

Summary
Objective
Health care providers can effectively participate in oral health promotion for children in primary care setting. Currently, there are no oral health promotion programs that involve primary health care professionals in Qatar. Hence, this study was undertaken to examine the knowledge, attitudes and practices of all health professionals who work in the Well baby Clinics in the primary health centers.
Method
A 23-item questionnaire was distributed across 20 primary health centers. The questionnaire sought information on the demographic data of health professionals, their knowledge of oral health and their practices and attitudes towards critical oral health issues. Data were examined by Pearson Chi-squared tests or Fisher’s Exact test (p = 0.05).
Results
The response rate of the health professionals was 67%. Only 35.7% of the 225 participants received some form of oral health training during their undergraduate programme. The participants would assess the dental problem of the child (p = 0.05) and discuss the importance of tooth brushing with the mother (p = 0.03). A significant number of respondents (p = 0.04) were unlikely to assess the children’s fluoride intake. There was a significant difference in the group of participants that would examine the child’s teeth (p = 0.1) and counsel the mothers on prevention of dental problems (p = 0.01). This group would also refer children to dentist at 12 months of age (p = 0.05).
Conclusions
Health professionals had a positive attitude towards the anticipatory guidance elements of oral health. However, the knowledge of healthcare professionals on childhood oral health is rather limited.
Keywords: Oral health promotion, Attitude of health personnel, Preventive dentistry, Health knowledge, Health care surveys, Primary health care
Introduction
Oral health, now considered an inherent component of general health, is defined by the World Health Organization (WHO) as “a state when an individual is free of chronic oro-facial pain, oral sores or cancer, craniofacial defects such as oral clefts, gum diseases, dental decay, tooth loss or any other disorders affecting oro-dental tissues” [1]. Numerous studies have shown the association of oral health with systemic health and general well being including major chronic conditions such as obesity, cardiac diseases, diabetes and respiratory infections [2-4]. The most widely proposed mechanisms by which oral health status affects systemic heath include: a) inflammatory mechanisms: inflammation derived from host immune response against dental and/ or periodontal pathogens give rise to molecules that gain access to the circulatory system, producing systemic inflammation; b) bacterial mechanisms: bacteria and its products directly invade the tissues of the organism; c) vascular mechanisms: dental and periodontal pathogens present in the systemic circulation cause platelet aggregation and thrombus formation [5, 6]. In spite of the significance of oral health and the association with general health, it has not received the necessary attention in many regions of the world including many parts of the South-East Asia Region (SEARO), Eastern Mediterranean Region (EMRO) and Western Pacific Region (WPRO) [7]. The oral health of children, in particular, remains a concern worldwide. Early childhood caries is a major health issue and can cause distress to young children [8, 9]. Despite the acute importance of oral health, periodic dental assessment and care for children is unorganized in most countries including but not limited to Afghanistan, Philippines, Madagascar, Bolivia, Burundi, Chad, Haiti, Myanmar, Nepal, Pakistan, India, Rawanda, Senegal, Yemen and Zimbabwe [7].
Primary health care professionals including Pediatricians, play a vital role in many preventive activities for young children such as assessment of milestones and immunizations. There is mounting evidence that health care providers play a significant role not only in the systemic health but also oral health promotion for children in the primary care setting [10-12].
A recent study analyzed data derived from 195 countries between 1990 and 2015 and found that based on mortality from causes amenable to personal healthcare Qatar has the best Healthcare Access and Quality Index in the GCC (Gulf Cooperation Council) region [13]. Further, it ranked 28th in the overall list and has shown substantial progress in the quality of healthcare in the past 30 years [13]. In spite of these healthcare developments, oral health remains a critical public concern for authorities in Qatar [14]. Several studies conducted in the Gulf Cooperation Council countries including Qatar have documented a high prevalence of dental caries in young children. These studies have strongly emphasized the necessity of community-based preventive programs and professional care that should begin during pregnancy and early childhood [15]. Routine Well Baby Clinics (WBCs) are established at all primary health centers throughout the country and they serve as vital tools to promote children’s general health. Further, child care at these clinics also helps to detect and eliminate the potential health problems affecting the development, behavior and education of children. All residents of Qatar have access to these primary health centers at exceptionally subsidized cost and their children can avail services of WBCs at these centers.
Oral health services in Qatar are given considerable attention by health care planners and the dental workforce is responsible for implementing these services. However, there are no standardized oral health promotion programs involving primary health care professionals (excluding dentists) caring for children in these WBCs. The healthcare workforce in Qatar includes professionals from various countries with different educational backgrounds and diverse clinical experience. Consequently, the language barrier arising out of this diversity may hinder the participation of these professionals in health promotion regimes [16]. Furthermore, it is essential to assess the level of oral health literacy and assess if health professionals have the desired knowledge before designing such a program for oral health promotion. Hence, the aim of this study was to examine the knowledge, attitudes and practices of all health professionals including paediatricians, family physicians, general medical practitioners and nurses who work in the Well baby Clinics in the primary health centers in Qatar.
