

Abstract
The COVID‐19 pandemic has resulted in an international shortage of personal protective equipment including N95 filtering facepiece respirators (FFRs), resulting in many institutions using ultraviolet germicidal irradiation (UVGI) technology for N95 FFR decontamination. To ensure proper decontamination, it is crucial to determine the dose received by various parts of the FFR in this process. Recently, our group customized a UVGI unit for N95 decontamination. With experimental and theoretical approach, this manuscript discusses the minimum dose received by various parts of the N95 respirator after one complete decontamination cycle with this UVGI unit. The results demonstrate that all parts of the N95 FFR received at least 1 J cm−2 after one complete decontamination cycle with this unit. As there are a variety of UVGI devices and different types of FFRs, this study provides a model by which UVC dose received by different areas of the FFRs can be accurately assessed to ensure proper decontamination for the safety of healthcare providers.
The COVID‐19 pandemic has resulted in an international shortage of personal protective equipment including N95 filtering facepiece respirators (FFRs), resulting in many institutions using ultraviolet germicidal irradiation (UVGI) technology for N95 FFR decontamination. To ensure proper decontamination, it is crucial to determine the dose received by various parts of the FFR in this process (recommended dose 1 J cm−2). As there are a variety of UVGI devices and different types of FFRs, this study provides a model by which UVC dose received by different areas of the FFRs can be accurately assessed to ensure proper decontamination for the safety of healthcare providers.
![]()
Introduction
The COVID‐19 pandemic has resulted in a shortage of personal protective equipment (PPE) including N95 filtering facepiece respirators (FFRs). As such, decontamination methods, such as ultraviolet germicidal irradiation (UVGI), are being utilized for their reuse. The decontamination efficacy of UVGI has been well documented in the literature with a >3 log reduction achieved after UVGI treatment with various doses (1, 2, 3, 4). Possible explanations for the variations in UVGI dosing may include (1) differences in the pathogens as each would need a dose based on the specific biologic formation, (2) the variation between substrates used which may be porous or nonporous, flat or curved, and (3) the distance from and uniformity of the UVGI radiation source (5, 6, 7). With multiple institutions repurposing their UVGI technology for N95 decontamination, hospital systems across the United States have started utilizing UVGI for FFR decontamination and reuse. Dosing is a crucial parameter, and insufficient doses would result in incomplete decontamination which can be hazardous to the healthcare worker. A dose of at least 1 J cm−2 has been recommended for N95 decontamination (8, 9, 10, 11). Considering that the UVC photons are only effective if they make direct contact with the surface and that N95 respirators have a curvature, it is important to account for the actual dose received by various parts of the respirator within the repurposed unit. Recently, our group customized a UVGI unit for N95 decontamination and reuse, referred to as Daavlin unit in this manuscript (4). With an experimental and theoretical approach, this manuscript discusses the minimum dose received by various parts of the N95 respirator after one complete decontamination cycle with this UVGI unit. This method, to determine the dose received by various parts of the N95 respirator, can be utilized as a model for other UVC units repurposed for N95 decontamination. In addition, parameters that healthcare institutions across the country might consider when investing and utilizing a UVGI unit for the purpose of N95 decontamination have also been suggested.
Materials and Methods
Daavlin desktop UVC germicidal lamp (Daavlin, Byron, OH), referred to as Daavlin unit in the manuscript, was utilized for UVGI irradiation (4). A 3M 1860 N95 FFR was utilized as a model FFR. To measure the variation in the dose received by various parts of the N95 FFR, two different factors were considered—the impact of the curvature of the N95, and the distance of the irradiated site from the lamp. To account for the effect of the FFR curvature, irradiance was measured at various angles between the surface normal and incident UVC. Fig. 1a is a schematic of the orientations of surface normal on a representative N95 respirator. Measurements were made by orienting a UVC sensor at angles ranging from 0‐90° between surface normal of the sensor and incident UVC (Fig. 1b). A calibrated UVC meter UV512C (General Tools and Instrument, Secaucus, NJ) was utilized. The sensor was placed on the stainless‐steel mayo stand tray, readily available in clinical settings, when making measurements. Of note, the tray/table was approximately 14 cm from the lamp, and the sensor was about 11.5 cm (height of sensor 2.5 cm) (Fig. 1b).
Fig. 1.
