

Key Points
Question
Does data-driven phenotyping based on the trajectories of organ dysfunction in the acute phase of critical illness among children with multiple organ dysfunction syndrome uncover phenotypes with prognostic and therapeutic relevance?
Findings
In this 2-center cohort study of 20 827 pediatric intensive care encounters, a data-driven approach to phenotyping patients with multiple organ dysfunction syndrome using the trajectories of 6 organ dysfunctions uncovered 4 reproducible and distinct phenotypes with prognostic and potential therapeutic relevance.
Meaning
In this study, data-driven phenotyping based on the type, severity, and trajectory of 6 organ dysfunctions showed promising results in critically ill children with multiple organ dysfunction syndrome.
This cohort study determines whether data-driven phenotypes of MODS based on the trajectory of 6 organ dysfunctions have prognostic and therapeutic relevance in critically ill children.
Abstract
Importance
Multiple organ dysfunction syndrome (MODS) is a dynamic and heterogeneous process associated with high morbidity and mortality in critically ill children.
Objective
To determine whether data-driven phenotypes of MODS based on the trajectories of 6 organ dysfunctions have prognostic and therapeutic relevance in critically ill children.
Design, Setting, and Participants
This cohort study included 20 827 pediatric intensive care encounters among 14 285 children admitted to 2 large academic pediatric intensive care units (PICUs) between January 2010 and August 2016. Patients were excluded if they were older than 21 years or had undergone cardiac surgery. The 6 subscores of the pediatric Sequential Organ Failure Assessment (pSOFA) score were calculated for the first 3 days, including the subscores for respiratory, cardiovascular, coagulation, hepatic, neurologic, and renal dysfunctions. MODS was defined as a pSOFA subscore of at least 2 in at least 2 organs. Encounters were split in a 80:20 ratio for derivation and validation, respectively. The trajectories of the 6 subscores were used to derive a set of data-driven phenotypes of MODS using subgraph-augmented nonnegative matrix factorization in the derivation set. Data analysis was conducted from March to October 2019.
Exposures
The primary exposure was phenotype membership. In the subset of patients with vasoactive-dependent shock, the interaction between hydrocortisone and phenotype membership and its association with outcomes were examined in a matched cohort.
Main Outcomes and Measures
The primary outcome was in-hospital mortality. Secondary outcomes included persistent MODS on day 7, and vasoactive-free, ventilator-free, and hospital-free days. Regression analysis was used to adjust for age, severity of illness, immunocompromised status, and study site.
Results
There were 14 285 patients with 20 827 encounters (median [interquartile range] age 5.2 years [1.5-12.7] years; 11 409 [54.8%; 95% CI, 54.1%-55.5%] male patients). Of these, 5297 encounters (25.4%; 95% CI, 24.8%-26.0%) were with patients who had MODS, of which 5054 (95.4%) met the subgraph count threshold and were included in the analysis. Subgraph augmented nonnegative matrix factorization uncovered 4 data-driven phenotypes of MODS, characterized by a combination of neurologic, respiratory, coagulation, and cardiovascular dysfunction, as follows: phenotype 1, severe, persistent encephalopathy (1019 patients [19.2%]); phenotype 2, moderate, resolving hypoxemia (1828 patients [34.5%]); phenotype 3, severe, persistent hypoxemia and shock (1012 patients [19.1%]); and phenotype 4, moderate, persistent thrombocytopenia and shock (1195 patients [22.6%]). These phenotypes were reproducible in a validation set of encounters, had distinct clinical characteristics, and were independently associated with outcomes. For example, using phenotype 2 as reference, the adjusted hazard ratios (aHRs) for death by 28 days were as follows: phenotype 1, aHR of 3.0 (IQR, 2.1-4.3); phenotype 3, aHR of 2.8 (IQR, 2.0-4.1); and phenotype 4, aHR of 1.8 (IQR, 1.2-2.6). Interaction analysis in a matched cohort of patients with vasoactive-dependent shock revealed that hydrocortisone had differential treatment association with vasoactive-free days across phenotypes. For example, patients in phenotype 3 who received hydrocortisone had more vasoactive-free days than those who did not (23 days vs 18 days; P for interaction < .001), whereas patients in other phenotypes who received hydrocortisone either had no difference or had less vasoactive-free days.
Conclusions and Relevance
In this study, data-driven phenotyping in critically ill children with MODS uncovered 4 distinct and reproducible phenotypes with prognostic relevance and possible therapeutic relevance. Further validation and characterization of these phenotypes is warranted.
Introduction
The development of multiple organ dysfunction syndrome (MODS) is a common final pathway for death among critically ill children.1 Even among survivors, children with more severe organ dysfunction are at higher risk of developing long-term morbidity after critical illness.2 Approximately one-third of children admitted to a pediatric intensive care unit (PICU) have MODS on presentation or develop it during their illnesses, so moderating the burden of MODS could significantly affect the outcomes of critically ill children.1,3,4,5
MODS can develop after many types of injury, but sepsis, trauma, and major surgery are the most common etiologies in the PICU.1,6,7 The most frequently described shared mechanism of MODS pathophysiology is the development of dysregulated inflammation; however, decades of drug trials targeting mediators of inflammation have failed to show effectiveness in the reduction of the MODS burden associated with sepsis and trauma.7,8,9,10,11 One of the most likely explanations for this is that MODS is a complex, dynamic, and heterogeneous process with many different phenotypes, and no single strategy will be effective in all phenotypes of MODS.
In recent years, considerable emphasis has been placed on characterizing the phenotypes of heterogenous syndromes in critically ill patients.12,13,14,15,16,17 These phenotypes may have prognostic and therapeutic implications and form the basis for precision medicine in the critical care setting.18 The derivation of these different phenotypes has included data-driven approaches using gene expression data12,17 and clinical data14,15,16 as well as expert-based approaches using biomarkers and clinical data.13 In general, these approaches have used a single time (eg, initial presentation) to define the different phenotypes and have not investigated the dynamic patterns of illness, despite evidence that this may be important in phenotyping.19,20,21,22 Furthermore, a single snapshot approach does not account for the fact that patients may present to a critical care setting at different points in their illness and that organ dysfunctions tend to peak between days 1 and 3 of admission.23
In this study we aimed to derive, validate, and characterize novel phenotypes of MODS in critically ill children using a data-driven approach based on the type, severity, and trajectory of organ dysfunctions in the acute phase of critical illness. Furthermore, we aimed to determine whether these phenotypes had prognostic and therapeutic relevance.
