

Abstract
Background
Most patients have high expectations about restoration of the knee function after TKA, expecting a more active life after retirement. However, 20% to 30% of patients report that their expectations are not met postoperatively. Among those unmet expectations may be the anticipation to engage in sexual activity after surgery, but few studies have evaluated sexual activity after arthroplasty.
Questions/purposes
In this study, our purposes were (1) to evaluate the anticipation and the fulfillment of sexual activity after TKA in men and women, and (2) to identify prognostic factors for the fulfillment of anticipated postoperative sexual activity.
Methods
This was a prospective, multicenter study of all 1371 patients scheduled for TKA between June 2012 and July 2015. The study was part of the Longitudinal Leiden Orthopaedics Outcomes of Osteoarthritis Study (LOAS). After screening according to LOAS inclusion criteria, 1213 respondents remained. Our primary study endpoint was whether sexual expectations were met 1 year after TKA; we used the sexual-activity-expectation question from the Hospital for Special Surgery (HSS) Knee Replacement Expectations Survey, which allows the patient to score the result on a 5-point scale. To assess postoperative fulfillment of sexual activity 1 year after TKA, we asked the patient to score the current status of sexual activity on the same 5-point scale: 1 (back to normal), 2 (large improvement), 3 (moderate improvement), 4 (slight improvement), and 5 (does not apply). Patients with incomplete data on the preoperative expectation- and postoperative fulfillment-question of sexual activity were excluded, leaving 71% (866 of 1213) patients for analysis. The difference between the pre- and postoperative scores determined whether expectations of sexual activity were unfulfilled (lower than expected) or fulfilled/exceeded (neutral or higher than expected). Pre- and postoperatively, the Knee Injury and Osteoarthritis Outcome Score (KOOS), the Short Form-12 Mental and Physical Component Summary scores (SF-12 MCS and SF-12 PCS), the EuroQoL-5 Dimensions (EQ-5D), and the EQ-5D VAS scale were used. Multivariate regression models were used for analysis.
Results
Preoperatively, 54% patients (467 of 866) anticipated postoperative sexual activity after recovery from surgery. Both genders showed that the proportion who anticipated “back to normal” sexual activity decreased with higher age. Likewise, postoperative fulfillment of anticipated sexual activity was found in 58% (111 of 191 for men; 159 of 276 for women). Younger women (younger than 65 years of age) experienced fulfillment more often compared with younger men. A positive postoperative change in functional and health status was associated with fulfilled/exceeded scores of patients anticipating postoperative sexual activity. A better preoperative health status, the EQ-5D VAS score (odds ratio [OR] 1.02 [95% CI 1.01 to 1.03]; p = 0.006), was associated with a higher likelihood of fulfillment of anticipated postoperative sexual activity.
Conclusion
In both men and women, two of five patients who anticipated postoperative sexual activity indicated that their expectation of sexual activity was not met 1 year after TKA. These patients had worse functional recovery scores compared with patients who achieved the anticipated level of sexual activity. The latter is associated with functional recovery. Surgeons should be aware that many patients anticipate restoration of normal sexual activity, and that this may be the expectation for patients of all ages and for women and men alike. The results underscore the need for more qualitative research to understand this topic in greater depth.
Level of Evidence
Level II, therapeutic study.
Introduction
Sexual activity is an important aspect of quality of life during all ages [3, 33, 53]. Older patients today expect to remain active, and this includes sexual activity [37], but their ability to do so may be seriously limited by osteoarthritis (OA) [27]. Although TKA improves knee pain for many patients and implant durability is generally good [8, 9, 37], as much as 20% of patients have persistent limitations after recovery [9, 30, 37, 48].
Patients’ expectations about functional restoration of the knee after TKA are high [34], but they go unmet in 20% to 30% of patients [47, 48, 52]. Among those unmet expectations is the expectation to engage in sexual activity after surgery [36, 43, 47]. Although sexual activity is important to quality of life for men and women, few studies have evaluated this topic [27, 39, 40]. In 45% of patients, sexual activity was limited because of the knee [27], and 44% of the TKA population rated improvement of postoperative sexual activity as important [28, 36, 52]. However, it is uncommon for surgeons and patients to discuss this topic during a preoperative consultation [19, 27, 29, 50], even though patients expect surgeons to address the issue of sexual activity as it relates to knee complaints [27, 46].
We therefore sought (1) to evaluate the anticipation and the fulfillment of sexual activity after TKA in men and women, and (2) to identify prognostic factors for the fulfillment of anticipated postoperative sexual activity.
Patients and Methods
Study Design
This was a prospective, multicenter study of primary TKA patients. The study was part of the Longitudinal Leiden Orthopaedics Outcomes of Osteoarthritis Study (LOAS) [31, 45]. The LOAS study is an ongoing multicenter, longitudinal, prospective cohort study designed to determine long-term, patient-reported outcomes (PROs) in THA and TKA (Trial ID NTR3348).
Setting
In the present study, we considered as potentially eligible all patients scheduled for primary TKA recruited in seven participating hospitals [31, 45], which were all located in the urban Randstad region of the Netherlands. Participating hospitals included five general hospitals (each around 300 beds), one university (882 beds) and one teaching hospital (around 500 beds).
Participants
Patients were eligible for the study if they were diagnosed with primary knee OA and scheduled for TKA. We excluded patients who were younger than 18 years of age, who did not understand the Dutch language, who were physically or mentally unable to complete questionnaires, who were undergoing revision surgery, hemiarthroplasty, or TKA because of tumor or rheumatoid arthritis, and those with the inability or unwillingness to provide informed consent [31]. Eligible patients were informed about the study through written and oral information by their treating medical specialist at the outpatient clinic. Only patients who agreed to be approached by the researcher received additional written information about the study by regular mail, as well as a questionnaire, a stamped return envelope, and an informed consent form. Patients who did not return their preoperative questionnaire within 1 week were contacted by telephone [31]. Patients were included once written informed consent was obtained according to the Declaration of Helsinki. For this analysis, we only included data from patients who had completed the item on sexual activity in both pre- and postoperative questionnaires. Ethical approval was granted by the Medial Ethics Committee of the Leiden University Medical Center (LUMC, registration number P12.047).
