

Abstract
Aim
To clarify the status of personal protective equipment (PPE) and coronavirus disease 2019 (COVID‐19) tests for pregnant women, we conducted an urgent survey.
Methods
The survey was conducted online from April 27 to May 1, 2020. Questionnaires were sent to core facilities and affiliated hospitals of the obstetrics and gynecology training program and to hospitals of the national perinatal medical liaison council.
Results
A total of 296 institutions participated in our survey; however, 2 institutions were excluded. Full PPE was used by doctors in 7.1% of facilities and by midwives in 6.8%. Our study also determined that around 65.0% of facilities for doctors and 73.5% of facilities for midwives used PPE beyond the “standard gown or apron, surgical mask, goggles or face shield” during labor of asymptomatic women. N95 masks were running out of stock at 6.5% of the facilities and goggles and face shields at 2.7%. Disposable N95 masks and goggles or face shields were re‐used after re‐sterilization in 12% and 14% of facilities, respectively. Polymerase chain reaction (PCR) testing of asymptomatic patients was performed for 9% of vaginal deliveries, 14% of planned cesarean sections and 17% of emergency cesarean sections. The number of PCR tests for obstetrics and gynecology per a week ranged from zero to five in 92% of facilities.
Conclusion
The shortage of PPE in Japan is alarming. Sufficient stockpiling of PPE is necessary to prevent unnecessary disruptions in medical care. Appropriate guidelines for PPE usage and COVID‐19 testing of pregnant women at delivery are needed in Japan.
Keywords: COVID ‐19, personal protective equipment, polymerase chain reaction, pregnancy
Introduction
The novel coronavirus disease 2019 (COVID‐19), caused by a new strain of coronavirus identified as severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2), has been detected in patients with pneumonia of unknown cause beginning in December 2019 in Wuhan, China. Since then, a COVID‐19 pandemic has become full‐blown worldwide, which eventually resulted in the shortage of personal protective equipment (PPE). During childbirth, large amounts of aerosols are reportedly produced due to inevitable screaming, defecation and urination associated with labor and delivery. During this time, pregnant women and midwives are in close proximity, and ventilation in the delivery room is minimized for heat retention to keep the newborn warm. In order to prevent COVID‐19 transmission, medical workers should take precautions by wearing PPE.
In New York, the location recently identified as the epicenter of the pandemic, universal screening using a polymerase chain reaction (PCR)‐based test is a requirement before delivery for all pregnant women. This PCR screening has revealed that about 15% are infected with COVID‐19, of which about 90% (13.5% of total pregnant women) have asymptomatic infections. 1 In Japan, only a small number of PCR tests have been used for diagnosis of COVID‐19. There are reports of SARS‐CoV‐2 infection transmitted from asymptomatic infected individuals. 2 Therefore, the risk of infection is very high for medical workers attending to pregnant women with asymptomatic COVID‐19 during labor. A lack of available PCR tests for COVID‐19 has prompted the usage of PPE, which eventually resulted in its shortage. 3
In order to clarify the status of PPE usage during labor and delivery and COVID‐19 tests for pregnant women, we conducted an urgent survey in Japan.
Methods
The survey was conducted using online from April 27 to May 1, 2020. We carried out this online survey by two methods. The first method used snowball sampling techniques. The questionnaires were sent to the core facilities of obstetrics and gynecology training program, from which questionnaires were forwarded to the affiliated hospitals. The second method used mailing‐list of hospitals of national perinatal medical liaison council in Japan. In the survey, we gathered informed consent for the collection and publication of the results. We then incorporated the data from facilities that provided informed consent for analysis.
