

Abstract
The COVID-19 pandemic has posed unique concerns and potential risks to women now pregnant or considering childbearing. Although no professional societies have issued recommendations that women avoid conception at this time, several professional organizations recommended a moratorium on infertility services including both medically assisted reproduction and assisted reproductive technology shortly after the World Health Organization declared COVID-19 infection to be a pandemic. Reasons cited for undertaking these extraordinary measures included prevention of possible complications of assisted reproductive technology and medically assisted reproduction and virus induced complications of pregnancy including potential vertical transmission to the fetus and optimization use of critical health care resources. A survey of reproductive health providers in 97 countries was undertaken to assess their response to the pandemic and recently issued guidance. Although different countries reacted differently with diverse responses and variable resources, the results suggest that the reproductive health community has largely been responsive to public health and individual patient concerns.
Keywords: ART, MART, Covid-19 pandemic, Infertility services
The possibility of risks specific for pregnant women and their fetuses became immediate concerns at the outbreak of the COVID-19 pandemic. In contrast to the 2015 Zika virus epidemic, when unique birth defects were identified early in the course of the spread, no novel fetal or maternal risks have yet been confirmed1. However, the limited extant data regarding the maternal and fetal effects of COVID-19 infection especially for the first trimester provide little reassurance. The pandemic posed an immediate dilemma for centers actively treating infertile couple with medically assisted reproduction (MAR) and assisted reproductive technology (ART), including in vitro fertilization.
Out of caution, several professional societies around the world recommended suspending therapy for infertility services initially on March 18, 2020, 1 week after the World Health Organization declared COVID-19 infection to be a pandemic2–4. All guidelines published by reproductive medicine societies at this time endorsed cessation of infertility services although some granted exemptions for exceptional circumstances, such as oocyte or sperm cryopreservation procedures in patients about to undergo chemotherapy or radiation, that would likely deplete their gamete number. Reasons cited for these extraordinary measures included preventing possible complications of ART and MAR, possible virus induced complications of pregnancy and concerns regarding potential vertical transmission to the fetus in SARS-CoV-2 positive mothers. Additional priorities included optimizing allocation of critical health care resources and supportive policy for recommendations for social distancing. Subsequent advisories have refined the original recommendations and proposed potential requisite criteria for reestablishing infertility services5,6. As the virus has spread globally, various countries and their fertility centers were impacted at different times and to different extents. Most countries previously actively engaged in ART and MAR services are now at various stages between suspension and resumption of services. As of May 31, 2020, COVID-19 has been reported to exist in 188 countries7. While local circumstances and resources have largely dictated response, a debate has also ensued pitting those prioritizing containment of the virus against those emphasizing patient autonomy.
Methods
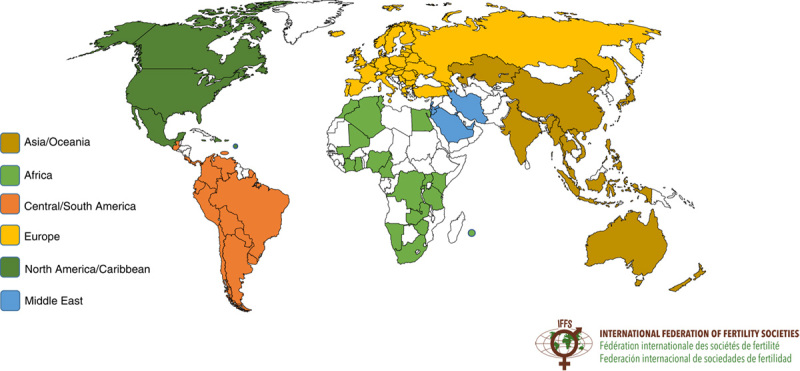
Since the outset of the pandemic, the International Federation of Fertility Societies (IFFS) has monitored international guidance, compiling a registry of relevant links and local responses. As part of this mission, a brief (11 question) descriptive research survey was undertaken which was posted online from April 21, 2020 through May 8, 2020 with the objective of assessing the status of availability of infertility services in each individual country recruited to the questionnaire. Respondents from 97 countries representing 207 individual centers completed the survey addressing the following questions.
Are fertility treatments regarded as an essential medical service that should continue despite the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or COVID-19 pandemic in your country?
Has your country modified its policy regarding fertility treatments along with the evolution of the COVID-19 pandemic?
What is the status of ART centers in your country in relation to the COVID-19 pandemic?
