

Abstract
Objectives:
To test whether 1) concussed athletes demonstrate slower tandem gait times compared to controls and 2) concussed female athletes display greater post-injury deficits than males.
Design:
Prospective longitudinal
Method:
Fifty concussed collegiate student-athletes (32% female, age= 20.18±1.27 years) completed tandem gait tests during pre-season (Time 1) and acutely (<72 hours) post-concussion (Time 2), and twenty-five controls (52% female, age=21.08±2.22 years) completed tandem gait at two time points, 1.96±0.46 days apart. Participants completed four single-task (ST) and dual-task (DT) trials. During DT trials, they simultaneously completed a cognitive assessment. The best ST and DT times were recorded, along with cognitive accuracy, and the change score between the two assessments was calculated. A positive change in tandem gait time was indicative of worsening performance. A 2×2 (group*sex) ANOVA was used to examine change between pre-injury and post-injury tests for ST/DT tandem gait time and DT cognitive accuracy.
Results:
The change in tandem gait time from Time 1 to Time 2 was significantly higher for the concussion group relative to controls during both ST (Concussion: 1.36±2.6 seconds, Controls: −1.16±0.8 seconds, p<0.001) and DT (Concussion: 1.70±3.8 seconds, Controls: −0.94±1.7 seconds, p=0.002) tandem gait. There were no interactions or main effects of sex for tandem gait time or cognitive accuracy.
Conclusions:
There were no sex-specific differences in the change in tandem gait performance among concussed collegiate athletes or controls. However, all concussed participants, regardless of sex, performed significantly worse on tandem gait than male and female controls, who both improved between testing time points.
Keywords: Gait, Balance, Mild Traumatic Brain Injury, Sex Differences
Introduction
Sports with the highest overall concussion rate, such as ice hockey and football, are seeing a rise in concussion incidence.1 Male sports continue to have higher concussion rates; however, females sustain more concussions than their male counterparts when participating in the same sports.1,2 Concussions are individualized injuries that do not conform to a “one size fits all” approach when it comes to recovery; thus, it is important to continue exploring the individual factors that contribute to post-concussion performance, such as sex.
Due to the individualized nature and presentation for patients with a concussion, a multifaceted approach of symptom, neurocognitive, and postural control assessments is recommended following concussion.3 Symptom burden, neurocognitive function, and recovery differences between females and males have been explored in the literature, whereby females typically present with a larger number of symptoms in the somatic, emotional, and cognitive domains, take longer to become asymptomatic, and have greater impairments in reaction time and visual memory than males.4–6 Conversely, males frequently report greater cognitive impairments (i.e. amnesia, confusion, disorientation) as their primary symptoms.7 Despite these recent advancements in understanding differences between female and male athletes after concussion, the literature remains mixed8,9, and sex specific differences in postural control have received even less attention.
The Balance Error Scoring System (BESS) is the most frequently used assessment for post-concussion postural control, and currently published work suggests that there are no sex differences in baseline or post-concussion BESS scores.10–12 While BESS scores typically increase (get worse) post-concussion, sex does not mediate these changes. In addition to the BESS, other tests have emerged to augment balance evaluations for concussion patients. The tandem gait test, included as a part of the Sport Concussion Assessment Tool (SCAT5), is a clinically feasible task that has successfully identified postural control impairments following concussion and appears to be more sensitive to the acute effects of a concussion than the BESS.13–15 Deficits in post-concussion tandem gait have been elicited under both single-task (ST) and dual-task (DT) conditions, and dual-task conditions, whereby the individual is asked to complete the tandem gait test while they concurrently perform a cognitive task, reveal more prominent and longer lasting deficits.13,14,16
Prior work using instrumented paradigms found that concussed females had a greater change in step frequency between ST and DT trials compared to concussed males.17 Instrumented gait analysis requires sophisticated technology that is cost prohibitive and largely unavailable to the majority of clinical settings. Thus, further work is needed to determine if female or male athletes demonstrate balance impairments following a concussion using a clinically feasible test. As most clinicians will not have ccess to instrumented gait labs, exploring the differences in male and female performance on tandem gait may allow for a translational approach from the laboratory to the clinic. Therefore, the purpose of this investigation was to examine whether changes between baseline and acute post injury tandem gait performance, both single and dual-task, differed between male and female collegiate athletes. We hypothesized that 1) athletes with a concussion would demonstrate slower tandem gait times compared to healthy controls and 2) female athletes with concussion would display greater post-injury deficits compared to males with concussion.
