

Abstract
An increase in coronavirus disease (COVID‐19) infections prompted Level 4 lockdown throughout New Zealand from 25 March 2020. We have investigated trends in coronary and electrophysiology (EP) procedures before and during this lockdown. The number of acute procedures for ST elevation myocardial infarction remained stable. In contrast, the number of in‐patient angiograms and percutaneous intervention procedures fell by 53% compared with the previous 4 weeks in 2020 and by 56% compared with the corresponding period in 2019. Further study is required to determine the reasons for these trends.
Keywords: COVID‐19 pandemic, percutaneous coronary intervention, STEMI, cardiac electrophysiology, coronary angiography
Severe respiratory infection and death because of coronavirus disease (COVID‐19) was first reported among patients and health workers in Wuhan, China, in January 2020. Our Ministry of Health set up the National Health Coordination Centre in late January in response to concerns that this virus was spreading around the world. COVID‐19 became a notifiable disease on 30 January, and restrictions were imposed on foreign travellers from China into New Zealand on 3 February.
The first case of COVID‐19 in New Zealand was reported on 28 February in a person who was unwell on returning from a trip to Iran. Subsequent cases were all travellers who had returned to New Zealand from Singapore, United States and Australia and from cruise ships. Our borders were closed to non‐residents on 19 March. A total of 23 cases had been reported by the time the Level 2 lockdown was imposed on 21 March, and 205 cases by the time we entered Level 4 lockdown just 4 days later on the night of 25 March. Level 4 lockdown was eased to Level 3 on 27 April.
We report the number of procedures performed in our two cardiac catheterisation laboratories at Christchurch Public Hospital during the nine fortnights from 30 December 2019 to 3 May 2020 inclusive, and then compare these numbers with the equivalent fortnights from 31 December 2018 to 5 May 2019. Our hospital is the only hospital admitting patients with acute coronary syndromes and only acute percutaneous intervention (PCI) centre for a population in excess of 400 000. Data were collated from a prospective database compiled by our radiographer team at the end of each procedure. This analysis does not include publicly funded elective coronary angiography procedures performed at another hospital.
The number of acute coronary angiogram/PCI (for ST elevation myocardial infarction (STEMI)), all angiograms, all PCI, all other interventional cardiology procedures and permanent pacemaker insertions, and all electrophysiological procedures was stable through to 23 March 2020.
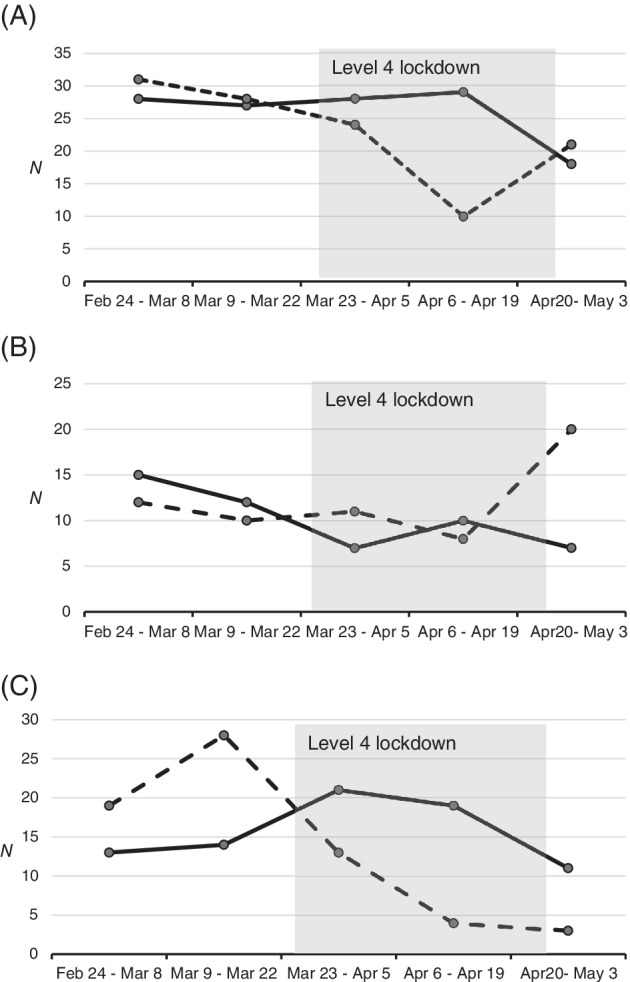
The number of acute PCI procedures for STEMI remained stable during Level 4 lockdown (Fig. 1A). However, the total number of catheter lab procedures fell by 60% to a nadir of 45 total procedures in the fortnight 6 April 6 to 19 April inclusive compared with 103 during the corresponding fortnight in 2019. This was largely due to falls in other coronary angiogram or PCI procedures (from 63 to 21) and EP procedures from 29 to 9 cases.