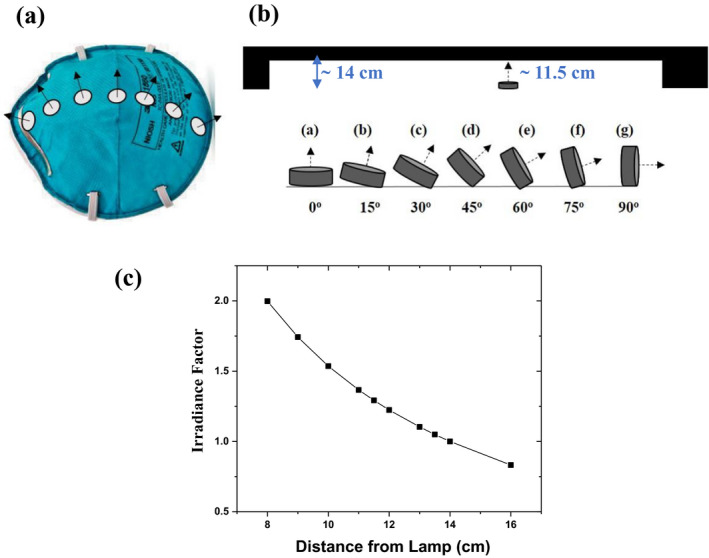
(a) Schematic of the surface normal from various parts of a representative N95 respirator, and (b) schematic of sensor orientations (0–90°) at which irradiance measurements were made (c) Irradiance factor as a function of distance from the lamp
To estimate the effect of distance on irradiance, a simplistic approach was to consider that a radiation source, including a UVC lamp, is a point source that irradiates uniformly in all directions. In this case, irradiance at a distance r from the source follows the inverse square law and is proportional to 1/r 2, where r is the distance from the lamp (12). However, this approximation is valid only when irradiance is measured at distances greater than five times the longest dimension of the source. The longest dimension of the lamp used in the Daavlin unit was approximately 38.5 cm, and the tray containing the N95 FFRs was placed at a distance of approximately 14 cm from it. Since this distance is much smaller than five times of the longest dimension of the lamp (5*38.5 = 192.5 cm), it made the point source approximation invalid in this situation. To make a conservative approximation of the variation in intensity with distance from the lamp, with detector directly facing the lamp, line source model (13) described by the Eq. 1 was utilized instead.
| (1) |
Here, E is the irradiance, is the intensity per unit length, ɸ is the useful UVC intensity (at 254 nm), L is the length of the lamp, h is the distance from the end of the lamp (for a point located at the midpoint of the lamp h = L/2), and d is distance between lamp and irradiated site. ɸ was approximated to be 12 W which is about one third of the wattage of the UVC lamp (36 W), L was 38.5 cm (the length of the UVC lamp), h was used as L/2, and d was varied to account for change in irradiance with distance from the lamp. Equation 1 was utilized to calculate the irradiance factor. This factor, in combination with the measured irradiance values with the UVC meter, provided the irradiance variation as a function of distance from the lamp. Equation 1 is applicable to all systems with set up similar to the one discussed in this manuscript, namely, Daavlin unit with tubular lamps. As discussed above, the irradiance estimation approach (approximately 1/r vs 1/r 2) is impacted by the device geometry, type of lamp, distance between the lamp and N95, etc., and should be selected accordingly.
Additional experiments were also performed with UV strips. Tesa UV strips 54140 (©tesa SE – A Beiersdorf Company, UK) were utilized which consisted of UVC sensitive polymer film that changes color after exposure to UVC. UV dosage was measured using a compatible Hoenle UV scan (Hoenle UV America, Inc., Marlboro, MA) that determines the UVC dose received based on the change in color. The strips had a linear detection range up to 200 mJ cm−2. Hoenle scan measurements were calibrated against those made by the UV sensor integrated within the Daavlin unit. This was done by placing the UV strips at a fixed distance from the lamp and comparing the doses measured by the UV scan to those by the sensor integrated within the Daavlin unit located at the top of the unit above the lamp. Following this, the strips were utilized to (1) validate the accuracy and consistency of the above‐mentioned experiments by placing the UV strip at the top of the N95 respirator and at the curved surface (Fig. 2a) and (2) to investigate the percentage of UVC penetration through all the layers of the N95 FFR by placing the UV strip on the side being directly and indirectly irradiated (Fig. 2b).
Fig. 2.
