

Abstract
Proportional modes of ventilation assist the patient by adapting to his/her effort, which contrasts with all other modes. The two proportional modes are referred to as neurally adjusted ventilatory assist (NAVA) and proportional assist ventilation with load-adjustable gain factors (PAV+): they deliver inspiratory assist in proportion to the patient’s effort, and hence directly respond to changes in ventilatory needs. Due to their working principles, NAVA and PAV+ have the ability to provide self-adjusted lung and diaphragm-protective ventilation. As these proportional modes differ from ‘classical’ modes such as pressure support ventilation (PSV), setting the inspiratory assist level is often puzzling for clinicians at the bedside as it is not based on usual parameters such as tidal volumes and PaCO2 targets. This paper provides an in-depth overview of the working principles of NAVA and PAV+ and the physiological differences with PSV. Understanding these differences is fundamental for applying any assisted mode at the bedside. We review different methods for setting inspiratory assist during NAVA and PAV+ , and (future) indices for monitoring of patient effort. Last, differences with automated modes are mentioned.
Keywords: Mechanical ventilation, Proportional modes, Inspiratory assist, Respiratory effort
Take-home message
| This review explains how proportional ventilation modes improve the match between the patient and the ventilator and provide the potential for both lung and diaphragm-protective ventilation. We discuss different methods to titrate inspiratory assist levels, which is a key challenge at the bedside, as optimal targets of respiratory muscle effort may vary among patients and over the course of critical illness. |
Introduction
Proportional modes of ventilation work by amplifying the effort of the patient’s respiratory muscle activity, providing the necessary support to improve the imbalance between capacity and demand and to reach the patient’s ventilation goal at the same time. Proportional modes have the potential to provide lung and respiratory muscle-protective ventilation by maintaining the patient’s control mechanisms against both lung overdistention and ventilator over-assistance, and avoiding the development of diaphragm disuse atrophy [1, 2]. Inspiratory assist is delivered in synchrony with patient effort during the total inspiratory cycle, and thus, by contrast with other modes, directly responds to changes in ventilatory demands [3, 4]. This is fundamentally different from conventional partially supported modes of ventilation such as pressure support ventilation (PSV), where the same pressure is delivered by the ventilator for every breath and is independent of the metabolic needs and the magnitude of the patient’s effort and also, most often, of its timing. Hence, patient-ventilator asynchrony and ventilator over-assistance are common and often unnoticed in conventional modes such as PSV [5–9].
Modes of proportional ventilation readily available in clinical practice on dedicated ventilators are neurally adjusted ventilatory assist (NAVA) [3], and proportional assist ventilation with load-adjustable gain factors (PAV+) [2]. Their physiological effects are very similar, but they differ in the signal used to control the ventilator. NAVA delivers inspiratory assist in proportion to the diaphragm electrical activity (EAdi), which closely reflects central respiratory drive and is measured via a dedicated nasogastric (feeding) tube with embedded electrodes [3]. PAV+ delivers assist in proportion to the instantaneous flow and volume generated by the patient’s inspiratory effort or muscular pressure (Pmus), which is estimated from semi-continuous automatic measurements of respiratory mechanics applying the equation of motion of the respiratory system [10, 11]. As patients tailor the amount of assist themselves, proportional modes simplify the implementation of assisted mechanical ventilation [12]. An important barrier to wide implementation of those modes, however, is the unfamiliarity with the settings and functioning, which differ from conventional modes. Real-time monitoring of respiratory drive (EAdi time course during NAVA) and patient effort (semi-continuous estimation of Pmus in PAV+) is also available in proportional modes and allows quantification of the physiological response to changes in ventilatory assist. Although proportional modes have been increasingly used, setting inspiratory assist levels remains a challenge at the bedside as it cannot be based on usual parameters such as tidal volumes and PaCO2 targets [13, 14]. Moreover, safe targets for respiratory effort may vary among patients, depending on the severity of lung injury and diaphragm function [15–17]. The uncertainty regarding titration of inspiratory support with NAVA and PAV+ might be one of the reasons why there is still limited data showing improved clinical outcomes when using proportional modes as compared to conventional modes [18, 19], but clinical benefits of NAVA compared to PSV were recently demonstrated in difficult-to-wean patients [20, 21]. At the same time, despite having very complex physiological consequences, PSV maintains an appearance of simplicity and is the most frequently used partially supported mode of ventilation [22].
This review provides a physiological understanding of proportional modes during invasive mechanical ventilation in the adult intensive care unit (ICU) population and their differences with PSV, which is fundamental to understand when applying any assisted mode at the bedside. We discuss methods for titrating inspiratory assist during NAVA and PAV+ , and (future) indices for monitoring of patient effort. Last, we also highlight key differences with automated modes.
Principles of operation
NAVA
Measured with a dedicated nasogastric feeding tube, EAdi reflects the intensity of the electrical field produced by the diaphragm contraction and is the closest available signal to the respiratory centers’ output. EAdi is the most precise surrogate of neural respiratory drive provided that neuromuscular transmission and muscle fibre membrane excitability are intact, and the diaphragm is used as the main inspiratory muscle (i.e., no significant difference across different accessory muscles) [3, 23, 24]. EAdi mainly reflects crural diaphragm activity, but is representative of activity from the costal parts of the diaphragm. EAdi correlates well to transdiaphragmatic pressure [25, 26] and the signal remains reliable at different lung volumes [27]. Ventilator algorithms continuously correct for interference from cardiac activity and motion artefacts due to cardiac contractions and esophageal peristalsis.
NAVA is unique compared to all other ventilator modes, as it uses EAdi to control the ventilator, especially triggering, level of inspiratory assist and cycle-off. Inspiratory pressure (Paw) applied above positive end-expiratory pressure (PEEP) during NAVA is determined by the proportionality gain (NAVA level, in cmH2O/µV) set by the clinician:
| 1 |
Thus, when EAdi amplitude is 10 µV and the NAVA level 1.5 cmH2O/µV, peak Paw reaches 15 cmH2O above PEEP. Inspiratory assist is proportional to EAdi over the inspiratory cycle; it is triggered for every EAdi increase > 0.5 µV above baseline and is terminated when EAdi amplitude falls at 70% of its peak value, which probably approximates reasonably the end of the active contraction. The EAdi signal is pneumatically independent and thus triggering is not directly affected by the presence of leaks or intrinsic PEEP; assisted breaths can be triggered either by EAdi, Paw or flow, according to a hierarchy that follows the “first-come first-served” principle [3]. EAdi allows real-time monitoring of diaphragm activity, which is not limited to the use in NAVA mode and even possible in a non-intubated patient. When using EAdi for monitoring purposes, it is important to realize that an increase in EAdi can have many causes such as an increased mechanical load imposed on the respiratory muscles (e.g., increase in resistance), an increased ventilatory demand (e.g., increase in CO2 production), or an increase in drive unrelated to the load (e.g., inflammation) [28–30]. Because tidal volume is controlled primarily by the brain stem respiratory centres, changing the level of assist may not affect tidal volume.