Methods
Fifty (64% Female, Age= 20.18±1.27 years) NCAA Division I student-athletes from two institutions with diagnosed concussions completed the study (Table 1). Diagnoses were made by a certified athletic trainer and subsequently confirmed by a team physician in accordance with the criteria established from the 5th International Conference on Concussion in Sport.3 Healthy active controls (52% Female, Age=21.08±2.22 years) were recruited from the general student population. All participants in the concussion group were active members of an NCAA team that had been medically cleared for athletic participation prior to the preseason baseline test. Participants in both groups were excluded if they reported any neurological disorder, current or previous lower extremity orthopedic injury that may impair gait performance, any metabolic, vestibular, vision disorder not associated with their acute concussion that may impair gait performance, or a previous concussion within the last six months. Oral and written consent was provided from each participant prior to data collection, and testing procedures were reviewed and approved by the respective Institutional Review Boards.
Table 1.
Participant demographics. There were significant differences (*) between the concussion and control groups for age, and number of days between testing time points.
| Demographics | Concussion (n=50) | Controls (n=25) | p-value |
|---|---|---|---|
| Males/Females (n) | 18/32 | 12/13 | --- |
| Age (years) | 20.18 ± 1.27 | 21.08 ±2.22 | 0.03* |
| Height (cm) | 175.03 ± 11.52 | 170.71 ±9.65 | 0.12 |
| Mass (kg) | 72.61 ± 14.87 | 72.76 ±16.97 | 0.97 |
| Concussion History (n) Range |
0.66 ± 0.94 21/50(42%) 0–4 |
0.32 ±0.85 5/25 (20%) 0–4 |
0.13 |
| Days from Time 1 to Time 2 (n) | 223.40 ±200.19 | 1.96 ±0.46 | <0.001* |
| Days from Concussion to Acute (n) | 1.58 ±1.05 | --- | --- |
Tandem gait measures were collected consistent with the guidelines established by the SCAT-3, which were the guidelines in place at the time of data collection.18 Participants were instructed to stand with their feet together behind a 3-meter long line made by placing standard sports tape (38mm width) along the floor. Following a verbal cue, they were instructed to walk with a heel-to-toe gait the length of the line as quickly and accurately as possible. After reaching the end of the line, they completed a 180° turn and returned the starting line while maintaining the heel-to-toe pattern. All trials were timed using a handheld stopwatch or stopwatch app on a smartphone. Trials in which the participant failed to maintain a heel-to-toe pattern or stepped off the line were deemed unsuccessful and repeated. None of our participants required more than one repeated trial. Four successful trials were completed for each condition (ST and DT), and the fastest time was used for analysis.18
The DT condition required participants to perform a cognitive task while simultaneously completing the tandem gait test. The cognitive tasks consisted of mini-mental style questions and have been successful in identifying impairments in DT tandem gait.14,16 These tasks included spelling 5 letter words backward, repeatedly subtracting by 6s or 7s from a randomly presented number, and listing the months of the year in reverse order. Prior to each trial, the investigator explained the task, but there were no prioritization instructions included, meaning the participants were not instructed to focus on either the motor or cognitive task over the other. The order of tasks was randomized for each participant at each testing session, and all three task types were scored the same. The number of correct responses and total number of responses were recorded with the percentage of correct responses being used as the cognitive accuracy outcome measure.
For the concussion group, pre-injury data was collected at the time of pre-season baseline testing prior to the competitive seasons. (Time 1) All concussed participants were then retested acutely (<72 hours) post-injury. (Time 2) Control participants completed testing on a predetermined day (Time 1) and again within 72 hours of the first test. (Time 2)
This was a prospective, longitudinal study. The independent variables were group (concussion, control) and sex (male, female). Our primary dependent variables were change in best ST tandem gait time between the two testing days, change in best DT tandem gait time between the two testing days, and change in cognitive accuracy between the two testing days. The change score was calculated from subtracting the best Time 1 tandem gait time from best Time 2 tandem gait time for both ST and DT: Change=(DT best time – ST best time). A positive change in tandem time was indicative of worsening (i.e. slower) performance. Conversely, a positive change in cognitive accuracy demonstrated improvement.