What is the status of your ART center in relation to the COVID-19 pandemic?
If your ART center is closed, what was the closure mandated by?
If a mandate to close was issued, were there any exceptions made for patients with certain conditions (eg, gamete banking before chemotherapy)?
Are you providing any fertility treatments?
If you answered “Yes” to question 7, what fertility treatments are being provided?
If a mandate to close ART centers was issued, are you aware of any centers that have remained open?
Are you aware of any reproductive health care providers that have contracted COVID-19?
Are you aware of any reproductive health care provider that have died from COVID-19?
Results
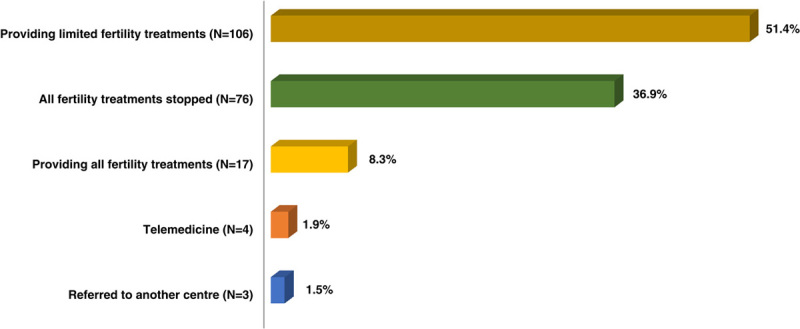
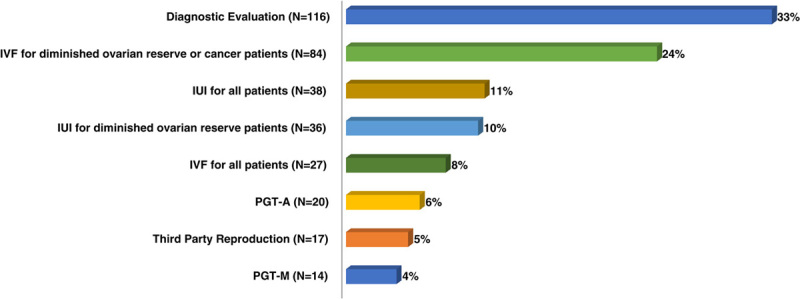
Respondents from 97 countries representing 6 continents completed the questionnaire (Figs. 1, 2). In 75% of countries, infertility services were not regarded as an essential medical service that should be continued through the SARS-CoV-2 pandemic and 60% modified policies regarding fertility treatment in response (Figs. 3, 4). In 82.5% of countries, ART centers were completely closed or only offered limited access for special circumstances and 14.5% had centers that were open with no restrictions to access (Figs. 5, 6). However, when individuals were queried about the status of their particular ART center 37.5% were closed due to government mandate and 56.5% offered limited access for special circumstances (Fig. 7). When ART centers were closed, closure was almost equally attributable to government mandate (33.1%), voluntary (32%), and professional guidelines (30.1%) (Fig. 8). If a mandate was issued, 66% of countries made provisions for exemptions for special circumstances such as gamete banking before chemotherapy or women with low ovarian reserves facing earlier loss of fertility potential (Fig. 9). Slightly over half (51.4%) of individual respondents continued to provide some MAR or ART (Fig. 10). Of those still active, one third were performing diagnostic testing, followed by 24% offering in vitro fertilization for special circumstances and 11% performing intrauterine inseminations (Fig. 11). Participants representing 38% of countries knew of ART centers that had defied national mandates and stayed open (Fig. 12). Regarding personal experiences, 21% of all of the respondents knew of reproductive health care providers that had contracted COVID-19 and 5% knew of deaths in this community (Figs. 13, 14).
Figure 1.
Are fertility treatments regarded as an essential medical service that should continue despite the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or COVID-19 pandemic in your country?
Figure 2.
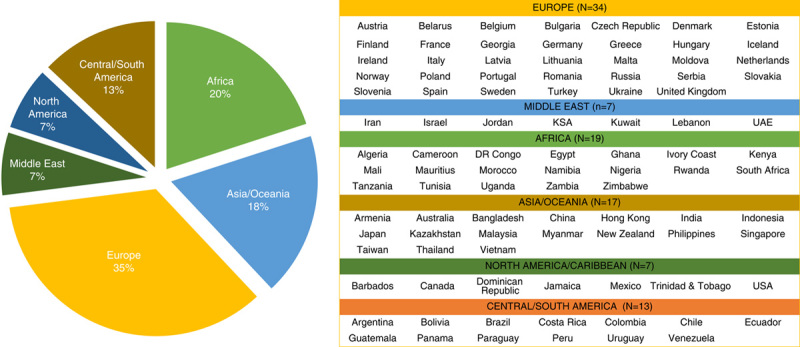
Distribution of countries.