Between June 2012 and July 2015, a total of 1371 patients were scheduled for TKA. After screening with LOAS inclusion criteria, 1213 were enrolled in the LOAS study. In total, 1138 participants (94%) completed the preoperative Hospital for Special Surgery (HSS) Knee Replacement Expectations Survey item on sexual activity. Patients with postoperative incomplete sexual activity data were excluded, leaving 71% (866 of 1213) patients for analysis (Fig. 1). Postoperative follow-up was carried out approximately 1 year after TKA (median 397 days; interquartile range 380 to 421 days).
Fig. 1.
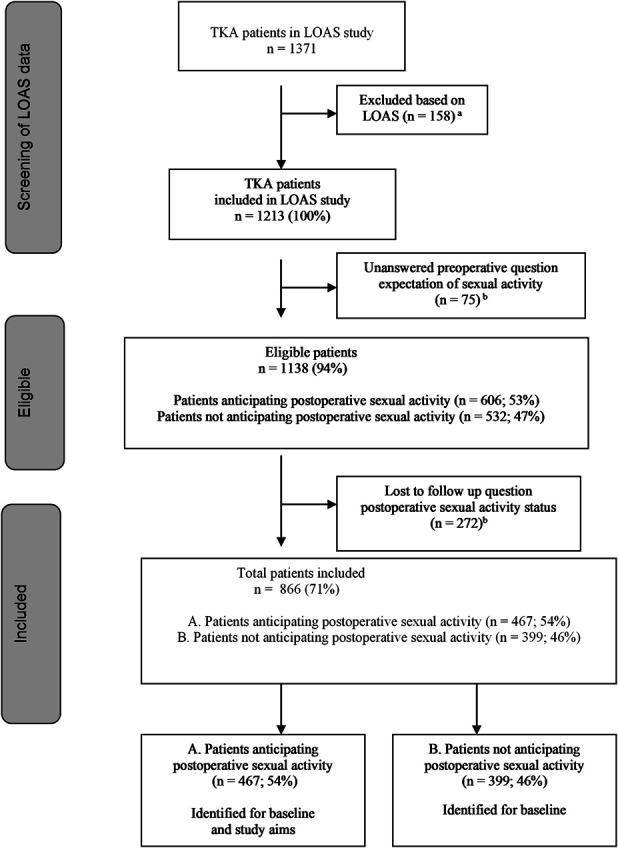
A flowchart of the study is shown here. The study included two subgroups: Patients anticipating and not anticipating postoperative sexual activity. aLOAS exclusion criteria: younger than18 years of age, inability to understand Dutch language, physical or mental inability to complete questionnaires, revision surgery, hemiarthroplasty, TKA because of tumor or rheumatoid arthritis, or inability or unwillingness to provide informed consent. bExclusion: no answer in response to preoperative and/or postoperative HSS question on sexual activity.
Data comparison of included and excluded patients showed no differences in terms of patients’ characteristics. With regard to functional and health status, we found some differences in 5 out of 11 variables. On these items, included patients showed slightly better results compared to excluded patients: respectively mean ± SD, for KOOS pain, 39 ± 18 compared with 36 ± 19; p = 0.028; KOOS ADL, 45 ± 18 compared with 43 ± 20; p = 0.039; for SF-12 MCS, 56 ± 9 compared with 54 ± 10; p = 0.003; for EQ-5D, 0.65 ± 24 compared with 0.60 ± 26; p = 0.001, and for EQ-5D VAS, 69 ±17 compared with 64 ± 19; p < 0.001.
Assessments
Sociodemographic Characteristics
Preoperatively, we collected patient characteristics, including self-reported age, gender, weight (kg) and height (m) to calculate the BMI. Living status was collected as: partner “yes” or “no”, “unknown”/ “missing.”
Comorbidities
Preoperative comorbidity information was gathered by self-report, based on standardized items developed and used by Statistics Netherlands [10, 11], asking for the presence or absence of 19 different comorbidities in the previous year, which were categorized in two domains: musculoskeletal or non-musculoskeletal comorbidities. Comorbidities were summed within each of these categories and dichotomized as follows: presence (one or more comorbidity within this domain) or absence (no comorbidities within the domains) [32, 42]. Musculoskeletal comorbidities were: severe back pain (including slipped disc); severe neck or shoulder pain; severe elbow, wrist or hand pain; and, other chronic rheumatic diseases. Non-musculoskeletal comorbidities were asthma or chronic obstructive pulmonary disease; severe cardiac disorder or coronary disease; arteriosclerosis (abdomen or legs); hypertension; the consequences of stroke; severe bowel disorder; diabetes mellitus; migraine; psoriasis; chronic eczema; cancer; urinary incontinence; sensory impairments, such as hearing impairments during group and face-to-face conversation; short- and long-distance vision impairments; dizziness in combination with falling. Data were gathered at baseline.
Functional Status and Health Status
To assess knee-related functional status, we used the Knee Injury and Osteoarthritis Outcome Score (KOOS; scale 0 to 100), and its sub-domains: KOOS Activities of Daily Living (ADL); KOOS Pain; KOOS Quality of Life (QoL); KOOS Sport; KOOS Symptoms [6]. To assess health status, we used the Short Form-12 Mental and Physical Component Summary (SF-12 MCS and SF-12 PCS, scale 0 to 100) [12, 23], the EuroQoL-5 Dimensions (EQ-5D, scale 0 to 1), and the EQ-5D VAS (scale 0 to 100) [51]. For all functional and health status scores, higher scores indicate better functioning or less pain. Data were gathered at baseline and follow-up.