Demographic variables were reported as the mean ± SD and compared between both the concussion and control groups, and male and female participants with independent sample t-tests. A 2 (group) × 2 (sex) ANOVA was employed to determine any differences among the dependent variables. Any significant interactions and/or main effects were followed up with pairwise comparisons. The level of significance was set at P < 0.05 and all statistical analyses were performed with SPSS (version 22; IBM Inc, Armonk, NY).
Results
All participants completed the tandem gait trials successfully without incident. The control group was significantly older than the concussion group (p=0.03), and the concussion group had a significantly longer time interval between tests than the control group (p<0.001). There was no significant difference in height, mass, or proportion with a prior concussion history between the concussion and control groups (Table 1). Male participants were older (21.12±2.06 vs 20.01±1.21 years, p=0.01), taller (182.63±7.93 vs 167.79±8.27 cm, p<0.001), and heavier (86.39±13.45 vs 63.60±7.81 kg, p<0.001) than female participants. There was no significant difference in the mean number of previous concussions between male and female participants (0.73±1.11 vs. 0.43±0.75, p=0.15).
There was no significant interaction (F= 0.81, p=0.37, η2=0.01) or main effect for sex (F=0.00, p=0.99, η2=0.00) for ST tandem gait time. Male and female participants did not significantly differ in ST tandem gait performance from Time 1 to Time 2 (Figure 1). There was a significant difference between groups (F=21.60, p<0.001, η2=0.23). The control group improved across time (Time 1: 10.22±1.86 seconds, Time 2: 9.07±1.78 seconds) while the concussion group got worse (Time 1: 10.51±2.09 seconds, Time 2: 11.80±2.46 seconds).
Figure 1.
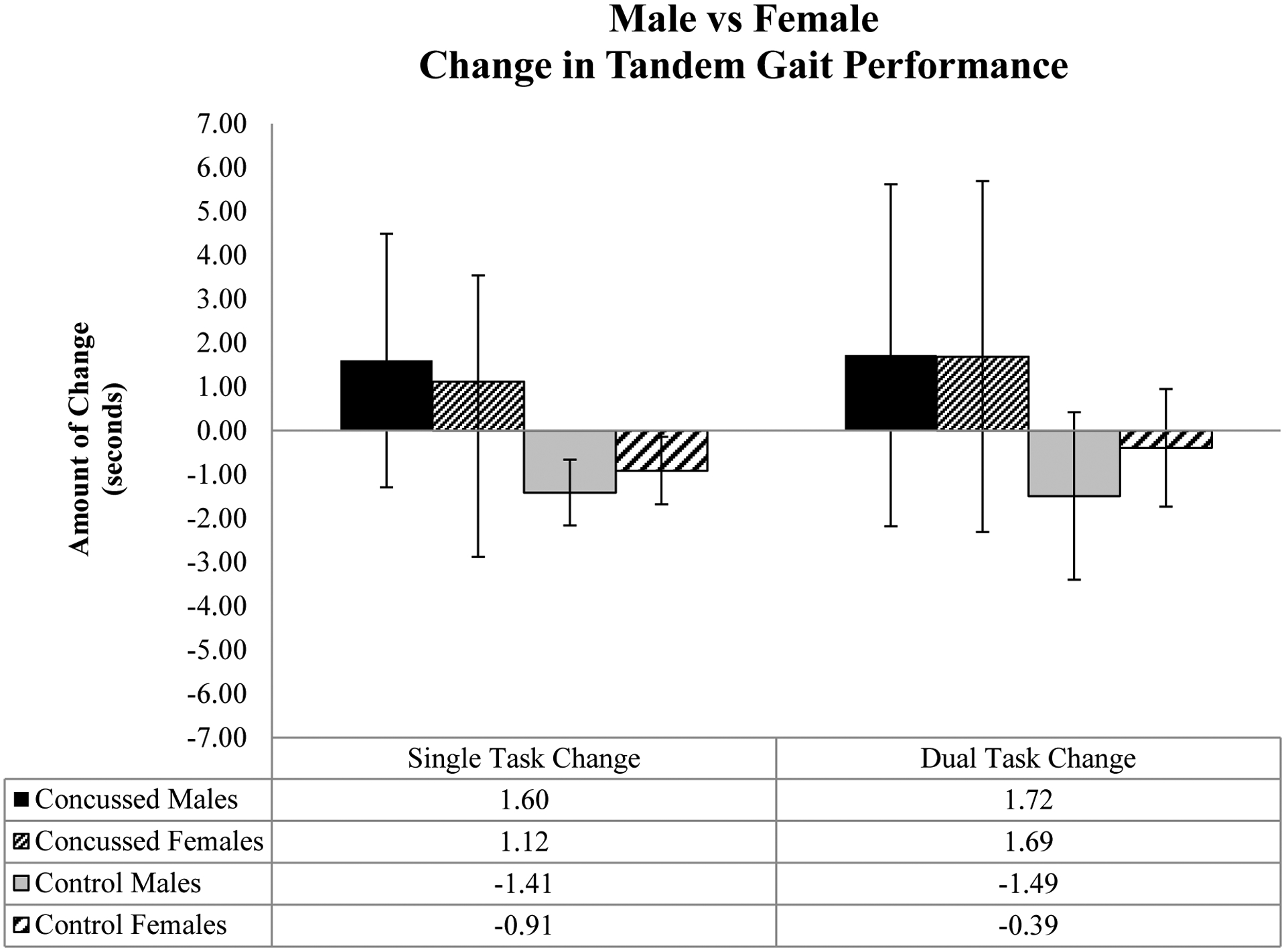
Sex differences for change in tandem gait performance between Time 1 and Time 2. There were no significant differences between males and females for ST (F=0.00, p=0.99) or DT (F=0.40, p=0.53) tandem gait performance across the two time points. A positive change reflects a worsening in performance between time points.
There was no significant interaction (F= 0.44, p=0.51, η2=0.01) or main effect for sex (F=0.40, p=0.53, η2=0.01) with DT tandem gait. Male and female participants did not significantly differ in DT tandem gait performance from Time 1 to Time 2 (Figure 1). There was a significant difference between groups (F=9.84, p=0.002, η2=0.12). The control group improved across time (Time 1: 12.27±2.64 seconds, Time 2: 11.35±3.03 seconds) while the concussion group got worse (Time 1: 13.76±3.44 seconds, Time 2: 15.46±3.89 seconds).