Figure 3.
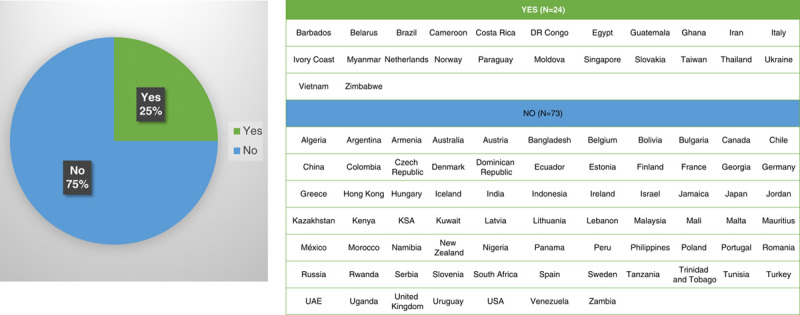
Are fertility treatments regarded as an essential medical service that should continue despite the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or COVID-19 pandemic in your country?
Figure 4.

Has your country modified its policy regarding fertility treatments along with the evolution of the COVID-19 pandemic?
Figure 5.
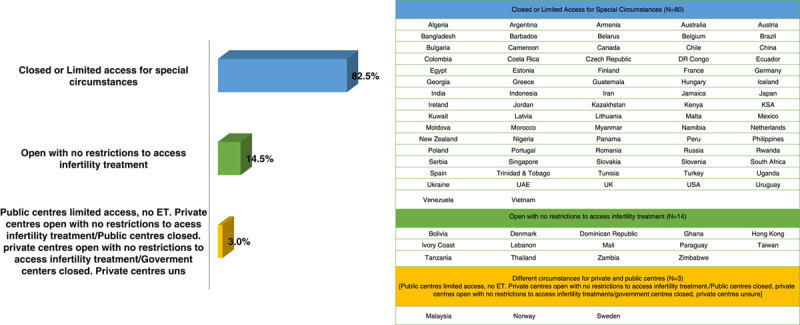
What is the status of assisted reproductive technology centers in your country in relation to the COVID-19 pandemic?
Figure 6.
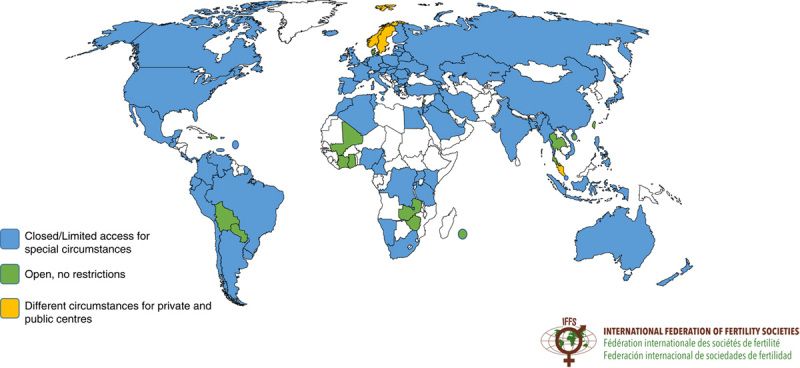
What is the status of assisted reproductive technology centers in your country in relation to the COVID-19 pandemic?
Figure 7.
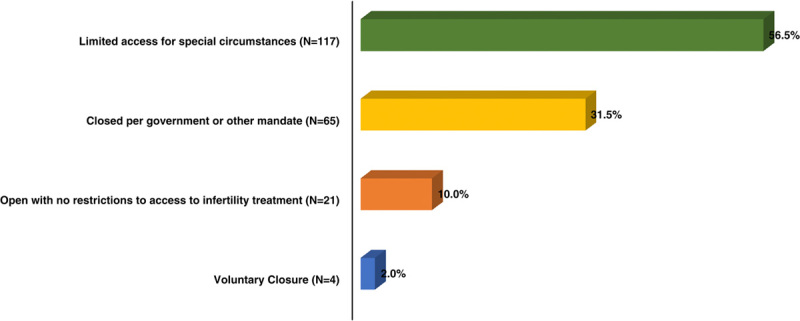
What is the status of your assisted reproductive technology center in relation to the COVID-19 pandemic?