Methods
Study Design and Population
This was a retrospective cohort study of critically ill children admitted to 2 large, academic PICUs in Chicago, Illinois, between January 1, 2010, and August 31, 2016. Patients were excluded if they were older than 21 years or were recovering from cardiac surgery. Data were extracted from the 2 institutions’ data warehouses using structured queries and underwent quality checks for conformity, completeness, and plausibility. Data analysis was conducted from March to October 2019. The institutional review boards at the Ann and Robert H. Lurie Children’s Hospital of Chicago and The University of Chicago approved this study with a waiver of informed consent because of the retrospective nature of the analysis with minimal risk to patients. The reporting of this cohort study was performed using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.37
Organ dysfunction severity was measured using the subscores of the pediatric Sequential Organ Failure Assessment (pSOFA) score, which measures dysfunction for the respiratory, cardiovascular, coagulation, hepatic, neurologic, and renal systems on a scale from 0 to 4 for each system.24 Patients had the 6 pSOFA subscores calculated for each 24-hour period between PICU admission and day 3, which was considered the acute phase of critical illness.23 Individual pSOFA subscores were carried forward for as long as 24 hours if they were not remeasured; otherwise, missing variables were assumed to be normal and the corresponding subscore was assigned a 0.
Patients with MODS were defined as those with a pSOFA subscore of at least 2 in at least 2 organ systems within the first 3 days of admission. Severity of illness on admission was determined using the Pediatric Risk of Mortality (PRISM) III score using variables from the first 24 hours.25 Chronic comorbidities were based on the classification system developed by Feudtner et al.26 Patients with immunocompromised status were defined as those with an oncologic disease or transplant recipients. Patients who received antibiotics and microbiological cultures during the first 3 days were considered to have a confirmed or suspected infection. Each patient encounter was treated independently, but only the first PICU admission in a given hospitalization was included in the analysis.
Primary and Secondary Outcomes
The primary outcome was in-hospital mortality. The secondary outcomes included the presence of persistent MODS on day 7 after PICU admission (which included patients who died in the first week), and vasoactive-free, ventilator-free, and hospital-free days at 28 days after PICU admission.
Data-Driven Phenotyping
We used subgraph-augmented nonnegative matrix factorization to group patients with MODS into phenotypes based on the type, severity, and trajectory of each of the 6 pSOFA subscores in the first 3 days of PICU stay (Figure 1; eAppendix in the Supplement).21 Briefly, subgraph mining was used to extract the subgraphs representing the trajectory of individual organ dysfunctions.27 We then split the cohort of 5054 encounters with MODS and adequate subgraph counts into a derivation set (4044 encounters [80.0%]) and a validation set (1010 encounters [20.0%]). Nonnegative matrix factorization (NMF) was implemented on the patient-subgraph count matrix in the derivation set, which resulted in a patient-phenotype distribution matrix and a phenotype-subgraph mixture coefficient matrix.21,28 Patients in the derivation and validation set were then assigned phenotype membership based on the highest probability group in the mixture coefficient matrix. Patients assigned to each phenotype were then compared across the derivation and validation sets.
Figure 1. Data-Driven Phenotyping Using Subgraph Augmented Nonnegative Matrix Factorization.
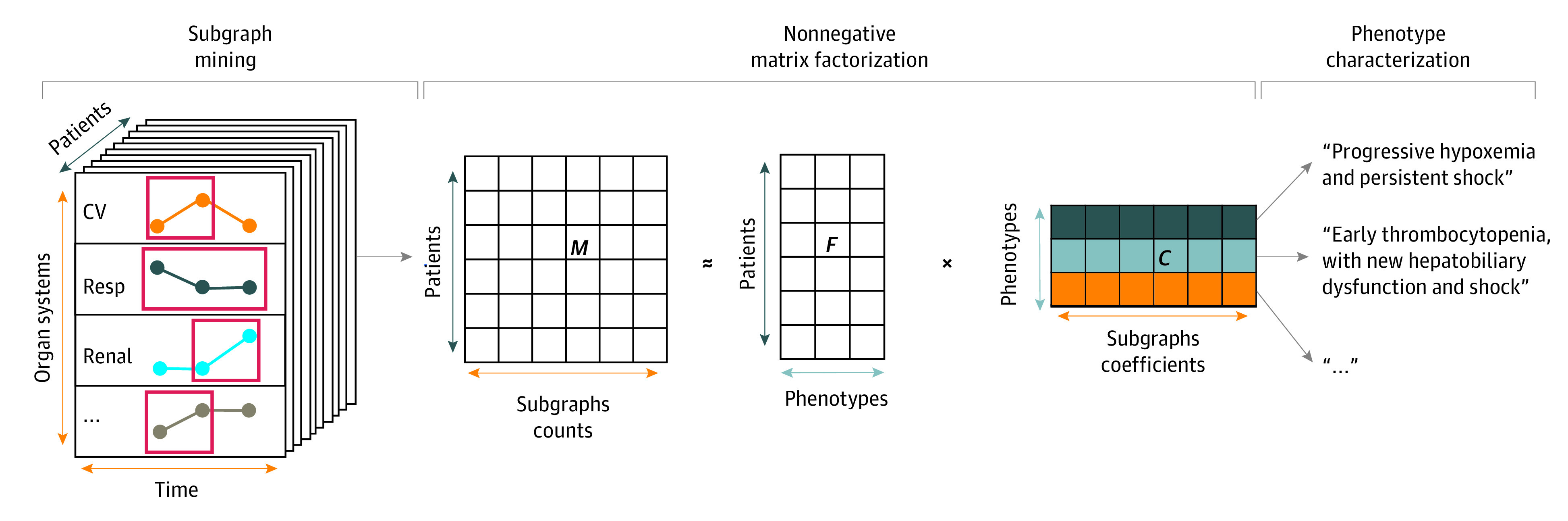
Subgraph mining extracts representative subgraphs from the trajectories of the 6 pediatric Sequential Organ Failure Assessment subscores in patients with MODS, which results in a matrix, M, of patient-subgraph counts. Nonnegative matrix factorization is used to derive a matrix, F, of hidden features (in this case the phenotypes), and a matrix of mixture coefficient C with the coefficients that compose the subgraph-based phenotypes. The factorization is done by iteratively updating F and C using the sparse nonnegative matrix factorization with sparseness in the left factor algorithm to gradually reduce the error between M and F × C. Once the nonnegative matrix factorization is completed, the final phenotypes can be characterized given the highly interpretable nature of the algorithm. Of note, the size of the matrices, number of groups, and the phenotype characterization examples here are used for illustration purposes only. CV indicates cardiovascular; resp, respiratory.
