

Abstract
Objective
Solid pseudopapillary neoplasm (SPN) of the pancreas is a rare tumor. This study aims to examine the clinicopathological features and surgical treatments of SPN and compare the clinical behavior and prognosis between men and women with SPN.
Methods
We collected the population data of patients with SPN diagnosed between 2004 and 2017 from the SEER database. The Kaplan‐Meier method was used to analyze overall survival (OS) and disease‐specific survival (DSS), and log‐rank tests were used to evaluate the differences between subgroups. Univariate and multivariate Cox regression analyses were performed to screen out prognostic risk factors of SPN.
Results
A total of 378 patients with SPN were included, with 246 (65.1%) female patients. 1‐, 3‐, and 5‐year overall survival rates were 98.9%, 95.7%, and 93.7%, respectively. Survival analysis revealed that regardless of stage, patients with SPN who underwent surgical interventions still had a significantly better prognosis than those without surgical interventions (P < .001). The patients with lymphatic dissection had a significantly better prognosis than those without lymphatic dissection (P < .001). Moreover, compared with female patients, male patients had significantly poorer OS and DSS (P < .001). Female SPN showed a bimodal age‐frequency distribution with early‐onset incidence at 28 years and late‐onset peak incidence at 62 years, while male SPN presented a unimodal distribution with peak incidence at approximately age 64 years. In female patients, the tumor size in premenopausal females (<65 years old) was significantly larger than that in postmenopausal females (≥65 years old) (P < .001). Clinicopathological characteristic profiles were different not only between male SPN and premenopausal female SPN but also between premenopausal and postmenopausal female SPN.
Conclusion
SPN presents indolent behavior and predominantly occurs in young women. Regardless of stage, surgical intervention is recommended. Moreover, our study is the first large enough study to demonstrate sex‐related discrepancies in SPN. Thus, different treatment strategies should be designed for patients of different sexes at different ages and hormone therapy is a promising approach for SPN.
Keywords: hormone, SEER, sex‐related discrepancy, solid pseudopapillary neoplasm of the pancreas
Our study is the first large enough study to emphasize the sex‐related discrepancies in solid pseudopapillary neoplasm (SPN), and to observe that clinicopathological characteristic profiles were more common for male SPN and postmenopausal female SPN. It may provide inspiration for different management strategies for male and female patients and imply the possibility of hormone therapy for SPN.

1. INTRODUCTION
Solid pseudopapillary neoplasms (SPNs) of the pancreas are uncommon, borderline tumors, accounting for approximately 1%‐2.7% of all pancreatic tumors. 1 , 2 Recently, the incidence of SPN has been steadily growing, 3 , 4 and with the development and extensive use of imaging, the number of asymptomatic patients with SPN will increase. 5 It has already attracted increasing attention from clinicians and researchers.
To date, surgical resection remains the optimal treatment for resectable SPN. 6 Nevertheless, it has been reported that up to 19% of patients with SPN suffer from distant metastasis or localized invasion. 7 Moreover, recurrence after radical resection can occur in up to 9% of cases, 1 , 7 and even after re‐resections, recurrence can still occur. 6 There is no consensus on treatment for unresectable SPNs, and postoperative recurrence and metastasis, which indicates that other adjuvant treatments should be taken into consideration.
In addition, it has been established that SPN predominantly occurs in women with a women‐to‐men ratio of 10 to 1 7 and usually affects women of reproductive age. 8 , 9 This discrepancy suggests that sex could be a possible epidemiologic risk factor. 10 Several studies reported that progesterone receptors were present in 79%‐100% of patients with SPN. 11 , 12 All of the abovementioned facts suggest that sex hormones may play a role in the pathogenesis of SPN. We hypothesized that there was likely a difference between male and female patients with SPN. However, to our knowledge, a limited number of small case studies comparing men and women with SPN are available, and some controversies remain. Therefore, this study not only aimed to examine the clinicopathological features and the value of surgical treatments for SPN but also to compare the clinical behavior and prognosis between men and women with SPN based on a relatively large cohort study. It may provide inspiration for different management strategies for male and female patients and imply the possibility of hormone therapy for SPN.
2. METHODS
2.1. Data collection and study cohort
Data from this study were collected from the the Surveillance, Epidemiology, and End Results (SEER) database of the National Cancer Institute using SEER*Stat 8.3.6 software. We restricted our study to the SEER database (2004‐2017) because detailed Collaborative Stage (CS) data of SPN were not available before 2004. Patients were enrolled in this study if 1 the ICD Histologic Type ICD‐O‐3 code was 8452 or 8453 2 ; SPN was the only primary malignant tumor 3 ; patients were diagnosed with positive histology and/or cytology 4 ; clinicopathological information for sex, age at diagnosis, year of diagnosis, race, marital status, tumor location, tumor size, T‐classification, number of positive regional nodes, number of examined regional nodes, N‐classification, distant metastasis status, summary stage, surgery types, and radiotherapy or chemotherapy experience was included; and 5 the vital status and cause of death were known, and patients were diagnosed more than 1 month prior to death. The detailed process of selecting patients is shown in Figure 1.
