

Abstract
Background
The optimal MAP target for patients with cardiogenic shock (CS) remains unknown. We sought to determine the relationship between mean arterial pressure (MAP) and mortality in the cardiac intensive care unit (CICU) patients with CS.
Methods
Using a single-center database of CICU patients admitted between 2007 and 2015, we identified patients with an admission diagnosis of CS. MAP was measured every 15 min, and the mean of all MAP values during the first 24 h (mMAP24) was recorded. Multivariable logistic regression determined the relationship between mMAP24 and adjusted hospital mortality.
Results
We included 1002 patients with a mean age of 68 ± 13.7 years, including 36% females. Admission diagnoses included acute coronary syndrome in 60%, heart failure in 74%, and cardiac arrest in 38%. Vasoactive drugs were used in 72%. The mMAP24 was higher (75 vs. 71 mmHg, p < 0.001) among hospital survivors (66%) compared with non-survivors (34%). Hospital mortality was inversely associated with mMAP24 (adjusted OR 0.9 per 5 mmHg higher mMAP24, p = 0.01), with a stepwise increase in hospital mortality at lower mMAP24. Patients with mMAP24 < 65 mmHg were at higher risk of hospital mortality (57% vs. 28%, adjusted OR 2.0, 95% CI 1.4–3.0, p < 0.001); no differences were observed between patients with mMAP24 65–74 vs. ≥ 75 mmHg (p > 0.1).
Conclusion
In patients with CS, we observed an inverse relationship between mMAP24 and hospital mortality. The poor outcomes in patients with mMAP24 < 65 mmHg provide indirect evidence supporting a MAP goal of 65 mmHg for patients with CS.
Keywords: Cardiogenic shock, Shock, Cardiac intensive care unit, Critical care, Mortality, Hypotension, Blood pressure
Background
Cardiogenic shock (CS) is the second-most common form of circulatory shock in all critical care units and the most common form of shock among patients admitted to cardiac intensive care units (CICUs) [1, 2]. CS manifests in clinical, hemodynamic, and biochemical derangements characterized by arterial hypotension and tissue hypoperfusion, resulting in significant morbidity and mortality despite appropriate treatment [3]. The mainstay of management is early intervention to address the inciting cause, in conjunction with supportive care, to restore end-organ perfusion and prevent multi-organ failure and death [3]. In cases of acute myocardial infarction, emergency revascularization is indicated in order to improve cardiac function [4].
Immediate restoration of adequate systemic blood pressure using intravenous inotropes, vasopressors, and/or mechanical circulatory support is a priority in CS [3]. The optimal blood pressure target in CS must balance the maintenance of adequate end-organ perfusion with the adverse effects of excessive cardiac afterload and arrhythmias induced by catecholamine vasopressors. The ideal target mean arterial pressure (MAP) for patients with CS is unclear, and current strategies are based on evidence from patients with vasodilatory shock and cardiac arrest (CA) [3, 5, 6]. Furthermore, it has been suggested that patients with pre-existing hypertension may benefit from higher MAP goals [7], and a history of hypertension is common among patients with cardiovascular disease [8]. By contrast, recent evidence has demonstrated favorable outcomes among older patients supported with permissive hypotension (MAP 60–65 mmHg) [9].
Given the sparsity of evidence to support specific MAP targets in patients with CS, we sought to describe the relationship between MAP and hospital mortality among patients with CS. We hypothesized that hospital mortality among patients with CS would increase as a function of lower MAP and that a threshold MAP may identify an optimal MAP range. Our secondary aim was to evaluate the prevalence of organ failure as a function of MAP.