As a sensitivity analysis to determine external validity of the phenotypes, the same procedures were conducted using patients with MODS in the second hospital (PICU B) as the external validation set. Additional details can be found in the eAppendix in the Supplement.
Phenotype Characteristics and Clinical Relevance Evaluation
Clinical Characteristics of the MODS Phenotypes
The clinical characteristics of patients in each of the MODS phenotypes were compared across phenotypes. These included demographic characteristics, severity of illness, organ support, comorbidities, microbiologic and laboratory test results by day 3, and associated outcomes. The laboratory tests and summary measures included were based on those frequently used in prior pediatric organ dysfunction and severity of illness scores.3,25,29,30
Prognostic Relevance of the MODS Phenotypes
The prognostic relevance of the MODS phenotypes was tested by comparing the association of each phenotype with the outcomes of interest after adjusting for common confounders of PICU-related morbidity and mortality, including age, immunocompromised state, severity of illness on admission using the PRISM-III score, and study site.4,31 The phenotype with the lowest overall in-hospital mortality was used as reference. Additionally, the association of noncharacteristic organ dysfunctions and in-hospital mortality was analyzed in each of the phenotypes. Noncharacteristic organ dysfunctions were defined as those organ systems that were not used to characterize a specific phenotype and had a pSOFA subscore of at least 2 by day 3 of PICU stay.
Therapeutic Relevance of the MODS Phenotypes in Patients With Vasoactive-Dependent Shock
There are few organ dysfunction–specific treatments routinely used in patients with MODS. One exception is the use of intravenous (IV) hydrocortisone in patients with vasoactive-dependent shock. Hydrocortisone may contribute to hemodynamic stability through pleiotropic effects; however, mixed results in large randomized clinical trials among adults with septic shock have led to variable use among practitioners.32,33,34,35,36 Given that shock is a common feature of MODS, we tested the hypothesis that the heterogeneity of treatment effect of IV hydrocortisone in patients with vasoactive-dependent shock is in part explained by their phenotype. Vasoactive-dependent shock was defined as the use of dopamine greater than 5 µg/kg/min or any dose of epinephrine or norepinephrine infusions in patients with MODS. To balance the confounders across treatment groups, we first performed propensity score matching of patients based on the propensity to receive IV hydrocortisone, using age, immunocompromised state, PRISM-III score, study site, and phenotype membership as covariates. We then performed an interaction effect analysis for in-hospital mortality and vasoactive-free days, using phenotype membership, treatment group (ie, receiving ≥2 mg/kg/d of IV hydrocortisone or not), and their interaction as covariates to determine whether there was a differential treatment effect associated with phenotype membership. Additional details can be found in the eAppendix in the Supplement.
Statistical Analysis
Data were analyzed using R version 3.6.1 (R Project for Statistical Computing). Categorical variables were compared using the χ2 test and continuous variables using the Kruskal-Wallis test. Regression analysis was used to adjust for confounders when comparing outcomes. Logistic regression was used to compare binary outcomes, and Poisson regression was used to compare count outcomes. Survival analysis to 28 days was performed using Kaplan-Meier curves and adjusted Cox regression analysis. Statistical significance was set at P < .05, and all tests were 2-tailed.
Results
Study Population
There were 20 827 patient encounters among 14 285 unique patients in the 2 PICUs during the study period. The median (interquartile range [IQR]) age was 5.2 (1.5-12.7) years, and 11 409 (54.8%; 95% CI, 54.1%-55.5%) were male patients. A total of 5297 patients (25.4%; 95% CI, 24.8%-26.0%) met MODS criteria, and these patients had an associated in-hospital mortality of 449 (8.5%; 95% CI, 7.7%-9.3%). The clinical characteristics and outcomes of patients with and without MODS are presented in Table 1.
Table 1. Demographic and Clinical Characteristics of Patients With and Without MODS.
| Clinical variables | Patients, No. (%) | P value | |
|---|---|---|---|
| With MODS (n = 5297) | Without MODS (n = 15 530) | ||
| Age, median (IQR), y | 4.7 (1.0-12.6) | 5.4 (1.6-12.7) | <.001 |
| Male patients | 2898 (54.7) | 8511 (54.8) | .90 |
| Race/ethnicity | |||
| Non-Hispanic | <.001 | ||
| White | 1700 (32.1) | 4966 (32) | |
| Black | 1726 (32.6) | 5515 (35.5) | |
| Hispanic | 1342 (25.3) | 3650 (23.5) | |
| Other | 529 (10) | 1399 (9) | |
| PRISM-III score on admission, median (IQR) | 7 (4-13) | 0 (0-4) | <.001 |
| Vasoactives by day 3 | 1222 (23.1) | 84 (0.5) | <.001 |
| Mechanical ventilation by day 3 | 3883 (73.3) | 3108 (20) | <.001 |
| Immunocompromised state | 922 (17.4) | 1422 (9.2) | <.001 |
| Multiple chronic comorbidities | 3153 (59.5) | 5806 (37.3) | <.001 |
| Postoperative | 1286 (24.3) | 3679 (23.7) | .40 |
| Trauma | 200 (3.8) | 827 (5.3) | <.001 |
| Infection by day 3 | 3145 (59.4) | 4665 (30) | <.001 |
| Maximum pSOFA score by day 3, median (IQR) | 7 (6-9) | 2 (1-3) | <.001 |
| Maximum PELOD-2 score by day 3, median (IQR) | 7 (5-10) | 2 (2-4) | <.001 |
| MODS on day 7 | 1418 (26.8) | 124 (0.8) | <.001 |
| Length of stay, median (IQR), d | 9.1 (4.8-17.9) | 3.2 (1.8-5.9) | <.001 |
| In-hospital mortality | 449 (8.5) | 73 (0.5) | <.001 |
Abbreviations: IQR, interquartile range; MODS, multiple organ dysfunction syndrome; PRISM-III, Pediatric Risk of Mortality III; pSOFA, pediatric Sequential Organ Failure Assessment; PELOD-2, Pediatric Logistic Organ Dysfunction, version 2.
Data-Driven Phenotyping
After performing subgraph mining of the pSOFA subscore trajectories during the first 3 days among patients with MODS and eliminating redundant, rare, and nonrepresentative subgraphs based on the criteria described in the eAppendix in the Supplement, there were 145 representative subgraphs uncovered. A total of 243 patient encounters (4.6%) with MODS (with an in-hospital mortality of 3 [1.2%]) had none of these representative subgraphs and were therefore excluded from the remainder of the analysis, resulting in 5054 encounters (95.4%) with patients with MODS in the final cohort. Of the 145 subgraphs representing pSOFA subscore trajectories in these 5054 encounters, 31 (21.4%) represented worsening organ dysfunction, 24 (16.6%) represented moderate-to-severe organ dysfunction with no change, and 90 (62.1%) represented improvement in organ dysfunction.