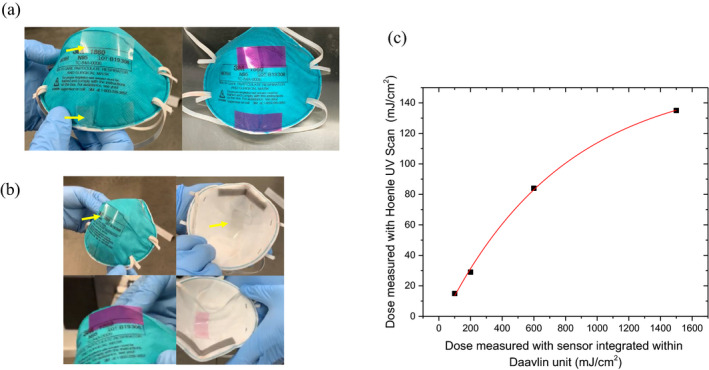
(a) N95 respirator with UV strips placed at the surface closest to the lamp and at the edge (yellow arrows). Left: before and right: after UVC treatment. Note the strip changed color after UV exposure. (b) Strips placed at surface being directly and indirectly irradiated. Upper panel: before irradiation, lower panel: after irradiation. (c) Hoenle UV scan dose measurements as a function of dose measured with UV sensor integrated within the Daavlin unit
Results
To measure the variation in the dose received by various parts of the N95 FFRs, two different factors were considered—the first being the impact of the curvature of the N95 and the second being the distance of the irradiated site from the lamp. For the Daavlin unit, the effect of the FFR curvature was accounted by measuring the irradiance at various angles between the surface normal (Fig. 1a) and incident UVC. With the sensor facing the incident UVC radiation (orientation a in Fig. 1b), an irradiance of approximately 10 mW cm−2 with less than 10% variation was measured at various sites within the irradiation area. However, as expected, with changes in sensor orientation, a reduction in irradiance by less than a factor of 2 was observed between the two extreme orientations from 10.2 mW cm−2 (at orientation a in Fig. 1b) to 6.2 mW cm−2 (at orientation g in Fig. 1b). Considering that the N95 respirator has a small curvature, it can be approximated that the lowest irradiance received at the curved surface corresponds to the sensor orientation f in Fig. 1b. Toward the edge of the unit, the measured irradiance for this orientation was 4.0 mW cm−2. In order to minimize the effect of irradiance variation near the edges of the unit, for the Daavlin unit, it is suggested that the placement of the respirators be such that there is at least a 10 cm distance between the edge of the N95 respirator and the unit edge on the controller side and approximately 5 cm on the other side. This recommendation is based on the lamp positioning within the unit. This will ensure that the lowest irradiance is at least 6 mW cm−2. As such, curved parts of the N95 respirator closer to the tray will observe 60% of the dose administered referred to as curvature factor in Table 1.
Table 1.
Representative calculations for observed dose considering irradiation of outside‐facing surface with 1.5 J cm−2
| Distance from Lamp (cm) | Curvature factor | Irradiance factor | Received dose (Eq. 2) (J cm−2) |
|---|---|---|---|
| 8 | 1.000 | 1.998 | 2.997 |
| 9 | 0.918 | 1.742 | 2.401 |
| 10 | 0.903 | 1.536 | 2.080 |
| 11 | 0.867 | 1.366 | 1.778 |
| 12 | 0.750 | 1.224 | 1.378 |
| 13 | 0.602 | 1.104 | 0.997 |
| 14 | 0.602 | 1.000 | 0.903 |
Following the effect of curvature, the effect of distance of the irradiated site from the lamp was investigated. For the Daavlin unit, when a dose of 1.5 J cm−2 was entered into the control panel, the time was automatically accounted for by the UV sensor integrated into the unit. The sensor, located at the top of the unit above the lamp, was calibrated to use irradiance at a distance of 14 cm from the UVC lamp which corresponded to the distance between the lamp and the table/tray surface (Fig. 1b). Areas closer to the lamp should observe a higher irradiance resulting in a higher dose received. Irradiance factor, shown in Fig. 1c, was calculated from Eq. 1 by normalizing against irradiance at a distance of 14 cm from the lamp. Irradiance values at various distances from the lamp were determined by utilizing the irradiance factor and the measured irradiance values of approximately 8 mW cm−2 at a distance of 14 cm from the lamp and approximately 10 mW cm−2 at a distance of 11.5 cm from the lamp. The height of the N95 FFR varies with the model, and a conservative approximation is about 6 cm. Considering this, the closest part of the respirator, when treating either surface, will be approximately 8 cm from the lamp and will observe 1.99 times the irradiance observed at a distance of 14 cm from the lamp (Fig. 1c, Table 1).