FIGURE 1.
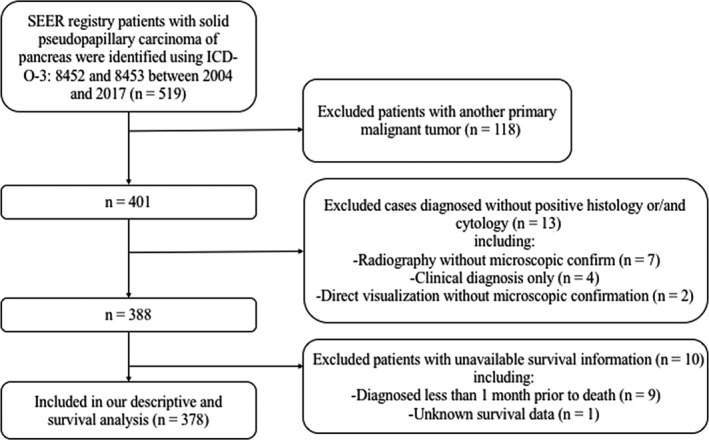
Flow diagram of patients selection in our study from the SEER database 2004‐2017
2.2. Study variables
The following variables were obtained from the selected data: sex, age at diagnosis, year of diagnosis, race, marital status, tumor location, tumor size, T‐classification, number of positive regional nodes, number of examined regional nodes, N‐classification, distant metastases status, summary stage, surgery types, radiotherapy or chemotherapy experience, vital status, cause of death, and survival months. According to seer coding manuals (https://seer.cancer.gov/tools/codingmanuals/), all data were precisely decoded. In this study, operation methods are divided into operative treatment (included local excision of tumor, partial pancreatectomy, partial or local pancreatectomy and duodenectomy without distal/partial gastrectomy, Whipple's procedure, extended pancreatoduodenectomy, total pancreatectomy with subtotal gastrectomy or duodenectomy, NanoKnife, and irreversible electroporation) and nonoperative treatment.
2.3. Statistical analysis
The patients’ demographic and clinicopathological parameters were summarized by descriptive statistics. Reverse Kaplan‐Meier methods were performed to estimate the median follow‐up time. The chi‐square test or Fisher's exact test was used to compare patient characteristics between the male and female groups. We used Kaplan‐Meier methods to analyze overall survival (OS) and disease‐specific survival (DSS) and log‐rank tests to evaluate the differences between subgroups. Univariate and multivariate Cox regression analyses were used to assess independent prognostic risk factors associated with the OS and DSS of patients with SPN. We presented the results as hazard ratios (HRs) and 95% confidence intervals (CIs). All of the statistical analyses were performed using GraphPad Prism 8 (GraphPad Software) and SPSS Statistics 22.0 (IBM). Differences were considered to be statistically significant when P values were less than .05.
3. RESULTS
3.1. Patient demographic and clinicopathological parameters
In total, 378 patients were identified in this study, and their characteristics in the entire cohort are listed in Table 1. The age of the patients ranged from 8 to 91 years (mean, 50.8 years). There were 277 (73.3%) patients who were white. Fewer than half of the patients were male (34.9%) and unmarried (32.8%). Regarding treatment, most patients never received radiotherapy (90.7%) or chemotherapy (78.8%) treatment. Overall, 330 (87.3%) patients had surgery experience, whereas 48 (12.7%) patients did not undergo surgery. Over half of the SPNs occurred in the head of the pancreas (53.4%), followed by the tail (30.4%) and body of the pancreas (14.3%). The tumor size was more than 40 mm in 191 patients, who accounted for 50.5% of 378 cases. More than half of patients with SPN were diagnosed at the localized stage (57.9%) without positive lymph nodes (84.7%) or distant metastasis (92.3%).
TABLE 1.