Methods
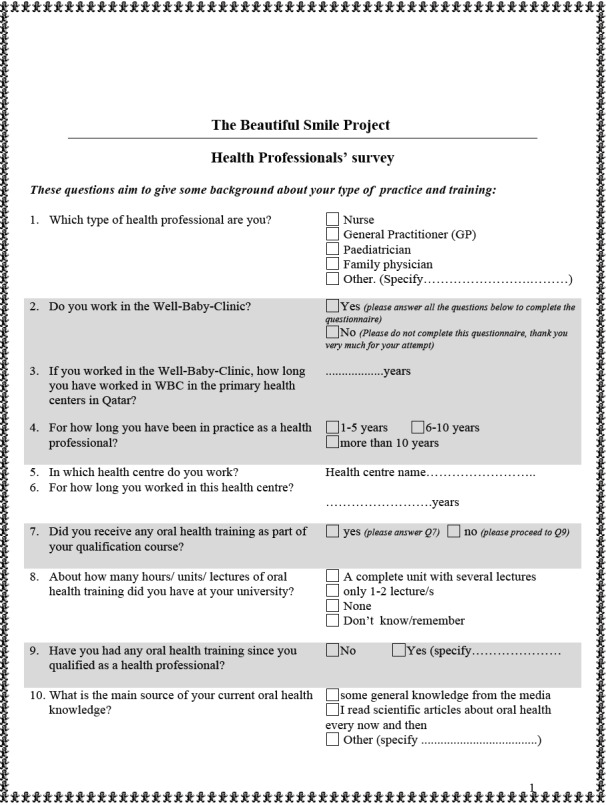
This descriptive cross-sectional study was conducted an all 20 WBCs at all primary health care centers in Qatar. The data was collected via a two-page self-completed paper-based questionnaire developed after reviewing the relevant literature (Appendix 1). A literature search was carried out by applying the key terms including and relating to oral health knowledge of health care practitioners to appropriate data sources (Medline [MeSH] via OVID, Embase via OVID, Pubmed, Cochrane Central Register of Controlled Trials and OpenSiGLE). The key words “oral health promotion”, “attitude of health personnel”, “preventive dentistry”, “health knowledge”, “health care surveys”, “primary health care”. The questionnaire was primarily adopted from a previous study by Lewis and co-workers (2000) [10] but was modified slightly concordant with the protocols at WBCs. The questionnaire was tested in a pilot study which preceded the main study to test the feasibility of this approach. The data from the pilot study were not included in the main study. The standardized instrument underwent reliability testing with Cronbach’s alpha score of 0.79.
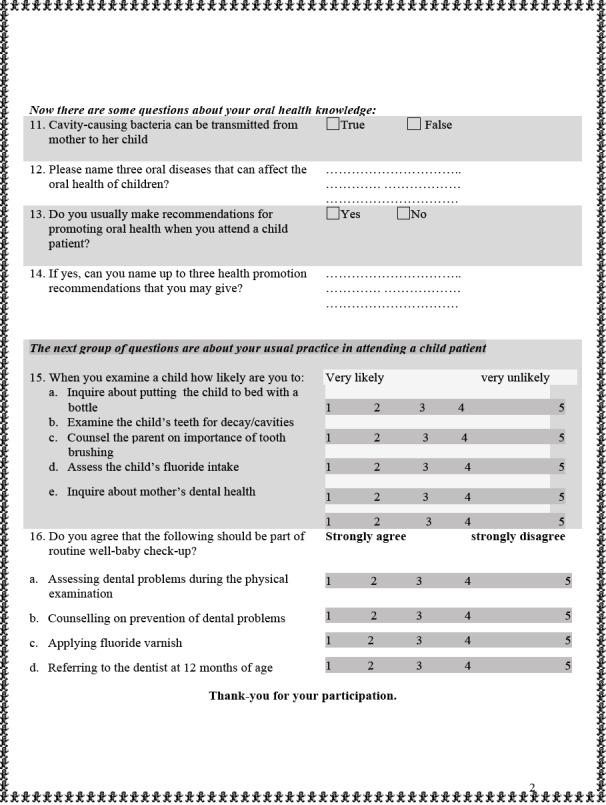
The questionnaire contained 3 sections and 16 items. The first section contained demographic data including details of experience and training. Also, this section included two questions about the involvement of the health practitioners with the WBC. Participants were asked to specify their profession and whether they worked in the WBC. If they were not working in the WBCs then they were asked to refrain from completing the questionnaire. Participation in the WBC thus became the sole inclusion criterion for the study. The second section sought information about the knowledge of health practitioners about oral diseases and oral health promotion approaches. This section was designed to include information regarding oral health training received by the health care provider during under graduate training, the type of oral health training; further oral health training received after graduation and their source of oral health knowledge at the time the investigation was conducted. Also, this component inquired the health care practitioners’ knowledge on transmission of caries causing bacteria from mother to child [17] and if they provided oral health recommendations to their patients. The third section comprised questions about the practices and attitudes of the health practitioner towards critical oral health issues. This segment comprised questions that explored oral health practices of health care practitioners including enquiring about nocturnal bottle feeding, assessing dental problems, discussing importance of tooth brushing with mother, assessing the child’s fluoride intake [18] and scrutinize the mothers ‘oral health status. The respondents marked their answers as one of the following - very likely, likely, neutral, unlikely or very unlikely. Further, this section assessed the attitudes of participants towards dental examination of children, counseling mothers on prevention of dental problems, application of topical fluoride varnish [19, 20], and referral of children to dentist at 12 months of age. The participants were asked to select one of the following responses: strongly agree, agree, neutral, disagree or strongly disagree. Table I shows the dependent and independent variables used to explore the survey results.