Sparse NMF was performed in the derivation set (4044 encounters [80.0%]) using the counts of the 145 subgraphs as sole input. This uncovered 4 distinct phenotypes based on the changes in pSOFA subscore in the first 3 days. Phenotype membership was then assigned to patients in the entire cohort based on the highest probability group membership according to the mixture coefficient matrix. Patients in each phenotype were then compared across the derivation and validation sets. Within each of the 4 phenotypes, patients had similar distributions of pSOFA subscores on day 1 to day 3 (eTable 1 in the Supplement), laboratory test characteristics by day 3 (eTable 2 in the Supplement), and outcomes (eTable 3 in the Supplement).
In the sensitivity analysis using 3013 patient encounters (59.6%) in PICU A as derivation and 2041 patient encounters (40.4%) in PICU B as validation, again sparse NMF uncovered 4 phenotypes, which were consistent with those in the original analysis. The distributions of pSOFA subscores, laboratory test results, and outcomes were similar within phenotypes across the derivation patient encounters in PICU A and the external validation patient encounters in PICU B (eTable 4 in the Supplement). Patients within each phenotype from the original NMF were merged and used for the remainder of the analyses.
Characterization of the MODS Phenotypes
The most representative subgraphs for each phenotype were chosen from the mixture coefficient matrix of the NMF model, such that the selected subgraphs accounted for at least 75% of the phenotype group coefficients. The 10 most representative subgraphs for each of the 4 MODS phenotypes and the relative weight of each organ dysfunction subscore in the first 3 days, stratified by phenotype, appear in Figure 2 and eFigure 1 in the Supplement. These representative subgraphs were used to characterize the phenotypes based on the most distinctive characteristics, using the organ dysfunction type, severity, and trajectory in the first 3 days of PICU stay. Based on this, the 4 MODS phenotypes were characterized as follows: phenotype 1, severe, persistent encephalopathy (1019 patients [19.2%]); phenotype 2, moderate, resolving hypoxemia (1828 patients [34.5%]); phenotype 3: severe, persistent hypoxemia and shock (1012 patients [19.1%]); and phenotype 4, moderate, persistent thrombocytopenia and shock (1195 patients [22.6%])
Figure 2. Common Subgraphs in Each of the 4 Data-Driven MODS Phenotypes.

The most common subgraphs in each phenotype and the proportion of patients who had each of them.
The clinical characteristics and associated outcomes of patients in each of the 4 MODS phenotypes are presented in Table 2. When compared across age groups, the distribution and outcomes associated with the 4 MODS phenotypes remained consistent (eTable 5 in the Supplement).
Table 2. Demographic and Clinical Characteristics and Outcomes of the 4 MODS Phenotypes.
| Clinical variable | No. (%) | P value | |||
|---|---|---|---|---|---|
| Phenotype 1, severe, persistent encephalopathy (n = 1019) | Phenotype 2, moderate, resolving hypoxemia (n = 1828) | Phenotype 3, severe, persistent hypoxemia and shock (n = 1012) | Phenotype 4, moderate, persistent thrombocytopenia and shock (n = 1195) | ||
| Age, median (IQR), y | 4.3 (1.0-12.0) | 3.9 (0.9-11.3) | 3.5 (0.8-11.3) | 8.1 (1.8-15.2) | <.001 |
| Male patients | 555 (54.5) | 989 (54.1) | 557 (55.0) | 671 (56.2) | .73 |
| Race/ethnicity | |||||
| Non-Hispanic | <.001 | ||||
| White | 311 (30.5) | 557 (30.5) | 319 (31.5) | 447 (37.4) | |
| Black | 410 (40.2) | 636 (34.8) | 318 (31.4) | 285 (23.8) | |
| Hispanic | 197 (19.3) | 453 (24.8) | 265 (26.2) | 353 (29.5) | |
| Other | 101 (9.9) | 182 (10) | 110 (10.9) | 110 (9.2) | |
| PRISM-III score on admission, median (IQR) | 8 (5-15) | 6 (2-10) | 10 (5-19) | 9 (5-13) | <.001 |
| Vasoactives by day 3 | 179 (17.6) | 107 (6) | 392 (38.7) | 542 (45.3) | <.001 |
| Mechanical ventilation by day 3 | 926 (91) | 1409 (77.1) | 880 (87) | 553 (46.3) | <.001 |
| Immunocompromised state | 105 (10.3) | 240 (13.1) | 154 (15.2) | 382 (32) | <.001 |
| Multiple chronic comorbidities | 607 (59.6) | 1043 (57.1) | 608 (60) | 760 (63.4) | .004 |
| Postoperative | 223 (21.9) | 527 (28.8) | 164 (16.2) | 307 (25.7) | <.001 |
| Trauma | 72 (7.1) | 55 (3) | 41 (4.1) | 30 (2.5) | <.001 |
| Infection by day 3 | 595 (58.4) | 953 (52.1) | 724 (71.5) | 755 (63.2) | <.001 |
| Primary site | |||||
| Bloodstream | 59 (5.8) | 117 (6.4) | 119 (11.2) | 193 (16.2) | <.001 |
| Respiratory | 334 (32.8) | 510 (27.9) | 385 (38) | 193 (16.2) | <.001 |
| Urinary | 66 (6.5) | 96 (5.3) | 62 (6.1) | 81 (6.8) | .32 |
| Other sites | 36 (3.5) | 60 (3.3) | 35 (3.5) | 45 (3.8) | .92 |
| Culture negative | 194 (19) | 308 (16.8) | 252 (24.9) | 328 (27.4) | <.001 |
| Microorganism | |||||
| Bacteria | |||||
| Gram positive | 133 (13.1) | 184 (10.1) | 159 (15.7) | 127 (10.6) | <.001 |
| Gram negative | 165 (16.2) | 224 (12.3) | 178 (17.6) | 137 (11.5) | <.001 |
| Other bacteria | 32 (3.1) | 50 (2.7) | 22 (2.2) | 39 (3.3) | .42 |
| Fungi | 12 (1.2) | 17 (0.9) | 18 (1.8) | 21 (1.8) | .14 |
| Viruses | 170 (16.7) | 333 (18.2) | 230 (22.7) | 184 (15.4) | <.001 |
| Laboratory results by day 3, median (IQR) | |||||
| Minimum white blood cell count, /μL | 7900 (5200-11 000) | 8300 (5600-11 600) | 7000 (3800-10 900) | 5900 (2500-9400) | <.001 |