Figure 8.
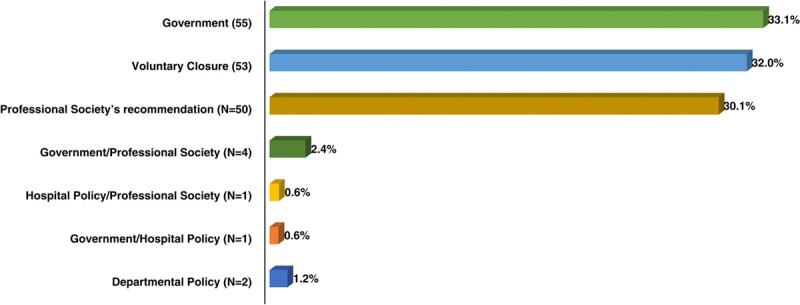
If your assisted reproductive technology center is closed, was the closure mandated by?
Figure 9.
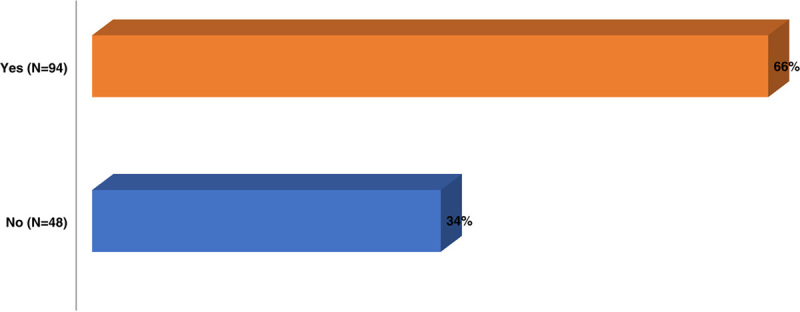
If a mandate to close was issued, were there any exceptions made for patients with certain conditions (eg, gamete banking before chemotherapy/diminished ovarian reserve)?
Figure 10.
Are you providing any fertility treatments?
Figure 11.
If you providing fertility treatments, what fertility treatments are being provided?
Figure 12.
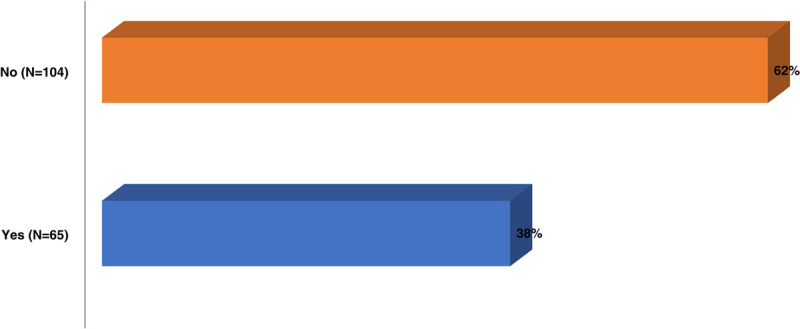
If a mandate to close assisted reproductive technology centers was issued, are you aware of any centers that have remained open?
Figure 13.
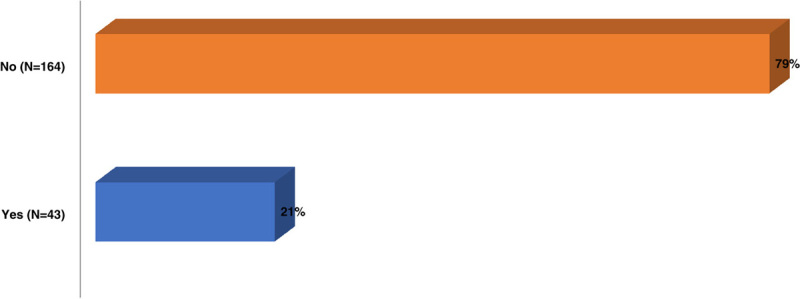
Are you aware of any reproductive health care providers that have contracted COVID-19?
Figure 14.

Are you aware of any reproductive health care provider that have died from COVID-19?
Discussion
These results attest to a reproductive health community that has largely been responsive to public health and individual patient concerns. As the full brunt of the pandemic unfolds, this survey records diverse responses to the challenge in different countries impacted differently and with variable resources. In a broader sense, they also reflect the variability in ART practice patterns noted in the more intensive review undertaken of global ART practices in International Federation of Fertility Societies’ Surveillance (IFFS) 2019: Global Trends in Reproductive Policy and Practice, 8th Edition8.