Methods
Study population
This study was approved by the Institutional Review Board of Mayo Clinic (IRB # 16-000722) as posing minimal risk to patients and was performed under a waiver of informed consent. We retrospectively analyzed a database containing data from the initial CICU admission for consecutive unique adult patients aged ≥ 18 years admitted to the CICU at Mayo Clinic Hospital St. Mary’s Campus between January 1, 2007, and December 31, 2015 [10–12]. The Mayo Clinic CICU is a closed unit serving critically ill cardiac medical patients, but not postoperative cardiac surgery patients and patients receiving extracorporeal membrane oxygenation (ECMO) support. We included only those patients with an admission diagnosis of CS, defined as an International Classification of Diseases (ICD)-9 code of 785.51 documented within 1 day of CICU admission. We excluded all patients without an admission diagnosis of CS (including those without available admission diagnosis data), even if they had an ICD-9 code for CS documented at another time during hospitalization. Patients without available data on MAP were also excluded. Patients who declined Minnesota Research Authorization, according to Minnesota state law statute 144.295, were excluded from the study.
Data sources
We recorded demographic, vital sign, laboratory, clinical, and outcome data, as well as procedures and therapies performed during the CICU and hospital stay, as previously described [10–12]. All relevant data were extracted electronically from the medical record using the Mayo Clinic Multidisciplinary Epidemiology and Translational Research in Intensive Care Data Mart [13]. The admission value of all vital signs, clinical measurements, and laboratory values was defined as either the first value recorded after CICU admission or the value recorded closest to CICU admission. In addition, vital signs were recorded every 15 min, and the maximum, minimum, and mean values over the first 1, 6, and 24 h were recorded. Blood pressure was preferentially recorded from invasive measurements, when available, and otherwise was recorded from noninvasive measurements. Peak vasopressor and inotrope doses were used to calculate the Vasoactive-Inotropic Score [14]. Admission diagnoses included all ICD-9 diagnostic codes recorded on the day of CICU admission and the day before or after CICU admission; these admission diagnoses were not mutually exclusive, and the primary admission diagnosis could not be determined. Admission diagnoses of interest included CS, acute coronary syndrome (ACS), heart failure (HF), supraventricular tachycardia, atrial fibrillation, ventricular fibrillation, ventricular tachycardia, CA, respiratory failure, and sepsis. Discharge ICD-9 diagnostic codes were reviewed for a diagnosis of hypertension. Severe acute kidney injury (AKI) was defined as KDIGO stage 2 or 3 AKI during the CICU stay (i.e., doubling of serum creatinine or increase in serum creatinine to ≥ 4.0 mg/dl or new dialysis initiation in the CICU); mild AKI was defined as KDIGO stage 1 AKI (an increase in creatinine by ≥ 0.3 mg/dl or 50% from baseline) [11, 15]. Baseline creatinine was considered to be the latest creatinine within 1 year prior to the index hospital admission, and patients who had previously received dialysis were excluded from this AKI analysis. Non-cardiovascular organ failure was defined as a score ≥ 3 on any day 1 SOFA organ subscore [16].
Statistical analysis
The primary endpoint was all-cause hospital mortality; secondary endpoints included CICU mortality and post-discharge mortality up to 1 year among hospital survivors. Mortality and other outcome data were extracted from Mayo Clinic electronic databases, the state of Minnesota electronic death certificates, and the Rochester Epidemiology Project database [17]. Categorical variables are reported as number (percentage), and the Pearson chi-squared test was used to compare groups. Continuous variables are reported as mean (± standard deviation); the Wilcoxon rank-sum test was used to compare groups. The calculation of 24-h mean MAP (mMAP24) was performed using invasive blood pressure measurements, if available; otherwise, mMAP24 was calculated using noninvasive blood pressure values. Logistic regression was used to determine the association between mMAP24 with hospital mortality before and after adjusting for age, gender, race, Charlson Comorbidity Index (CCI), and Acute Physiology and Chronic Health Evaluation IV (APACHE-IV) predicted mortality; admission diagnoses of CA, sepsis, HF, and ACS; peak 24-h VIS; and the use of intra-aortic balloon pump (IABP), dialysis, pulmonary artery catheter (PAC), coronary angiography, percutaneous coronary intervention (PCI), and mechanical ventilation. Subgroup analysis was performed by repeating multivariable logistic regression after excluding patients with SCAI shock stages A or B or sepsis; besides, logistic regression was repeated in the overall cohort after adjusting for SCAI shock stages. Discrimination was assessed using the area under the receiver-operator characteristic curve (AUC, c-statistic) value, and the optimal cutoff defined using Youden’s J index. Post-discharge survival among hospital survivors was evaluated using the Kaplan-Meier survival analysis and Cox proportional-hazards analysis. Two-tailed p values < 0.05 were considered statistically significant. Statistical analyses were performed using JMP Pro version 14.1.0 (SAS Institute, Cary, NC).