| Minimum lymphocyte count, /μL | 1300 (700-2200) | 1300 (700-2300) | 1100 (500-2000) | 800 (300-1500) | <.001 |
| Maximum blood urea nitrogen, mg/dL | 12 (8-18) | 12 (8-18) | 14 (9-23) | 15 (10-28) | <.001 |
| Maximum creatinine, mg/dL | 0.4 (0.3-0.6) | 0.4 (0.2-0.6) | 0.4 (0.3-0.8) | 0.5 (0.3-0.9) | <.001 |
| Minimum albumin, g/dL | 3.1 (2.5-3.6) | 3.1 (2.6-3.7) | 2.7 (2.2-3.3) | 2.8 (2.3-3.4) | <.001 |
| Maximum aminotransferase, U/L | |||||
| Aspartate | 53 (31-147) | 49 (30-111) | 61 (34-201) | 62 (32-141) | <.001 |
| Alanine | 28 (18-17) | 27 (17-71) | 36 (19-122) | 37 (18-97) | <.001 |
| Maximum total bilirubin, mg/dL | 0.5 (0.3-1.2) | 0.5 (0.2-2.2) | 0.6 (0.3-1.5) | 1.2 (0.5-3.2) | <.001 |
| Minimum hemoglobin, g/dL | 9 (7.4-11) | 9.6 (7.8-11.3) | 8.8 (7.2-10.5) | 8.3 (7-10) | <.001 |
| Minimum platelet count, /μL | 185 000 (104 000-268 000) | 188 000 (94 000-270 000) | 156 000 (68 000-249 000) | 82 000 (27 000-179 000) | <.001 |
| Maximum international normalized ratio | 1.4 (1.2-1.7) | 1.3 (1.2-1.6) | 1.5 (1.2-2.1) | 1.4 (1.2-1.7) | <.001 |
| Maximum partial thromboplastin time, s | 35 (30-45) | 35 (30-44) | 40 (32-59) | 39 (31-54) | <.001 |
| Maximum lactate, mg/dL | 18.9 (10.8-35.1) | 14.4 (9.9-26.1) | 22.5 (12.6-52.2) | 18.0 (11.7-34.2) | <.001 |
| Outcomes | |||||
| Vasoactive-free days at 28 d, median (IQR) | 28 (27-28) | 28 (28-28) | 28 (24-28) | 27 (26-28) | <.001 |
| Ventilator-free days at 28 d, median (IQR) | 23 (13-26) | 26 (21-27) | 20 (6-26) | 27 (22-28) | <.001 |
| Hospital-free days at 28 d, median (IQR) | 16 (1-23) | 20 (12-24) | 12 (1-21) | 17 (4-22) | <.001 |
| Persistent MODS on day 7 | 320 (31.4) | 319 (17.5) | 448 (44.3) | 307 (25.7) | <.001 |
| In-hospital mortality | 116 (11.3) | 60 (3.3) | 176 (17.4) | 94 (7.9) | <.001 |
Abbreviations: IQR, interquartile range; MODS, multiple organ dysfunction syndrome; PRISM-III, Pediatric Risk of Mortality III.
SI conversion factors: To convert alanine aminotransferase and aspartate aminotransferase to microkatals per liter, multiply by 0.0167; albumin and hemoglobin to grams per liter, multiply by 10; blood urea nitrogen to millimoles per liter, multiply by 0.357; creatinine to micromoles per liter, multiply by 88.4; lymphocyte, platelet, and white blood cell count to ×109 per microliter, multiply by 0.001; and total bilirubin to millimoles per liter, multiply by 17.104.
Prognostic Relevance of the MODS Phenotypes
The outcomes associated with each of the 4 phenotypes after adjusting for confounders including age, immunocompromised state, PRISM-III score, and study site are presented in eTable 6 in the Supplement. After adjusting for the same confounders in Cox regression analysis and using phenotype 2, which had the lowest mortality as reference, the adjusted hazard ratios (aHRs) for death by 28 days were as follows: phenotype 1, aHR of 3.0 (IQR, 2.1-4.3); phenotype 3, aHR of 2.8 (IQR, 2.0-4.1); and phenotype 4, aHR of 1.8 (IQR, 1.2-2.6). The Kaplan-Meier survival curves for the 4 phenotypes are presented in eFigure 2 in the Supplement. The multivariable logistic regression analyses of the association of noncharacteristic organ dysfunctions and in-hospital mortality showed significant differences between phenotypes and are presented in eTable 7 in the Supplement.
Therapeutic Relevance of the MODS Phenotypes in Patients With Vasoactive-Dependent Shock
A total of 1220 of 5054 patient encounters (24.1%; 95% CI, 23.0%-25.3%) had vasoactive-dependent shock by day 3, with an associated in-hospital mortality of 299 patients (24.5% [95% CI, 22.1%-27%]). Of these, 342 (28.0%; 95% CI, 25.5%-30.6%) received IV hydrocortisone. Using propensity score matching, 330 treated patients were successfully matched 1:1 with 330 untreated patients using age, immunocompromised state, PRISM-III score, study site, and phenotype membership as covariates. The matched cohort demonstrated a balanced distribution of covariates, with absolute standardized mean difference of less than 0.1 (eFigure 3 in the Supplement). Interaction analysis in the matched cohort revealed that IV hydrocortisone had a differential treatment effect on vasoactive-free days across phenotypes, most notably with phenotype 3 having most benefit associated with treatment (23 vasoactive-free days in treated patients vs 18 vasoactive-free days in treated patients; P for interaction < .001). The interaction was not significant for in-hospital mortality (Table 3).
Table 3. Differences in Response to IV Hydrocortisone by Phenotype in a Propensity Score Matched Cohort of Patients With Vasoactive-Dependent Shock.
| Outcome | Phenotype 1 (n = 72) | Phenotype 2 (n = 71) | Phenotype 3 (n = 287) | Phenotype 4 (n = 230) | P valuea | ||||
|---|---|---|---|---|---|---|---|---|---|
| Treated (n = 39) | Untreated (n = 33) | Treated (n = 36) | Untreated (n = 35) | Treated (n = 146) | Untreated (n = 141) | Treated (n = 109) | Untreated (n = 121) | ||
| Vasoactive-free days, median (IQR) | 15 (0-25) | 17 (1-24) | 25 (23-26) | 24 (21-27) | 23 (1-26) | 18 (0-26) | 26 (23-27) | 26 (24-27) | <.001 |
| In-hospital mortality, No.(%) | 20 (51.3) | 14 (42.4) | 4 (11.1) | 4 (11.4) | 50 (34.2) | 65 (46.1) | 14 (12.8) | 9 (7) | .11 |
Abbreviations: IQR, interquartile range; IV, intravenous.