PAV+
In PAV+ , the trigger functions similarly to other assisted modes of ventilation; the ventilator detects inspiratory effort by instantaneous measures of flow and volume that is pulled in by the patient and delivers pressure assist accordingly [10, 11]. The inspiratory assist is instantaneously calculated from the measured flow and volume using the equation of motion of the respiratory system and an adjustable gain that determines the percentage of the total pressure calculated to be delivered [2, 4]. The total pressure delivered to the respiratory system (Ptotal) is then the sum of Paw and Pmus and it overcomes both resistive and elastic recoil pressure:
| 2 |
The ventilator automatically calculates respiratory system resistance [10] and elastance [11] by performing short end-inspiratory occlusions every 8–15 breaths (of note: this is specific to PAV+ and does not exist in simple ‘PAV’ or in ‘proportional pressure support’) and uses the gain as %assist:
| 3 |
Using Eq. 2, this relationship can be further written as
| 4 |
Paw is thus a fraction of Ptotal and proportional to the instantaneous Pmus during the full inspiratory cycle (Fig. 1); the gain indicates a percentage of respiratory muscle unloading, set by the clinician. Hence, if the gain is set at 75%, it means that the ventilator delivers 75% of the total pressure, the remaining 25% being assumed by the patient’s Pmus (Eq. 3): Paw equals three times Pmus along the inspiratory phase (Eq. 4). Practically, this gain can be between 5% and 85%. Indeed, assist levels close to 100% would put the patient at risk of over-assistance in case of errors in the automated calculations of respiratory mechanics resulting in overestimation of the pressure needed. Similar to NAVA, because the patient’s brain controls the desired volume, the volume delivered to the patient may show little variations when varying the level of assist [31]. Inspiration is cycled-off when flow decreases to a low pre-set level (by default set to 3 L/min). This cycling-off mechanism usually makes the end of ventilator assistance extremely close to the end of the neural inspiration. PAV+ cannot be used during non-invasive ventilation, as end-inspiratory occlusions cannot be performed in the presence of leaks. In addition, estimations of Ptotal do not correct for intrinsic PEEP, if present, which may lead to an underestimation of the delivered pressure in patients with significant hyperinflation [32].
Fig. 1.

Example of the working principle of proportional assist ventilation with load-adjustable gain factors (PAV+). Short inspiratory occlusions are automatically performed (indicated by * in the flow signal) for the calculation of respiratory system resistance and compliance. Arrows indicate that airway pressure (Paw) is delivered proportional to the patient’s effort (esophageal pressure (Pes))
Differences between proportional modes and PSV
Patient-ventilator interactions: Pmus-VT relationship and cycling-off criterion
The main physiological differences between PSV and proportional modes can be explained with the relationship between patient’s effort or Pmus and tidal volume (VT) delivered by the ventilator (Fig. 2a). During unassisted breathing, increases in Pmus result in a relatively linear increase in tidal volume (i.e., assuming a linear relationship between Pmus and PaCO2) [33, 34]. The slope of this relationship represents the efficiency of the respiratory muscles. With PSV, the Pmus-VT curve is shifted upwards and, therefore, does not start from zero volume (Fig. 2a); this is because a substantial tidal volume is still delivered despite minimal respiratory drive and no measurable effort (e.g., due to sedation or over-assistance); this volume depends mostly on the pressure support level and the respiratory system compliance [35, 36]. The presence of this ‘minimum tidal volume’ erroneously suggests to clinicians that the patient is spontaneously breathing, while the patient only triggers the ventilator and relaxes his inspiratory muscles thereafter, implying ventilator over-assistance (Fig. 3) [35]. Ventilator over-assistance results in excessive tidal volumes, very low diaphragm activity and possibly risk of disuse atrophy [5, 37]. Excessive inspiratory assist decreases patient effort to virtually zero [38] and leads to central apnea events during sleep as soon as the PaCO2 apneic threshold is reached. Apneas result in arousals and awakenings, making deep (restful) sleep difficult [39]. The initial slope of the Pmus-VT relationship is unaffected in PSV, as a constant pressure is applied regardless of patient effort. As such, patients with a high respiratory drive can also be under-assisted, with a risk of diaphragm load-induced injury and patient self-inflicted lung injury [15, 16]. Additionally, perfect patient-ventilator synchrony is frequently not achieved in PSV [19, 40, 41]. The risk of late cycling (i.e., mechanical insufflation finishing after the end of inspiratory effort; also known as prolonged insufflation or prolonged cycling) is high during PSV, as insufflation cycles-off to exhalation once the flow has reached a set percentage of the peak inspiratory flow: the higher the assist, the longer the time to reach the cycling-off criterion and the longer the mechanical inspiratory time, thereby increasing the mismatch with the patient’s neural inspiratory time [42, 43] (Fig. 2b). Since excessive ventilator assist promotes dynamic hyperinflation and decreases patient effort, this places the patient at risk of ineffective efforts [6, 8] (Fig. 2b). In addition, autotriggering resulting in delivery of a full breath may happen during PSV but not under proportional modes. Electrical artefacts in the EAdi signal can trigger some pressure delivery during NAVA; however, this will always be very low (proportional to the artefact) [44].
Fig. 2.

a Schematic illustration of the relationship between patient effort (respiratory muscle pressure, Pmus) and tidal volume (VT) in unassisted spontaneous breathing (dashed line), during pressure support ventilation (PSV) and for proportional modes such as proportional assist ventilation with load-adjustable gain factors (PAV+) and neurally adjusted ventilatory assist (NAVA). b Patient-ventilator interaction during PSV. Increasing the pressure support level increases VT (blue line) and ventilator inspiratory time (Ti, green line), while patient effort (Pmus, grey dotted line) is downregulated. In addition, neural Ti (dark blue line) remains unaltered with increasing levels of assist which results in late cycling. c Patient-ventilator interaction during NAVA and PAV+. Ventilator assist is delivered proportional to the patient’s demand over the full inspiratory cycle (neural Ti = ventilator Ti, note that the dashed green and dark blue lines overlap). Increasing the inspiratory assist level (NAVA level or PAV+ gain) downregulates Pmus (grey dotted line). Because the patient’s brain controls mainly the desired VT, changing the level of assist often has only minimal effects on the VT, as shown by the horizontal blue line on the Volume vs. level of assist curve
Fig. 3.

Representative example of over-assistance during pressure support ventilation (PSV). The patient was ventilated with an inspiratory pressure set at 10 cmH2O above a positive end-expiratory pressure of 8 cmH2O. A double-balloon nasogastric catheter was placed for measurements of esophageal pressure (Pes) and gastric pressure. Transdiaphragmatic pressure (Pdi) was calculated as gastric pressure minus Pes. As can be seen in the Pes waveform, the patient only triggers the ventilator (small drop in Pes) and relaxes inspiratory muscles thereafter, as demonstrated by the increase in Pes during the remaining of the inspiratory cycle and the absence of increases in Pdi
In contrast, during NAVA and PAV+, the proportionality gain set by the clinician determines the slope of the Pmus-VT curve [2, 35] (Fig. 2a), meaning that more assist is delivered with increased patient’s ventilatory demands. As the curve starts at zero (i.e., no upward shift as in PSV) some activity of the respiratory muscles is required to maintain adequate ventilation and ventilator assist is terminated as soon as patient effort diminishes (Fig. 2a, c). Therefore, proportional modes provide patient-ventilator synchrony over the full inspiratory cycle, preventing ventilator over-assistance, diaphragm disuse and avoiding apnea events during sleep. These principles explain why NAVA and PAV+ are more physiological as compared to PSV [41].
Respiratory muscle unloading and neuromuscular coupling
In patients recovering from acute respiratory failure, muscle unloading was comparable between PSV levels within the range of 7 to 25 cmH2O and NAVA levels ranging from 0.5 to 2.5 cmH2O/μV [38]. NAVA, however, improved patient-ventilator interactions, preserving breathing variability and allowing better synchronization. Interestingly, NAVA led to a larger contribution of the diaphragm to inspiratory efforts [45], which could potentially improve gas exchange due to enhanced ventilation in basal lung regions [46]. Another study confirmed improved diaphragm function with NAVA compared to PSV after prolonged controlled mechanical ventilation [47], while differences between PSV and PAV+ were not as pronounced [48]. However, in response to increases in elastic loading, a greater respiratory muscle efficiency was found with PAV+ compared to PSV [49, 50].