Tab. I.
The dependent and independent variables for the survey.
| Independent variables | Dependent variables |
|---|---|
Demographic characteristics:
|
Knowledge:
|
Oral health training received:
|
Practices:
|
Attitudes:
|
The targeted population was health professionals working in WBCs including nurses, pediatricians, family physicians and general medical practitioners (GPs). These health professionals were employed in the primary health care centers and were not exclusively posted in WBCs, but they attended the clinic on a rotational basis, once a week per calendar month.
The participants were recruited in two phases. In the first phase 168 health professionals from all 20 health centers were approached to participate. Health professionals from only seven health centers responded and the response rate was low (53.6%). This highlighted a problem in the survey distribution method, which was delivered via email through health centre directors. The situation was amended and the surveys were re-sent individually in envelopes to the remaining 13 health centers which had not responded in the first phase. The head nurse of each of these 13 health centers was assigned the responsibility to receive the surveys via the central mail of the Primary Health Care Centers. The questionnaires were sent to the participants in sealed envelopes via the central internal mail of the Primary Health Care Centers. Sealed boxes were provided at each health centre for collection of completed questionnaires to ensure confidentiality for participants. The sealed boxes were then returned to the research office via courier.
The questionnaire data were entered into Microsoft® Excel 2003 spread sheets (Microsoft Corporation, Seattle, Washington, USA) and exported to SPSS 20.0™ for Windows® (SPSS Incorporated, Chicago, Illinois, USA). The data were analyzed and descriptive statistics and frequency tables for dependent and independent variables were prepared. Categorical data were examined by Pearson Chi-squared tests (p = 0.05) or Fisher’s Exact test. The outcome measures (dependent variables) were the oral health knowledge of participants, and; their clinical practices and attitudes related to oral health of preschool children. The data analysis was based on determining whether the demographic characteristics of health professionals affected their knowledge, attitudes and practices towards oral health of young children.
Results
The response rate for the first phase was 53.6%, as 90 out of 168 health professionals responded to the questionnaire. However, this included the unanticipated response of 22 dental professionals. These respondents were excluded from the study as they did not meet the inclusion criteria of attending the WBCs. Moreover, their dental knowledge would differ significantly from the other participants and would induce bias in the study. Thus, a total of 68 out of 146 valid responses were obtained in the first phase. In the second phase, 190 questionnaires were distributed of which 157 health professionals responded (response rate = 82.6%). The data from both phases were pooled together in the analysis and the total number of respondents were 225 (response rate = 67.0%). There were no repeat responses as the participants from the seven health centers in the first phase were excluded in the second phase to avoid bias by “learned response”.
Furthermore, some participants did not respond to all the questions in the survey. These specific questions which were left unanswered were excluded from the analysis. However, the other responses which were marked from the same participants were evaluated. Hence, not all the questions in the survey received 225 responses.
Most respondents in the study were nurses (n = 174, 77.3%) (Tab. II). The participating health professionals were in clinical practice since 8 ± 5.6 years and the mean number of years these professionals had been in the WBC was 7 ± 4.3 years. Only 35.7% of the participants received some form of oral health training during their undergraduate programme. Further, 32.9% of these participants could not remember what sort of oral health education were they imparted. After graduation, only 41 (20.1%) participants received further oral health education. Besides, a little more than half of the participants (51.7%) cited “media” as their source of general knowledge on oral health, particularly television. (Tab. III).
Tab. II.
Distribution of occupation and years of clinical experience of responding health professionals.
| Demographics | Respondents (%) |
|---|---|
| Nurses General medical practitioners (GPs) Paediatricians Family physicians Medical health professionals (total) |
174 (77.3) 18(8) 23 (10.2) 10 (4.4) 225(100) |
| Years of clinical experience | 225(100) 26 (11.6) 53 (23.6) 146 (64.8) |
| 1-5 years 6-10 years More than 10 years |
Tab. III.
Distribution of responses of health professionals to oral health training and knowledge questions.
| Oral health training and knowledge | Responses (%) |
|---|---|
| Oral health training received in under graduate programme | 221(100) |
| Yes No |
79 (35.7) 142 (64.3) |
| Type of oral health training in under graduate qualification | 79(100) |
| Completed unit with several lectures Only 1-2 lectures Do not know/ cannot remember |
24 (30.4) 29 (36.7) 26 (32.9) |
| Any further oral health training received after graduation | 204(100) |
| Yes No |
41 (20.1) 163 (79.9) |
| Current sources of oral health knowledge | 201(100) |
| Some general knowledge from the media Read scientific articles about oral health occasionally Others |
104 (51.7) 79 (39.3) 18 (8.9) |
| Usually give oral health recommendations | 213(100) |
| Yes No |
166 (77.9) 47 (22.1) |
| Caries - causing bacteria can be transmitted from mother to child | 212(100) |
| True False |
100 (47.2) 112 (52.8) |
Many health care providers (52.8%) did not agree with the fact that caries-causing bacteria can be transmitted from mother to child [17] (Tab. III). Table IV shows the association between the type of health professional and oral health practices. Generally, the participants would assess the dental problem of the child (p = 0.05) and discuss the importance of tooth brushing with the mother (p = 0.03).