Baseline demographic and clinicopathological characteristics of 378 patients with solid pseudopapillary neoplasm (2004‐2017)
| Characteristics | Numbers (n) | Percentage |
|---|---|---|
| Age | ||
| ≤30 | 87 | 23.0 |
| 30‐64 | 177 | 46.8 |
| ≥65 | 114 | 30.2 |
| Sex | ||
| Male | 132 | 34.9 |
| Female | 246 | 65.1 |
| Race | ||
| White | 277 | 73.3 |
| American Indian/Alaska Native | 3 | 0.8 |
| Asian or Pacific Islander | 47 | 12.4 |
| Black | 47 | 12.4 |
| Unknown | 4 | 1.1 |
| Marital status at diagnosis | ||
| Married | 174 | 46.0 |
| Single or Unmarried | 124 | 32.8 |
| Divorced or Separated | 26 | 6.9 |
| Widowed | 30 | 7.9 |
| Unknown | 24 | 6.3 |
| Surgical procedures | ||
| 0 | 48 | 12.7 |
| 1 | 4 | 1.1 |
| 2 | 166 | 43.9 |
| 3 | 102 | 27.0 |
| 4 | 50 | 13.2 |
| 5 | 8 | 2.1 |
| Received radiotherapy | ||
| Yes | 35 | 9.3 |
| No | 343 | 90.7 |
| Received chemotherapy | ||
| Yes | 80 | 21.2 |
| No/unknown | 298 | 78.8 |
| Tumor location | ||
| Head of pancreas | 202 | 53.4 |
| Body of pancreas | 54 | 14.3 |
| Tail of pancreas | 115 | 30.4 |
| Unknown | 7 | 1.9 |
| SEER historic stage | ||
| Localized | 219 | 57.9 |
| Regional | 128 | 33.9 |
| Distant | 24 | 6.3 |
| Unstaged | 7 | 1.9 |
| Tumor size (mm) | ||
| Mean ± SD | 48.1 ± 33.9 | |
| ≤40 | 181 | 47.9 |
| >40 | 191 | 50.5 |
| Unknown | 6 | 1.6 |
| Lymph nodes positive | ||
| 0 LN+ | 320 | 84.7 |
| 1‐3 LN+ | 26 | 6.9 |
| ≥4 LN+ | 16 | 4.2 |
| Unknown | 16 | 4.2 |
| Distant metastases | ||
| M0 | 349 | 92.3 |
| M1 | 24 | 6.4 |
| Unknown | 5 | 1.3 |
Surgical procedures: 0: No surgery of primary site; 1: local excision of tumor; 2: partial pancreatectomy and partial or local pancreatectomy and duodenectomy without distal/partial gastrectomy; 3: Whipple's procedure; 4: Total pancreatectomy and subtotal gastrectomy or duodenectomy and extended pancreatoduodenectomy; and 5: other surgical approaches; LN: Lymph nodes.
3.2. Survival analysis and prognostic factors
In this study, the median follow‐up time was 44 months (range, 1‐154 months). During follow‐up, 103 (27.2%) deaths occurred, of which 80 deaths were attributed to SPN (Table S1). The OS and DSS of patients with SPN are shown in Figure 2A,B. We found that the survival time of patients with SPN was optimistic. The 1‐, 3‐, and 5‐year overall survival rates were 98.9%, 95.7%, and 93.7%, respectively. For DSS, the 1‐, 3‐, and 5‐year survival rates were 99.2%, 96.0%, and 93.2%, respectively. Additionally, we found that only a small proportion of patients with SPN had four or more positive lymph nodes (4.2%) and distant metastasis (6.4%) (Table 1; Figure 2C,D).
FIGURE 2.

Solid pseudopapillary neoplasm (SPN) exhibited indolent behaviors. A, Survival analysis for overall survival in patients with SPNs; B, Survival analysis for disease‐specific survival in patients with SPNs; C, Lymph nodes metastasis status in SEER cohorts; D, Distant metastasis status in SEER cohorts
Next, we used univariate Cox regression to analyze the factors associated with OS and DSS in patients with SPN (Tables S2 and S3). The univariate analysis revealed that age, sex, surgery experience, tumor location, tumor size, lymph node metastasis, and distant metastasis were all significant prognostic factors for OS and DSS of patients with SPN. We found that patients with SPN who underwent surgical interventions had significantly better OS and DSS than those without surgical interventions (P < .001; Figure 3). The 1‐ and 3‐year overall survival rates in the surgery group were 98.5% and 97.2%, respectively, compared with 78.8% and 33.5% in the nonsurgery group (P < .001; Figure 3A). For DSS, the 1‐ and 3‐year survival rates for patients without surgery interventions were 76.3% and 25.4%, respectively, which were significantly lower than those for patients with surgery interventions (P < .001; Figure 3A). Interestingly, we found that regardless of stage, patients still had better survival after surgery than those without surgery (P < .001; Figure 3B,C). For lymphadenectomy, patients who received lymphatic dissection had significantly better OS and DSS than those without lymphatic dissection (P < .001; Figure 4A‐C).
FIGURE 3.

Survival analysis for overall survival and disease‐specific survival in patients with solid pseudopapillary neoplasm based on surgical intervention
FIGURE 4.

Survival analysis for overall survival and disease‐specific survival in patients with solid pseudopapillary neoplasm based on lymphadenectomy
Prognostic factors of OS and DSS were further assessed by multivariate Cox regression models, which revealed that age (P < .001), sex (P < .05), surgery experience (P < .001), lymph node metastasis status (P < .001), and distant metastasis status (P < .001) were all independent prognostic factors. However, marital status, tumor size, and tumor location were not found to be significant factors (Tables S2 and S3).