Proportional modes for lung and diaphragm-protective ventilation
Proportional modes improve patient-ventilator synchrony, neuromuscular coupling and gas exchange, and restore breathing variability [19, 41, 50–53]. This improved patient-ventilator interaction is a potential mechanism by which NAVA and PAV+ might provide lung and diaphragm-protective ventilation. Lung overdistention is prevented due to two known physiological mechanisms. First, the Hering–Breuer inflation–inhibition biological feedback mechanism downregulates respiratory drive (and thus EAdi amplitude and patient effort) at higher tidal volumes to avoid hyperinflation [27, 54, 55]. Second, with increasing lung volumes the diaphragm shortens and may become a less effective pressure generator, thereby decreasing effort [27, 56]. Indeed, Carteaux et al. [38] showed that most patients could self-regulate their tidal volumes in a protective range (between 6 and 8 mL/kg PBW) despite increasing NAVA levels within a certain ‘reasonable’ range. Furthermore, it was recently shown that patients ventilated in PAV+ after acute respiratory distress syndrome were able to avoid lung overdistention, as indicated by a driving pressure kept below 15 cmH2O [57]. Increasing support levels during PSV, by contrast, increases tidal volumes despite a downregulation of neural drive [45]. Proportional modes may, therefore, protect the patient from harmful tidal volumes and simultaneously prevent diaphragm disuse atrophy. It should be stressed, however, that excessive respiratory drive may overwhelm lung-protective reflexes, and hence, additional caution is required when using proportional modes in patients with high respiratory drive and extremely impaired respiratory mechanics.
Clinical comparisons of proportional modes and PSV
The use of proportional modes, especially PAV+, has been associated with a shorter weaning duration compared to PSV [19] in small studies and increased probability of remaining with assisted spontaneous ventilation [58]. It was reasoned that this was because of better patient-ventilator interaction, reduced sedation requirements [12, 59] and improvement in sleep quality [60–62]. Because of these reasons, increased patient comfort during proportional modes is often assumed to be present but has rarely been measured [53, 63, 64]. Although reduced asynchronies during sleep were reported, the direct effects of proportional modes on sleep quality were small, improving sleep in two studies [60, 61] but not in all [62].
Differences in weaning duration or ICU outcome were not demonstrated in a large randomized study (n = 128) that compared NAVA with PSV in patients recovering from acute respiratory failure [18]. It is important to note, however, that EAdi monitoring was also available in the PSV group. In that study, NAVA reduced patient-ventilator asynchrony and the rate of post-extubation application of non-invasive ventilation, and feasibility and safety of NAVA over several days was successfully demonstrated. A recent study confirmed acceptable adherence to the assigned mode beyond 48 h when comparing NAVA with PSV [21]. Furthermore, Liu et al. recently showed shorter weaning duration with NAVA compared to PSV in selected difficult-to-wean patients [20].
Setting inspiratory assist during NAVA
Different methods for NAVA titration starting from PSV or based on a thorough physiological assessment in NAVA mode exist and are summarized in Table 1. Before starting any titration, adequate EAdi catheter placement according to published recommendations [65] and the manufacturer’s positioning tool (using a calculated distance and ECG artefacts in the signal) and EAdi signal quality should be confirmed. If EAdi is abnormally low or absent despite correct catheter placement, ventilator over-assistance, excessive sedation, central apneas, severe diaphragm weakness or pre-existing neuromuscular diseases should be considered as possible reasons for low EAdi. Direct phrenic nerve lesions could hamper NAVA application if no inspiratory EAdi can be measured, but this is quite rare.
Table 1.
Methods of inspiratory assist titration in NAVA and PAV+ and their pros and cons
| Method | Pros | Cons |
|---|---|---|
| NAVA preview | ||
| Pawpeak matching |
Intuitive and straightforward Implemented in the ventilator Helpful for detecting asynchronies in PSV mode |
Pawpeak matching does not guarantee similar assist levels due to differences in Paw profile Depends on quality of initial PSV titration Breath-by-breath variability in EAdi amplitude may make matching difficult Does not consider variation in EAdi caused by the change from PSV to NAVA |
| Pawmean matching |
Same pros as above Results in more similar assist levels between PSV and NAVA |
Depends on quality of initial PSV titration Breath-by-breath variability in EAdi amplitude may make matching difficult Does not consider potential variation in EAdi caused by the change from PSV to NAVA |
| Ventilation matching | Simple |
Depends on quality of initial PSV titration One cannot control ventilation with NAVA Does not incorporate the EAdi signal |
| NAVA titration based on patient’s response | ||
| Two-phased response of Paw and VT |
Physiologically sound Reflects changes in respiratory muscle output Shown to result in a more personalized level compared to using NAVA preview |
May be difficult to perform at the bedside, especially when considering the curvilinear relationship between EAdi and respiratory muscle effort depending on the level of assist Achieving a two-phased response in patients with very high respiratory drive and/or an overwhelmed Hering–Breuer reflex can be difficult |
| 60% of EAdimaxSBT |
Physiologically sound Provides daily re-assessment of the NAVA level and EAdi. Can theoretically be applied during any assisted ventilation mode |
Limited to the use during after a failed PS 7/PEEP 0 cmH2O SBT EAdimaxSBT may be different according to the SBT method (i.e., T-piece or CPAP trial) Does not take into account accessory respiratory muscles that are often recruited during SBT failure 60% target is arbitrarily chosen; this may result in high inspiratory efforts in patients with high respiratory drive |
| Unloading based on NVE |
Physiologically sound Easy to perform at the bedside Recommended to use 40% unloading target |
Limited to the weaning phase NVE reflects ventilatory efficiency and not directly breathing effort A zero-assist breath is not fully unassisted, as the ventilator always provides a minimum level of inspiratory pressure (2-3 cmH2O) that slightly overestimates NVE |
| PAV+ titration | ||
| Pawmean matching | Simple and intuitive |
Depends on quality of initial PSV titration Paw matching does not guarantee similar assist levels due to differences in Paw profile |
| Inspiratory effort (Pmus, PTPmus) |
Physiologically sound Grid incorporated in the ventilator |
Target values may be difficult to achieve in patients with excessive respiratory drive |
EAdi diaphragm electrical activity, EAdimaxSBT maximum EAdi amplitude during a spontaneous breathing trial (SBT), CPAP continuous positive airway pressure, NAVA neurally adjusted ventilatory assist, NVE neuroventilatory efficiency index, Paw airway pressure, PEEP positive end-expiratory pressure, Pmus muscular pressure, PTP pressure–time product, PS pressure support, PSV pressure support ventilation, VT tidal volume
NAVA “preview”
A grey curve (Fig. 4) displayed on the monitor during PSV shows a “preview” of the estimated Paw that would exist if the patient was ventilated in NAVA mode with current proportionality setting. The shape of the Paw curve resembles the EAdi profile (i.e., proportionality), while the amount of assist depends on the EAdi amplitude and the selected NAVA level.
Fig. 4.
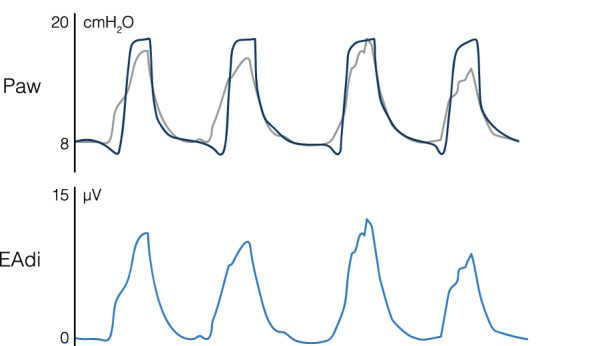
Example of the neurally adjusted ventilatory assist (NAVA) preview during pressure support ventilation (inspiratory assist of 10 cmH2O above a positive end-expiratory pressure of 8 cmH2O). The grey curve shows a “preview” of the estimated airway pressure (Paw) that would exist if the patient was ventilated in NAVA mode. The shape of this Paw curve resembles the diaphragm electrical activity (EAdi) curve (i.e., proportionality). The amount of assist depends on the EAdi amplitude and the selected NAVA level (0.8 cmH2O/µV for this example)
Airway pressure targets
The most frequently used method is setting the NAVA level such that inspiratory assist reaches the same peak Paw (Pawpeak) that is obtained in PSV. However, when applying this method, differences in the shape of the Paw curve explain why the pressure delivered (i.e., area under the Paw curve) is generally lower with NAVA than PSV. It is suggested to target NAVA levels to obtain similar mean Paw (Pawmean) values [45]. The main uncertainty regarding the relevance of this method is whether support was adequate (no over-assist or under-assist) in PSV.