Tab. IV.
Association between type of health professional and oral health practices.
| Oral health practices When attending a child patient how likely are you to |
Very likely/likely (%) | Neutral/unlikely/very unlikely (%) | Sig. (2 - sided exact test) |
|---|---|---|---|
| Inquire about nocturnal bottle feeding | |||
| Nurses | 59 (30.7) | 96(50) | 0.09 |
| GP | 7 (3.7) | 11 (5.7) | |
| Paediatrician | 10 (5.2) | 5 (2.6) | |
| Family physician | 4 (2.1) | 0 (0) | |
| Total (n = 192) | 80 (41.7) | 112 (58.3) | |
| Assess dental problems | |||
| Nurse | 98 (47.6) | 59 (28.6) | 0.05 |
| GP | 11 (5.3) | 6 (2.9) | |
| Paediatrician | 13 (6.4) | 10 (4.9) | |
| Family physician | 4 (1.9) | 5 (2.4) | |
| Total (n = 206) | 126 (61.2) | 80 (38.8) | |
| Discuss importance of tooth brushing with mother | |||
| Nurse | 114 (55.9) | 40 (19.6) | 0.03 |
| GP | 11 (5.4) | 7 (3.4) | |
| Paediatrician | 17 (8.3) | 6 (2.9) | |
| Family physician | 7 (3.4) | 2 (1.0) | |
| Total (n = 204) | 149 (73.0) | 55 (26.9) | |
| Assess child’s fluoride intake | |||
| Nurse | 60(30) | 91 (45.5) | 0.04 |
| GP | 6(3) | 11 (5.5) | |
| Paediatrician | 8(4) | 15 (7.5) | |
| Family physician | 0 (0) | 9 (4.5) | |
| Total (n = 200) | 74(37) | 126(63) | |
| Inquire about mother’s dental health | |||
| Nurse | 76 (37.3) | 78 (38.2) | 0.23 |
| GP | 8 (3.9) | 10 (4.9) | |
| Paediatrician | 5 (2.5) | 18 (8.8) | |
| Family physician | 0 (0) | 9 (4.4) | |
| Total (n = 204) | 89 (43.7) | 115 (56.4) | |
A significant number of respondents (p = 0.04) were unlikely to assess the children’s fluoride intake [18]. Further, there was a significant difference in the group of participants that would examine the child’s teeth (p = 0.01) and counsel the mothers on prevention of dental problems (p = 0.01) (Tab. V). This group would also refer children to dentist at 12 months of age (p = 0.05).
Tab. V.
Association between type of health professionals and anticipatory guidance.
| Anticipatory guidance recommendations: To what extent do you agree the following should be part of well baby clinic routine care? |
Strongly agree/agree (%) | Neutral/disagree/strongly disagree (%) | Sig. (2 - sided exact test) |
|---|---|---|---|
| Dental examination | |||
| Nurse | 134 (63.8) | 27 (12.9) | 0.01 |
| GP | 15 (7.1) | 2 (1.0) | |
| Paediatrician | 20 (9.5) | 3 (1.4) | |
| Family physician | 9 (4.3) | 0 (0) | |
| Total (n = 210) | 178 (84.7) | 32 (15.3) | |
| Counseling mothers on prevention of dental problems | |||
| Nurse | 131 (61.8) | 31 (14.6) | 0.01 |
| GP | 17 (8.0) | 1 (0.5) | |
| Paediatrician | 20 (9.4) | 3 (1.4) | |
| Family physician | 9 (4.3) | 0 (0) | |
| Total (n = 212) | 177 (83.5) | 35 (16.5) | |
| Applying topical fluoride varnish | |||
| Nurse | 77 (38.3) | 76 (37.8) | 0.37 |
| GP | 6 (3.0) | 10 (5.0) | |
| Paediatrician | 15 (7.5) | 8 (4.0) | |
| Family Physician | 4 (2.0) | 5 (2.5) | |
| Total (n = 201) | 102 (50.8) | 99 (49.2) | |
| Referring children to dentist at 12 months of age | |||
| Nurse | 102 (51.9) | 51 (24.3) | 0.05 |
| GP | 10 (4.7) | 8 (3.8) | |
| Paediatrician | 13 (6.2) | 10 (4.7) | |
| Family physician | 6 (2.9) | 3 (1.4) | |
| Total (n = 210) | 138 (65.7) | 72 (34.3) | |
Medical professionals with more than 10 years of experience were willing to assess children’s’ dental problems (p = 0.05) and counsel mothers on prevention of dental problems (p = 0.04) compared to those professionals with less than 10 years of experience. Also, these individuals with more than 10 years of experience were likely to apply topical fluoride varnish for children (recommended every 3-6 months [19, 20]) (p = 0.05) and refer them to dentists at 12 months of age (p = 0.04) (Tab. VI).