The questionnaire included the following items:
1. Location of the facility.
2. Annual number of deliveries.
3. Status of PPE use among doctors and midwives during labor of women without symptoms of COVID‐19.
4. Status of PPE use at outpatient clinics.
5. State of PPE stockpiling in the facility.
6. Status of COVID‐19 testing for asymptomatic women at vaginal delivery.
7. Status of COVID‐19 testing for asymptomatic women at cesarean section.
8. Status of COVID‐19 testing for asymptomatic patients at scheduled surgery (other than obstetric surgery).
9. Number of PCR tests available per week in the facility.
10. Number of PCR tests performed on obstetric and gynecologic patients per week prior to this survey.
Descriptive statistics were analyzed in the present survey. Full PPE is defined as gown‐type or one‐piece prevention wear, and using N95 masks, goggles, double gloves, caps and shoe covers and other is defined as not full PPE. According to the state of emergency on April 7, special warning area included in Tokyo, Osaka, Hokkaido, Ibaraki, Saitama, Chiba, Kanagawa, Ishikawa, Gifu, Aichi, Kyoto, Hyogo and Fukuoka. Each category variable between full PPE and not full PPE was performed by Chi‐square test or Fisher's exact test. All statistical analyses were performed using an assumed type I error rate of 0.05. Statistical analyses were performed using IBM spss Statistics 26 for Windows (IBM Japan).
Results
In this survey, we obtained questionnaire responses from 296 facilities including 117 (75%) of a total of 156 core facilities of obstetrics and gynecology training program, located in 46 prefectures throughout Japan. Also, 77 of the General and 100 Regional Perinatal Maternal and Child Care Center were included, representing 70% and 33% of the facilities nationwide, respectively. We excluded responses from two facilities that did not provide consent for publication; subsequently, we analyzed responses from the 294 facilities. The characteristics and locations of these facilities are shown in Table 1. The number of annual deliveries at the General Perinatal Maternal and Child Care Center was determined to be higher than that of the Regional Perinatal Maternal and Child Care Center or other facilities (P < 0.01).
Table 1.
Annual number of deliveries according to characteristics and location of facilities
| Number of deliveries | Total | 0 | ≤350 | 351–500 | 501–700 | ≥701 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | P‐value* | |
| Total | 294 | 100 | 12 | 4.1 | 82 | 27.9 | 72 | 24.5 | 62 | 21.1 | 66 | 22.4 | |
| General PMCC | 77 | 26.2 | 0 | 0.0 | 6 | 7.8 | 15 | 19.5 | 26 | 33.8 | 30 | 39.0 | |
| Regional PMCC | 100 | 34.0 | 0 | 0.0 | 35 | 35.0 | 30 | 30.0 | 17 | 17.0 | 18 | 18.0 | <0.001 |
| Others | 117 | 39.8 | 12 | 10.3 | 41 | 35.0 | 27 | 23.1 | 19 | 16.2 | 18 | 15.4 | |
| Hokkaido | 19 | 6.5 | 1 | 5.3 | 4 | 21.1 | 3 | 15.8 | 8 | 42.1 | 3 | 15.8 | |
| Tohoku | 15 | 5.1 | 0 | 0.0 | 6 | 40.0 | 4 | 26.7 | 3 | 20.0 | 2 | 13.3 | |
| Kanto | 95 | 32.3 | 4 | 4.2 | 19 | 20.0 | 26 | 27.4 | 15 | 15.8 | 31 | 32.6 | |
| Chubu | 40 | 13.6 | 1 | 2.5 | 17 | 42.5 | 9 | 22.5 | 7 | 17.5 | 6 | 15.0 | 0.262 |
| Kinki | 60 | 20.4 | 4 | 6.7 | 16 | 26.7 | 15 | 25.0 | 10 | 16.7 | 15 | 25.0 | |
| Chugoku | 17 | 5.8 | 0 | 0.0 | 3 | 17.6 | 7 | 41.2 | 5 | 29.4 | 2 | 11.8 | |
| Shikoku | 12 | 4.1 | 0 | 0.0 | 4 | 33.3 | 2 | 16.7 | 4 | 33.3 | 2 | 16.7 | |
| Kyushu | 36 | 12.2 | 2 | 5.6 | 13 | 36.1 | 6 | 16.7 | 10 | 27.8 | 5 | 13.9 | |
| Special warning area † | 187 | 63.6 | 4 | 3.7 | 35 | 32.7 | 28 | 26.2 | 26 | 24.3 | 14 | 13.1 | 0.060 |
| Others | 107 | 36.4 | 8 | 4.3 | 47 | 25.1 | 44 | 23.5 | 36 | 19.3 | 52 | 27.8 | |
Chi‐square test.