Ventilation targets
Coisel et al. [66] set the NAVA level to obtain the same minute ventilation as determined by a prior 5-min application of PSV with tidal volumes of 6–8 mL/kg PBW and a respiratory rate of 20–30 breaths/min. Similar as for Paw targets, this method depends on the quality of the initial PSV titration. In addition, ventilation is not really ‘controlled’ by the settings.
Assessment of physiological response to inspiratory assist
The above methods do not take advantage of the working principle of NAVA as a proportional mode. The following methods for NAVA titration are based on the fact that neural drive and patient effort, and not necessarily tidal volume, vary with the level of inspiratory assist.
Two-phased response of Paw and tidal volumes
Starting from a condition of ventilator under-assist (i.e., minimal ventilator assist of ~ 3 cmH2O), Brander et al. [67] assessed changes in Paw and tidal volumes during a stepwise increase in NAVA level. A two-phased response was observed: the initial increase in NAVA level resulted in a steep increase in both Paw and tidal volumes (first response) and, at some point, further increasing the NAVA level resulted in less Paw increase and no change in tidal volume (second response). The optimal NAVA level was identified at the transition point, describing a change from an initial insufficient assist level to an assist level that meets the patient’s respiratory demand as indicated by a stable tidal volume. In the initial phase, the patient allows Paw and tidal volumes to increase, while in this second phase tidal volume reaches a plateau (EAdi downregulation) since ventilation meets the patient’s demands. The same group confirmed this response in resistively loaded rabbits [54]. Another study compared this method to an initial NAVA level set using the preview tool with matching NAVA Pawpeak to the Pawpeak measured during PSV; although not significant, a trend toward overestimation of the NAVA level when using the NAVA preview tool was reported [68]. It is not clear how often this procedure is feasible, since many patients do not demonstrate clearly these two phases [38].
Percentage of the maximum EAdi during a failed SBT
In difficult-to-wean patients, Rozé et al. [69] set the NAVA level to obtain EAdi amplitudes corresponding to ~ 60% of the EAdi peak (level chosen arbitrarily) that was measured during a failed spontaneous breathing trial under PSV (PS 7 cmH2O, no PEEP); this level was referred to as EAdimaxSBT. This procedure was repeated daily, allowing a progressive reduction of the NAVA level until extubation. Setting the NAVA level using EAdimaxSBT, was reasoned to be a non-fatiguing and objective target more relevant than volumetric goals, but additional monitoring may be required in patients with excessive respiratory drive [70].
Neuroventilatory efficiency index (NVE)
In patients who had started weaning, Campoccia et al. [71] titrated NAVA to unloading targets. The ratio of unloading provided by the ventilator can be calculated as the tidal volume provided by the ventilator only, divided by total tidal volume (VTtot, volume resulting from patient effort + ventilator assistance). The tidal volume provided by the ventilator can be estimated by the difference between the assisted tidal volume minus the non-assisted tidal volume generated by the patient. The latter can be obtained during one unassisted breath, where the NAVA level is zeroed. The neuroventilatory efficiency index (NVE) can then be calculated (Fig. 5a). The NVE describes the capacity of the respiratory muscles to convert EAdi to tidal volume (VT/EAdi, in mL/µV). The percentage of unloading provided by the ventilator is calculated as: (1-(NVE × EAdipeak/VTtot)) × 100%. Unloading targets of 40% and 60% were feasible to implement and less unloading was associated with greater diaphragm activity and improved ventilation in the dorsal dependent lung regions [71].
Fig. 5.

a Example of the calculations of the neuroventilatory efficiency index (NVE) and the patient-ventilator breath contribution index (PVBC). An unassisted breath is obtained by reducing the neurally adjusted ventilatory assist level to zero for one breath. NVE is calculated as the ratio of the tidal volume to peak diaphragm electrical activity (EAdi). When dividing this NVE by the ratio of tidal volume and EAdi of the previous assisted breath, a PVBC index is obtained. b Example of the calculation of the neuromechanical efficiency index (NME) during an end-expiratory hold manoeuvre. During the occlusion (zero flow), the ratio of delta airway pressure (Paw) and EAdi represents the NME
Patients with high respiratory drive
For most patients the NAVA level can be kept below 2.5 cmH2O/μV [38]. Setting inspiratory assist in patients with high respiratory drive can, however, be especially challenging. High NAVA levels should be prevented to limit excessive inspiratory assist. Excessive pressures during inspiration could be prevented by appropriate Paw alarm settings, and NAVA will cycle-off at 3 cmH2O below the set maximal Paw. Paradoxically, the combination of high NAVA levels and a pressure limit has been used in several studies to deliver a square pressure like in PSV [72–74]. High support is then delivered at the start of a breath in synchrony with the patient’s demands, while excessive Paw is prevented. Of note, this neurally triggered PSV mode is not yet available for clinical use, and using “alarm settings” to control the ventilator is potentially unsafe and cannot be recommended.
Potential EAdi-derived indices
Patient-ventilator breath contribution index
The inspiratory tidal volume (VT,insp) during NAVA reflects the volume resulting from the patient’s effort plus the proportional ventilator assist. An ‘effort-sharing’ index can be derived by comparing assisted to unassisted breaths. This patient-ventilator breath contribution (PVBC) index is defined as the ratio of VT,insp/ΔEAdi of an unassisted breath (i.e., NVE, as described above) to that of a breath with ventilator assistance (Fig. 5a) [73, 75]:
PVBC values can range between 0 (VT,insp fully provided by the ventilator) and 1 (VT,insp completely generated by the patient) and have been validated against measurements of transpulmonary pressure [73, 75]. Reliability of PVBC improves when comparing unassisted and assisted breaths with similar respiratory drive (i.e., EAdi amplitude and slope) [76]. PVBC interpretation is complex. For instance, high PVBC values can be found in patients with low respiratory drive that are ready to be weaned (patient effort is low but sufficient to perform the majority of the work), but also in patients with excessive respiratory drive (the patient is under-assisted). Interpretation must take into account absolute ventilator assist and patient effort.
Estimates of breathing effort
The neuromechanical efficiency index (NME) quantifies the amount of pressure the respiratory muscles can generate, normalized to EAdi (in cmH2O/μV) [26]. Calculating NME during brief end-expiratory occlusions (NMEoccl) can allow a non-invasive estimate: in the absence of airflow, changes in Paw equals changes in Pmus. NMEoccl can thus simply be calculated at the bedside as Pawoccl/EAdioccl [26, 77] (Fig. 5b). Taking an average of three out of five measurements with lowest variability is recommended [77].
NMEoccl could be used to estimate inspiratory muscle pressure during unoccluded tidal breathing, using the following equation: Pmus = EAdi × NMEoccl/1.5. The correction factor (/1.5) is required, because in the presence of an occlusion, the diaphragm generates more pressure for the same EAdi than with an open airway [26]. NME calculations over a brief airway occlusion of 200 ms at inspiratory onset tightly reflect NMEoccl [78], and estimate inspiratory effort. A change in NME could also indicate recruitment of accessory respiratory muscles, since EAdi is insensitive to recruitment of accessory muscles.
When using PVBC and NME in clinical practice, it is important to confirm adequate EAdi signal quality, as suboptimal signal filtering could affect reliability of these indices [44, 76, 77].
Setting inspiratory assist during PAV+
Some approaches have been described to set the gain for PAV+ and are described in Table 1.
Airway pressure targets
Costa et al. [48] suggested to set PAV+ such that the same Pawmean as in the current PSV mode is obtained, and found that respiratory pattern, gas exchange and inspiratory effort where comparable while improving patient-ventilator interaction.