Considering the impact of both curvature and distance from the lamp, the dose received by various parts of the N95 during UVC treatment of one surface with 1.5 J cm−2 was found to range from approximately 900–2900 mJ cm−2 (Fig. 3, Table 1). The received dose was calculated using Eq. 2.
| (2) |
Fig. 3.
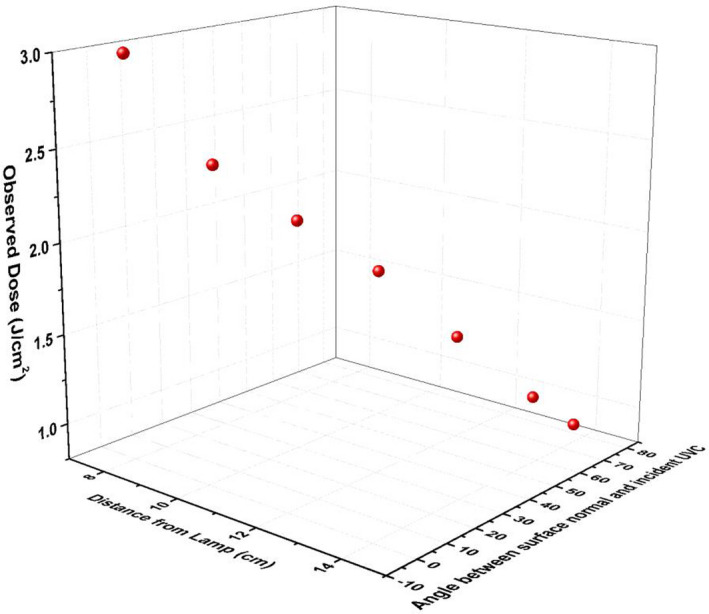
Received dose as a function of angle between surface normal and incident UVC and the distance from the lamp. The top part of the model FFR, approximately 8 cm from the lamp with 0° between surface normal and incident UVC, received approximately 3 J cm−2, whereas the lateral part of the lamp, at a vertical distance of 14 cm from the lamp with approximately 75° between surface normal and incident UVC, received approximately 900 mJ cm−2
Here, for the Daavlin unit, the administered dose when irradiating one surface was 1.5 J cm−2.
UV strip experiments were performed to validate the accuracy and consistency of the above‐mentioned experiments, and to investigate the percentage of UVC penetration through all the layers of the N95 FFR. These strips changed color upon exposure to UVC, and the accumulated dose was measured with the Hoenle UV scan. Figure 2c shows the measurements made with the Hoenle UV scan as a function of those made by the sensor integrated within the Daavlin unit. The variations in the measurements can be explained in part by the variations in the spectral sensitivity curves of the UV tape and the UV meter from the respective manuals. UV tape was applied on the outside‐facing surface of the respirator at the surface closest to the lamp and at the edge which was farther from the lamp and had a curvature (Fig. 2a). The measured values indicated that the edge received 29% of the dose compared to the top, 610 mJ cm−2 at the top and 175 mJ cm−2 at the edge. Figure 2b demonstrates placement of UV strips on the top of the respirator at both the outside‐facing and wearer‐facing surfaces before and after UVC treatment. The outside‐facing surface was irradiated (719 mJ cm−2), and measurements indicated that approximately 10.5% of the administered UVC was detected at the wearer‐facing (75 mJ cm−2) surface.
Discussion
One complete decontamination cycle with the Daavlin unit consisted of treating the outside‐facing surface of the N95 respirator and then flipping the respirator to treat the wearer‐facing surface. This unit can decontaminate approximately 18 N95 respirators at the same time. A UVC dose of 1.5 J cm−2 was administered for each surface; total dose 3 J cm−2. This dose, delivered in approximately 6 min (~3 min per side), corresponded to table/tray surface with areas closer to the lamp receiving a relatively higher dose. The results of the UV meter experiments demonstrated that after irradiating the outside‐facing surface of the N95 respirator with 1.5 J cm−2, all parts of the respirator on this surface received a dose of at least 900 mJ cm−2, while the top part of the FFR, being closest to the light source, received approximately 3 J cm−2. The UV strip experiments further supported this finding with the lateral part of the FFR receiving approximately 29% of the dose received at the top. In addition, UV strip experiments suggest that approximately 10% of the UVC dose could penetrate through all the layers of the N95 respirator. This suggests that after one complete decontamination cycle, the observed dose for all parts of the N95 respirator should be at least ≈1 J cm−2 as recommended by the consensus groups (10) to repurpose N95 respirators.
