ± 3.1 cm H2O of positive end-expiratory pressure (PEEP) at the time of examination (range, 4–19 cm H2O).
TABLE 1.
Characteristics of Patients Examined in the Prone Position

Adequate apical four-chamber views were obtained in all patients, and adequate five-chamber views were obtained in 26 out of 27 patients (96.3%). Adequate lateral IVC windows were obtained in 25 out of 27 patients (92.6%). In the first two patients studied, the lateral IVC window was not attempted as this was not part of our initial protocol for TTE examination.
Adequate quantitative assessment of RV function, which included TAPSE, RV S′, and TR PG, was performed in 24 out of 27 patients (88.9%). Adequate quantitative assessment of LV function, which included mitral inflow velocities, mitral annulus peak velocities, MAPSE, and LV outflow tract VTI, was performed in 26 out of 27 patients (96.3%).
At the request of the clinical team, we performed an agitated saline bubble study in one patient to determine the presence of intracardiac shunting that may be exacerbated by high levels of PEEP (Fig. 4).
Figure 4.
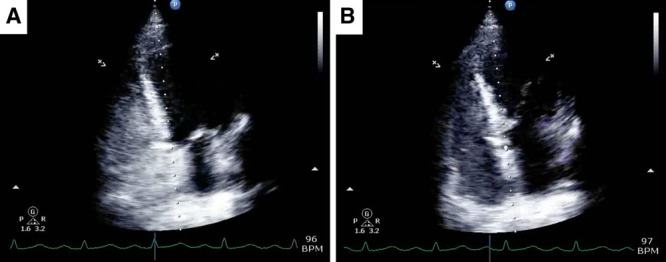
Agitated saline bubble echocardiography study performed on a patient in the prone position (Supplemental Video 3, Supplemental Digital Content 3, http://links.lww.com/CCX/A258; legend, Supplemental Digital Content 6, http://links.lww.com/CCX/A261). Injection of agitated saline caused opacification of the right ventricular (A) without the appearance of bubbles in the left heart (B), indicating absence of intracardiac shunting. BPM = beats per minute.
DISCUSSION
TTE Can Be Reliably Performed on Obese Patients in the Prone Position on High PEEP
Obesity and high levels of PEEP (≥ 15 cm H2O) have been shown to have a high failure rate in critically ill patients, and transesophageal echocardiography (TEE) has been suggested as the modality of choice (6, 7). In this study, we were unable to obtain an adequate TR PG on three patients, all of whom were on greater than or equal to 10 cm H2O PEEP. However, we found that prone positioning permitted focused TTE examination to assess RV and LV function in the vast majority (> 85%) of ARDS patients including many who were obese and on high levels of PEEP. We were also able to detect valvular abnormalities in three prone patients that had not been previously documented.
Prone Positioning May Enhance Image Quality by Anterior Cardiac Displacement
Chino and Marks (8) previously found that the lateral and superior aspects of the heart were displaced anteriorly by 2 cm in the prone position, and the volume of interposed lung between the heart and chest wall when lying prone is markedly reduced (3 vs 25 mL). This could translate to less acoustic barrier and superior image quality in the prone versus supine position. Particularly in ARDS, high levels of PEEP and diffuse B lines from interstitial edema in overlying lung fields can further obscure echocardiographic images. Interestingly, we noted improved image quality in the prone position for multiple examined patients including many who were obese and on high levels of PEEP. Apical views obtained from the same patient taken in the supine (Fig. 5A) and prone (Fig. 5B) positions are shown, demonstrating a case in which better delineation of the cardiac chambers was obtained in the prone position. Although we found that the “swimmer position” (3) allowed for the best visualization of cardiac chambers in the prone position, others (9) have recently described image acquisition in prone patients without the need to adopt this position.
Figure 5.