3.3. Sex pattern
Based on sex, we divided the cohort into male and female groups. Their characteristics were compared and are illustrated in Table 2. We observed that female SPN occurred more frequently at the body/tail of the pancreas (54.7%) than male SPN (28.1%). Male patients were less frequently diagnosed at a localized stage (48.5%) than female patients (64.9%). We also found that almost half (49.2%) of male patients were diagnosed at 65 years and older, whereas most (80.1%) female patients were diagnosed younger than 65 years (Table 2 and Figure 5A). As the age‐frequency distribution showed, male SPN demonstrated a unimodal skewness distribution with peak incidence at approximately age 64 years (median age). However, female SPN showed a bimodal distribution with early‐onset and late‐onset peak incidence at 28 (lower quartile age) and 62 years (upper quartile age) (Figure 5B).
TABLE 2.
Comparison of selected clinicopathological characteristics between male and female with solid pseudopapillary neoplasm
| Characteristics | Male | Female | P | <65 years female | ≥65 years female | P | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| Age | ||||||||||
| ≤30 | 6 | 4.5 | 81 | 32.9 | .000 ** | |||||
| 30‐64 | 61 | 46.2 | 116 | 47.2 | ||||||
| ≥65 | 65 | 49.2 | 49 | 19.9 | ||||||
| Race | ||||||||||
| White | 103 | 78.0 | 174 | 70.7 | .304 | 134 | 68.0 | 40 | 81.6 | .131 |
| Black | 13 | 9.8 | 34 | 13.8 | 31 | 15.7 | 3 | 6.1 | ||
| Others/unknown | 16 | 12.1 | 38 | 15.4 | 32 | 16.2 | 6 | 12.2 | ||
| Marital status at diagnosis | ||||||||||
| Unmarried | 28 | 21.2 | 96 | 39.0 | .000 ** | 90 | 45.7 | 6 | 12.2 | .000 ** |
| Married | 78 | 59.1 | 96 | 39.0 | 76 | 38.6 | 20 | 40.8 | ||
| Others/unknown | 26 | 19.7 | 54 | 22.0 | 31 | 15.7 | 23 | 46.9 | ||
| Received operation | ||||||||||
| No | 22 | 16.7 | 26 | 10.6 | .090 | 15 | 7.6 | 11 | 22.4 | .003 * |
| Yes | 110 | 88.3 | 220 | 89.4 | 182 | 92.4 | 38 | 77.6 | ||
| Tumor location | ||||||||||
| Head of pancreas | 92 | 71.9 | 110 | 45.3 | .000 ** | 78 | 39.8 | 32 | 68.1 | .000 ** |
| Body/tail of pancreas | 36 | 28.1 | 133 | 54.7 | 118 | 60.2 | 15 | 31.9 | ||
| SEER historic stage | ||||||||||
| Localized | 64 | 48.5 | 155 | 64.9 | .003 * | 130 | 68.4 | 25 | 51.0 | .065 |
| Reginal | 56 | 42.4 | 72 | 30.1 | 51 | 26.8 | 21 | 42.9 | ||
| Distant | 12 | 9.1 | 12 | 5.0 | 9 | 4.7 | 3 | 6.1 | ||
| Tumor size (mm) | ||||||||||
| ≤40 | 64 | 49.2 | 117 | 48.3 | .871 | 82 | 42.3 | 35 | 72.9 | .000 ** |
| >40 | 66 | 508 | 125 | 51.7 | 112 | 57.7 | 13 | 27.1 | ||
| Lymph nodes positive | ||||||||||
| 0 LN+ | 109 | 83.2 | 211 | 89.4 | .089 | 174 | 92.1 | 37 | 78.7 | .008 * |
| ≥1 LN+ | 22 | 16.8 | 25 | 10.6 | 15 | 7.9 | 10 | 21.3 | ||
| M | ||||||||||
| M0 | 120 | 90.9 | 229 | 93.1 | .122 | 183 | 92.9 | 46 | 93.9 | .713 |
| M1 | 12 | 9.1 | 12 | 4.9 | 9 | 4.6 | 3 | 66.1 | ||
The unknown variables were not included.
P < .05.
P < .001.
FIGURE 5.

Solid pseudopapillary neoplasm (SPN) presented gender‐related discrepancies. A, Age‐gender distribution of male SPN and female SPN; B, Age‐frequency distribution of male SPN and female SPN; C, Survival analysis for overall survival and disease‐specific survival comparing male and female patients with SPN
Considering the age of natural menopause and the population characteristics in our cohort, we divided female patients into two groups: younger than 65 years and 65 years and older, representing premenopausal females and postmenopausal females, respectively. Interestingly, we observed that the tumor size in premenopausal females was significantly larger than that in postmenopausal females (Figure 6A).
FIGURE 6.

The difference between premenopausal female and postmenopausal female. A, Survival analysis for overall survival and disease‐specific survival comparing premenopausal female and postmenopausal female with solid pseudopapillary neoplasm (SPN); B, Tumor size distribution of SPN in premenopausal female and postmenopausal female
Survival analysis revealed that male patients had significantly poorer OS and DSS than female patients (P < .001, Figure 5C). For female, OS and DSS of postmenopausal patients were significantly poorer than postmenopausal patients (P < .001, Figure 6B).