Tab. VI.
Distribution of responses by medical professionals to oral health recommendations based on years of practice.
| “Strongly agree” or “agree” the following to be a part of WBC routine care for children | Number of years in practice | Chi–square test | ||
|---|---|---|---|---|
| 1-5 | 6-10 | > 10 | ||
| Assessing children’s dental problems | ||||
| Nurse | 20 | 41 | 96 | 0.05 |
| GP | 0 | 5 | 12 | |
| Pediatrician | 2 | 2 | 19 | |
| Family physician | 0 | 3 | 6 | |
| Total (n = 206) | 22 | 51 | 133 | |
| Counseling mothers on prevention of dental problems | ||||
| Nurse | 21 | 41 | 100 | 0.04 |
| GP | 0 | 6 | 12 | |
| Pediatrician | 2 | 2 | 19 | |
| Family physician | 0 | 3 | 6 | |
| Total (n = 212) | 23 | 52 | 137 | |
| Applying topical fluoride varnish | ||||
| Nurse | 20 | 39 | 94 | 0.05 |
| GP | 0 | 7 | 9 | |
| Pediatrician | 2 | 2 | 19 | |
| Family physician | 0 | 3 | 6 | |
| Total (n = 201) | 22 | 51 | 127 | |
| Referring children to dentist at 12 months of age | ||||
| Nurse | 20 | 41 | 99 | 0.04 |
| GP | 0 | 6 | 12 | |
| Pediatrician | 2 | 2 | 19 | |
| Family physician | 0 | 3 | 6 | |
| Total (n = 210) | 22 | 52 | 136 | |
Discussion
The results of this study revealed interesting insights. As far as it could be ascertained, this was the first study to assess the knowledge, attitudes and practices of primary health care providers towards oral health of preschool children in Qatar. Health professionals believed that they have an important role in oral health promotion and many were likely to include some anticipatory guidance. The majority of participants in this study were nurses and it demonstrates their willingness to participate in health related surveys. Another possible explanation for this finding could be the fact that during the second phase of data collection the head nurse of each health centre was assigned the task of receiving the questionnaires via the central mailing system. This may have prompted other subordinate nursing staff to respond to the questionnaire.
It is difficult to identify a cause-effect relationship in studies which utilize self-administered questionnaire for gathering health related information [20, 21]. Nevertheless, all efforts were made to address this issue by maximizing confidentiality during data collection. Moreover, this method of data collection has been adapted and tested previously and has demonstrated adequate reliability [10, 12].
A very small number of participants in the study had received oral health related training during their under graduate programme. Further, for a majority of them, the training only included one or two lectures on oral health. This finding reflects in the fact that more than half of the participants incorrectly responded to a basic fact on oral health that “caries-causing bacteria” can be transmitted from mother to child. Interestingly, these practitioners usually gave oral health recommendations to the parents of their preschoolers. Other studies have reported similar findings where health professionals including pediatricians have received little to no formal training on oral health education, yet, most of them provide oral health recommendations to the parents and their children [22, 23].
Health practitioners with limited knowledge of oral health should be cautious while providing oral health recommendations. Providing incorrect or improper oral health advice to parents may inadvertently cause poor oral health of children. However, there are initiatives taken in this regards and reports suggest that pediatricians and other health care professionals now receive relevant training in oral health. A study conducted on Flemish pediatricians in 2008 revealed that 71% of the participants had education on dental topics [24]. In the USA, increased attention has been given to oral health education and many pediatric boards in the country now require candidates to successfully complete an oral health education component before receiving certification [25]. In the present study, though, only 20.1% of health professionals received further oral health training after graduation. Besides, more than half of them relied on general information from media to update themselves on oral health knowledge. It is beyond the scope of this investigation to compare and contrast the different university courses across various medical specialties and sub-specialties. However, one proposition would be to include a mandatory component on oral health education by relevant medical board authorities in the form of workshops, seminars and conferences before health care practitioners can renew their practicing licenses.
A large number of practitioners assessed the dental problems of children and a significant number of them discussed the importance of tooth brushing with the mothers as well as counsel them on prevention of dental problems including those before teeth erupt. This finding was consistent across all professions including nurse, GPs, pediatricians and family physicians and is a clear indication that these professionals regard tooth brushing as one of the most critical factors essential for maintaining oral hygiene. Occasionally, both parents would attend WBCs and when present, fathers would also be given counseling. However, majority of respondents failed to inquire about the nocturnal feeding habits and about mother’s dental health.
Routinely, pediatricians have taken responsibility to assess a child’s fluoride intake [10]. However, in the current study, a significantly lower number of pediatricians would assess the fluoride intake of children. This finding was also reported across nurses, GPs and family physicians. Though it was not the objective of the study to explore the causes of this finding, one possible explanation for this result could be that healthcare workers may be under the presumption that children residing in Qatar consume water which has adequate amounts of fluoride [26].
Limited knowledge and lack of familiarity with oral health related issues seems to be the most important barrier to greater involvement in oral health promotion by medical professionals [22, 23, 25]. In the present study, only 35.7% of participants received some form of oral health training during their under graduate training. Furthermore, only 20.1% had received any form of oral health training after graduation. Similar figures have been reported across the world where medical professionals receive minimal to no training on oral health related subjects including countries like the United Kingdom [23], Norway [27] and Iran [28].