There was no significant interaction (F=0.02, p=0.89, η2=0.00) for change in cognitive accuracy. Male and female participants did not significantly differ in their change in cognitive accuracy (1.70±16.46% vs. 1.10±12.99%, p= 0.87, η2=0.00) Similarly, the change in cognitive accuracy between the concussion and control groups was not significantly different (1.56±16.71% vs. 1.24±8.18%, p=0.93, η 2=0.00).
Discussion
The primary finding from our investigation suggests that male and female participants in both the concussion and control groups did not significantly differ in tandem gait performance across two time points. While we did not observe significant differences between females and males on the amount of change between pre- and post-injury assessments, the concussion group demonstrated greater tandem gait impairments (i.e. a positive change in time) between Time 1 and Time 2 than the healthy controls, which further supports the use of tandem gait as an acute assessment of dynamic postural control following concussion.
There were no significant differences for ST or DT tandem gait performance from Time 1 to Time 2 between males and female athletes. Both males and female athletes with a concussion had similar decreases in performance between Time 1 and 2 on both ST and DT tandem gait. Likewise, the male and female controls both improved ST and DT tandem gait performance between Time 1 and Time 2. These results build upon the established normative values for tandem gait, whereby sex was not a determinant of time to completion in collegiate athletes19 or a healthy adult population.20 Howell et al., identified significant differences in DT gait cadence between adolescent males and females with concussion, where females demonstrated a lower cadence (94.8 versus 102.2 steps/min) during unobstructed walking than males.17 However, these alterations were elucidated under instrumented gait analysis, and we could not extrapolate cadence directly from tandem gait in this investigation. The similar tandem gait performance we observed between males and female participants has also been reflected in BESS scores, under both normative10 and post-concussion conditions.11,12 The maintenance of postural control requires complex interaction from the vestibular, visual, and somatosensory systems, all of which reach the adult level by 16 years of age, and while female individuals demonstrate balance superiority to males until 11–12 years old, beyond that age, there are no significant developmental sex differences.21 Thus, the underlying mechanism of control does not appear to be different between males and females, even though BESS is a measure of postural control via quiet stance and tandem gait is a task of dynamic postural control.