Figure 1.

Trends in acute, in‐patient and elective coronary procedures. (A) Acute angio/PCI (STEMI). (B) In‐patient angio/PCI. (C) Elective angio/PCI. ( ) 2019, (
) 2019, ( ) 2020. Angio, coronary angiogram; PCI, percutaneous intervention; STEMI, ST elevation myocardial infarction.
) 2020. Angio, coronary angiogram; PCI, percutaneous intervention; STEMI, ST elevation myocardial infarction.
Procedures performed for in‐patients from 23 March to 3 May are compared with elective procedures in Figures 1 and 2. In the 4 weeks from 23 March, the number of angiograms and PCI procedures on in‐patients fell by 53% to 41procedures compared with 87 procedures in the previous 4 weeks in 2020, and by 56% compared with 94 in the corresponding period in 2019 (Fig. 1B). This fall in in‐patient PCI procedures was the main reason for the fall in total angiogram and PCI procedures. There was also a fall in elective procedures (Fig. 1C). Indeed, no outpatient coronary angiograms or PCI procedures were performed in the 4 weeks beginning 23 March compared with 34 procedures in the previous 4 weeks and 31 procedures in the corresponding 4 weeks in 2019. Dates of final elective angiogram and PCI procedures were 19 March and 20 March, respectively, preceding the move to Level 2 and then to Level 3 lockdown. In‐patient procedures have returned to normal early in Stage 3 lockdown (Fig. 1B).
Figure 2.
Trends in all, in‐patient, and elective electrophysiology procedures. (A) All EP procedures. (B) In‐hospital EP procedures. (C) Elective EP procedures. ( ) 2019, (
) 2019, ( ) 2020. EP, electrophysiology procedures including EP studies, ablation procedures, implantation of pacemakers, defibrillators, CRT devices and reveal devices, and box changes.
) 2020. EP, electrophysiology procedures including EP studies, ablation procedures, implantation of pacemakers, defibrillators, CRT devices and reveal devices, and box changes.
Contrasting data were presented for EP procedures in Figure 2. The fall in total EP procedures was largely due to reduced elective volumes. The number of in‐patient EP procedures has remained relatively constant throughout Level 4 lockdown with 19 procedures during the 4 weeks from 23 March compared with 22 procedures in the previous 4 weeks of 2020, and 17 procedures during the corresponding 4 weeks in 2019 (Fig. 2B). Outpatient EP studies were continued throughout the lockdown period but at reduced volumes with 16, 4 and 3 procedures, respectively, in the fortnights commencing 23 March, 6 April and 20 April compared with 21, 19 and 11 procedures in the corresponding fortnights in 2019 (Fig. 2C).
Discussion
We did not detect a fall in acute PCI procedures to treat STEMI during the Level 4 lockdown for COVID‐19. This finding is in contrast to recent reports from Spain, 1 United States, 2 Austria 3 and Italy. 4 Those reports were from ‘hub’ hospitals in countries experiencing a major pandemic of COVID‐19 cases and disruption of their medical systems of care including transportation to PCI‐capable hospitals. The very large majority of our acute STEMI patients present directly to our hospital and are not referred to from other hospitals. Furthermore, our hospital treated very few COVID‐19 cases during Level 4 lockdown, community prevalence was low, and ambulance and hospital services were not overwhelmed.