Also, studies from Sweden [29], Spain [30] and USA [31] have indicated that health care professionals at the primary level are inclined to provide preventive treatment but they face severe constraint in the form of limited time and resources due to an overload of curative care. These findings are concurrent with the results of the current study where health professionals were amenable to provide anticipatory guidance in the form of counseling mothers on prevention of dental problems and examining the children’s oral cavity. Also, a significantly large number of professionals strongly agreed to refer children to dentist at 12 months of age. However, only half of the respondents were willing to apply topical fluoride varnish to children.
The number of years of clinical practice of health professionals had a positive impact on their inclination to provide oral health recommendations. Health professionals with more than 10 years of experience were not only willing to assess children’s oral health status and counsel mothers on prevention of dental problems but also had a propensity to apply topical fluoride varnish and refer children to dentist at 12 months of age. Similar results have been observed in studies elsewhere where health providers with greater experience were more likely to engage in practice addressing the oral health of their patients [11, 32, 33]. In the present study, the mean number of years all respondents had been working in the WBCs was 7 (± 4.3) years. This reflects a reasonable experience in dealing with preschool children and explains the favorable response of these health care workers to oral health practices.
The ethnic diversity of the population in Qatar may provide some explanation for the contrasting findings of this study. The majority of the population in Qatar includes citizens from India, Nepal, Bangladesh, Philippines, Egypt, Pakistan and other south Asian and north and central African countries. The local Qataris are a minority since decades [34]. A similar diversity is reflected among professionals working in the healthcare sector where people from different environments make up the group of healthcare providers. This diversity suggests different educational, cultural and linguistic backgrounds. It has been suggested that healthcare providers are discouraged while working with health promotion due to lack of adherence by the patients and also language difficulties. Healthcare professionals may not be inclined to discuss health promotion/ preventive regimes with patients because of these language barriers and due to paucity of adequate knowledge and information on oral health [16]. Nevertheless, it has been demonstrated that it is possible to employ staff from a wide range of specialties and different levels of education to deliver interventions targeting oral health promotion successfully [12].
The widespread neglect of oral health of preschool children in Qatar has been well documented [15]. Number of reasons have been cited for the high caries prevalence rate including high consumption of refined sugars, ineffective fluoridation policy and absence of oral health awareness among parents [15, 24]. This scenario and the findings from the current study make it imperative to introduce concrete and effective preventive programmes particularly at the Primary Health Care level. Various opportunities to deliver such programmes exist in the primary health care system and the results of this study clearly indicate that the health care providers are willing to support this cause. However, accurate oral health education and precise training of the health providers need to be undertaken to successfully execute these measures.
In spite of the straightforward methodological approach to determine the knowledge, attitudes and practices of primary health care providers, the study has certain limitations. The first phase of the study had a poor response rate and hence the questionnaires were re-sent in the second phase. Although speculative, this could imply that less participants responded in the first phase since many of them were unaware of the information sought via the survey. Regardless, resending the questionnaire to the head nurses in the second phase would have strained them to acquire more participants in the second phase who consequently may have responded to the questionnaire passively. Besides, this approach may have inadvertently introduced a bais in the study as more nurses responded in the second phase. Furthermore, no attempt was made to explain the questions to the respondents if they had any query and hence some questions were left unanswered by the participants. Nevertheless, the large sample size and the unequivocal results improve our understanding of the attitude and practices of primary health care providers.
Conclusions
Health professionals had a positive attitude towards the anticipatory guidance elements of oral health. However, the knowledge of healthcare professionals on childhood oral health is rather limited. More attention should be given to oral health education during training in pediatrics and other professions and a focused continued education plan is needed for these professionals who provide care for children to address the shortcomings in their oral health knowledge.
SIGNIFICANCE OF THE STUDY
The study explored the attitude of primary health care professionals towards oral health of children. It highlights the lack of adequate proficiency and up-to-date information of these professionals on oral health and hygiene. Further, it emphasizes that harbouring a positive attitude towards oral health is insufficient and intensive training and continuing education programmes are needed to address the issue.
Figures and tables
Acknowledgements
Funding sources: this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Appendix 1
Footnotes
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
AA conceived the experiment design, performed the survey, was involved in data collection, data analayisis and interpretation; and drafted the article. MTS was involved in the study design and in composing the preliminary draft of the article. LB Messer supervised the project and provided critical revision of the article. MP contributed substantially to the design of the study and data analysis. MM supervised the project. AS provided critical revision of the article and contributed to data analaysis and interpretation and co-wrote the paper. All authors discussed the results and contributed to the final manuscript.