Preoperative Expectation of Sexual Activity
Our primary study endpoint was whether sexual expectations were met 1 year after TKA. We used a single question from the validated Dutch translation [1] of the HSS Knee Replacement Expectation Survey [35, 55]: the expectation of sexual activity after surgery, which allows the patient to score the result on a 5-point scale: 1 (back to normal), 2 (large improvement), 3 (moderate improvement), 4 (slight improvement), and 5 (does not apply) [1]. In the analysis of preoperative data, answers to this item were categorized into two subgroups: those who before surgery anticipated sexual activity after TKA (score 1 to 4), and those with score 5 who did not anticipate sexual activity (choosing the answer “does not apply”). Only the data of patients who anticipated sexual activity (score 1 to 4) were used for analysis of postoperative fulfillment of anticipated sexual activity.
Postoperative Fulfillment of Expectation of Sexual Activity
The study endpoint was whether expectations were met regarding anticipated sexual activity 1 year after TKA. To measure expectation fulfillment, the preoperative HSS questionnaire was modified for use in longitudinal LOAS research. This postoperative equivalent of the (preoperative) HSS questionnaire was based on the same 17 items and was composed of the same 5-point scale. Only the heading of the questionnaire was changed: asking the patient to report the “actual status” of the 17 function/activities (such as, sexual activity). Patients were not reminded of their preoperative responses.
We calculated “fulfillment of anticipated postoperative sexual activity” by subtracting the postoperative score (the current status regarding sexual activity) from the preoperative anticipated score of sexual activity. A negative score (≤ -1) indicated less improvement than expected and was categorized as “unfulfilled.” A neutral score (0) and a “greater than expected” score (≥ 1) indicated a score as predicted or that expectations were exceeded. The latter two categories were collapsed and labeled “fulfilled/exceeded.”
Statistical Analyses
We analyzed and stratified the data to gender and in four age groups: ≤ 60 years, 61 to 65 years, 66 to 70 years, ≥ 71 years. To assess potential selection bias due to attrition, we compared the following baseline characteristics: age, sex, BMI, living status, comorbidities, all KOOS (total) domains, SF-12 PCS and SF-12 MCS of the included and excluded patients.
To address our first research purpose, we evaluated differences in baseline characteristics in patients anticipating and not anticipating postoperative sexual activity (Table 1). Armitage’s trend test was used for ordinal categorical variables and Pearson’s chi-square test for nominal categorical variables. We evaluated anticipated postoperative sexual activity by age groups and gender (Table 2).
Table 1.
Preoperative patient characteristics

Table 2.
Preoperative anticipations of sexual activity per age group and in men and women

Pearson’s chi-square test (categorical variables), and independent samples t-test (continuous variables) were used to evaluate whether patients with fulfilled anticipations on postoperative sexual activity have different preoperative characteristics for age, gender, baseline functional status, baseline health status, and comorbidity status compared with patients with unfulfilled expectations (Table 3).
Table 3.
Postoperative fulfillment in patients anticipating postoperative sexual activity related to baseline

To assess whether fulfillment of the anticipated postoperative sexual activity was associated with changes in postoperative functional and health status, we used the Armitage’s trend test for ordinal categorical variables and the independent sample t-test for continuous variables. To assess clinical relevance, we used the minimal clinical important differences (MCID); we used MCID 9.1 points for KOOS (total) domains [44]; MCID 4.5 points for SF-12 MCS and PCS [5, 12], and MCID 0.074 points for EQ-5D [51] (Table 4).
Table 4.
Fulfillment related to pre- and postoperative functional and health status recovery

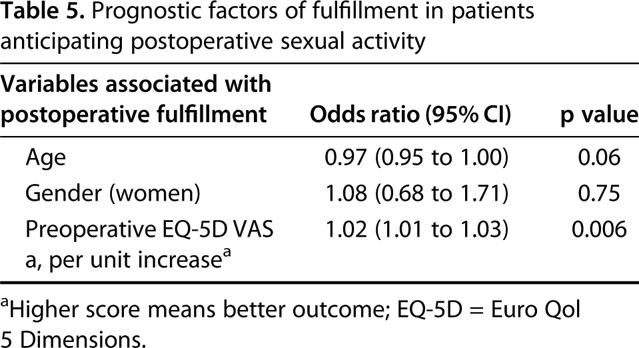
To address our second research purpose, we evaluated prognostic factors for the fulfillment of anticipated postoperative sexual activity using a binary logistic regression analysis with backward Wald selection (Table 5). Age (as a continuous variable) and gender were included in the models, irrespective of statistical significance. For the selection of covariates for the multivariate logistic regression, we performed a univariate test for BMI, living status, all (preoperative) KOOS (total) domains, the SF-12 MCS, the SF-12 PCS, and the EQ-5D scores, including EQ-5D VAS. We selected covariates for multivariate modeling if the univariate p value was less than 0.10 [49]. The level of significance for removing variables in the backward selection in the multivariate analyses was set at p < 0.05.
Table 5.
Prognostic factors of fulfillment in patients anticipating postoperative sexual activity
Statistical analyses were performed with SPSS Statistics version 24 for Windows/Mac (IBM Corp, Armonk, NY, USA).
Results
Anticipation of Sexual Activity After TKA and Fulfillment of Expectations
What Are the Differences in the Baseline Characteristics Between Patients Anticipating and not Anticipating Postoperative Sexual Activity?