Results
Study population
The database included 10,004 unique CICU patient admissions, of whom 1078 had an admission diagnosis CS and were potentially eligible for inclusion [10]. We excluded 76 of these patients due to lack of available data for MAP (Supplemental Figure 1). The final study population of 1002 unique patients had a mean age of 67.7 ± 13.7 years, including 36.4% females (Table 1). The mean CCI was 2.4 ± 2.5, and the mean APACHE-IV predicted hospital mortality was 38.4% ± 29.3 overall. Concomitant admission diagnoses included ACS in 599 (59.8%) patients, HF in 740 (73.9%), sepsis in 199 (19.9%), and CA in 379 (37.8%); 77 (7.7%) patients had neither ACS nor HF as an admission diagnosis. Non-cardiovascular organ failure developed on the first day in 690 (68.9%) patients; 630 (73.2%) patients developed AKI during the CICU stay, including 314 (36.5%) with severe AKI.
Table 1.
Baseline characteristics of the study population. Data represented as mean ± standard deviation for continuous variables and n (%) for categorical variables
| Overall (n = 1002) | MAP < 65 mmHg (n = 186) | MAP 65–75 mmHg (n = 426) | MAP ≥ 75 mmHg (n = 390) | p value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age | 67.7 ± 13.8 | ||||
| Female gender | 365 (36.4%) | 75 (40.3%) | 156 (36.6%) | 134 (34.4%) | 0.38 |
| White race | 921 (91.9%) | 173 (93.0%) | 385 (90.4%) | 363 (93.1%) | 0.31 |
| Body mass index | 29.3 ± 6.8 | 29.9 ± 8.1 | 29.1 ± 6.4 | 29.5 ± 6.6 | 0.59 |
| Severity of illness | |||||
| APACHE-III score | 86.2 ± 33.0 | 100.8 ± 35.3 | 87.5 ± 32.0 | 77.9 ± 30.2 | < 0.0001 |
| APACHE-IV predicted mortality | 0.38 ± 0.29 | 0.48 ± 0.29 | 0.40 ± 0.29 | 0.32 ± 0.28 | < 0.0001 |
| SOFA score | 7.6 ± 4.2 | 9.5 ± 4.4 | 7.9 ± 4.1 | 6.4 ± 3.8 | < 0.0001 |
| Maximum week 1 SOFA score | 8.4 ± 4.2 | 10.0 ± 4.4 | 8.7 ± 4.1 | 7.3 ± 3.9 | < 0.0001 |
| Cardiovascular SOFA score | 2.5 ± 1.3 | 3.0 ± 1.2 | 2.6 ± 1.2 | 2.1 ± 1.3 | < 0.0001 |
| Comorbidities | |||||
| Charlson Comorbidity Index | 2.4 ± 2.5 | 2.84 ± 2.7 | 2.4 ± 2.5 | 2.1 ± 2.4 | 0.01 |
| Prior myocardial infarction | 200 (20.0%) | 35 (18.8%) | 95 (22.4%) | 70 (18.1%) | 0.29 |
| Prior heart failure | 193 (19.4%) | 48 (25.8%) | 90 (21.2%) | 55 (14.3%) | 0.002 |
| Prior hypertension | 348 (34.7%) | 64 (34.4%) | 145 (34.0%) | 139 (35.6%) | 0.89 |
| Prior diabetes mellitus | 287 (28.8%) | 60 (32.3%) | 119 (28.0%) | 108 (28.0%) | 0.51 |