Next, we performed univariate and multivariate analyses based on sex, and we observed that factors affecting survival differed. In male patients, univariate analysis found that factors related to overall survival included age, surgery experience, stage, the number of positive lymph nodes, and distant metastasis status (Table S4). In addition to the above factors, tumor location was found to be a prognostic factor in the female group (Table S4). For DSS, tumor size was significantly associated with prognosis for male SPN (Table S5), but it was not a significant prognostic factor for female SPN. Additionally, tumor site was not a prognostic factor in male patients but was considered a prognostic factor in female patients (Table S5). The multivariate analysis with Cox regression showed that age, surgery performance, and distant metastasis status were independent variables associated with OS and DSS in male patients (Tables 3 and 4). However, distant metastasis status was not found to be an independent prognostic factor for female patients and the number of positive lymph nodes was considered a prognostic factor in female patients (Tables 3 and 4).
TABLE 3.
Multivariate analysis of factors associated with overall survival for patients with solid pseudopapillary neoplasms
| Characteristics | Male | Female | ||||
|---|---|---|---|---|---|---|
| P value | HR | 95% CI | P value | HR | 95% CI | |
| Age | ||||||
| <65 | Reference | Reference | ||||
| ≥65 | .015 * | 2.159 | 1.163‐4.009 | .000 ** | 6.247 | 2.922‐13.352 |
| Marital status at diagnosis | ||||||
| Single or unmarried | Reference | Reference | ||||
| Married | .504 | 1.339 | 0.559‐3.151 | .784 | 1.132 | 0.467‐2.476 |
| Divorced or separated or widowed | .009 * | 3.990 | 1.413‐1.267 | 0.873 | 1.085 | 0.101‐2.939 |
| Received surgery | ||||||
| No | Reference | Reference | ||||
| Yes | .000 ** | 0.224 | 0.107‐0.472 | .002 * | 0.243 | 0.098‐0.603 |
| Tumor location | NI | |||||
| Head of pancreas | Reference | |||||
| Body/tail of pancreas | .266 | 0.617 | 0.264‐1.443 | |||
| Tumor size (mm) | NI | |||||
| ≤40 | Reference | |||||
| >40 | .921 | 1.021 | 0.561‐1.897 | |||
| Lymph nodes positive | ||||||
| 0 LN+ | Reference | Reference | ||||
| 1‐3 LN+ | .219 | 0.434 | 0.114‐1.643 | .000 ** | 6.034 | 2.367‐15.377‐ |
| ≥4 LN+ | .002 * | 4.104 | 1.660‐10.148 | .000 ** | 13.404 | 4.401‐40.823 |
| M | ||||||
| M0 | Reference | Reference | ||||
| M1 | .000 ** | 4.860 | 2.105‐11.224 | .058 | 3.419 | 0.960‐12.177 |
Abbreviation: NI, not included in multivariate survival analysis.
P < .05.
P < .001.
TABLE 4.
Multivariate analysis of factors associated with disease‐specific survival for patients with solid pseudopapillary neoplasms
| Characteristics | Male | Female | ||||
|---|---|---|---|---|---|---|
| P value | HR | 95% CI | P value | HR | 95% CI | |
| Age | ||||||
| <65 | Reference | Reference | ||||
| ≥65 | .021 * | 2.260 | 1.129‐4.523 | .000 ** | 8.698 | 3.454‐21.907 |
| Marital status at diagnosis | ||||||
| Single or unmarried | Reference | Reference | ||||
| Married | .246 | 1.804 | 0.666‐4.886 | .903 | 0.940 | 0.347‐2.545 |
| Divorced or separated or widowed | .003 * | 6.151 | 1.890‐20.014 | .623 | 0.740 | 0.223‐2.454 |
| Received surgery | ||||||
| No | Reference | Reference | ||||
| Yes | .000 ** | 0.200 | 0.085‐0.466 | .001 * | 0.162 | 0.054‐0.487 |
| Tumor location | NI | |||||
| Head of pancreas | Reference | |||||
| Body/tail of pancreas | .140 | 0.462 | 0.165‐1.290 | |||
| Tumor size (mm) | NI | |||||
| ≤40 | Reference | |||||
| >40 | .984 | 0.993 | 0.487‐2.024 | |||
| Lymph nodes positive | ||||||
| 0 LN+ | Reference | Reference | ||||
| 1‐3 LN+ | .171 | 0.361 | 0.084‐1.555 | .000 ** | 7.318 | 2.538‐21.097 |
| ≥4 LN+ | .021 * | 3.515 | 1.209‐10.218 | .000 ** | 16.937 | 5.111‐56.132 |
| M | ||||||
| M0 | Reference | Reference | ||||
| M1 | .000 ** | 6.573 | 2.417‐17.877 | .057 | 4.436 | 0.954‐20.620 |
Abbreviation: NI, not included in multivariate survival analysis.
P < .05.
P < .001.