A number of studies have identified that male and female athletes differ in their post-concussion symptoms, with males reporting primarily cognitive symptoms (i.e. amnesia, confusion/disorientation)7,22 and females presenting with a greater number of symptoms in the somatic, cognitive, and emotional domains (i.e. headache, sensitivity to light, difficulty concentrating, feeling slowed down, more emotional/irritable) when compared to their male counterparts.4,5 However, there are still mixed findings in regards to clinically significant sex differences, and continuing research is warranted.9,23 In addition to a possible increased symptom burden, female athletes consistently take longer than males to become asymptomatic; however, male athletes were recently found to recover dual-task gait abilities slower than females, suggesting sex differences after concussion may vary based on assessment type.4–6,8,24 Regardless of sex, the second most common post-concussion symptom is dizziness, which is often a vestibular symptom that can result in concurrent balance impairments.25,26 As a result, vestibulo-ocular assessments, such as The Vestibular and Ocular Motor Screening (VOMS), have become commonplace in most concussion testing batteries and usually consist of a balance and vision assessment.4 Unlike the clinical balance assessments, vision tests have demonstrated mixed results when it comes to sex differences, with some studies observing no differences11,27 and others finding that females perform worse.12,28 While no sex differences were observed in the near point convergence component of the VOMS, individuals with receded near point convergence have demonstrated gait deficits following concussion;29 thus, it is possible that only particular vestibular symptoms manifest differently in male and female athletes, and a combination of balance and vision assessments should continue to be utilized after a concussive injury.
In addition to a lack of sex differences in the motor component of tandem gait, our results do not reflect a difference in performance on cognitive accuracy during a motor task between male and female collegiate athletes. Dual-task paradigms serve as an indicator of executive function, and following concussion, females have displayed greater executive function deficits than males.30,31 Both sexes, herein, performed worse on DT tandem gait at Time 2; however, both sexes also improved their cognitive accuracy scores at Time 2, which suggests there is no difference in how males and females prioritize tasks, as suggested in prior DT gait studies.17,32 When given no instructions, healthy young males and females walked at similar gait speeds under DT conditions, but when instructed to make gait the priority, females increased gait speed while males kept gait speed consistent.32 Not only did the females walk faster, but they also maintained their cognitive task, despite the instruction to prioritize the motor component.32 This raises the possibility that females are more efficient at dual tasking under certain conditions. It could also be a reflection of better adherence to the given instructions by young female athletes. Within our investigation, male and female participants both appeared to prioritize the cognitive component over the motor component during DT tandem gait, as both performed slower on tandem gait across time while also improving cognitive accuracy; however, we did not give any specific instructions as to how the participants were to prioritize tandem gait time and cognitive accuracy. Therefore, future research should examine this balance further to see if the sex differences observed under different priority instructions during gait hold true for tandem gait as well.
Despite a lack of sex differences, we observed significant differences between the concussion and control groups for both ST and DT tandem gait. The acute worsening in tandem gait time by the concussion group coincides with what has been observed in similar populations for both ST13,14 and DT14 and further reinforces tandem gait as a useful clinical assessment that is sensitive to identifying changes in postural control acutely post-concussion. For the acutely concussed participants, the mean worsening in performance (1.29 seconds) exceeded 0.38 seconds, which was previously established as the minimum detectable change (MDC) for tandem gait;13 thus, the deficits observed cannot be explained as normal examiner variability. In a clinical setting, a post-concussion change in tandem gait time greater than 0.38 seconds may be treated as evidence of within-subject postural control impairment, but any worsening in time is considered “failed.” We currently only have the MDC for clinical judgement, and more work on clinically meaningful differences needs to be performed on tandem gait to establish these values. Unlike previous literature,13 the healthy controls herein also exceeded 0.38 seconds during their improvement in tandem gait performance, which suggests a practice effect may be present and warrants future research. As tandem gait research continues to advance, it is becoming more evident that the impairments in dynamic postural control manifest as slower times to complete the task. This reflection of worsened tandem gait performance has been seen from youth to college athletes.13,14,16 The best timed trial was the suggested outcome variable in the SCAT-3,18 but in the transition to the SCAT-5 been removed and replaced with a subjective “yes/no” without objective criteria for “failing.”15 Clinicians might consider continuing to include the timed aspect of tandem gait, as it appears more sensitive in identifying postural control impairments after concussion than a simple pass/fail measurement criterion.13,14
This study is not without limitations. Our tandem gait assessments were performed with collegiate athletes in a quiet environment, away from sideline or game distractions; therefore, applicability to other populations and settings is limited. We acknowledge that the significant difference in the number of days from Time 1 to Time 2 between the concussion and control groups could influence our results. However, unobstructed gait has demonstrated to be stable over time in adults,33 and tandem gait was found to have high test-retest reliability in both adolescents and adults;34,35 therefore, we do not believe the time difference influenced our results. We used the best of the four tandem gait trials as our outcome, but future research could consider using the mean to explore potential differences between groups. Unsurprisingly, males were significantly taller and heavier than the females. However, our within-subjects study design accounts for these differences. Lastly, we only utilized one type of DT challenge, and future research should start to explore other domains of DT to see if different styles can elicit additional alterations in performance.