| Prior CKD | 202 (20.2%) | 49 (26.3%) | 82 (19.3%) | 71 (18.4%) | 0.07 |
| Prior dialysis | 88 (8.8%) | 32 (17.2%) | 34 (8.0%) | 22 (5.6%) | 0.0001 |
| Prior stroke | 121 (12.1%) | 23 (12.4%) | 58 (13.7%) | 40 (10.4%) | 0.36 |
| Prior cancer | 214 (21.5%) | 54 (29.0%) | 97 (22.8%) | 63 (16.3%) | 0.002 |
| Admission diagnoses | |||||
| Cardiac arrest | 379 (37.8%) | 63 (33.9%) | 149 (35.0%) | 167 (42.8%) | 0.03 |
| Sepsis | 199 (19.9%) | 46 (24.7%) | 96 (22.5%) | 57 (14.6%) | 0.003 |
| Respiratory failure | 645 (64.4%) | 115 (61.8%) | 288 (67.6%) | 242 (62.1%) | 0.18 |
| Acute coronary syndrome | 599 (59.8%) | 98 (52.7%) | 260 (61.0%) | 241 (61.8%) | 0.09 |
| Heart failure | 740 (73.9%) | 139 (74.7%) | 326 (76.5%) | 275 (70.5%) | 0.14 |
| SCAI cardiogenic shock stage | |||||
| Stage A | 151 (15.1%) | 7 (3.8%) | 63 (14.8%) | 81 (20.8%) | < 0.0001 |
| Stage B | 336 (33.5%) | 50 (26.9% | 146 (34.3%) | 140 (35.9%) | < 0.0001 |
| Stage C | 116 (11.6%) | 19 (10.2%) | 41 (9.6%) | 56 (14.4%) | < 0.0001 |
| Stage D | 329 (32.8%) | 84 (45.2%) | 150 (35.2%) | 95 (24.4%) | < 0.0001 |
| Stage E | 70 (7.0%) | 26 (14.0%) | 26 (6.1%) | 18 (4.6%) | < 0.0001 |
| CICU admission clinical parameters | |||||
| Heart rate (HR, beats per minute) | 90.7 ± 24.1 | 93.8 ± 26.8 | 91.3 ± 23.7 | 88.6 ± 22.9 | 0.09 |
| Systolic blood pressure (SBP, mmHg) | 110.8 ± 27.8 | 97.0 ± 24.0 | 105.9 ± 23.6 | 120.0 ± 30.6 | < 0.0001 |
| Diastolic blood pressure (mmHg) | 65.3 ± 18.8 | 56.9 ± 15.9 | 63.9 ± 17.0 | 71.8 ± 19.7 | < 0.0001 |
| Mean arterial pressure (first 24 h, mmHg) | 73.4 ± 10.1 | 68.5 ± 18.0 | 76.9 ± 17.3 | 87.4 ± 20.9 | < 0.0001 |
| Shock index (HR/SBP) | 0.86 ± 0.30 | 1.0 ± 0.31 | 0.87 ± 0.3 | 0.79 ± 0.9 | < 0.0001 |
| Oxygen saturation (%) | 92.9 ± 10.9 | 91.3 ± 12.1 | 92.6 ± 11.6 | 93.9 ± 9.2 | 0.006 |
| Admission laboratory values | |||||
| Sodium | 137.0 ± 5.1 | 137.1 ± 5.9 | 136.7 ± 5.0 | 137.3 ± 4.8 | 0.11 |
| Potassium | 4.3 ± 0.9 | 4.4 ± 0.9 | 4.4 ± 0.87 | 4.3 ± 0.8 | 0.08 |
| Bicarbonate | 21.2 ± 5.2 | 20.9 ± 6.0 | 21.0 ± 5.1 | 21.5 ± 4.8 | 0.18 |
| Anion gap | 14.1 ± 4.8 | 16.4 ± 6.0 | 13.7 ± 4.8 | 13.8 ± 4.0 | < 0.0001 |
| Creatinine | 1.6 ± 1.1 | 2.2 ± 1.6 | 1.5 ± 1.0 | 1.3 ± 0.8 | < 0.0001 |
| Hemoglobin | 12.1 ± 2.4 | 11.1 ± 2.1 | 12.0 ± 2.3 | 12.7 ± 2.4 | < 0.0001 |
| Lactate | 3.9 ± 3.7 | 5.1 ± 4.6 | 3.6 ± 3.4 | 3.7 ± 3.4 | 0.009 |
| Troponin (initial) | 2.3 ± 4.5 | 2.7 ± 6.6 | 2.2 ± 4.2 | 2.1 ± 3.8 | 0.48 |