Of note, presence of UVC lamps on either side will increase the observed dose. In addition, utilization of a highly reflective surface, such as polished aluminum, as a base/tray (and on interior sides and back) with the Daavlin unit will further increase the uniformity as well as overall UVC irradiance within the unit resulting in a higher received dose.
Due to the shortage of PPE across the US, various institutions have repurposed their UVGI technologies for N95 decontamination. Since N95 respirators have curved surfaces and all the UVGI devices have unique geometries, methodology described in this manuscript should be utilized to collect irradiance data for variation due to angle and distance from UVC lamp. This data will help determine the dose received (Eq. 2) by various parts of the N95 decontaminated by utilizing the corresponding UVC unit. In addition, irradiance measurement, as a function of angle, performed near the edge of the unit will provide important instructions regarding placement of N95 respirators during a decontamination cycle to ensure appropriate dosing is received.
A limitation of UVC decontamination systems is that UVC photons may only be effective if they make direct contact with the surface. Considering this and the fact that N95 respirators have a curvature, it is important to account for the actual dose observed by various parts of the respirator within the repurposed unit. Relatively low decontamination level of the strap is another limitation of UVC‐mediated decontamination of N95 respirators. To address this, the N95Decon group has suggested wiping the straps with a compatible wipe along with UVC treatment to attain desired decontamination levels (14).
Important factors to be considered when determining and comparing efficacy of potential UVGI devices, specifically for N95 decontamination, include maximum irradiance of the UVC unit, if the irradiance was measured or calculated, availability of fit‐testing data after UVC treatment, number of decontamination cycles after which the FFR would pass fit testing, the maximum number of respirators that can be treated during 1 cycle, cost, and whether or not the device requires a ventilated room. To facilitate these considerations, these parameters are included in Table 2 with suggested scoring which can be used to gather device‐specific information by institutions to compare UVGI devices. This scoring system was developed to serve as a screening tool when our hospital system was approached by multiple vendors with the repurposed UVC technologies for N95 decontamination. Although not validated, it proved to be practical and useful. Other institutions may benefit from this as well.
Table 2.
Parameters that can be used to compare various UVGI devices
| 1. Maximum irradiance: The higher the maximum irradiance, the quicker the dose will be delivered making the unit time efficient. | ||
|---|---|---|
| Time efficiency/Maximum irradiance | Example: Time to deliver 1.5 J cm−2 at given irradiances | Score |
| >10 mW cm−2 | <2 min 30 s | 5 |
| 5–10 mW cm−2 | 2 min 30 s–5 min | 4 |
| 1–5 mW cm−2 | 5 min–25 min | 3 |
| 0.5–1 mW cm−2 | 25 min–50 min | 2 |
| <0.5 mW cm−2 | >50 min | 1 |
| 2. Irradiance data | |
|---|---|
| Irradiation data | Score |
| Measured | 5 |
| Calculated | 1 |
| 3. Fit‐testing post‐UVC treatment | |
|---|---|
| Fit‐testing data | Score |
| Available for certain N95 models | 5 |
| No data available | 0 |
| 4. Maximum number of respirators treated in one cycle | |
|---|---|
| Number of respirators per cycle | Score |
| >45 | 5 |
| 30–45 | 4 |
| 15–30 | 3 |
| 5–15 | 2 |
| <5 | 1 |
| 5. Cost per respirator: This comparison can be done by dividing the cost of the unit by number of respirators that can be sterilized in one cycle. Since the units will be used multiple times, the actual cost per respirator will be lower. Only one cycle can be considered for a simple comparison | |
|---|---|
| Cost per respirator | Score |
| <$100.00 | 5 |
| $100.00–$200.00 | 4 |
| $200.00–300.00 | 3 |
| $300.00–$400.00 | 2 |
| > $400 per respirator | 1 |
| 6. Ventilation: Some units emit ozone and might need ventilation | |
|---|---|
| Ventilation | Score |
| Not needed | 2 |
| Needed | 1 |
Maximum possible score: 5 + 5 + 5 + 5+5 + 2 = 27.