P value for interaction between IV hydrocortisone and phenotype membership using phenotype 2 as reference group (ie, 3 interaction terms) and analysis of deviance to test global significance.
Discussion
We derived and validated 4 novel, data-driven phenotypes of MODS in critically ill children based on organ dysfunction trajectories. These phenotypes have distinct clinical characteristics, are independently associated with outcomes, and have different sets of organ dysfunction–based risk factors for death. In a subset of patients with vasoactive-dependent shock who were matched based on the propensity to receive IV hydrocortisone, treatment was associated with a difference in vasoactive-free days across phenotypes, suggesting that these phenotypes may be associated with differences in response to therapy.
Our findings share similarities with previously described data-driven phenotypes of sepsis and sepsis-induced MODS, particularly phenotypes 3 and 4, which were the MODS phenotypes most frequently associated with infections in our cohort. Phenotype 3 shares similarities with the “shock with hypoxemia and altered mental status” phenotype described by Knox et al15 and the γ phenotype described by Seymour et al14 in adult patients, especially in terms of hypoxemia, vasoactive-dependence, low albumin levels, and high mortality. Phenotype 4 shares similarities with the hepatic disease phenotype described by Knox et al15 and the δ phenotype described by Seymour et al,14 particularly in terms of the thrombocytopenia, hepatobiliary dysfunction, and shock as well as the relatively preserved pulmonary function. To our knowledge, our study is the first to use a data-driven approach to derive MODS phenotypes in critically ill children. Further biomarker and molecular endotyping analyses will be needed to compare our phenotypes with other previously described clinical phenotypes and endotypes in pediatric and adult patients.12,13,17
The association of IV hydrocortisone administration with differential treatment effect on vasoactive-free days in patients with vasoactive-dependent shock, particularly in phenotype 3, could partially be explained by the enrichment with patients suffering severe hypoxemia, severe shock, and infections. Prior randomized clinical trials and secondary analyses of trial data have found that the use of hydrocortisone was associated with improved outcomes in patients with sepsis-associated acute respiratory distress syndrome.38,39 However, our results should be interpreted with caution because they are part of an interaction effect analysis on a propensity score matched cohort. The standard approach is to perform an interaction effects analysis across subgroups with a treatment assignment that has been randomized to ensure a better balance of all possible confounders.16 Given the selection bias inherent in observational data, we used propensity score matching to balance observed covariates, but it is likely that we did not account for all possible confounders. Therefore, these results require further validation and are only hypothesis generating at this point.
Our data-driven phenotyping approach to MODS has several important implications. We describe a broad stratification of patients that can be readily performed using widely available electronic health record data and that appears to have prognostic relevance and, potentially, therapeutic value. It is likely that many of the patients within each phenotype share many of the same underlying pathophysiological disturbances and dysregulated host responses, as evidenced by the shared clinical characteristics and laboratory test results. Understanding the common features of these underlying pathophysiologies could help determine which interventions may be most beneficial to individual patients, regardless of the etiology of MODS and beyond the traditional boundaries of syndromes like sepsis or acute respiratory distress syndrome. For example, cardiovascular dysfunction is associated with the most detrimental outcomes in patients with severe encephalopathy in phenotype 1, suggesting that targeted blood pressure management and close cerebral perfusion monitoring, as recommended for patients with traumatic brain injury, may be warranted in patients with this phenotype even if most do not have traumatic brain injury.40 Similarly, renal dysfunction seems to most negatively affect patients in phenotype 3 who suffer severe hypoxemia and shock, indicating that careful fluid management and nephrotoxin avoidance might be most beneficial in this group of patients. In addition, further endotyping and molecular characterization of these broad phenotypes may uncover relevant MODS subphenotypes that may benefit from novel targeted interventions, including immunomodulatory strategies.41,42,43 Furthermore, the molecular characterization of these phenotypes may help in the task of assigning phenotype membership shortly after patients are admitted, which would make this phenotyping schema more clinically actionable in the critical care setting. In short, data-driven phenotyping may help develop precision medicine strategies that can reduce the mortality and morbidity associated with MODS, but further investigation into the value of this phenotyping approach in research and clinical care is warranted.18
Limitations
Our findings are subject to several limitations. First, the data for this study were collected retrospectively from 2 academic PICUs in the same city, limiting the generalizability of our findings. Second, our data-driven phenotyping approach was intentionally sparse, using only organ dysfunction trajectories to define broad phenotypes and determine their prognostic and therapeutic relevance, but performing deeper phenotyping using other clinical features and biomarkers may result in phenotypes with potentially higher resolution and greater clinical utility. Third, the therapeutic relevance of IV hydrocortisone was studied using an interaction effect analysis on a propensity score matched cohort, and the results must be interpreted with caution, as previously discussed. Fourth, although we described the MODS phenotypes as distinct entities, it is likely that many patients share features of more than 1 phenotype, and future analyses to better understand the implications of these overlaps are warranted.
Conclusions
In this study, we derived and validated 4 data-driven phenotypes of MODS in critically ill children that have distinct clinical characteristics, are independently associated with outcomes, and may be therapeutically relevant in the subset of patients with vasoactive-dependent shock. Our data-driven phenotyping approach in MODS shows promising results, but further characterization of these broad phenotypes and validation in different settings is warranted.
eAppendix. Supplementary Methods
eFigure 1. Alluvial Plots of Organ Dysfunction Burden by Day in the 4 MODS Phenotypes
eFigure 2. Kaplan-Meier Survival Curves for the First 28 Days for the 4 MODS Phenotypes
eFigure 3. Covariate Balance in the Propensity Score Matched Cohort of Patients With Vasoactive-Dependent Shock Who Received and Did Not Receive Intravenous Hydrocortisone
eTable 1. Maximum pSOFA Subscores Achieved by Day in Patients Within Each of the 4 MODS Phenotypes in the Derivation and Validation Sets
eTable 2. Laboratory Test Results by Day 3 of PICU Stay in the 4 MODS Phenotypes Across the Derivation and Validation Sets
eTable 3. Outcomes Associated With the 4 MODS Phenotypes Across the Derivation and Validation Sets
eTable 4. Laboratory Test Results and Outcomes Associated With the MODS Phenotypes When Using Patients in Hospital A as the Derivation Set and Patients in Hospital B as an External Validation Set
eTable 5. Distribution and Outcomes Associated With the 4 MODS Phenotypes Across Age Groups
eTable 6. Unadjusted and Adjusted Outcomes Associated With the 4 MODS Phenotypes
eTable 7. Multivariable Association Between Noncharacteristic Organ Dysfunctions and In-Hospital Mortality
eReferences.