4. DISCUSSION
In our study, we analyzed the SEER database of 378 patients with SPN and mainly elaborated the following three points:
First, we evaluated the biological behavior of SPNs by analyzing demographic and clinicopathological characteristics. Consistent with conventional views, we observed that SPN exhibited indolent behaviors with a relatively low risk of lymph node metastasis (12.4%) and distant metastasis (4.5%) in the SEER cohort. Most patients with SPN were diagnosed at the localized stage (85.1%). We also found that the SPN showed a favorable prognosis. The 1‐, 3‐, and 5‐year DSS rates were 98.9%, 95.7%, and 93.7%.
Second, we assessed the effect of surgery treatments on patients with SPN. Previous evidence confirmed that surgical resection was an effective approach to treat SPN, and satisfactory outcomes could be obtained by tumor debulking. 13 , 14 , 15 In our study, we demonstrated similar results in that patients with SPN after surgical resection had significantly better OS and DSS than those without surgical resection. Meanwhile, we identified that patients diagnosed at distant stages still had more favorable survival after surgical debulking than those without surgical debulking. However, the validity of lymphadenectomy remains a controversial issue. Some researchers claimed that there was no need to undertake formal lymphadenectomy routinely, 16 , 17 whiles other reported that lymphatic dissection is necessary. 14 , 18 We found that patients with lymphatic dissection had a significantly better prognosis than those without lymphatic dissection. Thus, surgical resection guarantees the good prognosis, but further studies need to evaluate the effectiveness of lymphatic dissection. Moreover, in view of long‐term survival and low‐grade malignancy, organ‐preserving surgery, such as duodenum‐preserving pancreatic head resection and spleen‐preserving resection, and laparoscopic surgery will be encouraged in specialized pancreatic centers. 19 , 20 , 21
Last but not least, investigating the sex feature of SPNs. In our current study, SPN showed a predilection for females in 65.1% of all cases. It is worth noting the distinctly different patterns of onset between males and females. We revealed that female SPNs showed a bimodal age‐frequency distribution, while male SPNs demonstrated a unimodal skewness distribution. Moreover, we found that female SPN had an early‐onset incidence at 28 years and a late‐onset peak incidence at 62 years, while male SPN had a peak incidence at approximately 64 years of age. Previous evidence implied that sex hormones might participate in the pathogenesis of SPN. 20 , 22 Strong immunoreactivity for progesterone has been identified in many studies. 11 , 12 , 23 Case reports showed that SPN grew rapidly during pregnancy, 24 , 25 , 26 and progesterone might act as an oncogenic factor in SPN. For estrogen, Tognarini I et al demonstrated the strong expression of ER in tumor tissue and the proliferative action of estrogen in vitro, offering potential treatment strategies for SPN via selective ER modulators. 27 Similarly, another study reported that antiestrogen drugs for cases with unresectable liver metastasis resulted in a favorable prognosis. 28 Therefore, in our study, we presumed that the early onset in women might be attributed to exposure to progesterone and/or estrogen during the reproductive period, while the late onset might be attributed to accumulated lifetime environmental exposure.
The age of natural menopause varies by individual, race, and ethnicity, with a range of 40‐60. 29 , 30 Considering the age of natural menopause and population characteristics in our cohort, we divided female patients into two groups: younger than 65 years and 65 years and older, representing premenopausal females and postmenopausal females, respectively. Interestingly, we observed that the tumor size in premenopausal females was significantly larger than that in postmenopausal females. It indicated that female hormones affect the growth of SPNs and that anti‐female hormone agents may be a promising adjuvant. However, the function of female hormones in development has not yet reached consensus and needs further study.
Our study also revealed that male patients had significantly poorer OS and DSS than female patients. This difference may be because male SPNs had a higher percentage of patients older than 65 years than female SPNs. Reported surveys and our analysis consistently identified that older age was an independent prognostic risk factor for SPN. 10 , 31 In addition, we found that the clinicopathological characteristic profiles were more similar for male SPN and postmenopausal female SPN. To our knowledge, our study is the first to describe this phenomenon in a male population. Moreover, it could partly explain that despite the larger tumor size in premenopausal females, the OS and DSS of premenopausal females were significantly better than those of postmenopausal females.
There are several limitations in our current population‐based study. First, due to the indolent behavior of SPNs, it was difficult to conduct large prospective studies. Our study is retrospective and may inevitably include biases, which affect the analysis. Second, the rarity of SPN in nature and the lower number of patients in the subgroups based on sex and age results in limited statistical power. Third, the lack of detailed information about chemotherapy and radiation made it difficult to evaluate their effect on SPN. Meanwhile, information on recurrence was not recorded, and factors that contributed to the sex disparities, such as serum levels of estrogen, progestogen, androgen, menstrual status, and reproductive histories, were not available in the SEER database. Therefore, it is difficult to precisely assess the difference between female and male patients with SPN at different ages. To better understand these complicated sex disparities and the role of sex hormones in the development of SPN, further clinical and fundamental research is needed. Despite these limitations, this is the first study that is large enough to demonstrate that male SPN was different from female SPN, which suggests that different treatment strategies should be designed for patients of different sexes at different ages and implies the possibility of hormone therapy.