Tokyo, Osaka, Hokkaido, Ibaraki, Saitama, Chiba, Kanagawa, Ishikawa, Gifu, Aichi, Kyoto, Hyogo, Fukuoka.
PMCC: Perinatal Maternal and Child Care Center.
Status of PPE use among doctors and midwives during labor of women without symptoms of COVID‐19
We defined full PPE as gown‐type or one‐piece prevention wear, N95 masks, goggles, double gloves, caps and shoe covers. In vaginal deliveries of women without symptoms of COVID‐19, full PPE was used by doctors in 7.1% of facilities and by midwives in 6.8% of facilities. Full PPE was most commonly adopted by facilities with 351–500 deliveries per year, of which 16.7% were reportedly used by doctors and 15.3% by midwives (Table 2). Overall, approximately 90% of the facilities lacking full PPE use employed water‐repelling gowns or aprons. Goggles or face shields were used by doctors in 63% of facilities and by midwives in 73% of facilities. Both doctors and midwives wore fewer shoe covers and caps (Fig. 1).
Table 2.
Status of PPE use among doctors and midwives during labor of women without symptoms of COVID‐19
| Total | Full PPE † of doctor | P‐value* | Full PPEa of midwife | P‐value* | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Full | Not full | Full | Not full | |||||||
| n | % | n | % | n | % | n | % | |||
| 21 | 7.1 | 273 | 92.9 | 20 | 6.8 | 274 | 93.2 | |||
| Annual number of deliveries | ||||||||||
| ≤350 | 4 | 4.2 | 90 | 95.8 | 4 | 4.2 | 90 | 95.8 | ||
| 351–500 | 12 | 16.7 | 60 | 83.3 | 0.660 | 11 | 15.3 | 61 | 84.7 | 0.567 |
| 501–700 | 2 | 3.2 | 60 | 96.8 | 3 | 4.8 | 59 | 95.2 | ||
| ≥701 | 3 | 4.5 | 63 | 95.5 | 2 | 3.0 | 64 | 97.0 | ||
| General PMCC | 7 | 9.1 | 70 | 90.9 | 5 | 6.5 | 72 | 93.5 | ||
| Regional PMCC | 9 | 9.0 | 91 | 91.0 | 0.299 | 9 | 9.0 | 91 | 91.0 | 0.525 |
| Others | 5 | 4.3 | 112 | 95.7 | 6 | 5.1 | 111 | 94.9 | ||
| University hospital | 4 | 4.9 | 77 | 95.1 | 0.365 | 3 | 3.7 | 78 | 96.3 | 0.193 |
| Others | 17 | 8.0 | 196 | 92.0 | 17 | 8.0 | 196 | 92.0 | ||
| Hokkaido | 0 | 0.0 | 19 | 100 | 0 | 0.0 | 19 | 100 | ||
| Tohoku | 1 | 6.7 | 14 | 93.3 | 1 | 6.7 | 14 | 93.3 | ||
| Kanto | 6 | 6.3 | 89 | 93.7 | 6 | 6.3 | 89 | 93.7 | ||
| Chubu | 3 | 7.5 | 37 | 92.5 | 3 | 7.5 | 37 | 92.5 | ||
| Kinki | 5 | 8.3 | 55 | 91.7 | 0.599 | 4 | 6.7 | 56 | 93.3 | 0.588 |
| Chugoku | 0 | 0.0 | 17 | 100 | 0 | 0.0 | 17 | 100 | ||
| Shikoku | 1 | 8.3 | 11 | 91.7 | 1 | 8.3 | 11 | 91.7 | ||
| Kyushu | 5 | 13.9 | 31 | 86.1 | 5 | 13.9 | 31 | 86.1 | ||
| Special warning area ‡ | 12 | 6.4 | 175 | 93.6 | 0.523 | 10 | 5.3 | 177 | 94.7 | 0.190 |
| Others | 9 | 8.4 | 98 | 91.6 | 10 | 9.3 | 97 | 90.7 | ||
Chi‐square test or Fisher's exact test.