References
- 1.Tamburro RF, Jenkins TL. Multiple organ dysfunction syndrome: a challenge for the pediatric critical care community. Pediatr Crit Care Med. 2017;18(3_suppl)(suppl 1):S1-S3. [DOI] [PubMed] [Google Scholar]
- 2.Matics TJ, Pinto NP, Sanchez-Pinto LN. Association of organ dysfunction scores and functional outcomes following pediatric critical illness. Pediatr Crit Care Med. 2019;20(8):722-727. doi: 10.1097/PCC.0000000000001999 [DOI] [PubMed] [Google Scholar]
- 3.Leteurtre S, Duhamel A, Salleron J, Grandbastien B, Lacroix J, Leclerc F; Groupe Francophone de Réanimation et d’Urgences Pédiatriques (GFRUP) . PELOD-2: an update of the Pediatric Logistic Organ Dysfunction score. Crit Care Med. 2013;41(7):1761-1773. doi: 10.1097/CCM.0b013e31828a2bbd [DOI] [PubMed] [Google Scholar]
- 4.Lin JC, Spinella PC, Fitzgerald JC, et al. ; Sepsis Prevalence, Outcomes, and Therapy Study Investigators . New or progressive multiple organ dysfunction syndrome in pediatric severe sepsis: a sepsis phenotype with higher morbidity and mortality. Pediatr Crit Care Med. 2017;18(1):8-16. doi: 10.1097/PCC.0000000000000978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leteurtre S, Duhamel A, Deken V, Lacroix J, Leclerc F; Groupe Francophone de Réanimation et Urgences Pédiatriques . Daily estimation of the severity of organ dysfunctions in critically ill children by using the PELOD-2 score. Crit Care. 2015;19:324. doi: 10.1186/s13054-015-1054-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hall MW, Gavrilin MA, Knatz NL, Duncan MD, Fernandez SA, Wewers MD. Monocyte mRNA phenotype and adverse outcomes from pediatric multiple organ dysfunction syndrome. Pediatr Res. 2007;62(5):597-603. doi: 10.1203/PDR.0b013e3181559774 [DOI] [PubMed] [Google Scholar]
- 7.Upperman JS, Lacroix J, Curley MA, et al. Specific etiologies associated with the multiple organ dysfunction syndrome in children: part 1. Pediatr Crit Care Med. 2017;18(3_suppl)(suppl 1):S50-S57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carcillo JA, Podd B, Aneja R, et al. Pathophysiology of pediatric multiple organ dysfunction syndrome. Pediatr Crit Care Med. 2017;18(3_suppl)(suppl 1):S32-S45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Seely AJ, Christou NV. Multiple organ dysfunction syndrome: exploring the paradigm of complex nonlinear systems. Crit Care Med. 2000;28(7):2193-2200. doi: 10.1097/00003246-200007000-00003 [DOI] [PubMed] [Google Scholar]
- 10.An G, Nieman G, Vodovotz Y. Computational and systems biology in trauma and sepsis: current state and future perspectives. Int J Burns Trauma. 2012;2(1):1-10. [PMC free article] [PubMed] [Google Scholar]
- 11.Hotchkiss RS, Sherwood ER. Immunology: getting sepsis therapy right. Science. 2015;347(6227):1201-1202. doi: 10.1126/science.aaa8334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wong HR, Cvijanovich NZ, Anas N, et al. Developing a clinically feasible personalized medicine approach to pediatric septic shock. Am J Respir Crit Care Med. 2015;191(3):309-315. doi: 10.1164/rccm.201410-1864OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Carcillo JA, Berg RA, Wessel D, et al. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network . A multicenter network assessment of three inflammation phenotypes in pediatric sepsis-induced multiple organ failure. Pediatr Crit Care Med. 2019;20(12):1137-1146. doi: 10.1097/PCC.0000000000002105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Seymour CW, Kennedy JN, Wang S, et al. Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis. JAMA. 2019;321(20):2003-2017. doi: 10.1001/jama.2019.5791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Knox DB, Lanspa MJ, Kuttler KG, Brewer SC, Brown SM. Phenotypic clusters within sepsis-associated multiple organ dysfunction syndrome. Intensive Care Med. 2015;41(5):814-822. doi: 10.1007/s00134-015-3764-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA; NHLBI ARDS Network . Subphenotypes in acute respiratory distress syndrome: latent class analysis of data from two randomised controlled trials. Lancet Respir Med. 2014;2(8):611-620. doi: 10.1016/S2213-2600(14)70097-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sweeney TE, Azad TD, Donato M, et al. Unsupervised analysis of transcriptomics in bacterial sepsis across multiple datasets reveals three robust clusters. Crit Care Med. 2018;46(6):915-925. doi: 10.1097/CCM.0000000000003084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Seymour CW, Gomez H, Chang CH, et al. Precision medicine for all? challenges and opportunities for a precision medicine approach to critical illness. Crit Care. 2017;21(1):257. doi: 10.1186/s13054-017-1836-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saria S, Goldenberg A. Subtyping: what it is and its role in precision medicine. IEEE Intell Syst. 2015;30(4):70-75. doi: 10.1109/MIS.2015.60 [DOI] [Google Scholar]
- 20.Schulam P, Wigley F, Saria S Clustering longitudinal clinical marker trajectories from electronic health data: applications to phenotyping and endotype discovery. Paper presented at: 29th Conference on Artificial Intelligence; January 25-30, 2015; Austin, TX. [Google Scholar]
- 21.Luo Y, Xin Y, Joshi R, Celi LA, Szolovits P Predicting ICU mortality risk by grouping temporal trends from a multivariate panel of physiologic measurements. Paper presented at: 30th AAAI Conference; February 12-17, 2016; Phoenix, AZ. [Google Scholar]
- 22.Bhavani SV, Carey KA, Gilbert ER, Afshar M, Verhoef PA, Churpek MM. Identifying novel sepsis subphenotypes using temperature trajectories. Am J Respir Crit Care Med. 2019;200(3):327-335. doi: 10.1164/rccm.201806-1197OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moreno R, Vincent J-L, Matos R, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care: results of a prospective, multicentre study, Working Group on Sepsis-Related Problems of the ESICM. Intensive Care Med. 1999;25(7):686-696. doi: 10.1007/s001340050931 [DOI] [PubMed] [Google Scholar]