In conclusion, this study presents a model for careful and methodical assessment of the efficacy of UVC in decontamination of N95 respirators. While a specific UVC device and one type of N95 respirator were used, the assessment process can be generalized to other UVGI devices and other types of respirators. It is imperative that this type of assessment be performed to make sure that the decontamination process is properly done. Failure to do so could result in catastrophic consequences for the front‐line healthcare workers.
Acknowledgements
The authors would like to acknowledge Akbar Hussaini, Singa Tobing, Steve Gail from BASF and Devais Parejo from Hoenle UV Scan for their technical assistance and support.
References
- 1. Mills, D. , Harnish D. A., Lawrence C., Sandoval‐Powers M. and Heimbuch B. K. (2018) Ultraviolet germicidal irradiation of influenza‐contaminated N95 filtering facepiece respirators. Am. J. Infect. Control 46(7), e49–e55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Fisher, E. M. and Shaffer R. E. (2011) A method to determine the available UV‐C dose for the decontamination of filtering facepiece respirators. J. Appl. Microbiol. 110(1), 287–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mills, D. S. , Lawrence C., Heimbuch B. and Harnish D. A. (2016) Ultraviolet germicidal irradiation of influenza‐contaminated N95 filtering facepiece respirators. [DOI] [PMC free article] [PubMed]
- 4. Hamzavi, I. H. , Lyons A. B., Kohli I., Narla S., Parks‐Miller A., Gelfand J. M., Lim H. W.and Ozog D. M. (2020) Ultraviolet germicidal irradiation: Possible method for respirator disinfection to facilitate reuse during the COVID‐19 pandemic. J. Am. Acad. Dermatol. 82(6), 1511–1522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Casini, B. , Tuvo B., Cristina M. L., Spagnolo A. M., Totaro M., Baggiani A. and Privitera G. B.(2019) Evaluation of an Ultraviolet C (UVC) light‐emitting device for disinfection of high touch surfaces in hospital critical areas. Int. J. Environ. Res. Public Health 16(19), 3572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Guridi, A. , Sevillano E., de la Fuente I., Mateo E., Eraso E. and Quindos G. (2019) Disinfectant activity of a portable ultraviolet C equipment. Int. J. Environ. Res. Public Health 16(23), 4747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Yang, J. H. , Wu U. I., Tai H. M. and Sheng W. H. (2019) Effectiveness of an ultraviolet‐C disinfection system for reduction of healthcare‐associated pathogens. J. Microbiol. Immunol. Infect. 52(3), 487–493. [DOI] [PubMed] [Google Scholar]
- 8. Narla, S. , Lyons A. B., Kohli I., Torres A. E., Parks‐Miller A., Ozog D. M., Hamzavi I. H.and Lim H. W. (2020) The importance of the minimum dosage necessary for UVC decontamination of N95 respirators during the COVID‐19 pandemic. Photodermatol Photoimmunol Photomed. 36(4):324–325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Heimbuch, B. K. and Harnish D..Research to Mitigate a Shortage of Respiratory Protection Devices during Public Health Emergencies. Available from: https://www.ara.com/news/ara‐research‐mitigate‐shortage‐respiratory‐protection‐devices‐during‐public‐health‐emergencies.
- 10. N95DECON . Technical Report for UV‐C‐Based N95 Resude Risk Management; 2020. Available from: https://static1.squarespace.com/static/5e8126f89327941b9453eeef/t/5e8541760211467623b1e4e4/1585791351199/200401_N95DECON_UV_technicalreport_v1.2_final.pdf
- 11. Prevention CfDCa . Decontamination and Reuse of Filtering Facepiece Respirators, 2020. Available from: https://www.cdc.gov/coronavirus/2019‐ncov/hcp/ppe‐strategy/decontamination‐reuse‐respirators.html
- 12. Ryder, A. (1997) The Light Measurement Handbook. International Light Technical Publications, Newbury, MA. [Google Scholar]
- 13. Grimes, D. R. , Robbins C. and O'Hare N. J. (2010) Dose modeling in ultraviolet phototherapy. Med Phys. 37(10), 5251–5257. [DOI] [PubMed] [Google Scholar]
- 14. N95DECON/MGB N95 Decontamination & Reuse Webinar: Evidence and Implementation. Available from: https://www.n95decon.org/resources [May 9th, 2020]