| Troponin (peak during hospital stay) | 3.9 ± 6.7 | 4.5 ± 8.9 | 3.9 ± 6.8 | 3.7 ± 5.4 | 0.57 |
| Procedures and therapies | |||||
| Number of vasoactive drugs | 1.5 ± 1.3 | 2.0 ± 1.4 | 1.6 ± 1.2 | 1.1 ± 1.3 | < 0.0001 |
| Vasopressors | 722 (72.1%) | 161 (86.6%) | 332 (77.9%) | 229 (58.7%) | < 0.0001 |
| Inotropes | 282 (28.1%) | 68 (36.6%) | 123 (28.9%) | 91 (23.3%) | < 0.0001 |
| Peak vasoactive infusion score (VIS) | 26.1 ± 54.3 | 47.6 ± 79.0 | 23.8 ± 46.3 | 18.5 ± 44.7 | < 0.0001 |
| Invasive ventilation | 599 (59.8%) | 105 (56.5%) | 269 (63.2%) | 225 (57.7%) | 0.17 |
| Noninvasive ventilation | 241 (24.1%) | 42 (22.6%) | 118 (27.7%) | 81 (20.8%) | 0.06 |
| Dialysis | 101 (10.1%) | 27 (14.5%) | 43 (10.1%) | 31 (8.0%) | 0.05 |
| Intra-aortic balloon pump | 389 (38.8%) | 41 (22.0%) | 193 (45.3%) | 155 (39.7%) | < 0.0001 |
| Pulmonary artery catheter | 240 (24.0%) | 40 (21.5%) | 112 (26.3%) | 88 (22.6%) | 0.32 |
| Coronary angiogram | 647 (64.6%) | 97 (52.2%) | 275 (64.6) | 275 (70.5%) | < 0.0001 |
| Percutaneous coronary intervention | 325 (32.4%) | 48 (25.8%) | 142 (33.3%) | 135 (34.6%) | 0.09 |
| Impella® | 8 (0.8%) | 2 (1.1%) | 5 (1.2%) | 1 (0.3%) | 0.25 |
| ECMO | 2 (0.2%) | 0 (0%) | 0 (0%) | 2 (0.5%) | 0.21 |
| Outcomes | |||||
| Severe acute kidney injury during CICU stay | 314 (36.5%) | 63 (46.0%) | 139 (36.7%) | 112 (32.5%) | 0.02 |
| Severe acute kidney injury during hospital | 392 (43.6%) | 71 (49.3%) | 172 (44.1%) | 149 (40.9%) | 0.22 |
| CICU length of stay | 4.3 ± 7.3 | 4.5 ± 14.1 | 4.6 ± 4.8 | 3.8 ± 3.8 | < 0.0001 |
| Hospital length of stay | 13.1 ± 18.1 | 14.4 ± 25.4 | 13.7 ± 18.5 | 11.7 ± 12.5 | 0.02 |
| CICU mortality | 234 (23.3%) | 80 (43.0%) | 81 (19.0%) | 73 (18.7%) | < 0.0001 |
| Hospital mortality | 338 (33.7%) | 106 (57.0%) | 127 (29.8%) | 105 (26.9%) | < 0.0001 |
APACHE Acute Physiology And Chronic Health Evaluation, BUN blood urea nitrogen, CICU cardiac intensive care unit, CKD chronic kidney disease, ECMO extracorporeal membrane oxygenation, IABP intra-aortic balloon pump, RBC red blood cell, SCAI Society for Cardiovascular Angiography and Interventions, SOFA Sequential Organ Failure Assessment, WBC white blood cell
The mMAP24 for the population was 73.4 ± 10.1 mmHg. A total of 186 (18.6%) patients had a mMAP24 < 65 mmHg, and 390 (38.9%) patients had a mMAP24 ≥ 75 mmHg. During the first 24 h of the CICU stay, 719 (71.8%) patients received vasoactive drugs, including vasopressors in 668 (66.7%), and inotropes in 282 (28.1%), with a mean peak 24-h VIS of 26.1 ± 54.3. IABP was used during the CICU admission in 389 (38.8%) of patients.