- 24.Matics TJ, Sanchez-Pinto LN. Adaptation and validation of a pediatric Sequential Organ Failure Assessment score and evaluation of the Sepsis-3 definitions in critically ill children. JAMA Pediatr. 2017;171(10):e172352. doi: 10.1001/jamapediatrics.2017.2352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Crit Care Med. 1996;24(5):743-752. doi: 10.1097/00003246-199605000-00004 [DOI] [PubMed] [Google Scholar]
- 26.Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14(1):199. doi: 10.1186/1471-2431-14-199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Borgelt C, Meinl T, Berthold M. MoSS: a program for molecular substructure mining. Proc First Int Workshop on Open Source Data Mining. 2005:6-15. doi: 10.1145/1133905.1133908 [DOI] [Google Scholar]
- 28.Gaujoux R, Seoighe C. A flexible R package for nonnegative matrix factorization. BMC Bioinformatics. 2010;11(1):367. doi: 10.1186/1471-2105-11-367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Graciano AL, Balko JA, Rahn DS, Ahmad N, Giroir BP. The Pediatric Multiple Organ Dysfunction Score (P-MODS): development and validation of an objective scale to measure the severity of multiple organ dysfunction in critically ill children. Crit Care Med. 2005;33(7):1484-1491. doi: 10.1097/01.CCM.0000170943.23633.47 [DOI] [PubMed] [Google Scholar]
- 30.Leteurtre S, Martinot A, Duhamel A, et al. Development of a pediatric multiple organ dysfunction score: use of two strategies. Med Decis Making. 1999;19(4):399-410. doi: 10.1177/0272989X9901900408 [DOI] [PubMed] [Google Scholar]
- 31.Wong HR, Cvijanovich NZ, Anas N, et al. Endotype transitions during the acute phase of pediatric septic shock reflect changing risk and treatment response. Crit Care Med. 2018;46(3):e242-e249. doi: 10.1097/CCM.0000000000002932 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Annane D, Renault A, Brun-Buisson C, et al. ; CRICS-TRIGGERSEP Network . Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378(9):809-818. doi: 10.1056/NEJMoa1705716 [DOI] [PubMed] [Google Scholar]
- 33.Menon K, McNally JD. Corticosteroids in pediatric septic shock are helpful. Crit Care Med. 2018;46(4):635-636. doi: 10.1097/CCM.0000000000002979 [DOI] [PubMed] [Google Scholar]
- 34.Menon K, McNally JD, Choong K, et al. A survey of stated physician practices and beliefs on the use of steroids in pediatric fluid and/or vasoactive infusion-dependent shock. Pediatr Crit Care Med. 2013;14(5):462-466. doi: 10.1097/PCC.0b013e31828a7287 [DOI] [PubMed] [Google Scholar]
- 35.Sprung CL, Annane D, Keh D, et al. ; CORTICUS Study Group . Hydrocortisone therapy for patients with septic shock. N Engl J Med. 2008;358(2):111-124. doi: 10.1056/NEJMoa071366 [DOI] [PubMed] [Google Scholar]
- 36.Venkatesh B, Finfer S, Cohen J, et al. ; ADRENAL Trial Investigators and the Australian–New Zealand Intensive Care Society Clinical Trials Group . Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378(9):797-808. doi: 10.1056/NEJMoa1705835 [DOI] [PubMed] [Google Scholar]
- 37.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573-577. doi: 10.7326/0003-4819-147-8-200710160-00010 [DOI] [PubMed] [Google Scholar]
- 38.Annane D, Sébille V, Bellissant E; Ger-Inf-05 Study Group . Effect of low doses of corticosteroids in septic shock patients with or without early acute respiratory distress syndrome. Crit Care Med. 2006;34(1):22-30. doi: 10.1097/01.CCM.0000194723.78632.62 [DOI] [PubMed] [Google Scholar]
- 39.Tongyoo S, Permpikul C, Mongkolpun W, et al. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: results of a randomized controlled trial. Crit Care. 2016;20(1):329. doi: 10.1186/s13054-016-1511-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kochanek PM, Tasker RC, Carney N, et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the Brain Trauma Foundation guidelines. Pediatr Crit Care Med. 2019;20(3S)(suppl 1):S1-S82. doi: 10.1097/PCC.0000000000001735 [DOI] [PubMed] [Google Scholar]
- 41.Fitzgerald JC, Weiss SL, Maude SL, et al. Cytokine release syndrome after chimeric antigen receptor T cell therapy for acute lymphoblastic leukemia. Crit Care Med. 2017;45(2):e124-e131. doi: 10.1097/CCM.0000000000002053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hall MW, Knatz NL, Vetterly C, et al. Immunoparalysis and nosocomial infection in children with multiple organ dysfunction syndrome. Intensive Care Med. 2011;37(3):525-532. doi: 10.1007/s00134-010-2088-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shakoory B, Carcillo JA, Chatham WW, et al. Interleukin-1 receptor blockade is associated with reduced mortality in sepsis patients with features of the macrophage activation syndrome: re-analysis of a prior phase III trial. Crit Care Med. 2016;44(2):275-281. doi: 10.1097/CCM.0000000000001402 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix. Supplementary Methods
eFigure 1. Alluvial Plots of Organ Dysfunction Burden by Day in the 4 MODS Phenotypes
eFigure 2. Kaplan-Meier Survival Curves for the First 28 Days for the 4 MODS Phenotypes
eFigure 3. Covariate Balance in the Propensity Score Matched Cohort of Patients With Vasoactive-Dependent Shock Who Received and Did Not Receive Intravenous Hydrocortisone
eTable 1. Maximum pSOFA Subscores Achieved by Day in Patients Within Each of the 4 MODS Phenotypes in the Derivation and Validation Sets
eTable 2. Laboratory Test Results by Day 3 of PICU Stay in the 4 MODS Phenotypes Across the Derivation and Validation Sets
eTable 3. Outcomes Associated With the 4 MODS Phenotypes Across the Derivation and Validation Sets
eTable 4. Laboratory Test Results and Outcomes Associated With the MODS Phenotypes When Using Patients in Hospital A as the Derivation Set and Patients in Hospital B as an External Validation Set
eTable 5. Distribution and Outcomes Associated With the 4 MODS Phenotypes Across Age Groups
eTable 6. Unadjusted and Adjusted Outcomes Associated With the 4 MODS Phenotypes
eTable 7. Multivariable Association Between Noncharacteristic Organ Dysfunctions and In-Hospital Mortality
eReferences.