

Following the report of numerous cases and deaths in several countries during December 2019 and early 2020 due to a new coronavirus disease named COVID‐19, the World Health Organization (WHO) declared the disease a pandemic on March 11, 2020. By March 19, 2020, nearly all US states declared a state of emergency, and on March 20, the Florida governor signed an executive order mandating all health care practitioners licensed in the state cease performing nonemergency elective services. At the national level in the United States, the Society of Breast Imaging (SBI) and the COVID‐19 Pandemic Breast Cancer Consortium issued recommendations calling for delaying screening breast imaging examinations. 1
We conducted a retrospective observational nonhuman subject study with the goal of evaluating the impact that the response to COVID‐19 has had on breast imaging services across five breast imaging centers that provide services at a single or at multiple locations across eight cities in Miami‐Dade and Broward counties, South Florida. The number of breast imaging examinations and image‐guided procedures performed during the month of April 2020, time at which the participating centers were under COVID‐19 lockdown measures, was obtained. For historical data comparison, the same data were obtained for the month of April during the prior 2 years, 2018 and 2019. The number of breast imaging examinations performed during the month of April 2020 at a single breast imaging center in the area, which was under COVID‐19 lockdown measures in March 2020, but not during April 2020, was obtained and used as control. Specifically, the number of screening and diagnostic mammograms, breast ultrasounds, breast MRIs, image‐guided breast biopsies, positive (malignant) outcomes, and image‐guided presurgical breast localizations was obtained. Information on the type of practice setting and on the type of breast imaging examination and procedure under rescheduling measures during the study time was also collected. Data are presented as numbers and percent.
The participating centers had a balanced distribution of academic and private settings, and the control facility was in a private setting.
Scheduling changes in response to COVID‐19 were initiated at all facilities by mid‐March to late March 2020, and these changes remained in place into mid‐May to early June 2020 for a period ranging from 6 to 8 weeks. The control facility had lifted these changes by April. Changes to the schedule included rescheduling all screening breast imaging examinations (mammogram, ultrasound, and MRI) and image‐guided localization of high‐risk breast lesions at all facilities. Diagnostic examinations for symptomatic patients and recalls from abnormal screening examinations remained in the schedule at all facilities, while diagnostic mammograms for short‐term follow‐ups (BI‐RADS 3) were rescheduled at only one of the facilities (Table 1).
Table 1.
Breast imaging facility characteristics, COVID‐19 rescheduling duration, and breast imaging procedures affected, April 2020
| Facility A | Facility B | Facility C | Facility D | Facility E | Facility F (control) | |
|---|---|---|---|---|---|---|
| Type of practice | Academic | Private/academic | Academic | Private | Private | Private |
| Date rescheduling started | March 23 | March 23 | March 16 | March 18 | March 30 | March 20 |
| Date rescheduling concluded | May 18 | May 4 | May 11 | May 11 | May 11 | March 30 |
| Duration rescheduling in effect (wk) | 8 | 6 | 8 | 8 | 6 | 2 |
| Screening mammogram | R | R | R | R | R | R |
| Diagnostic—symptomatic patient | NR | NR | NR | NR | NR | R |
| Diagnostic—screening callback | NR | NR | NR | NR | NR | R |
| Diagnostic—BI‐RADS 3 | NR | R | NR | NR | NR | R |
| Biopsies | NR | NR | NR | NR | NR | R |
| Screening breast ultrasound | R | R | R | R | R | R |
| Screening breast MRI | R | R | R | R | R | R |
| Diagnostic breast MRI | NR | NR | NR | NR | NR | R |
| Image‐guided localization for cancer | R | R | NR | NR | NP | R |
| Image‐guided localization for high‐risk lesion | R | R | R | NR | NP | R |
Abbreviations: NP, procedure not offered at facility; NR, rescheduling did not take place; R, Rescheduling took place.
The five facilities under COVID‐19 rescheduling measures in April 2020 had a combined historic monthly average of approximately 7190 breast imaging procedures for the month of April 2018 and 2019. That number declined almost sevenfold, to approximately 1090 breast procedures in 2020 (Table 2).