Inspiratory effort targets
Modifying the level of assistance during proportional modes mainly alters respiratory muscle unloading, as tidal volume remains relatively constant, insufflation time is kept close to the neural inspiratory time, and breathing variability and synchronization are preserved. Theoretically, the amount of respiratory muscle unloading would, therefore, be a relevant target to adjust the level of assistance in proportional modes to optimize patient-ventilator interactions. Carteaux et al. [14] assessed the feasibility of setting PAV+ gain to target a predefined range of effort. They used the ability of PAV+ to deliver a pressure proportional to Pmus, where Pmus was recalculated based on estimates from Paw:
A grid built from this equation was available on the ventilator monitor, providing an estimated Pmuspeak for each combination of gain and delta Paw (i.e., Pawpeak – PEEP). Pmus between 5 and 10 cmH2O was defined as a good objective to target a respiratory muscle pressure–time product (PTPmus, i.e., area under the Pmus curve during inspiration) between 50 and 150 cmH2O.s.min−1. The gain was initially set to 50%, and subsequently adjusted to obtain Pmuspeak values within the 5–10 target range. This approach was demonstrated feasible in clinical practice in most patients. It should be noted, however, that measurements of effort as provided by the ventilator may underestimate the patient’s true work of breathing, particularly when intrinsic PEEP is high [79]. Target values may be difficult to achieve in patients with excessive respiratory drive and impaired respiratory mechanics as lung-protective reflexes may be overridden [35, 57].
Monitoring of effort
During PAV+, the measured respiratory system resistance and elastance values provide information on respiratory mechanics and their changes over time or in response to different levels of inspiratory assist [10, 11]. Because compliance and tidal volume are provided, the driving pressure is easily monitored. Furthermore, with these parameters, the ventilator can estimate Pmus on a semi-continuous basis, detecting changes in patient effort over time [4, 14].
Differences with automated modes
Automated ventilation modes such as adaptive support ventilation (ASV) and SmartCare™ continuously adapt certain ventilator settings to keep the patient’s respiratory variables within target ranges set by the clinician [4, 80]. Although NAVA, PAV+, and automated modes all integrate closed-loop principles, it is important to stress that automated modes do not deliver proportional assist, nor directly measure patient effort. In contrast, automated modes incorporate algorithms that attempt to target a desired outcome by automatically modifying ventilator settings according to changes in the patient’s condition [80]. This may reduce the clinician’s workload. Among them, ASV controls minute ventilation by finding the optimum combination of respiratory rate and tidal volume using estimates of the respiratory system time constant [81]. This is based on Otis [82] and Mead [83] models, which postulated that there is an optimum respiratory rate minimizing breathing effort. ASV is suitable for both passive and spontaneously breathing patients, but does not necessarily deliver lung-protective ventilation, which depends on the initial parameters set by the clinician [84, 85]. Provided that it is properly programmed, ASV can provide safe ventilation in the general population; however, caution is required in acute lung injury patients with less compromised compliance as higher tidal volumes may occur [86]. One important difference between automated and proportional modes is the greater importance, with the former, of the way the clinician correctly adjusts the settings. Studies have shown that ASV reduces weaning duration most frequently in the postoperative period [87, 88]. The further evolved fully closed-loop ASV mode, IntelliVent-ASV, incorporates additional control for end-tidal CO2 and oxygen saturation and has shown to be feasible and able to deliver relatively protective ventilation in passive and spontaneously breathing patients with different lung conditions [81, 89]. The automated IntelliVent-ASV weaning protocol provides automatic gradual decreases in inspiratory assist levels while assessing readiness to wean criteria, and has been associated with reduced mechanical ventilation duration in different settings [87, 88]. SmartCare™, a PSV-based mode, was specifically designed to automatically facilitate and expedite the weaning process. It is mainly based on respiratory rate and also integrates values of tidal volume and end-tidal CO2 [90, 91]. Based on certain patient characteristics and targets set by the clinician, automated weaning involves adaptations in the PSV level, followed by an automatic gradual reduction of the PSV level and weaning tests when the level of support is sufficiently low [91]. Compared to non-automated weaning strategies, reductions in weaning time with SmartCare™ were demonstrated in several studies; adequately powered randomized clinical studies are warranted [92, 93].
Conclusion
During PSV ventilator over-assist and poor patient-ventilator interaction are common and often unnoticed. Proportional ventilation modes improve the match between the patient and the ventilator and provide the potential for both lung and diaphragm-protective ventilation. A key challenge is to titrate inspiratory assist levels at the bedside, as optimal targets of respiratory muscle effort may vary among patients and over the course of critical illness. During PAV+, titrating inspiratory assist to reach Pmus targets is feasible, and allows monitoring of breathing effort. In NAVA, it can be recommended as a first approach to set inspiratory assist levels through matching of Pawmean as obtained in PSV, which is a simple and feasible method to perform at the bedside, and readjust subsequently. EAdi-derived indices such as the NME and PVBC hold future promise, but require further studies on their use during the course of mechanical ventilation and in weaning trials. Automated modes differ by requiring the clinician to set parameters to achieve a certain ventilation goal.
Author contribution
The manuscript was drafted by AHJ with guidance of LB. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Compliance with ethical standards
Conflicts of interest
AHJ reports personal fees from Liberate Medical, outside the submitted work. GC reports personal fees from Air Liquide Medical System, personal fees from Löwenstein, outside the submitted work. LH has received grants from Orion Pharma and Liberate Medical and speakers fee from Getinge. LB conducts an investigator-initiated trial on PAV+ (NCT02447692) funded by the Canadian Institute for Health Research and a partnership with Medtronic Covidien; his laboratory also receives grants and non-financial support from Fisher & Paykel, non-financial support from Air Liquide Medical System, non-financial support from Philips, non-financial support from Sentec, other from General Electric. Other authors have nothing to declare.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vaporidi K. NAVA and PAV+ for lung and diaphragm protection. Curr Opin Crit Care. 2020;26:41–46. doi: 10.1097/MCC.0000000000000684. [DOI] [PubMed] [Google Scholar]
- 2.Younes M. Proportional assist ventilation, a new approach to ventilatory support: theory. Am Rev Respir Dis. 1992;145:114–120. doi: 10.1164/ajrccm/145.1.114. [DOI] [PubMed] [Google Scholar]