Full PPE is gown‐type or one‐piece prevention wear, N95 masks, goggles, double gloves, caps, and shoe covers.
Tokyo, Osaka, Hokkaido, Ibaraki, Saitama, Chiba, Kanagawa, Ishikawa, Gifu, Aichi, Kyoto, Hyogo, Fukuoka.
COVID‐19, coronavirus disease 2019; PMCC: Perinatal Maternal and Child Care Center, PPE: personal protective equipment.
Figure 1.
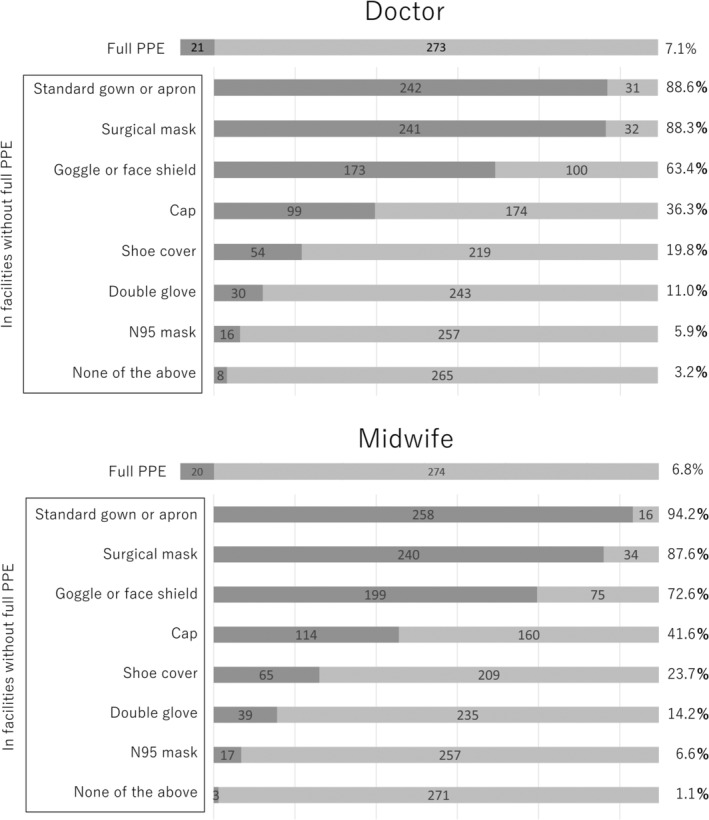
Status of personal protective equipment (PPE) use among doctors and midwives during labor of women without COVID‐19, coronavirus disease 2019 (COVID‐19) symptoms. (◼), Yes; (□), No.
Status of PPE use beyond “standard gown or apron, surgical mask, goggle or face shield” during labor of women without symptoms of COVID‐19
We defined the standard protection during vaginal delivery for asymptomatic women as a standard gown apron, surgical mask and goggles or face shield. Protective equipment for COVID‐19 beyond this standard protection was used by doctors in 65.0% of facilities and by midwives in 73.5% of facilities, with higher rates of use in facilities with a large number of deliveries (doctors P < 0.01, midwives P < 0.01). Doctors used this additional PPE at a higher rate of 70.6% in special warning areas compared to other areas (P < 0.01) (Table 3).