Overall, few differences were found between the patients who anticipated in engaging postoperative sexual activity (54%, 866 of 467) and the patients who did not (46%, 399 of 866). The group who anticipated postoperative sexual activity consisted of younger respondents and fewer females (age 65 years ± 8 and 59%, [276 of 467] women) compared with the group who did not anticipate sexual activity (age 70.0 years ± 8 and 75% [298 of 399] women). Living status, BMI, and baseline functional and health status scores were similar between both groups, except that those with less pain (higher KOOS pain score) were more likely to expect postoperative sexual activity. This group also reported 10% less non-musculoskeletal comorbidities (70%, 279 of 398) compared with those not anticipating postoperative sexual activity (81%, 255 of 315; p = 0.001) (Table 1).
In terms of gender, men more often had expectations regarding postoperative sexual activity: 35% (101 of 292) compared with 52% (298 of 574) of women were expecting “does not apply,” p < 0.001 (Table 2). And, in all age groups, more men expected a “back to normal” sexual activity after surgery, with the highest number in patients who were ≤ 60 years old; for men, 60% (33 of 55; p = 0.004) expected to return to normal and for women, 47% (58 of 124; p < 0.001) expected to return to normal. Both genders showed that anticipating “back to normal” sexual activity slightly decreased with higher age (Table 2).
Which Patient Characteristics Are Related to Fulfillment?
We did not find differences between the genders in terms of fulfilled expectations regarding sexual activity. Forty-two percent of men 42% (80 of 191) and 42% women (117 of 276) did not have their expectations met; 58% of men (111 of 191) and 58% of women (159 of 276) said that their expectations were fulfilled. Fulfillment of anticipation was slightly less frequently achieved in higher age groups. Patients with fulfilled/exceeded expectations had better baseline function and health status scores compared with those with unfulfilled anticipation, respectively mean ± SD: for KOOS ADL, 44 ± 19 versus 47 ± 17; p = 0.019; for SF12 -MCS, 54 ± 10 versus 57 ± 8; p = 0.006; and for EQ-5D VAS, 67 ± 16 versus 71 ±17; p = 0.026. Of the patients with musculoskeletal comorbidities, more patients were fulfilled/exceeded: 57% (85 of 150) compared with unfulfilled (43% [65 of 150]; p = 0.205). For the non-musculoskeletal comorbidity patients, the results were similar (Table 3).
Do Patients with Fulfilled Expectations Have a Better Postoperative Functional and Health Status?
Postoperatively, patients with fulfilled/exceeded expectations had better functional and health status after TKA than those with unfulfilled anticipations. Calculating the change between the patients’ pre- and postoperative KOOS-total items, we found better functional status for all KOOS subscales for the fulfilled/exceeded group compared with the unfulfilled group. The differences exceeded the MCID norm, indicating clinically relevant differences (norm MCID 9.1). Differences between patients with and without fulfilled anticipations were largest for KOOS-Sport, mean 14 ± 0; but also high for KOOS-ADL: mean 11 ± 7 and KOOS-Pain mean 11 ± 6. When calculating the change between pre- and postoperative health status scores (SF-12 PCS, EQ-5D, EQ-5D VAS), we also found differences between both groups in postoperative results, but this did not exceed MCID norms (Table 4).
Prognostic Factors Regarding Anticipation of Postoperative Sexual Activity
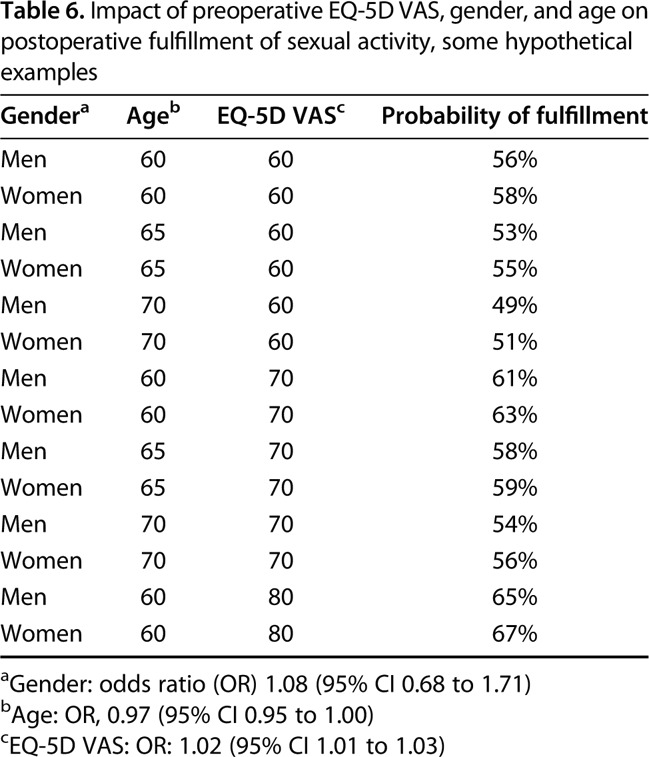
An increasing preoperative EQ-5D VAS score was the only prognostic factor we identified that was associated with an increased likelihood of fulfilled anticipation of sexual activity, one year after TKA, but the effect size was very small (odds ratio [OR] 1.02 [95% CI 1.01 to 1.03]) (Table 5). Some hypothetical examples are calculated. For instance, a 60-year-old male patient with an EQ-5D VAS score of 60 has a probability of expectation fulfillment of 56% while a 65-year-old female with an EQ-5D VAS score of 70 has a probability of expectation fulfilment of 59% (Table 6). The c-statistic of our model was 0.61 (fairly low).
Table 6.