- 3.Sinderby C, Navalesi P, Beck J, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med. 1999;5:1433–1436. doi: 10.1038/71012. [DOI] [PubMed] [Google Scholar]
- 4.Suarez-Sipmann F. New modes of assisted mechanical ventilation. Med Intensive Engl Ed. 2014;38:249–260. doi: 10.1016/j.medine.2014.04.001. [DOI] [PubMed] [Google Scholar]
- 5.Goligher EC, Fan E, Herridge MS, et al. Evolution of diaphragm thickness during mechanical ventilation impact of inspiratory effort. Am J Respir Crit Care Med. 2015;192:1080–1088. doi: 10.1164/rccm.201503-0620OC. [DOI] [PubMed] [Google Scholar]
- 6.Kondili E, Prinianakis G, Georgopoulos D. Patient-ventilator interaction. Br J Anaesth. 2003;91:106–119. doi: 10.1093/bja/aeg129. [DOI] [PubMed] [Google Scholar]
- 7.Leung P, Jubran A, Tobin MJ. Comparison of assisted ventilator modes on triggering, patient effort, and dyspnea. Am J Respir Crit Care Med. 1997;155:1940–1948. doi: 10.1164/ajrccm.155.6.9196100. [DOI] [PubMed] [Google Scholar]
- 8.Thille AW, Cabello B, Galia F, et al. Reduction of patient-ventilator asynchrony by reducing tidal volume during pressure-support ventilation. Intensive Care Med. 2008;34:1477–1486. doi: 10.1007/s00134-008-1121-9. [DOI] [PubMed] [Google Scholar]
- 9.Colombo D, Cammarota G, Alemani M, et al. Efficacy of ventilator waveforms observation in detecting patient–ventilator asynchrony. Crit Care Med. 2011;39:2452–2457. doi: 10.1097/CCM.0b013e318225753c. [DOI] [PubMed] [Google Scholar]
- 10.Younes M, Kun J, Masiowski B, et al. A method for noninvasive determination of inspiratory resistance during proportional assist ventilation. Am J Respir Crit Care Med. 2001;163:829–839. doi: 10.1164/ajrccm.163.4.2005063. [DOI] [PubMed] [Google Scholar]
- 11.Younes M, Webster K, Kun J, et al. A method for measuring passive elastance during proportional assist ventilation. Am J Respir Crit Care Med. 2001;164:50–60. doi: 10.1164/ajrccm.164.1.2010068. [DOI] [PubMed] [Google Scholar]
- 12.Xirouchaki N, Kondili E, Klimathianaki M, Georgopoulos D. Is proportional-assist ventilation with load-adjustable gain factors a user-friendly mode? Intensive Care Med. 2009;35:1599–1603. doi: 10.1007/s00134-009-1524-2. [DOI] [PubMed] [Google Scholar]
- 13.Terzi N, Piquilloud L, Rozé H, et al. Clinical review: update on neurally adjusted ventilatory assist - report of a round-table conference. Crit Care. 2012;16:225. doi: 10.1186/cc11297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Carteaux G, Mancebo J, Mercat A, et al. Bedside adjustment of proportional assist ventilation to target a predefined range of respiratory effort. Crit Care Med. 2013;41:2125–2132. doi: 10.1097/CCM.0b013e31828a42e5. [DOI] [PubMed] [Google Scholar]
- 15.Telias I, Brochard L, Goligher EC. Is my patient’s respiratory drive (too) high? Intensive Care Med. 2018;44:1936–1939. doi: 10.1007/s00134-018-5091-2. [DOI] [PubMed] [Google Scholar]
- 16.Yoshida T, Nakahashi S, Nakamura MAM, et al. Volume-controlled ventilation does not prevent injurious inflation during spontaneous effort. Am J Respir Crit Care Med. 2017;196:590–601. doi: 10.1164/rccm.201610-1972OC. [DOI] [PubMed] [Google Scholar]
- 17.Jonkman AH, de Vries HJ, Heunks LMA. Physiology of the respiratory drive in icu patients: implications for diagnosis and treatment. Crit Care. 2020;24:104. doi: 10.1186/s13054-020-2776-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Demoule A, Clavel M, Rolland-Debord C, et al. Neurally adjusted ventilatory assist as an alternative to pressure support ventilation in adults: a French multicentre randomized trial. Intensive Care Med. 2016;42:1723–1732. doi: 10.1007/s00134-016-4447-8. [DOI] [PubMed] [Google Scholar]
- 19.Kataoka J, Kuriyama A, Norisue Y, Fujitani S. Proportional modes versus pressure support ventilation: a systematic review and meta-analysis. Ann Intensive Care. 2018;8:123. doi: 10.1186/s13613-018-0470-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liu L, Xu X, Sun Q, et al (2020) Neurally adjusted ventilatory assist versus pressure support ventilation in diffiult weaning. Anesthesiology 1482–93 [DOI] [PubMed]
- 21.Hadfield DJ, Rose L, Reid F, et al. Neurally adjusted ventilatory assist versus pressure support ventilation: a randomized controlled feasibility trial performed in patients at risk of prolonged mechanical ventilation. Crit Care. 2020;24:220. doi: 10.1186/s13054-020-02923-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Esteban A, Ferguson ND, Meade MO, et al. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177:170–177. doi: 10.1164/rccm.200706-893OC. [DOI] [PubMed] [Google Scholar]
- 23.Tobin MJ, Gardner W. Principles and practice of intensive care monitoring. New York: McGraw-Hill; 1998. Monitoring the control of breathing; pp. 415–464. [Google Scholar]
- 24.Telias I, Spadaro S. Techniques to monitor respiratory drive and inspiratory effort. Curr Opin Crit Care. 2020;26:3–10. doi: 10.1097/MCC.0000000000000680. [DOI] [PubMed] [Google Scholar]
- 25.Beck J, Gottfried SB, Navalesi P, et al. Electrical activity of the diaphragm during pressure support ventilation in acute respiratory failure. Am J Respir Crit Care Med. 2001;164:419–424. doi: 10.1164/ajrccm.164.3.2009018. [DOI] [PubMed] [Google Scholar]
- 26.Bellani G, Mauri T, Coppadoro A, et al. Estimation of patient’s inspiratory effort from the electrical activity of the diaphragm. Crit Care Med. 2013;41:1483–1491. doi: 10.1097/CCM.0b013e31827caba0. [DOI] [PubMed] [Google Scholar]
- 27.Sinderby C, Beck J, Spahija J, et al. Inspiratory muscle unloading by neurally adjusted ventilatory assist during maximal inspiratory efforts in healthy subjects. Chest. 2007;131:711–717. doi: 10.1378/chest.06-1909. [DOI] [PubMed] [Google Scholar]
- 28.Spinelli E, Mauri T, Beitler JR, et al. Respiratory drive in the acute respiratory distress syndrome: pathophysiology, monitoring, and therapeutic interventions. Intensive Care Med. 2020;46:606–618. doi: 10.1007/s00134-020-05942-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tang G-J, Kou YR, Lin YS (1998) Peripheral neural modulation of endotoxin-induced hyperventilation. Crit Care Med 26 [DOI] [PubMed]
- 30.Jacono FJ, Mayer CA, Hsieh Y-H, et al. Lung and brainstem cytokine levels are associated with breathing pattern changes in a rodent model of acute lung injury. Respir Physiol Neurobiol. 2011;178:429–438. doi: 10.1016/j.resp.2011.04.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lilitsis E, Stamatopoulou V, Andrianakis E, et al. Inspiratory effort and breathing pattern change in response to varying the assist level: a physiological study. Respir Physiol Neurobiol. 2020 doi: 10.1016/j.resp.2020.103474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kacmarek RM. Proportional assist ventilation and neurally adjusted ventilatory assist. Respir Care. 2011;56:140–152. doi: 10.4187/respcare.01021. [DOI] [PubMed] [Google Scholar]
- 33.Georgopoulos D, Mitrouska I, Webster K, et al. Effects of inspiratory muscle unloading on the response of respiratory motor output to CO2. Am J Respir Crit Care Med. 1997;155:2000–2009. doi: 10.1164/ajrccm.155.6.9196108. [DOI] [PubMed] [Google Scholar]
- 34.Georgopoulos D, Mitrouska I, Bshouty Z, et al. Respiratory response to co2 during pressure-support ventilation in conscious normal humans. Am J Respir Crit Care Med. 1997;156:146–154. doi: 10.1164/ajrccm.156.1.9606055. [DOI] [PubMed] [Google Scholar]