Table 3.
Status of PPE use beyond “standard gown or apron, surgical mask, goggle or face shield” during labor of women without symptoms of COVID‐19
| Total | Beyond standard PPE † use of doctor | Beyond standard PPE † use of midwife | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | P‐value* | Yes | No | P‐value* | |||||
| n | % | n | % | n | % | n | % | |||
| 191 | 65.0 | 103 | 35.0 | 216 | 73.5 | 78 | 26.5 | |||
| Number of deliveries per year | ||||||||||
| ≤350 | 51 | 54.3 | 43 | 45.7 | 56 | 59.6 | 38 | 40.4 | ||
| 351–500 | 45 | 62.5 | 27 | 37.5 | <0.001 | 52 | 72.2 | 20 | 27.8 | <0.001 |
| 501–700 | 40 | 64.5 | 22 | 35.5 | 49 | 79.0 | 13 | 21.0 | ||
| ≥701 | 55 | 83.3 | 11 | 16.7 | 59 | 89.4 | 7 | 10.6 | ||
| General PMCC | 57 | 74.0 | 20 | 26.0 | 66 | 85.7 | 11 | 14.3 | ||
| Regional PMCC | 67 | 67.0 | 33 | 33.0 | 0.792 | 73 | 73.0 | 27 | 27.0 | 0.661 |
| Others | 67 | 57.3 | 50 | 42.7 | 77 | 65.8 | 40 | 34.2 | ||
| University hospital | 56 | 69.1 | 25 | 30.9 | 0.205 | 61 | 75.3 | 20 | 24.7 | 0.142 |
| Others | 135 | 63.4 | 78 | 36.6 | 155 | 72.8 | 58 | 27.2 | ||
| Hokkaido | 10 | 52.6 | 9 | 47.4 | 13 | 68.4 | 6 | 31.6 | ||
| Tohoku | 5 | 33.3 | 10 | 66.7 | 11 | 73.3 | 4 | 26.7 | ||
| Kanto | 72 | 75.8 | 23 | 24.2 | 74 | 77.9 | 21 | 22.1 | ||
| Chubu | 27 | 67.5 | 13 | 32.5 | 0.224 | 31 | 77.5 | 9 | 22.5 | 0.240 |
| Kinki | 38 | 63.3 | 22 | 36.7 | 42 | 70.0 | 18 | 30.0 | ||
| Chugoku | 10 | 58.8 | 7 | 41.2 | 12 | 70.6 | 5 | 29.4 | ||
| Shikoku | 6 | 50.0 | 6 | 50.0 | 9 | 75.0 | 3 | 25.0 | ||
| Kyushu | 23 | 63.9 | 13 | 36.1 | 24 | 66.7 | 12 | 33.3 | ||
| Special warning area ‡ | 132 | 70.6 | 55 | 29.4 | 0.004 | 141 | 75.4 | 46 | 24.6 | 0.111 |
| Others | 59 | 55.1 | 48 | 44.9 | 75 | 70.1 | 32 | 29.9 | ||
Chi‐square test or Fisher's exact test;
Standard PPE is standard gown or apron, surgical mask, goggle or face shield.
Tokyo, Osaka, Hokkaido, Ibaraki, Saitama, Chiba, Kanagawa, Ishikawa, Gifu, Aichi, Kyoto, Hyogo, Fukuoka.
COVID‐19, coronavirus disease 2019; PMCC: Perinatal Maternal and Child Care Center, PPE: personal protective equipment.
PPE status at outpatient clinics
Doctors in 42 facilities (14.3%) used goggles or face shields at outpatient clinics.