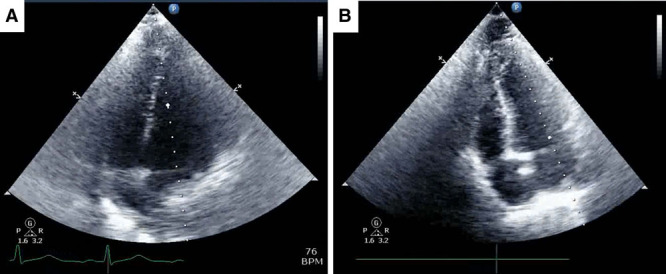
Comparison of apical four-chamber views obtained on the same patient while positioned supine (A; Supplemental Video 4, Supplemental Digital Content 4, http://links.lww.com/CCX/A259; legend, Supplemental Digital Content 6, http://links.lww.com/CCX/A261) and prone (B; Supplemental Video 5, Supplemental Digital Content 5, http://links.lww.com/CCX/A260; legend, Supplemental Digital Content 6, http://links.lww.com/CCX/A261). Images were acquired within a 24-hr period. BPM = beats per minute.
TTE Is the Optimal Imaging Modality in Prone ARDS Patients
Experts have historically considered TEE to be preferred over TTE for assessing prone patients due to superior image quality (10, 11). Although TEE may provide higher image quality, the images we obtained by TTE were adequate for focused assessment of RV and LV function. TTE is less labor intensive, poses far fewer risks to the patient, and can be readily performed by critical care physicians at the bedside of prone ARDS patients. Furthermore, TEE presents a rare but potentially catastrophic risk of esophageal perforation (12–14). TEE probe insertion and manipulation can be cumbersome and technically challenging in the prone position, further increasing risk for mechanical complications (15). Given that many patients with ARDS will have underlying respiratory infections, instrumentation of the oral cavity for TEE also carries the risk of aerosolization of infectious particles, thus presenting a hazard to staff particularly in COVID-19 era. We believe that TTE has the potential to offer the greatest benefits relative to risk in terms of monitoring disease progression and response to therapies in patients with ARDS.
The ability to monitor cardiac function and optimize ventilatory and hemodynamic variables to best support the RV may improve outcomes in ARDS (16). Pulmonary artery catheterization is considered the gold standard for monitoring pulmonary artery pressures and the transpulmonary gradient and may be indicated for some patients. Although pulmonary artery catheters are able to provide an estimate of RV afterload, they do not allow for direct assessment of RV function (17). TTE is an alternative tool that is noninvasive, poses very little risk to the patient, and can provide direct information regarding RV and LV function to make clinical decisions (18). For example, failure to wean from mechanical ventilation may be cardiac rather than respiratory in etiology, and LV diastolic dysfunction and volume status can be readily assessed and optimized by echocardiography to facilitate weaning from mechanical ventilation (2). Table 2 describes several indications for performing TTE in the management of critically ill patients with ARDS.
TABLE 2.
Indications for Performing Transthoracic Echocardiography in the Management of Critically Ill Patients With Acute Respiratory Distress Syndrome

Limitations
Our study has several limitations. Ultrasound studies performed consecutively in the supine and prone positions, without alterations in other clinical variables, would have provided the most direct comparison of image quality but would have disrupted patient care. Efforts were made to examine patients in both positions within close temporal proximity whenever possible; however, some exams were performed up to 48 hours apart and following changes in ventilation variables and hemodynamics. The highest BMI encountered in our study was 41, and whether patients at more extreme upper limits of BMI (> 50) may be more challenging to image in the prone position warrants further investigation. Another limitation of performing TTE in the prone position is the inability to obtain parasternal long- and short-axis views to compute E-point septal separation and fractional shortening as additional variables to assess LV function. Despite these limitations, our findings suggest that TTE in the prone position is feasible in many patients and its use should be recognized as means to enhance clinical care.
CONCLUSIONS
We have demonstrated that focused TTE examinations can be performed in the prone patient with ARDS, including in morbidly obese patients and patients on high levels of PEEP that was previously thought to be technically challenging. We hope that our findings will encourage the use of TTE to facilitate the diagnostic workup and optimization of prone patients with ARDS.
ACKNOWLEDGMENT
The authors would like to thank Mindray for equipment support.
Supplementary Material
Footnotes
This study was performed as part of an ongoing clinical trial funded by the U.S. National Institutes of Health (NCT04306393).