Countries that have implemented successful mitigation strategies are now grappling with the challenge of developing rational strategies to reactivate dormant economies without jeopardizing the progress already made in containing the virus. Considerable debate exists regarding the relative essential nature of infertility services although 3 societies, the American Society for Reproductive Medicine (ASRM), the European Society for Human Reproduction and Embryology (ESHRE), and the IFFS, representing >90% of global reproductive medicine practitioners, have recently issued a joint position statement affirming that reproduction is an essential human right that reproductive health professionals are uniquely suited to promote under the extraordinary circumstances posed by COVID-199. No professional body has recommended that women with presumptive normal fertility potential defer childbearing during the pandemic. Rather, they should be apprised of the limited state of our knowledge and that potential unknown risks may exist. As such, infertile couples should be extended the same opportunity to procreate as other individuals.
ASRM and ESHRE have issued guidance regarding relevant testing, counseling regarding risks of pregnancy with COVID-19, general recommendations for resuming various infertility treatments and for personal protective equipment (PPE), in addition to specific suggestions for recommencing specific ART services10,11. Their most recent references cited here are part of a series of reports that have been updated every few weeks. As critical information begins to emerge about this enigmatic virus, subsequent communications over the next 6–12 months should be able to provide more specific guidance for pregnancy based on data that is now being accrued.
Assistance with study
None.
Sources of funding
None.
Conflict of interest statement
The authors declare that they have no financial conflict of interest with regard to the content of this report.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 13 August 2020
References
- 1.Rasmussen SA, Jamieson DJ, Honein MA, et al. Zika virus and birth defects—reviewing the evidence for causality. N Engl J Med 2016;374:1981–7. [DOI] [PubMed] [Google Scholar]
- 2.British Fertility Society. British Fertility Society BFS Guidance for the care of fertility patients during the Coronavirus COVID19 Pandemic Comments. Available at: https://www.britishfertilitysociety.org.uk/2020/03/18/guidance-for-the-care-of-fertility-patients-during-the-coronavirus-covid-19-pandemic/ Accessed May 28, 2020.
- 3.ESHRE News. Available at: https://www.eshre.eu/Press-Room/ESHRE-News#COVID19P2 May 28, 2020.
- 4.American Society for Reproductive Medicine (ASRM). American Society for Reproductive Medicine (ASRM) Patient Management and Clinical Recommendations During the Coronavirus (COVID-19) PANDEMIC. Available at: https://www.asrm.org/globalassets/asrm/asrm-content/news-and-publications/covid-19/covidtaskforceupdate1.pdf Accessed May 28, 2020.
- 5.ESHRE News. Available at: https://www.eshre.eu/Press-Room/ESHRE-News#COVID19P2 Accessed May 28, 2020.
- 6.ASRM. Patient Management and Clinical Recommendations During the Coronavirus (COVID-19) Pandemic. Available at: https://www.asrm.org/news-and-publications/covid-19/statements/patient-management-and-clinical-recommendations-during-the-coronavirus-covid-19-pandemic/ Accessed May 28, 2020.
- 7.Johns Hopkins Coronavirus Resource Center. Available at: https://coronavirus.jhu.edu/map.htm Accessed May 28, 2020.
- 8.Global Reproductive Health. International Federation of Fertility Societies’ Surveillance (IFFS) 2019. Glob Reprod Health 2019;4:e29. [Google Scholar]
- 9.ASRM. American Society for Reproductive Medicine (ASRM) Patient Management and Clinical Recommendations During the Coronavirus (COVID-19) Pandemic. Available at: https://www.asrm.org/globalassets/asrm/asrm-content/news-and-publications/covid-19/covidtaskforceupdate4.pdf Accessed June 1, 2020.
- 10.COVID19WG. Available at: https://www.eshre.eu/Home/COVID19WG Accessed June 1, 2020.
- 11.Veiga A, Gianaroli L, Ory SJ, et al. COVID-19 and Human Reproduction Joint Statement: ASRM/ESHRE/IFFS. ASRM. Available at: https://www.asrm.org/news-and-publications/covid-19/statements/covid-19-and-human-reproduction-joint-statement-asrmeshreiffs/ Accessed June 1, 2020. [DOI] [PMC free article] [PubMed]