Impact of preoperative EQ-5D VAS, gender, and age on postoperative fulfillment of sexual activity, some hypothetical examples
Discussion
Sexual activity is an important aspect of quality of life, even more, since a new generation of active seniors expects more quality of life after retirement [27, 37]. Return to (normal) sexual activity may be an important goal for many TKA patients [27, 40], and the likelihood of achieving this goal may depend on how successful the surgery is in terms of overall pain relief [37]. We sought to evaluate expectation fulfillment and prognostic factors associated with sexual activity 1 year after TKA. Using a large, prospective cohort study, we additionally explored patients’ characteristics and PROs, in depth. We found that before surgery, men more often expected a return to normal sexual activity: 46% compared with 32% women anticipated (back to normal) sexual activity after surgery. As expected, anticipation decreased with increasing age, both for men and women. In our study, a high proportion of patients experienced unfulfilled expectations of sexual activity after surgery (approximately 40% for both men and women), a frequency that was much higher than one previous study, which found that proportion to be about 25% [47]. Our findings suggest that this topic deserves greater attention during presurgical consultation [38, 39].
Limitations
Patients with incomplete follow-up on fulfillment of sexual activity anticipations were excluded, but statistical testing between included and excluded respondents showed no differences in patient characteristics (such as, age, gender, preoperative functional, and health status), suggesting that selection bias was not likely to be a severe limitation of our study. There were, however, other important limitations. First, the assessment of preoperative anticipation and its fulfillment of sexual activity were limited to one item of the validated HSS Knee Replacement Expectations Survey. Even though the HSS questionnaire has been validated as a 17-item instrument, the reliability of extracting one item is unknown [6, 23, 51]. In single-subject research, prior studies have recommended the use of multi-item questionnaires [7, 22]. In our LOAS cohort, we aim to cover all International Classification of Functionality aspects of a person. Consequently, validated instruments for functional and health status recovery (pre- and postoperative stage) were employed in this prospective, single-subject study on sexual activity. Second, this is an exploratory study on sexual activity anticipation in TKA patients, a sensitive topic that is not frequently studied [4, 18]. Although we evaluated a large group of patients, we note that PROs are subjective. Even so, PRO research is increasingly being seen as important [15, 17, 25]. A related limitation is the use of the HSS questionnaire as a postoperative instrument [35]. Originally, the HSS questionnaire was developed for preoperative assessment of expectations and for communication in preoperative consultations, but not for assessment of postoperative expectation fulfillment [35]. Our approach, although not formally validated, was used before by other studies that measured postoperative anticipation fulfillment [36, 41, 43, 47], and we believe it has strong face validity. Still, this procedure could have reduced the reliability of this study [55].
Furthermore, the original HSS Knee Replacement Expectations Survey contains a “does not apply” and “I do not expect this” response option [26, 35]. And, over time the HSS changed and combined both scores to a single “does not apply” option [1, 2, 36], which is also in the validated Dutch version [1]. Related to this is the lack of exact definitions for answering options as “back to normal” and “does not apply.” The HSS answers may have been subject to multiple interpretations [20]. Patients may have had multiple reasons to fill in “does not apply,” such as not knowing how to answer or having expectations that were lower than the available scoring options (for example, expecting to worsen or not to improve) [47]. It also could be that sexually active patients without a preoperative expectation filled in this option because they do not anticipate a change in their sexual activity status. We therefore excluded the data of the respondents who filled in “does not apply” for further analysis [13].
Finally, the proportion of patients with unfulfilled expectations may be overrepresented, because a control or comparison non-TKA group was not surveyed. In addition, the current study is sufficiently generalizable to the Dutch population with symptomatic end-stage knee osteoarthritis who were scheduled for TKA. However, global generalizability is limited because of cultural differences on sexual activity [47]. For that matter, baseline information on patients’ sexual activity would make comparison with different populations possible; however, we did not collect this baseline.
Preoperative Expectations Regarding Sexual Activity and its Fulfillment
Several studies evaluated preoperative expectations of TKA in patients [13, 24, 35, 36, 43, 47, 54], but only three specifically reported on sexual activity [36, 43, 47]. Two of them compared preoperative expectation of sexual activity to postoperative fulfillment of expectation (measured with HSS survey) [43, 47]; and one related preoperative expectation of sexual activity (HSS) to postoperative satisfaction (with a self-developed instrument) [36]. But compared with the current study, these studies were smaller and the data on sexual activity were incomplete. Another prospective study found a proportion of 24% unfulfilled preoperative expectations of sexual activity 1 year after TKA compared with 42% in the current study [47]; these differences might be due to the fact that the data on the issue of sexual activity were incomplete as well. The two other studies [36, 43], which measured the “importance” of the expectation score, reported about sexual activity as the least important expectation. In one study, 63% of respondents did not report sexual activity (HSS questionnaire) [36] which may have influenced the findings. And, the other study gathered complete data, but in this study, patients considered sexual activity to be least important as well, although fulfillment was greater than expected [43]. Basic topics as “relief of pain,” “ability to walk,” “ability to put on shoes and socks,” even “psychological well-being” always will be of more importance compared with items such as “sexual activity” or “monetary reimbursement” (both not applying to every respondent) [36, 54]. Consequently, Cross et al. [13] found that the preoperative mean importance score of sexual activity (based on a follow-up time of 6 months) increased substantially after excluding the “does not apply” patients. This is important to know when investigating “less important issues.” Besides, it is known that the new generation of patients has higher expectations towards regaining high-level (leisure) activities [16, 37]. If studies continue counting “does not apply” answers (or “missing data”) in calculating mean results for entire samples, a clear picture of the impact of TKA on that specific issue will not be obtained, and consequently, it will not be recognized for achieving better quality care for patients.
With respect to the diversity of studies describing the patients’ pre- and postoperative functional and health status and preoperative expectations [13, 24, 35, 43, 47, 54], no study to our knowledge has looked to postoperative fulfilled or unfulfilled expectation per subgroup and related results to the change in the patients’ postoperative recovery, as we did. No study to our knowledge further calculated MCID between both subgroups (fulfilled and unfulfilled), but this study did and found high levels above the MCID norm for all KOOS functional variables.