Drs. Gibson and Chang performed data collection and analysis; both had access to all data and assumed responsibility for the submitted work. All authors wrote and reviewed the article.
The authors have disclosed that they do not have any potential conflicts of interest.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s website (http://journals.lww.com/ccejournal).
REFERENCES
- 1.Guérin C, Reignier J, Richard JC, et al. ; PROSEVA Study Group. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013; 368:2159–2168 [DOI] [PubMed] [Google Scholar]
- 2.Sanfilippo F, Scolletta S, Morelli A, et al. Practical approach to diastolic dysfunction in light of the new guidelines and clinical applications in the operating room and in the intensive care. Ann Intensive Care. 2018; 8:100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ugalde D, Medel JN, Romero C, et al. Transthoracic cardiac ultrasound in prone position: A technique variation description. Intensive Care Med. 2018; 44:986–987 [DOI] [PubMed] [Google Scholar]
- 4.Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010; 23:685–713; quiz 786–788 [DOI] [PubMed] [Google Scholar]
- 5.Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1–39.e14 [DOI] [PubMed] [Google Scholar]
- 6.Cook CH, Praba AC, Beery PR, et al. Transthoracic echocardiography is not cost-effective in critically ill surgical patients. J Trauma. 2002; 52:280–284 [DOI] [PubMed] [Google Scholar]
- 7.Mekontso Dessap A, Proost O, Boissier F, et al. Transesophageal echocardiography in prone position during severe acute respiratory distress syndrome. Intensive Care Med. 2011; 37:430–434 [DOI] [PubMed] [Google Scholar]
- 8.Chino JP, Marks LB. Prone positioning causes the heart to be displaced anteriorly within the thorax: Implications for breast cancer treatment. Int J Radiat Oncol Biol Phys. 2008; 70:916–920 [DOI] [PubMed] [Google Scholar]
- 9.Giustiniano E, Padua E, Negri K, et al. Echocardiography during prone-position mechanical ventilation in patients with COVID-19: A proposal for a new approach. J Am Soc Echocardiogr. 2020; 33:905–906 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yin WH, Wang XT, Liu DW, et al. ; Chinese Critical Ultrasound Study Group; Critical Hemodynamic Therapy Collaboration Group. [A Chinese consensus statement on the clinical application of transesophageal echocardiography for critical care (2019)]. Zhonghua Nei Ke Za Zhi. 2019; 58:869–882 [DOI] [PubMed] [Google Scholar]
- 11.Evrard B, Goudelin M, Vignon P. Transesophageal echocardiography remains essential and safe during prone ventilation for hemodynamic monitoring of patients with COVID-19. J Am Soc Echocardiogr. 2020 [Google Scholar]
- 12.Ahmed K, Lal Y, Condron S. Esophageal perforation: A rare complication of transesophageal echocardiography in a patient with asymptomatic esophagitis. Case Rep Gastroenterol. 2012; 6:760–764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim HC, Oh JH, Lee YC. Esophageal perforation after perioperative transesophageal echocardiography: A case report. J Med Case Rep. 2016; 10:338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kimura A, Mori T, Kihara Y, et al. A case of esophageal perforation after intraoperative transesophageal echocardiography in a patient with a giant left atrium: Unexpectedly large distortion of the esophagus revealed on retrospectively constructed three-dimensional imaging. JA Clin Rep. 2019; 5:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chui J, Craen RA. An update on the prone position: Continuing professional development. Can J Anaesth. 2016; 63:737–767 [DOI] [PubMed] [Google Scholar]
- 16.Lazzeri C, Cianchi G, Bonizzoli M, et al. The potential role and limitations of echocardiography in acute respiratory distress syndrome. Ther Adv Respir Dis. 2016; 10:136–148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gidwani UK, Mohanty B, Chatterjee K. The pulmonary artery catheter: A critical reappraisal. Cardiol Clin. 2013; 31:545–565, viii [DOI] [PubMed] [Google Scholar]
- 18.Caille V, Charron C, Vieillard-Baron A. Right ventricular function in ARDS patients. Clin Pulm Med. 2010; 17:82–87 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.