In‐hospital stockpiling of PPE
Regardless of the characteristics and locations of facilities, protective equipment of the trunk – a standard gown or apron – was sufficient in about 36.5% of facilities. N95 masks and goggles or face shields were also found sufficient only in 10.5% and 14.6% of facilities, respectively, and for the rest, PPE were re‐used after re‐sterilization in 12.2% and 14.3% of facilities, respectively. N95 masks and goggles or face shields were reported to be out of stock in 6.5% and 2.7% of facilities, respectively (Fig. 2, Table S1).
Figure 2.
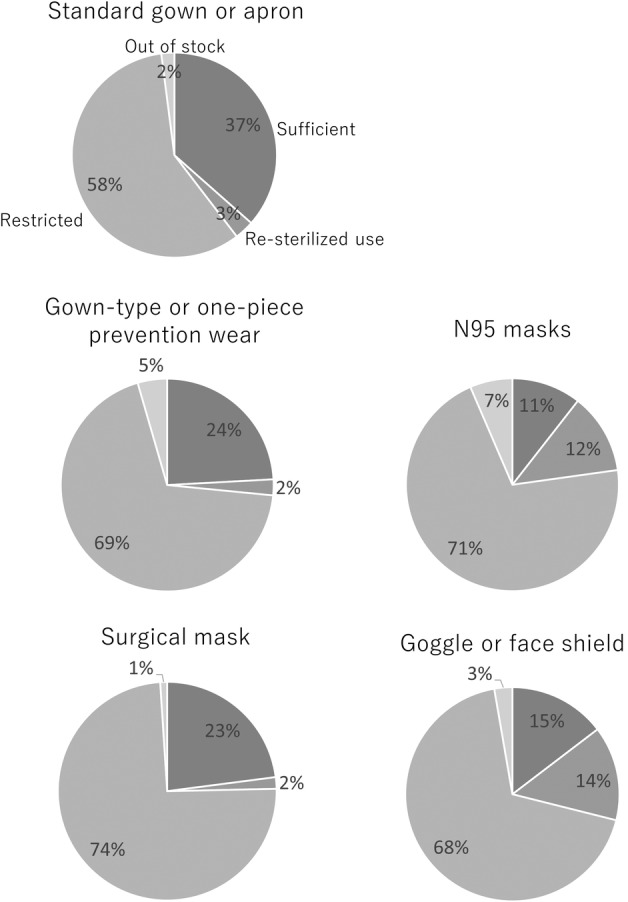
In‐hospital stockpiling of personal protective equipment (PPE). ( ), Sufficient; (
), Sufficient; ( ), re‐sterilized use; (
), re‐sterilized use; ( ) restricted; and (
) restricted; and ( ) out of stock.
) out of stock.
COVID‐19 testing status
Figure 3 shows the percentage of facilities that provide COVID‐19 tests for asymptomatic women. Pregnant women were tested for COVID‐19 not only in perinatal medical centers and university hospitals, but also other facilities, at a rate of 9–17% (Table S2). PCR testing of asymptomatic women was performed by 9% of facilities at vaginal delivery, 14% at planned cesarean section, 17% at emergency cesarean section and 15% at nonobstetric or nongynecological surgery.
Figure 3.