Conclusions
In conclusion, there were no significant differences between male and female athletes in pre and post-concussion tandem gait performance under either ST or DT conditions. There were, however, significant differences in performance between the concussion group and healthy controls, as the concussed individuals demonstrated a significant worsening in tandem gait time from pre-injury to post-injury tests compared to healthy controls who completed two tests. These deficits further support tandem gait as a clinically useful assessment of dynamic postural control. Despite the lack of sex differences within this investigation, concussions appear to manifest differently in males and females in other domains; thus, future work should continue to explore these individualized characteristics.
Table 2.
Mean, standard deviation, and 95% confidence intervals for ST and DT tandem gait data between males and females.
| Males | Females | ||
|---|---|---|---|
| Time 1 | Single Task Tandem Gait (seconds) |
9.80 ±1.73 (9.16–10.45) |
10.82 ±2.09 (10.19–11.44) |
| Dual Task Tandem Gait (seconds) |
12.34 ±2.91 (11.26–13.43) |
13.88 ±3.36 (12.87–14.89) |
|
| Cognitive Accuracy (%) |
88.14 ±13.03% (83.18%−93.09%) |
90.04 ± 12.60% (86.25%−93.93%) |
|
| Time 2 | Single Task Tandem Gait (seconds) |
10.20 ±2.69 (9.19–11.21) |
11.35 ±2.44 (10.61–12.08) |
| Dual Task Tandem Gait (seconds) |
12.78 ±3.65 (11.42–14.14) |
14.96 ±4.19 (13.71–16.22) |
|
| Cognitive Accuracy (%) |
89.16 ±15.38% (83.42%−94.90%) |
91.31 ± 10.53% (88.15%−94.47%) |
|
Practical Implications:
Tandem gait is a clinically relevant tool that is successful at identifying postural control impairments acutely following concussion.
Despite prior evidence that male and female athletes may differ on some concussion assessments and concussion recovery, they appear to perform similarly on tandem gait. Clinicians should use the same guidelines when evaluating both sexes.
Clinicians can expect to see a worse (slower) tandem gait time acutely post-concussion in both male and female athletes compared to their baseline times. It is unknown how long these impairments may persist beyond the acute post-injury window.
Using time as the primary outcome for tandem gait appears to be better suited for identifying postural control impairments in a clinical setting than pass/fail criteria.
Acknowledgements
Research reported in this publication was supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Number R01NS100952. We would like to acknowledge Melissa DiFabio, Ryan DeWolf, and Anna Brilliant for their assistance with data collection for this manuscript.