- 35.Vaporidi K, Akoumianaki E, Telias I, et al. Respiratory drive in critically ill patients. Pathophysiology and clinical implications. Am J Respir Crit Care Med. 2020;201:20–32. doi: 10.1164/rccm.201903-0596SO. [DOI] [PubMed] [Google Scholar]
- 36.Mitrouska J, Xirouchaki N, Patakas D, et al. Effects of chemical feedback on respiratory motor and ventilatory output during different modes of assisted mechanical ventilation. Eur Respir J. 1999;13:873. doi: 10.1034/j.1399-3003.1999.13d30.x. [DOI] [PubMed] [Google Scholar]
- 37.Brochard L, Harf A, Lorino H, Lemaire F. Inspiratory pressure support prevents diaphragmatic fatigue during weaning from mechanical ventilation. Am Rev Respir Dis. 1989;139:513–521. doi: 10.1164/ajrccm/139.2.513. [DOI] [PubMed] [Google Scholar]
- 38.Carteaux G, Córdoba-Izquierdo A, Lyazidi A, et al. Comparison between neurally adjusted ventilatory assist and pressure support ventilation levels in terms of respiratory effort. Crit Care Med. 2016;44:503–511. doi: 10.1097/CCM.0000000000001418. [DOI] [PubMed] [Google Scholar]
- 39.Parthasarathy S, Tobin MJ. Effect of ventilator mode on sleep quality in critically ill patients. Am J Respir Crit Care Med. 2002;166:1423–1429. doi: 10.1164/rccm.200209-999OC. [DOI] [PubMed] [Google Scholar]
- 40.Marini JJ, Rodriguez RM, Lamb V. The Inspiratory workload of patient-initiated mechanical ventilation. Am Rev Respir Dis. 1986;134:902–909. doi: 10.1164/arrd.1986.134.5.902. [DOI] [PubMed] [Google Scholar]
- 41.Doorduin J, Sinderby C, Beck J, et al. Assisted ventilation in patients with acute respiratory distress syndrome: lung-distending pressure and patient-ventilator interaction. Anesthesiology. 2015 doi: 10.1183/13993003.congress-2015.OA4478. [DOI] [PubMed] [Google Scholar]
- 42.Patroniti N, Bellani G, Saccavino E, et al. Respiratory pattern during neurally adjusted ventilatory assist in acute respiratory failure patients. Intensive Care Med. 2012;38:230–239. doi: 10.1007/s00134-011-2433-8. [DOI] [PubMed] [Google Scholar]
- 43.Spahija J, de Marchie M, Albert M, et al. Patient-ventilator interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med. 2010;38:518–526. doi: 10.1097/CCM.0b013e3181cb0d7b. [DOI] [PubMed] [Google Scholar]
- 44.Jonkman AH, Roesthuis LH, de Boer EC, et al. Inadequate assessment of patient-ventilator interaction due to suboptimal diaphragm electrical activity signal filtering. Am J Respir Crit Care Med. 2020;202:141–144. doi: 10.1164/rccm.201912-2306LE. [DOI] [PubMed] [Google Scholar]
- 45.Cecchini J, Schmidt M, Demoule A, Similowski T. Increased diaphragmatic contribution to inspiratory effort during neurally adjusted ventilatory assistance versus pressure support: an electromyographic study. Anesthesiology. 2014;121:1028–1036. doi: 10.1097/ALN.0000000000000432. [DOI] [PubMed] [Google Scholar]
- 46.Blankman P, Hasan D, van Mourik MS, Gommers D. Ventilation distribution measured with EIT at varying levels of pressure support and neurally adjusted ventilatory assist in patients with ALI. Intensive Care Med. 2013;39:1057–1062. doi: 10.1007/s00134-013-2898-8. [DOI] [PubMed] [Google Scholar]
- 47.Di Mussi R, Spadaro S, Mirabella L, et al. Impact of prolonged assisted ventilation on diaphragmatic efficiency: NAVA versus PSV. Crit Care. 2015;20:1. doi: 10.1186/s13054-015-1178-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Costa R, Spinazzola G, Cipriani F, et al. A physiologic comparison of proportional assist ventilation with load-adjustable gain factors (PAV+) versus pressure support ventilation (PSV) Intensive Care Med. 2011;37:1494–1500. doi: 10.1007/s00134-011-2297-y. [DOI] [PubMed] [Google Scholar]
- 49.Kondili E, Prinianakis G, Alexopoulou C, et al. Respiratory load compensation during mechanical ventilation: proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med. 2006;32:692–699. doi: 10.1007/s00134-006-0110-0. [DOI] [PubMed] [Google Scholar]
- 50.Akoumianaki E, Prinianakis G, Kondili E, et al. Physiologic comparison of neurally adjusted ventilator assist, proportional assist and pressure support ventilation in critically ill patients. Respir Physiol Neurobiol. 2014;203:82–89. doi: 10.1016/j.resp.2014.08.012. [DOI] [PubMed] [Google Scholar]
- 51.Wrigge H, Golisch W, Zinserling J, et al. Proportional assist versus pressure support ventilation: effects on breathing pattern and respiratory work of patients with chronic obstructive pulmonary disease. Intensive Care Med. 1999;25:790–798. doi: 10.1007/s001340050954. [DOI] [PubMed] [Google Scholar]
- 52.Piquilloud L, Vignaux L, Bialais E, et al. Neurally adjusted ventilatory assist improves patient–ventilator interaction. Intensive Care Med. 2011;37:263–271. doi: 10.1007/s00134-010-2052-9. [DOI] [PubMed] [Google Scholar]
- 53.Schmidt M, Kindler F, Cecchini J, et al. Neurally adjusted ventilatory assist and proportional assist ventilation both improve patient-ventilator interaction. Crit Care. 2015;19:56. doi: 10.1186/s13054-015-0763-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lecomte F, Brander L, Jalde F, et al. Physiological response to increasing levels of neurally adjusted ventilatory assist (NAVA) Respir Physiol Neurobiol. 2009;166:117–124. doi: 10.1016/j.resp.2009.02.015. [DOI] [PubMed] [Google Scholar]
- 55.Leiter JC, Manning HL. The Hering-Breuer reflex, feedback control, and mechanical ventilation: the promise of neurally adjusted ventilatory assist. Crit Care Med. 2010;38:1915–1916. doi: 10.1097/CCM.0b013e3181ee4039. [DOI] [PubMed] [Google Scholar]
- 56.Smith J, Bellemare F. Effect of lung volume on in vivo contraction characteristics of human diaphragm. J Appl Physiol. 1987;62:1893–1900. doi: 10.1152/jappl.1987.62.5.1893. [DOI] [PubMed] [Google Scholar]
- 57.Vaporidi K, Psarologakis C, Proklou A, et al. Driving pressure during proportional assist ventilation: an observational study. Ann Intensive Care. 2019;9:1. doi: 10.1186/s13613-018-0477-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Xirouchaki N, Kondili E, Vaporidi K, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med. 2008;34:2026–2034. doi: 10.1007/s00134-008-1209-2. [DOI] [PubMed] [Google Scholar]
- 59.Bosma KJ, Read BA, Bahrgard Nikoo MJ, et al. A pilot randomized trial comparing weaning from mechanical ventilation on pressure support versus proportional assist ventilation. Crit Care Med. 2016;44:1098–1108. doi: 10.1097/CCM.0000000000001600. [DOI] [PubMed] [Google Scholar]
- 60.Bosma K, Ferreyra G, Ambrogio C, et al. Patient-ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med. 2007;35:1048–1054. doi: 10.1097/01.CCM.0000260055.64235.7C. [DOI] [PubMed] [Google Scholar]
- 61.Delisle S, Ouellet P, Bellemare P, et al. Sleep quality in mechanically ventilated patients: comparison between NAVA and PSV modes. Ann Intensive Care. 2011;1:42. doi: 10.1186/2110-5820-1-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Alexopoulou C, Kondili E, Plataki M, Georgopoulos D. Patient–ventilator synchrony and sleep quality with proportional assist and pressure support ventilation. Intensive Care Med. 2013;39:1040–1047. doi: 10.1007/s00134-013-2850-y. [DOI] [PubMed] [Google Scholar]
- 63.Fernández-Vivas M, Caturla-Such J, de la Rosa JG, et al. Noninvasive pressure support versus proportional assist ventilation in acute respiratory failure. Intensive Care Med. 2003;29:1126–1133. doi: 10.1007/s00134-003-1768-1. [DOI] [PubMed] [Google Scholar]