Table 2.
Breast imaging procedures by breast imaging facility, April 2018 to 2020
| Facility A | Facility B | Facility C | Facility D | Facility E | Facility F (control) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2018 | 2019 | 2020 | 2018 | 2019 | 2020 | 2018 | 2019 | 2020 | 2018 | 2019 | 2020 | 2018 | 2019 | 2020 | |
| Screening mammogram | 614 | 695 | 1 | 292 | 317 | 2 | 257 | 545 | 1 | 284 | 362 | 4 | 1022 | 1056 | 97 | 535 | 558 | 135 |
| Diagnostic mammogram | 374 | 348 | 37 | 357 | 331 | 27 | 764 | 815 | 174 | 171 | 202 | 78 | 104 | 147 | 38 | 187 | 271 | 164 |
| Breast ultrasound | 275 | 225 | 32 | 619 | 643 | 48 | 426 | 532 | 138 | 218 | 330 | 60 | 218 | 389 | 89 | 401 | 526 | 246 |
| Breast MRI | 36 | 21 | 7 | 47 | 56 | 7 | 93 | 119 | 47 | 5 | 11 | 4 | 13 | 19 | 3 | NP | NP | 18 |
| Image‐guided breast biopsy | 65 | 51 | 15 | 97 | 141 | 45 | 114 | 129 | 65 | 28 | 29 | 10 | 5 | 12 | 0 | 31 | 34 | 34 |
| Positive (malignant) biopsy | 14 | 21 | 2 | 6 | 17 | 6 | 48 | 39 | 21 | 10 | 9 | 7 | 1 | 4 | 0 | 5 | 6 | 6 |
| Image‐guided presurgical localization | 7 | 9 | 2 | 16 | 16 | 5 | 20 | 17 | 20 | 4 | 3 | 5 | NP | NP | NP | NP | 2 | 2 |
| Total | 1385 | 1370 | 96 | 1434 | 1521 | 140 | 1722 | 2196 | 466 | 720 | 946 | 168 | 1363 | 1627 | 227 | 1159 | 1397 | 605 |
Abbreviation: NP, Procedure not offered at facility.
There was a steep decline in the number of all breast imaging examinations and procedures performed at each of the five facilities included in this study during the month of April 2020 as compared to the month of April of the prior 2 years (Table 2). In particular, there was a marked decrease in the number of screening mammograms, followed by breast ultrasound, diagnostic mammograms, and breast MRIs (Figure 1). The number of image‐guided breast biopsies and the number of biopsies with positive (malignant) results also showed a decrease, as did the number of image‐guided presurgical breast localizations (Figure 1).
FIGURE 1.
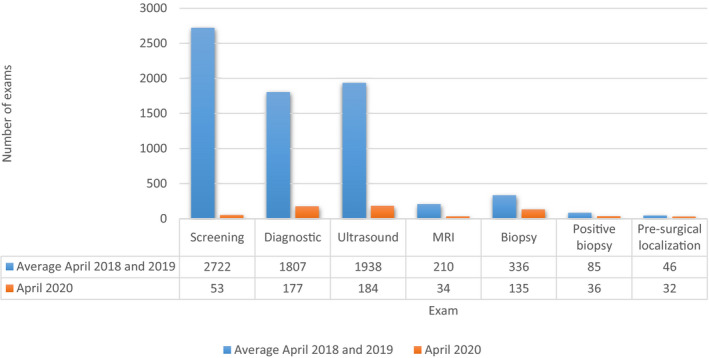
Breast imaging examinations and image‐guided procedures at five facilities under COVID‐19 rescheduling measures
Figure 2 shows that the percent change in the number of breast imaging examinations was more pronounced in the facilities under lockdown versus the control facility.
FIGURE 2.