Dr. Koerte has received funding related to this research from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health (R01NS100952). Dr. Meehan receives royalties from 1) ABC-Clio publishing for the sale of his books, Kids, Sports, and Concussion: A guide for coaches and parents, and Concussions; 2) Springer International for the book Head and Neck Injuries in Young Athlete and 3) Wolters Kluwer for working as an author for UpToDate. His research is funded, in part, by philanthropic support from the National Hockey League Alumni Association through the Corey C. Griffin Pro-Am Tournament and the National Football League. Dr. Howell receives research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD094560) and the National Institute of Neurological Disorders And Stroke (R01NS100952 and R41NS103698) of the National Institutes of Health. He has previously received research support from a research contract between Boston Children’s Hospital, Cincinnati Children’s Hospital Medical Center, and ElMindA Ltd, and the Eastern Athletic Trainers Association Inc. Dr. Buckley has received funding related to this research from the NIH/NINDS (R03NS104371) and the NCAA/DoD CARE Consortium (W81XWH-14-2-0151). For the remaining authors none were declared.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Zuckerman SL, Kerr ZY, Yengo-Kahn A, et al. Epidemiology of Sports-Related Concussion in NCAA Athletes From 2009–2010 to 2013–2014: Incidence, Recurrence, and Mechanisms. Am J Sports Med 2015. Doi: 10.1177/0363546515599634. [DOI] [PubMed] [Google Scholar]
- 2.Marar M, McIlvain NM, Fields SK, et al. Epidemiology of Concussions Among United States High School Athletes in 20 Sports. Am J Sports Med 2012; 40(4):747–755. Doi: 10.1177/0363546511435626. [DOI] [PubMed] [Google Scholar]
- 3.McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion ins sport-the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sport Med 2017; 51:838–847. [DOI] [PubMed] [Google Scholar]
- 4.Covassin T, Savage J, Bretzin A, et al. Sex differences in sport-related concussion long-term outcomes. Int J Psychophysiol 2018; 132:9–13. [DOI] [PubMed] [Google Scholar]
- 5.Baker J, Leddy J, Darling S, et al. Gender differences in recovery from sports-related concussion in adolescents. Clin Pediatr (Phila) 2016; 55(8):771–775. [DOI] [PubMed] [Google Scholar]
- 6.Broshek D, Kaushik T, Freeman J, et al. Sex differences in outcome following sports-related concussion. J Neurosurg 2005; 102(5):856–863. [DOI] [PubMed] [Google Scholar]
- 7.Brown D a, Elsass J a, Miller AJ, et al. Differences in symptom reporting between males and females at baseline and after a sports-related concussion: A systematic review and meta-analysis. Sport Med 2015; 45(7):1027–1040. Doi: 10.1007/s40279-015-0335-6. [DOI] [PubMed] [Google Scholar]
- 8.Iverson G, Gardner A, Terry D, et al. Predictors of clinical recovery from concussion: a systematic review. Br J Sport Med 2017; 51:941–948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Merritt V, Padgett C, Jak A. A systematic review of sex differences in concussion outcome: What do we know? Clin Neuropsychol 2019; 33(6):1016–1043. [DOI] [PubMed] [Google Scholar]
- 10.Ozinga S, Linder S, Koop M, et al. Normative performance on the Balance Error Scoring System by youth, high school, and collegiate athletes. J Athl Train 2018; 53(7):636–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Benedict P, Baner N, Harrold G. Gender and age predict outcomes of cognitive, balance and vision testing in a multidisciplinary concussion center. J Neurol Sci 2015; 353(1–2):111–115. [DOI] [PubMed] [Google Scholar]
- 12.Sufrinko A, Mucha A, Covassin T, et al. Sex differences in vestibular/ocular and neurocognitive outcomes after sport-related concussion. Clin J Sport Med 2017; 27(2):133–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Oldham J, DiFabio M, Kaminski T, et al. Efficacy of Tandem Gait to Identify Impaired Postural Control Following Concussion. Med Sci Sport Exerc 2018; 50(6):1162–1168. [DOI] [PubMed] [Google Scholar]
- 14.Howell D, Osternig L, Chou L. Single-task and dual-task tandem gait test performance after concussion. J Sci Med Sport 2017; 20(7):622–626. [DOI] [PubMed] [Google Scholar]
- 15.Echemendia RJ, Meeuwisse W, McCrory P, et al. The Sport Concussion Assessment Tool 5th Edition (SCAT5). Br J Sport Med 2017; 51. [DOI] [PubMed] [Google Scholar]