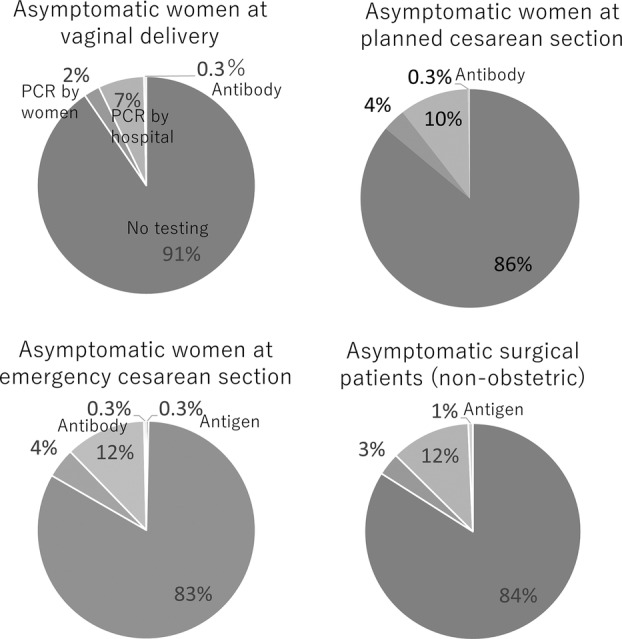
Facilities undergoing COVID‐19, coronavirus disease 2019 (COVID‐19) testing of asymptomatic women. ( ), no testing; (
), no testing; ( ), PCR by women; (
), PCR by women; ( ), PCR by hospital; (
), PCR by hospital; ( ), antibody test and (
), antibody test and ( ) antigen test
) antigen test
Between April 27 and May 1, 2020, 18 facilities (6.1%) have reported that they were performing PCR tests on all asymptomatic pregnant women admitted for labor and nonobstetric or nongynecological surgery. We performed a secondary interview in early May to confirm these reports and found that all pregnant women (vaginal delivery, planned and emergency cesarean section) received the PCR test at eight facilities nationwide, and six of the eight additionally tested all surgical patients.
PCR testing capacity
Approximately 61% of the participating facilities revealed that they performed PCR tests on less than 50 samples per week (Fig. 4). The number of PCR examinations available per week was higher in the General Perinatal Maternal and Child Care Center (P < 0.001) and university hospitals (P < 0.001) than in other facilities; it was also higher in special warning areas (P < 0.05) (Table S3). However, during the week prior to the survey, 92% of the facilities performed less than five PCR tests (Fig. 5).
Figure 4.
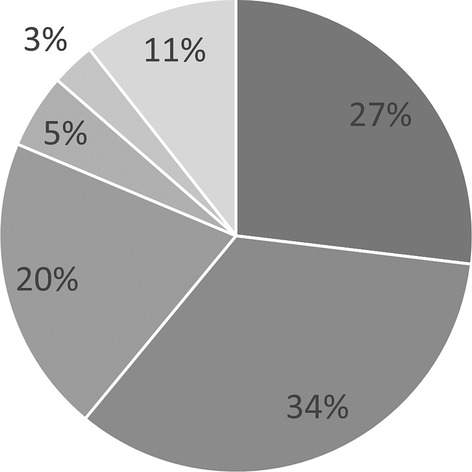
Number of weekly polymerase chain reaction (PCR) tests available. ( ), <50; (
), <50; ( ), 51–100; (
), 51–100; ( ), 101–150; (
), 101–150; ( ), 151–200 and (
), 151–200 and ( ) >200
) >200
Figure 5.
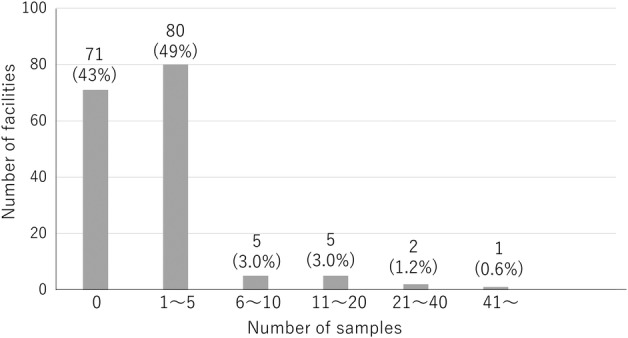
Number of polymerase chain reaction (PCR) tests performed on obstetric and gynecologic patients during the week prior to the survey.
Discussion
This is the first report that showed the nationwide state of the PPE and COVID‐19 testing. This survey clarified the actual PPE usage in core facilities and affiliated hospitals of the obstetrics and gynecology training program as well as hospitals of the national perinatal medical liaison council, between April 27 and May 1, 2020. During this time, Japan was in a national state of emergency due to the spread of COVID‐19 infections.