Prognostic Factors for Fulfillment of Expectations and Implications for Practice
Our study shows that the baseline EQ-5D VAS score was the most important prognostic factor for fulfillment of anticipated postoperative sexual activity. Others have studied prognostic factors for a broader set or more generic expectations; these studies found prognostic factors in mainly the baseline functional area, such as KOOS Quality of Life [21]. Surgeons should be aware when patients’ anticipation of postoperative sexual activity is unfulfilled, especially in patients with postoperative low functional recovery. When we compared this study with our previous study in THA patients, we found similar results (in both, there were approximately 40% of unfulfilled expectations in patients anticipating postoperative sexual activity, regardless of gender) [20]. This finding needs further research in both populations.
Another study compared the postoperative knee function of TKA patients to age- and gender-matched controls [52]. This study showed that sexual activity was deemed important in 70% of TKA subjects versus 67% of controls, and that control participants also reported a certain continuous deterioration of knee function. However, in regard to sexual activity, the control participants more often felt unrestricted (86%) compared with the TKA patients (64%, 1 year postoperative) [52]. When activities become more demanding, the gap between the controls and the TKA population widened, with four times as many difficulties when it came to activities like squatting and kneeling for the TKA population. Referring to the common sexual positions of Dahm et al. [14], a considerable number of these positions call for kneeling or squatting. It may be that patients with unfulfilled anticipations were mainly hindered by functional limitations, such the ability to kneel and squat, during more-demanding sexual activities. Although this aspect of functional limitations related to sexual activity needs more study, it may be relevant to patients to be educated about comfortable and safe sexual positions after TKA. It is not common for patients and surgeons to talk explicitly about sensitive issues such as these [14, 19, 50], and perhaps because of this omission, patients may set unrealistic expectations preoperatively. Patient education tailored to the needs of patients and partners may help establish realistic expectations. More knowledge of patients’ preoperative anticipation of sexual activity and postoperative fulfillment may help surgeons to provide adequate patient education, which may improve care quality and patient satisfaction.
Conclusions
Regardless of gender, we found that about two of five patients who anticipated postoperative sexual activity indicated that their expectations were not met 1 year after TKA. These patients had worse functional recovery scores compared with patients who achieved the anticipated level of sexual activity. Surgeons should be aware that many patients anticipate postoperative sexual activity, and that this applies to patients of all ages, and for women and men alike. The results underscore the importance of more qualitative research to clarify this important and infrequently discussed topic in orthopaedic practice.
Acknowledgments
We thank PhD candidate Claudia Leichtenberg, as a former member of the LOAS study Group, for her help collecting the data.
Footnotes
The institution of one or more of the authors (RTEH) has received, during the study period, funding from the Dutch Arthritis Association (LLP13).
Each author certifies that neither he or she, nor any member of his or her immediate family, have funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
This work was performed at the Departments of Orthopaedics and Biomedical Data Sciences, Leiden University Medical Center, Leiden, the Netherlands.
The LOAS Study Group includes: T. P. M. Vliet-Vlieland MD, PhD, H. M. J. van der Linden-van der Zwaag MD, PhD, B. L. Kaptein PhD, R. Onstenk MD, S. H. M. Verdegaal MD, PhD, S. B. W. Vehmeijer MD, PhD, H. H. Kaptijn MD, W. J. Marijnissen MD, PhD , P. J. Damen MD.
References
- 1.Akker-Scheek van den I, Van Raay JJ, Reininga IH, Bulstra SK, Zijlstra W, Stevens M. Reliability and concurrent validity of the Dutch hip and knee replacement expectations surveys. BMC Musculoskelet Disord . 2010;11:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Balck F, Kirschner S, Jeszenszky C, Lippmann M, Gunther K-P. Validity and Reliability of the German Version of the HSS Expectation Questionnaire on Hip Joint Replacement. Z Orthop Unfal.l 2016;154:606–611. [DOI] [PubMed] [Google Scholar]
- 3.Beckman N, Waern M, Östling S, Sundh V, Skoog I. Determinants of sexual activity in four birth cohorts of Swedish 70-year-olds examined 1971-2001. J Sex Med . 2014;11. [DOI] [PubMed] [Google Scholar]
- 4.Bell S, Reissing ED, Henry LA, VanZuylen H. Sexual activity after 60: A systematic review of associated factors. Sex Med Rev . 2017;5. [Google Scholar]
- 5.Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley Award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res . 2016;474:321–329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res . 2017;475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bierman AS1, TA B, Fisher ES, Wasson JH. How well does a single question about health predict the financial health of Medicare managed care plans? Eff Clin Pract . 1999;2:56–62. [PubMed] [Google Scholar]
- 8.Bloomfield MR, Hozack WJ. Total hip and knee replacement in the mature athlete. Sports Health . 2014;6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, Beard DJ. Knee replacement. Lancet . 2012;379:1331–1340. [DOI] [PubMed] [Google Scholar]