However, we have demonstrated that in‐patient angiogram and PCI procedures fell by more than 50%. As we had no major disruptions in resourcing or medical care, this decrease in coronary procedures could be due to a true decrease in incidence of other acute coronary syndromes (non‐STEMI and unstable angina) in our city during lockdown. Further investigation is required to confirm the possibility of a true decrease in incidence of acute coronary syndromes, and needs to include analysis of general practice consultations, analysis of trends in requests for troponin levels, emergency department case numbers, hospital discharge data and trends in mortality in the community.
Two of the recent European studies documented greater falls in presentations with non‐STEMI than with STEMI.3, 4 The Italian study reported a 41–44% fall in non‐STEMI admissions compared with a 23–25% fall in STEMI admissions. 4 We have not assessed admission or discharge diagnosis data from our hospital. A study of nationwide trends in acute coronary syndromes and catheter lab procedures using the ANZACS‐QI database is ongoing.
Alternatively, the fall in in‐patient coronary procedures could be a consequence of changes in thresholds for presentation or access to care at patient, community and hospital levels.
Did patients suffer symptoms at home and not seek assessment because of a vigorous nationwide advertising campaign that emphasised messages such as ‘do not burst your bubble’, ‘stay at home if you are over 70 years of age’ and other messages to encourage social distancing? Did New Zealanders prefer to suffer a heart attack in silence rather than create further risks to their health and the health of others by leaving their home and ‘bubble’, and presenting to a clinic or hospital?
Or was it more difficult to reach out for help? At the beginning of lockdown, all General Practice groups distributed advice that face‐to‐face consultations were cancelled but phone consultations were available. Many patients may have interpreted this as a barrier to access. If either of these factors was important, there could be a number of people with recent acute coronary syndromes who are untreated and at increased risk or recurrent events or sudden death in the near future.
Having reached the hospital, was there a change in the triaging of chest pain patients in ED or a reduction in referrals to the cardiology in‐patient service? Or was there a change in decision making and thresholds for referral to the catheter lab during cardiology ward rounds so patients might return home to their bubble as quickly as possible? The decrease in referrals to the catheter lab was not due to reduced resources. The catheter labs were manned by teams working 1 week on, 1 week off rosters. No member of staff contracted COVID‐19 and no staff were in self‐isolation.
In summary, we report a >50% decrease in in‐patient coronary procedures during the Level 4 lockdown. This occurred in the absence of resource limitations, disruption to medical care or widespread community infection. We hope this was due to a true decrease in the incidence of acute coronary syndromes rather than changes in investigation and management during lockdown. Indeed, there may be a rebound increase in presentations or demand for treatment as we exit lockdown.
Acknowledgements
We are grateful to our colleagues in the Department of Cardiology, Christchurch Hospital, Christchurch for their diligence in completion of the Cath Lab Log Book.
Funding: None.
Conflict of interest: None.
References
- 1. Rodriguez‐Leor O, Cid‐Alvarez B. ST‐segment elevation myocardial infarction care during COVID‐19: losing sight of the forest for the trees. JACC Case Rep 2020. 10.1016/j.jaccas.2020.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Garcia S, Albaghdadi MS, Meraj PM, Schmidt C, Garberich R, Jaffer FA et al Reduction in ST‐segment elevation cardiac catheterization laboratory activations in the United States during COVID‐19 pandemic. J Am Coll Cardiol 2020; 75: 2871–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Metzler B, Siostrzonek P, Binder RK, Bauer A, Reinstadler SJ. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID‐19: the pandemic response causes cardiac collateral damage. Eur Heart J 2020; 41: 1852–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. De Filippo O, D'Ascenzo F, Angelini F, Bocchino PP, Conrotto F, Saglietto A et al Reduced rate of hospital admissions for ACS during Covid‐19 outbreak in northern Italy. N Engl J Med 2020; 383: 88–9. [DOI] [PMC free article] [PubMed] [Google Scholar]