In New York, 14 of the 43 (33%) asymptomatic pregnant women tested positive for COVID‐19, 10 (71%) of which developed symptoms after PCR tests. 4 Furthermore, COVID‐19 screening among 215 pregnant women found that 32 (15%) tested positive, of which 29 (13.5% overall) were found asymptomatic. 1 Asymptomatic patients are contagious and thus are at a high risk of nosocomial infection. 2 Of those infected at a single institution, 41% were nosocomial and 29% were healthcare workers. 5 Therefore, if universal screening is not performed, strict PPE usage for doctors and midwives is necessary at labor when large amounts of aerosols are produced. However, this situation may result in the depleting supply of PPE in facilities, and the burden of wearing full PPE on healthcare professionals will become heavier.
In this survey, full PPE was used by doctors in 7.1% of facilities and by midwives in 6.8% of facilities (Table 2). However, N95 masks and goggles or face shields were out of stock in 6.5% and 2.7% of facilities, respectively. In addition, disposable N95 masks and goggles or face shields were re‐used after re‐sterilization in 12% and 14% of facilities, respectively (Fig. 2). The shortage of medical PPE in Japan is very alarming.
We determined that stockpiling was altered because facilities increased their normal stockpiling systems, rather than facilities increased their consumption due to the degree of COVID‐19 infection spread. This was apparent because locations of special warning areas were unrelated to stockpiling status.
The number of PCR tests administered to obstetric and gynecologic patients in the week prior to this survey ranged from zero to five in 92% of facilities (Fig. 5). However, 61% of the facilities administered less than 50 PCR tests per week, indicating that the majority of facilities were limited in their capacity for PCR testing (Fig. 4).
France ended their lockdown when 4.4% of the population had been infected, at which time population immunity was considered inadequate to avoid a second wave. 6 In Japan, sufficient stockpiling of PPE is needed to prevent disruptions in medical care due to nosocomial infections until adequate mass immunity is slowly achieved. Appropriate guidelines for PPE usage by medical providers and COVID‐19 testing for pregnant women before delivery are necessary in Japan.
Disclosure
None declared.
Supporting information
Table S1: Stockpiling of PPE according to characteristics and location of facilities
Table S2. COVID‐19 tests according to characteristics and location of facilities (multiple selection
Table S3. Number of PCR tests available per week in the facility
References
- 1. Sutton D, Fuchs K, D'Alton M, Goffman D. Universal screening for SARS‐CoV‐2 in women admitted for delivery. N Engl J Med 2020; 382: 2163–2164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rothe C, Schunk M, Sothmann P et al. Transmission of 2019‐nCoV infection from an asymptomatic contact in Germany. N Engl J Med 2020; 382: 970–971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mehrotra P, Malani P, Yadav P. Personal protective equipment shortages during COVID‐19—supply chain–related causes and mitigation strategies. JAMA Health Forum 2020. [Cited 12 May, 2020]. Available from URL: https://jamanetwork.com/channels/health-forum/fullarticle/2766118 [DOI] [PubMed]
- 4. Breslin N, Baptiste C, Gyamfi‐Bannerman C et al. COVID‐19 infection among asymptomatic and symptomatic pregnant women: Two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am J Obstet Gynecol MFM 2020; 2: 100118. 10.1016/j.ajogmf.2020.100118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wang D, Hu B, Hu C et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus‐infected pneumonia in Wuhan, China. JAMA 2020. Feb 7; 323: 1061–1069. 10.1001/jama.2020.1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Salje H, Tran Kiem C, Lefrancq N et al. Estimating the Burden of SARS‐CoV‐2 in France. Science 2020; 369: 208–211. 10.1126/science.abc3517. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1: Stockpiling of PPE according to characteristics and location of facilities
Table S2. COVID‐19 tests according to characteristics and location of facilities (multiple selection
Table S3. Number of PCR tests available per week in the facility