- 10.Central Bureau Statistics The Netherlands. Netherlands pilot project on morbidity statistics. Report. Available at: https://www.cbs.nl/en-gb/background/2012/11/netherlands-pilot-project-on-morbidity-statistics. Accessed March 14, 2012. [Google Scholar]
- 11.Central Bureau Statistics The Netherlands. Health lifestyle and the use of health care, 2000 - 2009. Report. Available at: https://opendata.cbs.nl/Dataportaal/index.html#/CBS/nl/dataset/03799/table?ts=1533812926590. Accessed October 16, 2016. [Google Scholar]
- 12.Clement ND, MacDonald D, Simpson AHRW. The minimal clinically important difference in the Oxford knee score and Short Form 12 score after total knee arthroplasty. Knee Surgery, Sport Traumatol Arthrosc . 2014;22:1933–1939. [DOI] [PubMed] [Google Scholar]
- 13.Cross M, Lapsley H, Barcenilla A, Parker D, Coolican M, March L. Patient expectations of hip and knee joint replacement surgery and postoperative health status. Adis Data Inf BV (original Res Artic. 2009;2:51–60. [DOI] [PubMed] [Google Scholar]
- 14.Dahm DL, Jacofsky D, Lewallen DG. Surgeons rarely discuss sexual activity with patients after THA; a survey of members of the American Association of Hip and Knee Surgeons. Clin Orthop Relat Res . 2004;428:237–240. [PubMed] [Google Scholar]
- 15.Franklin PD, Lewallen D, Bozic K, Hallstrom B, Jiranek W, Ayers DC. Implementation of patient-reported outcome measures in U.S. total joint replacement registries: rationale, status, and plans. J Bone Joint Surg Am . 2014;96:104–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ghomrawi HMK, Ferrando NF, Mandl LA, Do H, Noor N, Gonzalez Della Valle A, Gonzalez A, Valle D. How often are patient and surgeon recovery expectations for total joint arthroplasty aligned? Results of a pilot study. HSS J . 2011;7:229–234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gioe TJ, Pomeroy D, Suthers K, Singh JA. Can patients help with long-term total knee arthroplasty surveillance? Comparison of the American Knee Society Score self-report and surgeon assessment. Rheumatology . 2009;48:160–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Harmsen RTE, Haanstra TM, Sierevelt IN, Jansma EP, Nolte PA, Wall PDH, Van Royen BJ. Does total hip replacement affect sexual quality of life? BMC Musculoskelet Disord . 2016;198:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Harmsen RTE, MPJ Nicolai, Den Oudsten BL, Putter H, Haanstra TM, Nolte PA, Van Royen BJ, Elzevier H. Patient sexual function and hip replacement surgery: A survey of surgeon attitudes. Int Orthop . 2017;41:2433-2445. [DOI] [PubMed] [Google Scholar]
- 20.Harmsen RTE, Den Oudsten BL, Putter H, Leichtenberg CS, LOAS Group S, Elzevier HW, Nelissen RGHH. Patient expectations of sexual activity after total hip arthroplasty. JBJS Open Access.2018;0:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hepinstall MS, Rutledge JR, Bornstein LJ, Mazumdar M, Westrich GH. Factors that impact expectations before total knee arthroplasty. J Arthroplasty . 2011;26:870–876. [DOI] [PubMed] [Google Scholar]
- 22.Hulscher JBF, de Haes JCJM, Sprangers MAG, van Sandick JW, Stalmeier PFM, de Boer AGEM, van Lanschot JJB. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual Life Res . 2004;13:311–320. [DOI] [PubMed] [Google Scholar]
- 23.Hurst NP, Ruta DA, Kind P. Comparison of the MOS short form-12 (SF12) health status questionnaire with the SF36 in patients with rheumatoid arthritis. Br J Rheumatol . 1998;37:862–869. [DOI] [PubMed] [Google Scholar]
- 24.Smith E J., Soon VL, Boyd A, McAllister J, Deakin AH, Sarungi M. What do Scottish patients expect of their total knee arthroplasty? J Arthroplasty . 2016;31:786–792. [DOI] [PubMed] [Google Scholar]
- 25.Janse AJ, Gemke RJBJ, Uiterwaal CSPM, Van Der Tweel I, Kimpen JLL, Sinnema G. Quality of life: Patients and doctors don’t always agree: A meta-analysis. J Clin Epidemiol . 2004;57:653–661. [DOI] [PubMed] [Google Scholar]
- 26.Jourdan C, Poiraudeau S, Descamps S, Nizard R, Hamadouche M, Anract P, Boisgard S, Galvin M, Ravaud P. Comparison of patient and surgeon expectations of total hip arthroplasty. PLoS One . 2012;7:e30195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kazarian GS, Lonner JH, Hozack WJ, Woodward L, Chen AF. Improvements in sexual activity after total knee arthroplasty. J Arthroplasty . 2017;32:1159–1163. [DOI] [PubMed] [Google Scholar]
- 28.Kim TK, Kwon SK, Kang YG, Chang CB, Seong SC. Functional disabilities and satisfaction after total knee arthroplasty in female Asian patients. J Arthroplasty . 2010;25:458-464.e1–2. [DOI] [PubMed] [Google Scholar]
- 29.Lavernia CJ, Villa JM. High rates of interest in sex in patients with hip arthritis. Clin Orthop Relat Res . 2015;474:293–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Leichtenberg C, Kroon H, Dekker J, Nelissen R, Vlieland TV, Esch M vd, vd Esch M. Self-reported knee instability associated with pain and activity limitations prior and one year after total knee arthroplasty in patients with knee osteoarthritis. Osteoarthritis Cartil . 2017;(25 Suppl):S349–S350. [Google Scholar]
- 31.Leichtenberg CS, Meesters JJL, Kroon HM, Verdegaal SHM, Tilbury C, Dekker J, Nelissen RGHH, Vliet Vlieland TPM, van der Esch M. No associations between self-reported knee joint instability and radiographic features in knee osteoarthritis patients prior to Total Knee Arthroplasty: A cross-sectional analysis of the Longitudinal Leiden Orthopaedics Outcomes of Osteo-Arthritis study. Knee . 2017;24:816–823. [DOI] [PubMed] [Google Scholar]