References
- [1].Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol 2003;31(Suppl 1):3-23. https://doi.org/10.1046/j.2003.com122.x 10.1046/j.2003.com122.x [DOI] [PubMed] [Google Scholar]
- [2].Li X, Kolltveit KM, Tronstad L, Olsen I. Systemic diseases caused by oral infection. Clin Microbiol Rev 2000;13:547-58. https://doi.org/10.1128/cmr.13.4.547-558-2000 10.1128/cmr.13.4.547-558-2000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Bahekar AA, Singh S, Saha S, Molnar J, Arora R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: a meta-analysis. Am Heart J 2007;154:830-7. https://doi.org/10.1016/j.ahj.2007.06.037 10.1016/j.ahj.2007.06.037 [DOI] [PubMed] [Google Scholar]
- [4].Roleder J, Wilczyńska-Borawska M, Nowosielski C, Malyszko J. Interdisciplinary nature of oral diseases - clinical implications. Przegl Lek 2016;73:233-7. [PubMed] [Google Scholar]
- [5].Meurman JH, Sanz M, Janket SJ. Oral health, atherosclerosis, and cardiovascular disease. Crit Rev Oral Biol Med 2004;15:403-13. https://doi.org/10.1177/154411130401500606 10.1177/154411130401500606 [DOI] [PubMed] [Google Scholar]
- [6].Gil-Montoya JA, de Mello AL, Barrios R, Gonzalez-Moles MA, Bravo M. Oral health in the elderly patient and its impact on general well-being: a nonsystematic review. Clin Interv Aging 2015;10:461-7. https://doi.org/10.2147/CIA.S54630 10.2147/CIA.S54630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Bourgeois DM, Llodra JC. Global burden of dental condition among children in nine countries participating in an international oral health promotion programme, 2012-2013. Int Dent J 2014;64:27-34. https://doi.org/10.1111/idj.12129 10.1111/idj.12129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Javed F, Feng C, Kopycka-Kedzierawski DT. Incidence of early childhood caries: A systematic review and meta-analysis. J Investig Clin Dent 201;8:1-6. https://doi.org/10.1111/jicd.12238 10.1111/jicd.12238 [DOI] [PubMed] [Google Scholar]
- [9].Rajendra Santosh AB, Ogle OE, Williams D, Woodbine EF. Epidemiology of oral and maxillofacial infections. Dent Clin North Am 2017;61:217-33. https://doi.org/10.1016/j.cden.2016.11.003 10.1016/j.cden.2016.11.003 [DOI] [PubMed] [Google Scholar]
- [10].Lewis CW, Grossman DC, Domoto PK, Deyo RA. The role of pediatrician in the oral health of children: a national survey. Pediatrics 2000;106:e84 https://doi.org/10.1542/peds.106.6.e84 10.1542/peds.106.6.e84 [DOI] [PubMed] [Google Scholar]
- [11].Di Giuseppe G, Nobile CGA, Marinelli A, Angelillo IF. Knowledge, attitude and practices of pediatricians regarding the prevention of oral diseases in Italy. BMC Public Health 2006;6:176-83. https://doi.org/10.1186/1471-2458-6-176 10.1186/1471-2458-6-176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Abou El Fadl R, Blair M, Hassounah S. Integrating maternal and children’s oral health promotion into nursing and midwifery practice - a systematic review. PLoS One 2016;11:e0166760 https://doi.org/10.1371/journal.pone.0166760 10.1371/journal.pone.0166760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal healthcare in 195 countries and territories, 1990-2005: a novel analysis from the Global Burden of Disease Study 2015. Lancet 2017;390:231-66. https://doi.org/10.1016/S0140-6736(17)30818-8 10.1016/S0140-6736(17)30818-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Cheema S, Maisonneuve P, Al-Thani MH, Al-Thani AAM, Abraham A, Al-Mannai GA, et al. Oral health behavior and factors associated with poor oral status in Qatar: results from a national health survey. J Public Health Dent 2017;77:308-16. https://doi.org/10.1111/jhpd.12209 10.1111/jhpd.12209 [DOI] [PubMed] [Google Scholar]
- [15].Alkhtib A, Ghanim A, Temple-Smith M, Messer LB, Pirotta M, Morgan M. Prevelance of early childhood caries and enamel defects in four and five year-year old Qatari preschool children. BMC Oral Health 2016;16:73 https://doi.org/10.1186/s12903-016-0267-z 10.1186/s12903-016-0267-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Gold J. Streptococcus mutans is vertically transmitted from mother to child. J Evid Based Dent Pract 2015;15:53-4. https://doi.org/10.1016/j.jebdp.2015.03.002 10.1016/j.jebdp.2015.03.002 [DOI] [PubMed] [Google Scholar]
- [17].Heilman JR, Kiritsy MC, Levy SM, Wefel JS. Fluoride concentrations of infant foods. J Am Dent Assoc 1997;128:857-63. https://doi.org/10.14219/jada.archive.1997.0335 10.14219/jada.archive.1997.0335 [DOI] [PubMed] [Google Scholar]
- [18].Abreu-Placeres N, Garrido LE, Castillo Jáquez I, Féliz-Matos LE. Does applying fluoride varnish every three months better prevent caries lesions in erupting first permanent molars? A randomized clinical trial. Oral Health Prev Dent 2019;17:541-6. https://doi.org/10.3290/j.ohpd.a43566 10.3290/j.ohpd.a43566 [DOI] [PubMed] [Google Scholar]