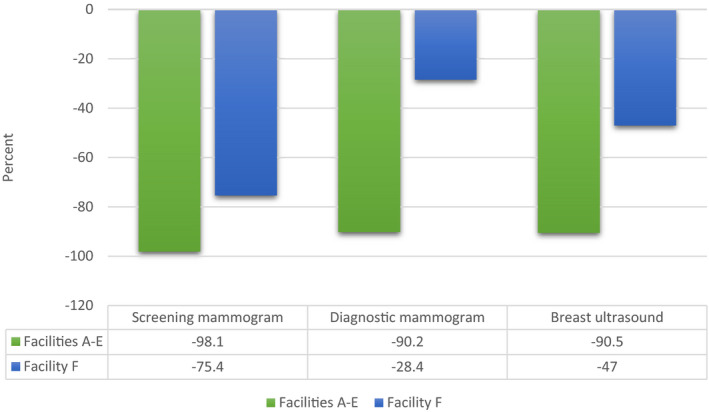
Percent decrease in number of breast imaging examinations during April 2020 as compared to April 2018‐2019. Facilities under COVID‐19 rescheduling measures (A‐E) versus control facility not under such measures (F)
To our knowledge, this is the first study to report on the impact that the response to COVID‐19 has had on breast imaging services across breast imaging facilities in South Florida. The facilities in this study vary in type from fully academic, mixed private/academic, and private, providing an examination of the impact of COVID‐19 across all aspects of breast imaging in a given community.
Similar decline in mammography services due to COVID‐19 was reported at a large health care system in New York. 2
Similar measures to reduce the risk of COVID‐19 transmission were implemented at other breast imaging centers across the United States. 3
The observed decline in the number of image‐guided presurgical breast localizations is in line with the recommendations made by the COVID‐19 Pandemic Breast Cancer Consortium, which called for elective surgeries to be canceled. This recommendation was made based on the fact that many patients with recently diagnosed breast cancer do not necessarily need immediate surgical resection, and can instead be initially treated with neo‐adjuvant chemotherapy or hormonal therapy. 4
Since the wide implementation of screening mammography in the United States, rescheduling and cancelation of breast imaging examinations and procedures have never taken place with such magnitude as during the time of COVID‐19. A recent conservative analysis of the impact these measures could have on breast cancer mortality suggests a ~1% increase in deaths, with the number of excess deaths per year expected to peak in the next year or two. 5 Thus, to ameliorate such an impact it is imperative for all breast imaging facilities that implemented rescheduling measures to keep clear records of and to contact all patients whose examinations and/or procedures were rescheduled or canceled. These patients should be rescheduled as soon as possible, so that any resulting delay in diagnosis and treatment of breast cancer is kept to the least possible time interval.
Finally, the results of this study could serve as a baseline for further studies on the long‐term consequences of COVID‐19 on breast imaging services.
REFERENCES
- 1. Society of Breast Imaging Statement on Breast Imaging during the COVID‐19 Pandemic. https://www.sbi‐online.org/Portals/0/Position%20Statements/2020/society‐of‐breast‐imagingstatement‐on‐breast‐imaging‐during‐COVID19‐pandemic.pdf. Accessed March 6, 2020.
- 2. Naidich JJ, Boltyenkov A, Wang JJ, Chusid J, Hughes D, Sanelli PC. Impact of the COVID‐19 pandemic on imaging case volumes. J Am Coll Radiol. 2020;17:865‐872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Moy L, Toth HK, Newell MS, Plecha D, Leung JWT, Harvey JA. Response to COVID‐19 in breast imaging. J Breast Imaging. 2020;2(3):180‐185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Recommendations for Prioritization, Treatment and Triage of Breast Cancer Patients During the COVID ‐19 Pandemic . The COVID‐19 Pandemic Breast Cancer Consortium. https://www.sbi‐online.org/Portals/0/Position%20Statements/2020/ASBrS‐NAPBC‐CoCNCCN‐ACR‐B‐Covid_Rev1‐4_7_2020.pdf. Accessed March 6, 2020. [DOI] [PMC free article] [PubMed]
- 5. Sharpless NE. COVID‐19 and cancer. Science. 2020;368(6497):1290. [DOI] [PubMed] [Google Scholar]