- 32.Leichtenberg CS, Vliet Vlieland TPM, Kroon HM, Dekker J, Marijnissen WJ, Damen P-J, Nelissen RGHH, van der Esch M, On behalf of the LOAS Study Group. Self-reported knee instability associated with pain, activity limitations, and poorer quality of life before and 1 year after total knee arthroplasty in patients with knee osteoarthritis. J Orthop Res . 2018;36:2671–2678. [DOI] [PubMed] [Google Scholar]
- 33.Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med . 2007;357:762–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mancuso CA, Jout J, Salvati EA, Sculco TP. Fulfillment of patients’ expectations for total hip arthroplasty. J Bone Joint Surg Am . 2009;91:2073–8. [DOI] [PubMed] [Google Scholar]
- 35.Mancuso CA, Sculco TP, Wickiewicz TL, Jones EC, Robbins LD, Warren RW, Williams-Russo P. Patients’ Expectations of Knee Surgery. J Bone Joint Surg Am . 2001;83:1005–1012. [DOI] [PubMed] [Google Scholar]
- 36.Neuprez A, Delcour J-P, Fatemi F, Gillet P, Crielaard J-M, Bruyère O, Reginster J-Y. Patients’ expectations impact their satisfaction following total hip or knee arthroplasty. PLoS One . 2016;11:e0167911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nilsdotter AK, Toksvig-Larsen S, Roos EM. Knee arthroplasty: Are patients’ expectations fulfilled? A prospective study of pain and function in 102 patients with 5-year follow-up. Acta Orthop . 2009;80:55–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Noble PC, Gordon MJ, Weiss JM, Reddix RN, Conditt MA, Mathis KB. Does total knee replacement restore normal knee function? Clin Orthop Relat Res . 2005:157–165. [DOI] [PubMed] [Google Scholar]
- 39.Nordentoft T, Schou J, Carstensen J. Changes in sexual behavior after orthopedic replacement of hip or knee in elderly males, a prospective study. Int J Impot Res . 2000;12:143–146. [DOI] [PubMed] [Google Scholar]
- 40.Nunley RM, Nam D, Bashyal RK, Della Valle CJ, Hamilton WG, Berend ME, Parvizi J, Clohisy JC, Barrack RL. The impact of total joint arthroplasty on sexual function in young, active patients. J Arthroplasty . 2015;30:335–40. [DOI] [PubMed] [Google Scholar]
- 41.Palazzo C, Jourdan C, Descamps S, Nizard R, Hamadouche M, Anract P, Boisgard S, Galvin M, Ravaud P, Poiraudeau S. Determinants of satisfaction 1 year after total hip arthroplasty: The role of expectations fulfilment. BMC Musculoskelet Disord . 2014;15:1–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Peter WF, Dekker J, Tilbury C, Tordoir RL, Verdegaal SHM, Onstenk R, Bénard MR, Vehmeijer SB, Fiocco M, Vermeulen HM, van der Linden-van der Zwaag HMJ, Nelissen RGHH, Vliet Vlieland TPM. The association between comorbidities and pain, physical function and quality of life following hip and knee arthroplasty. Rheumatol Int. 2015;35:1233–1241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Scott CEH, Bugler KE, Clement ND, MacDonald D, Howie CR, Biant LC. Patient expectations of arthroplasty of the hip and knee. J Bone Joint Surg Br . 2012;94-B:974–981. [DOI] [PubMed] [Google Scholar]
- 44.Singh JA, Luo R, Landon GC, Suarez-Almazor M. Reliability and clinically important improvement thresholds for osteoarthritis pain and function scales: A multicenter study. J Rheumatol . 2014;41:509–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.van Steenbergen LN, Denissen GAW, Spooren A, van Rooden SM, van Oosterhout FJ, Morrenhof JW, Nelissen RGHH. More than 95% completeness of reported procedures in the population-based Dutch Arthroplasty Register. Acta Orthop . 2015;3674:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Stern SH, Fuchs MD, Ganz SB, Classi P, Sculco TP, Salvati EA. Sexual function after total hip arthroplasty. Clin Orthop Relat Res . 1991;269:228–35. [PubMed] [Google Scholar]
- 47.Tilbury C, Haanstra TM, Leichtenberg CS, Verdegaal SHM, Ostelo RW, de Vet HCW, Nelissen RGHH, Vliet Vlieland TPM. Unfulfilled expectations after total hip and knee arthroplasty surgery: There is a need for better preoperative patient information and education. J Arthroplasty . 2016;10:2139–45. [DOI] [PubMed] [Google Scholar]
- 48.Tolk JJ, van der Steen MC, Janssen RPA, Reijman M. Total knee arthroplasty: What to expect ? A survey of the members of the Dutch Knee Society on long-term recovery after total knee arthroplasty. J Knee Surg . 2017;30:612–616. [DOI] [PubMed] [Google Scholar]
- 49.Twisk J.W.R. P dr. Inleiding in de toegepaste biostatistiek. 4th ed. Houten, The Netherlands: Bohn Stafleu Van Loghum, 2016 [Google Scholar]
- 50.Wall PDH, Hossain M, Ganapathi M, Andrew JG. Sexual activity and total hip arthroplasty: a survey of patients’ and surgeons’ perspectives. Hip Int 2011;21:199–205. [DOI] [PubMed] [Google Scholar]
- 51.Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 2005;14:1523–1532. [DOI] [PubMed] [Google Scholar]
- 52.Weiss JM, Noble PC, Conditt MA, Kohl HW, Roberts S, Cook KF, Gordon MJ, Mathis KB. What functional activities are important to patients with knee replacements? Clin Orthop Relat Res 2002;404:172–188. [DOI] [PubMed] [Google Scholar]
- 53.World Health Organization. Sexual and reproductive health: Defining sexual health. Available at: http://www.who.int/reproductivehealth/topics/sexual_health/sh_definitions/en/. Accessed May 30, 2014.
- 54.Yoo JH, Kang YG, Kim SJ, Seong SC. Patient expectations of total knee replacement and their association with sociodemographic factors and functional status. J Bone Joint Surg Br. 2011;93:337–344. [DOI] [PubMed] [Google Scholar]
- 55.Zywiel MG, Mahomed A, Gandhi R, Perruccio A V., Mahomed NN. Measuring expectations in orthopaedic surgery: A systematic review. Clin Orthop Relat Res . 2013;471:3446–3456. [DOI] [PMC free article] [PubMed] [Google Scholar]