5. CONCLUSION
In conclusion, this population‐based study demonstrated that SPN present indolent behavior and predominantly occurs in young women. Regardless of stage, surgical intervention is recommended. Moreover, our study is the first large enough study to emphasize the sex‐related discrepancies in SPN, and to observe that clinicopathological characteristic profiles were more common for male SPN and postmenopausal female SPN. Thus, different treatment strategies should be designed for patients with different genders at different ages and hormone therapy was a promising approach.
CONFLICT OF INTEREST
None of the authors have any potential conflict of interest to declare.
AUTHOR CONTRIBUTIONS
SL, JW, and YM designed the project. JW, YJ, PY, and SS performed the experiments and data extraction. JW, YM, YJ, and YS contributed statistical analysis. JW and YM wrote the manuscript. All authors reviewed the manuscript.
Supporting information
Supplementary Materials
ACKNOWLEDGMENTS
This work was supported by grants from the National Key Research and Development Plan (No. 2017YFC0910002).
Wu J, Mao Y, Jiang Y, et al. Sex differences in solid pseudopapillary neoplasm of the pancreas: A population‐based study. Cancer Med. 2020;9:6030–6041. 10.1002/cam4.3180
Jiali Wu and Yize Mao contributed equally to this work.
DATA AVAILABILITY STATEMENT
All data generated for this study are available from the corresponding author upon request.
REFERENCES
- 1. Kang CM, Choi SH, Kim SC, Lee WJ, Choi DW, Kim SW. Predicting recurrence of pancreatic solid pseudopapillary tumors after surgical resection: a multicenter analysis in Korea. Annals Surgery. 2014;260(2):348‐355. [DOI] [PubMed] [Google Scholar]
- 2. de Castro SMM, Singhal D, Aronson DC, et al. Management of solid‐pseudopapillary neoplasms of the pancreas: a comparison with standard pancreatic neoplasms. World J Surg. 2007;31(5):1130‐1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Law JK, Ahmed A, Singh VK, et al. A systematic review of solid‐pseudopapillary neoplasms: are these rare lesions? Pancreas. 2014;43(3):331‐337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Martin RC, Klimstra DS, Brennan MF, Conlon KC. Solid‐pseudopapillary tumor of the pancreas: a surgical enigma? Ann Surg Oncol. 2002;9(1):35‐40. [DOI] [PubMed] [Google Scholar]
- 5. Hu S, Zhang H, Wang X, et al. Asymptomatic versus symptomatic solid pseudopapillary tumors of the pancreas: clinical and MDCT manifestations. Cancer Imaging. 2019;19(1):13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Talukdar R, Nageshwar RD. Treatment of pancreatic cystic neoplasm: surgery or conservative? Clin Gastroenterol Hepatol. 2014;12(1):145‐151. [DOI] [PubMed] [Google Scholar]
- 7. Huffman BM, Westin G, Alsidawi S, et al. Survival and prognostic factors in patients with solid pseudopapillary neoplasms of the pancreas. Pancreas. 2018;47(8):1003‐1007. [DOI] [PubMed] [Google Scholar]
- 8. Carlotto JRM, Torrez FRA, Gonzalez AM, et al. Solid pseudopapillary neoplasm of the pancreas. Arq Bras Cir Dig. 2016;29(2):93‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Patnayak R, Jena A, Parthasarathy S, et al. Solid and cystic papillary neoplasm of pancreas: a clinic‐pathological and immunohistochemical study: a tertiary care center experience. South Asian J Cancer. 2013;2(3):153‐157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Machado MCC, Machado MAC, Bacchella T, Jukemura J, Almeida JL, Cunha JEM. Solid pseudopapillary neoplasm of the pancreas: distinct patterns of onset, diagnosis, and prognosis for male versus female patients. Surgery. 2008;143(1):29‐34. [DOI] [PubMed] [Google Scholar]
- 11. Yeh TS, Jan YY, Chiu CT, et al. Characterisation of oestrogen receptor, progesterone receptor, trefoil factor 1, and epidermal growth factor and its receptor in pancreatic cystic neoplasms and pancreatic ductal adenocarcinoma. Gut. 2002;51(5):712‐716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Nguyen NQ, Johns AL, Gill AJ, et al. Clinical and immunohistochemical features of 34 solid pseudopapillary tumors of the pancreas. J Gastroenterol Hepatol. 2011;26(2):267‐274. [DOI] [PubMed] [Google Scholar]
- 13. Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature. J Am Coll Surg. 2005;200(6):965‐972. [DOI] [PubMed] [Google Scholar]