- 16.Howell D, Wilson J, Brilliant A, et al. Objective clinical tests of dual-task dynamic postural control in youth athletes with concussion. J Sci Med Sport 2018; Epub ahead. [DOI] [PubMed] [Google Scholar]
- 17.Howell D, Stracciolini A, Geminiani E, et al. Dual-task gait differences in female and male adolescents following sport-related concussion. Gait Posture 2017; 54:284–289. [DOI] [PubMed] [Google Scholar]
- 18.SCAT3. Br J Sports Med 2013; 47:259–263. [PubMed] [Google Scholar]
- 19.Oldham JR, DiFabio MS, Kaminski TW, et al. Normative Tandem Gait in Collegiate Student-Athletes: Implications for Clinical Concussion Assessment. Sports Health 2017; 9(4). Doi: 10.1177/1941738116680999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schneiders AG, Sullivan SJ, Gray AR, et al. Normative values for three clinical measures of motor performance used in the neurological assessment of sports concussion. J Sci Med Sport 2010; 13(2):196–201. Doi: 10.1016/j.jsams.2009.05.004. [DOI] [PubMed] [Google Scholar]
- 21.Steindl R, Kunz K, Schrott-Fischer A, et al. Effect of age and sex on maturation of sensory systems and balance control. Dev Med Child Neurol 2006; 48:477–482. [DOI] [PubMed] [Google Scholar]
- 22.Frommer L, Gurka K, Cross K, et al. Sex differences in concussion symptoms of high school athletes. J Athl Train 2011; 46(1):76–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Black A, Sergio L, Macpherson A. The Epidemiology of Concussions: Number and Nature of Concussions and Time to Recovery Among Female and Male Canadian Varsity Athletes 2008 to 2011. Clin J Sport Med 2017; 27(1):52–56. [DOI] [PubMed] [Google Scholar]
- 24.Howell D, Oldham J, Lanois C, et al. Dual-Task Gait Recovery after Concussion among Female and Male Collegiate Athletes. Med Sci Sport Exerc 2020; Epub ahead. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kerr Z, Zuckerman S, Wasserman E, et al. Concussion symptoms and return to play time in youth, high school, and college American football athletes. JAMA Pediatr 2016; 170(7):647–653. [DOI] [PubMed] [Google Scholar]
- 26.Valovich McLeod T, Hale T. Vestibular and balance issues following sport-related concussion. Brain Inj 2015; 29(2):175–184. [DOI] [PubMed] [Google Scholar]
- 27.Pearce K, Sufrinko A, Lau B, et al. Near point of convergence after a sport-related concussion measurement reliability and relationship to neurocognitive impairment and symptoms. Am J Sport Med 2015; 43(12):3055–3061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Henry L, Elbin R, Collins M, et al. Examining recovery trajectories after sport-related concussion with a multimodal clinical assessment approach. Neurosurgery 2016; 78(2):232–241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Howell D, O’Brien M, Raghuram A, et al. Near point convergence and gait deficits in adolescents after sport-related concussion. Clin J Sport Med 2018; 28(3):262–267. [DOI] [PubMed] [Google Scholar]
- 30.Cossette I, Gagne M, Ouellet M, et al. Executive dysfunction following a mild traumatic brain injury revealed in early adolescence with locomotor-cognitive dual-tasks. Brain Inj 2016; 30(13–14):1648–1655. [DOI] [PubMed] [Google Scholar]
- 31.Lax I, Paniccia M, Agnihotri S, et al. Developmental and gender influences on executive function following concussion in youth hockey players. Brain Inj 2015; 29(12):1409–1419. [DOI] [PubMed] [Google Scholar]
- 32.Yogev-Seligmann G, Rotem-Galili Y, Mirelman A, et al. How does explicit prioritization alter walking during dual-task performance? Effects of age and sex on gait speed and variability. Phys Ther 2010; 90(2):177–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Stolze H, Kuhtz-Buschbeck J, Mondwurf C, et al. Retest reliability of spatiotemporal gait paramters in children and adults. Gait Posture 1998; 7(2):125–130. [DOI] [PubMed] [Google Scholar]
- 34.Schneiders AG, Sullivan SJ, McCrory PR, et al. The effect of exercise on motor performance tasks used in the neurological assessment of sports-related concussion. Br J Sports Med 2008; 42(12):1011–1013. Doi: 10.1136/bjsm.2007.041665. [DOI] [PubMed] [Google Scholar]
- 35.Howell D, Brilliant A, Meehan III W. Tandem Gait Test-Retest Reliability Among Healthy Child and Adolescent Athletes. J Athl Train 2019; 54(12):Online Ahead of Print. [DOI] [PMC free article] [PubMed] [Google Scholar]