- [19].Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev 2013;11:CD002279 https://doi.org/10.1002/14651858.CD002279.pub2 10.1002/14651858.CD002279.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Burt BA. How useful are cross-sectionals data from surveys of dental caries? Community Dent Oral Epidemiol 1997;25:36-41. https://doi.org/10.1111/j.1600-0528.1997.tb00897.x 10.1111/j.1600-0528.1997.tb00897.x [DOI] [PubMed] [Google Scholar]
- [21].Mota A, Oswal KC, Sajnani DA, Sajnani AK. Oral health knowledge, attitude and approaches of pre-primary and primary school teachers in Mumbai, India. Scientifica 2016;5967427 https://doi.org/10.1155/2016/5967427 10.1155/2016/5967427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Sánchez OM, Childers NK, Fox L, Bradley E. Physician’s view on pediatric preventive dental care. Pediatr Dent 1997;19:377-83. [PubMed] [Google Scholar]
- [23].Kalkani M, Ashley P. The role of pediatricians in oral health of preschool children in the United Kingdom: a national survey of pediatric postgraduate specialty trainees. Eur Arch Paediatr Dent 2013;14:319-24. https://doi.org/10.1007/s40368-013-0087-7 10.1007/s40368-013-0087-7 [DOI] [PubMed] [Google Scholar]
- [24].Bottenberg P, Van Melckebeke L, Louckx F, Vandenplas Y. Knowledge of Flemish pediatricians about children’s oral health - results of a survey. Acta Paediatr 2008;97:959-63. https://doi.org/10.1111/j.1651-2227.2008.00827.x 10.1111/j.1651-2227.2008.00827.x [DOI] [PubMed] [Google Scholar]
- [25].Lewis CW, Boulter S, Keels MA, Krol DM, Mouradian WE, O’Connor KG, Quinonez RB. Oral health and pediatricians: results of a national survey. Acad Pediatr 2009;9:457-61. https://doi.org/10.1016/j.acap.2009.09.016 10.1016/j.acap.2009.09.016 [DOI] [PubMed] [Google Scholar]
- [26].Almulla HI, King NM, Alnsour HM, Sajnani AK. Fluoride content of bottled drinking waters in Qatar. Biol Trace Elem Res 2016;174:471-6. https://doi.org/10.1007/s12011-016-0718-z 10.1007/s12011-016-0718-z [DOI] [PubMed] [Google Scholar]
- [27].Wooten KT, Lee J, Jared H, Boggess K, Wilder RS. Nurse practitioners and certified nurse midwives’ knowledge, opinions and practice behaviors regarding periodontal disease and adverse pregnancy outcomes. J Dent Hyg 2011;85:122-31 [PubMed] [Google Scholar]
- [28].Golkari A, Khosropanah H, Saadati F. Evaluation of knowledge and practice behaviors of a group of Iranian obstetricians, general practitioners, and midwives, regarding periodontal disease and its effect on the pregnancy outcome. J Public Health Res 2013;2:e15 https://doi.org/10.4081/jphr.2013.e15ì 10.4081/jphr.2013.e15i [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Carlfjord S, Lindberg M, Andersson A. Staff perceptions of addressing lifestyle in primary health care: a qualitative evaluation 2 years after the introduction of a lifestyle intervention tool. BMC Fam Pract 2012;13:99 https://doi.org/10.1186/1471-2296-13-99 10.1186/1471-2296-13-99 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Calderón C, Balaqué L, Cortada JM, Sánchez A. Health promotion in primary care: how should we intervene? A qualitative study involving both physicians and patients. BMC Health Serv Res 2011;11:62 https://doi.org/10.1186/1472-6963-11-62 10.1186/1472-6963-11-62 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Galuska DA, Fulton JE, Powell KE, Burgeson CR, Pratt M, Elster A, Griesemer BA. Pediatrician counseling about preventive health topics: results from the Physicians’ practices survey, 1998-1999. Pediatrics 2002;109:e83 https://doi.org/10.1542/peds.109.5.e83 10.1542/peds.109.5.e83 [DOI] [PubMed] [Google Scholar]
- [32].Walid EI, Nasir F, Naidoo S. Oral health knowledge, attitudes and behavior among nursing staff in Lesotho. SADJ 2004;59:288-92. [PubMed] [Google Scholar]
- [33].George A, Dahlen HG, Reath J, Ajwani S, Bhole S, Korda A, Chok HN, Miranda C, Villarosa A, Johnson M. What do antenatal care providers understand and do about oral health care during pregnancy: a cross-sectional survey in New South Wales, Australia. BMC Pregnancy Childbirth 2016;16:382 https://doi.org/10.1186/s12884-016-1163-x 10.1186/s12884-016-1163-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Ministry of Development Planning and Statistics 2017. http://www.mdps.gov.qa/en/statistics1/pages/topicslisting.aspx?parent=Population&child=Population (accessed on July 15, 2017).
- [35].Parker WA, Steyn NP, Levitt NS, Lombard CJ. They think they know but do they? Misalignment of perceptions of lifestyle modification knowledge among health professionals. Public Health Nutr 2011;14:1429-38. https://doi.org/10.1017/S1368980009993272 10.1017/S1368980009993272 [DOI] [PubMed] [Google Scholar]