- 14. Kim MJ, Choi DW, Choi SH, Heo JS, Sung JY. Surgical treatment of solid pseudopapillary neoplasms of the pancreas and risk factors for malignancy. Br J Surg. 2014;101(10):1266‐1271. [DOI] [PubMed] [Google Scholar]
- 15. Cheng‐hong P, Dong‐feng C, Guang‐wen Z, et al. The solid‐pseudopapillary tumor of pancreas: the clinical characteristics and surgical treatment. J Surg Res. 2006;131(2):276‐282. [DOI] [PubMed] [Google Scholar]
- 16. Klimstra DS, Wenig BM, Heffess CS. Solid‐pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Semin Diagn Pathol. 2000;17(1):66‐80. [PubMed] [Google Scholar]
- 17. Tipton SG, Smyrk TC, Sarr MG, Thompson GB. Malignant potential of solid pseudopapillary neoplasm of the pancreas. Br J Surg. 2006;93(6):733‐737. [DOI] [PubMed] [Google Scholar]
- 18. Tajima Y, Kohara N, Maeda J, et al. Peritoneal and nodal recurrence 7 years after the excision of a ruptured solid pseudopapillary neoplasm of the pancreas: report of a case. Surg Today. 2012;42(8):776‐780. [DOI] [PubMed] [Google Scholar]
- 19. Liu M, Liu J, Hu Q, et al. Management of solid pseudopapillary neoplasms of pancreas: a single center experience of 243 consecutive patients. Pancreatology. 2019;19(5):681‐685. [DOI] [PubMed] [Google Scholar]
- 20. Naar L, Spanomichou D‐A, Mastoraki A, Smyrniotis V, Arkadopoulos N. Solid pseudopapillary neoplasms of the pancreas: a surgical and genetic enigma. World J Surg. 2017;41(7):1871‐1881. [DOI] [PubMed] [Google Scholar]
- 21. Nakamura Y, Matsushita A, Katsuno A, et al. Clinical outcomes for 14 consecutive patients with solid pseudopapillary neoplasms who underwent laparoscopic distal pancreatectomy. Asian J Endosc Surg. 2016;9(1):32‐36. [DOI] [PubMed] [Google Scholar]
- 22. Pettinato G, Di Vizio D, Manivel JC, Pambuccian SE, Somma P, Insabato L. Solid‐pseudopapillary tumor of the pancreas: a neoplasm with distinct and highly characteristic cytological features. Diagn Cytopathol. 2002;27(6):325‐334. [DOI] [PubMed] [Google Scholar]
- 23. Zou Y, Huang Y, Hong B, Xiang X, Zhou B, Wei S. Comparison of the clinicopathological features of pancreatic solid pseudopapillary neoplasms between males and females: gender does matter. Histol Histopathol. 2019;18156. [DOI] [PubMed] [Google Scholar]
- 24. Huang S‐C, Wu T‐H, Chen C‐C, Chen T‐C. Spontaneous rupture of solid pseudopapillary neoplasm of the pancreas during pregnancy. Obstet Gynecol. 2013;121(2 Pt 2 Suppl 1):486‐488. [DOI] [PubMed] [Google Scholar]
- 25. Ganepola GA, Gritsman AY, Asimakopulos N, Yiengpruksawan A. Are pancreatic tumors hormone dependent?: A case report of unusual, rapidly growing pancreatic tumor during pregnancy, its possible relationship to female sex hormones, and review of the literature. Am Surg. 1999;65(2):105‐111. [PubMed] [Google Scholar]
- 26. Huang TT, Zhu J, Zhou H, Zhao AM. Solid pseudopapillary neoplasm of pancreas in pregnancy treated with tumor enucleation: case report and review of the literature. Niger J Clin Pract. 2018;21(9):1234‐1237. [DOI] [PubMed] [Google Scholar]
- 27. Tognarini I, Tonelli F, Nesi G, et al. In vitro effects of oestrogens, antioestrogens and SERMs on pancreatic solid pseudopapillary neoplasm‐derived primary cell culture. Cell Oncol. 2010;32(5–6):331‐343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Shorter NA, Glick RD, Klimstra DS, Brennan MF, Laquaglia MP. Malignant pancreatic tumors in childhood and adolescence: The Memorial Sloan‐Kettering experience, 1967 to present. J Pediatr Surg. 2002;37(6):887‐892. [DOI] [PubMed] [Google Scholar]
- 29. Honour JW. Biochemistry of the menopause. Ann Clin Biochem. 2018;55(1):18‐33. [DOI] [PubMed] [Google Scholar]
- 30. Monteleone P, Mascagni G, Giannini A, Genazzani AR, Simoncini T. Symptoms of menopause – global prevalence, physiology and implications. Nat Rev Endocrinol. 2018;14(4):199‐215. [DOI] [PubMed] [Google Scholar]
- 31. Lam KY, Lo CY, Fan ST. Pancreatic solid‐cystic‐papillary tumor: clinicopathologic features in eight patients from Hong Kong and review of the literature. World J Surg. 1999;23(10):1045‐1050. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Materials
Data Availability Statement
All data generated for this study are available from the corresponding author upon request.