- 64.de la Oliva P, Schüffelmann C, Gómez-Zamora A, et al. Asynchrony, neural drive, ventilatory variability and COMFORT: NAVA versus pressure support in pediatric patients. A non-randomized cross-over trial. Intensive Care Med. 2012;38:838–846. doi: 10.1007/s00134-012-2535-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Sinderby C, Beck J. Neurally adjusted ventilatory assist. In: Martin JT, editor. Principles and practice of mechanical ventilation. 3. New York: McGraw-Hill; 2013. pp. 351–375. [Google Scholar]
- 66.Coisel Y, Chanques G, Jung B, et al. Neurally adjusted ventilatory assist in critically ill postoperative patients: a crossover randomized study. Anesthesiology. 2010;113:925–935. doi: 10.1097/ALN.0b013e3181ee2ef1. [DOI] [PubMed] [Google Scholar]
- 67.Brander L, Leong-Poi H, Beck J, et al. Titration and implementation of neurally adjusted ventilatory assist in critically ill patients. Chest. 2009;135:695–703. doi: 10.1378/chest.08-1747. [DOI] [PubMed] [Google Scholar]
- 68.Barwing J, Linden N, Ambold M, et al. Neurally adjusted ventilatory assist vs. pressure support ventilation in critically ill patients: an observational study. Acta Anaesthesiol Scand. 2011;55:1261–1271. doi: 10.1111/j.1399-6576.2011.02522.x. [DOI] [PubMed] [Google Scholar]
- 69.Rozé H, Lafrikh A, Perrier V, et al. Daily titration of neurally adjusted ventilatory assist using the diaphragm electrical activity. Intensive Care Med. 2011;37:1087–1094. doi: 10.1007/s00134-011-2209-1. [DOI] [PubMed] [Google Scholar]
- 70.Bertoni M, Telias I, Urner M, et al. A novel non-invasive method to detect excessively high respiratory effort and dynamic transpulmonary driving pressure during mechanical ventilation. Crit Care. 2019;23:346. doi: 10.1186/s13054-019-2617-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Campoccia Jalde F, Jalde F, Wallin MKEB, et al. Standardized unloading of respiratory muscles during neurally adjusted ventilatory assist: a randomized crossover pilot study. Anesthesiology. 2018;129:769–777. doi: 10.1097/ALN.0000000000002335. [DOI] [PubMed] [Google Scholar]
- 72.Cammarota G, Longhini F, Perucca R, et al. New setting of neurally adjusted ventilatory assist during noninvasive ventilation through a helmet. Anesthesiology. 2016;125:1181–1189. doi: 10.1097/ALN.0000000000001354. [DOI] [PubMed] [Google Scholar]
- 73.Liu L, Xia F, Yang Y, et al. Neural versus pneumatic control of pressure support in patients with chronic obstructive pulmonary diseases at different levels of positive end expiratory pressure: a physiological study. Crit Care. 2015;19:244. doi: 10.1186/s13054-015-0971-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Beloncle F, Piquilloud L, Rittayamai N, et al. A diaphragmatic electrical activity-based optimization strategy during pressure support ventilation improves synchronization but does not impact work of breathing. Crit Care. 2017;21:21. doi: 10.1186/s13054-017-1599-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Grasselli G, Beck J, Mirabella L, et al. Assessment of patient–ventilator breath contribution during neurally adjusted ventilatory assist. Intensive Care Med. 2012;38:1224–1232. doi: 10.1007/s00134-012-2588-y. [DOI] [PubMed] [Google Scholar]
- 76.Jonkman AH, Jansen D, Gadgil S, et al. Monitoring patient-ventilator breath contribution in the critically ill during neurally adjusted ventilatory assist: reliability and improved algorithms for bedside use. J Appl Physiol. 2019;127:264–271. doi: 10.1152/japplphysiol.00071.2019. [DOI] [PubMed] [Google Scholar]
- 77.Jansen D, Jonkman AH, Roesthuis L, et al. Estimation of the diaphragm neuromuscular efficiency index in mechanically ventilated critically ill patients. Crit Care. 2018;22:238. doi: 10.1186/s13054-018-2172-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Coppadoro A, Rona R, Bellani G, Foti G. A brief airway occlusion is sufficient to measure the patient’s inspiratory effort/electrical activity of the diaphragm index (PEI) J Clin Monit Comput. 2020 doi: 10.1007/s10877-020-00459-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Beloncle F, Akoumianaki E, Rittayamai N, et al. Accuracy of delivered airway pressure and work of breathing estimation during proportional assist ventilation: a bench study. Ann Intensive Care. 2016;6:30. doi: 10.1186/s13613-016-0131-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.van der Staay M, Chatburn RL. Advanced modes of mechanical ventilation and optimal targeting schemes. Intensive Care Med Exp. 2018;6:30. doi: 10.1186/s40635-018-0195-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Arnal J-M, Wysocki M, Novotni D, et al. Safety and efficacy of a fully closed-loop control ventilation (IntelliVent-ASV®) in sedated ICU patients with acute respiratory failure: a prospective randomized crossover study. Intensive Care Med. 2012;38:781–787. doi: 10.1007/s00134-012-2548-6. [DOI] [PubMed] [Google Scholar]
- 82.Otis AB, Fenn WO, Rahn H. Mechanics of breathing in man. J Appl Physiol. 1950;2:592–607. doi: 10.1152/jappl.1950.2.11.592. [DOI] [PubMed] [Google Scholar]
- 83.Mead J. Control of respiratory frequency. J Appl Physiol. 1960;15:325–336. doi: 10.1152/jappl.1960.15.3.325. [DOI] [Google Scholar]
- 84.Sulemanji D, Marchese A, Garbarini P, et al. Adaptive support ventilation: an appropriate mechanical ventilation strategy for acute respiratory distress syndrome? Anesthesiology. 2009;111:863–870. doi: 10.1097/ALN.0b013e3181b55f8f. [DOI] [PubMed] [Google Scholar]
- 85.Dongelmans DA, Veelo DP, Bindels A, et al. Determinants of tidal volumes with adaptive support ventilation: a multicenter observational study. Anesth Analg. 2008;107:932–937. doi: 10.1213/ane.0b013e31817f1dcf. [DOI] [PubMed] [Google Scholar]
- 86.Dongelmans DA, Paulus F, Veelo DP, et al. Adaptive support ventilation may deliver unwanted respiratory rate–tidal volume combinations in patients with acute lung injury ventilated according to an open lung concept. Anesthesiology. 2011;114:1138–1143. doi: 10.1097/ALN.0b013e31820d8676. [DOI] [PubMed] [Google Scholar]
- 87.Gruber PC, Gomersall CD, Leung P, et al. Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology. 2008;109:81–87. doi: 10.1097/ALN.0b013e31817881fc. [DOI] [PubMed] [Google Scholar]
- 88.Chen C-W, Wu C-P, Dai Y-L, et al. Effects of implementing adaptive support ventilation in a medical intensive care unit. Respir Care. 2011;56:976–983. doi: 10.4187/respcare.00966. [DOI] [PubMed] [Google Scholar]
- 89.Arnal J-M, Garnero A, Novonti D, et al. Feasibility study on full closed-loop control ventilation (IntelliVent-ASV™) in ICU patients with acute respiratory failure: a prospective observational comparative study. Crit Care. 2013;17:R196. doi: 10.1186/cc12890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Lellouche F, Mancebo J, Jolliet P, et al. A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. Am J Respir Crit Care Med. 2006;174:894–900. doi: 10.1164/rccm.200511-1780OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Dojat M, Brochard L, Lemaire F, Harf A. A knowledge-based system for assisted ventilation of patients in intensive care units. Int J Clin Monit Comput. 1992;9:239–250. doi: 10.1007/BF01133619. [DOI] [PubMed] [Google Scholar]
- 92.Burns KE, Lellouche F, Nisenbaum R, et al. Automated weaning and SBT systems versus non-automated weaning strategies for weaning time in invasively ventilated critically ill adults. Cochrane Database Syst Rev. 2014 doi: 10.1002/14651858.CD008638.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Lellouche F, Brochard L. Advanced closed loops during mechanical ventilation (PAV, NAVA, ASV, SmartCare) Best Pract Res Clin Anaesthesiol. 2009;23:81–93. doi: 10.1016/j.bpa.2008.08.001. [DOI] [PubMed] [Google Scholar]