Patients with a mMAP24 < 65 mmHg differed from patients with a mMAP24 65–75 mmHg or mMAP24 ≥ 75 mmHg (Table 1), with greater severity of illness (APACHE-III score 100.8 ± 35.3 vs. 87.5 ± 32.0 vs. 77.9 ± 30.2, p < 0.001), more severe CS based on Society for Cardiovascular Angiography and Interventions (SCAI) staging, increased incidence of severe AKI (30.0% vs. 19.8% vs. 14.8%, p = 0.001, Fig. 1a), greater use of vasoactive infusions (85.5% vs. 78.9% vs. 54.4%, p < 0.001), and an increased number of non-cardiac organ injury (mean 1.4 vs. 1.1 vs. 0.9, < 0.001, Fig. 1b). Conversely, patients with mMAP24 < 65 mmHg underwent fewer coronary angiograms (52.5% vs. 64.6% vs. 70.5%, p < 0.001) and were less often supported with an IABP or Impella device (Abiomed, Danvers, MA, USA) (30.1% vs. 50.5% vs. 46.4%, respectively, p < 0.001).
Fig. 1.

a, b Incidence of acute kidney injury by stage (a) and non-cardiac organ failure (by number of organs affected, b) as a function of the 24-h average mean arterial pressure (mMAP24)
Hospital mortality
Hospital mortality was 33.7%, including 23.4% of patients who died in the CICU. Patients who died in the hospital had lower mMAP24 (70.8 vs. 74.7 mmHg, p < 0.001). Crude hospital mortality was higher in patients with mMAP24 < 65 mmHg compared with patients with mMAP24 65–75 mmHg or mMAP24 ≥ 75 mmHg (57.0% vs. 29.8% vs. 26.9%, p < 0.001 for mMAP24 < 65 mmHg vs. other groups and p = 0.36 between other groups). The mMAP24 was inversely associated with hospital mortality (unadjusted OR 0.82 per 5 mmHg higher mMAP24, 95% CI 0.76–0.88, p < 0.001; optimal cutoff 64.6 mmHg; Fig. 2). Similar findings were observed in patients with ACS or HF (Supplemental Figures 2A and 2B), patients with CA (Supplemental Figures 3A and 3B), patients with a pre-admission diagnosis of hypertension (Supplemental Figures 4A and 4B), and patients aged 65 years and older (Supplemental Figure 5). Mean values of systolic, diastolic, and mean BP were significantly lower for inpatient deaths at all time points (1, 6, and 24 h), although the magnitude of these differences was relatively modest (Supplemental Figure 6). The association between mMAP24 and mortality remained after excluding patients with SCAI stages A and B of CS (adjusted OR 0.850 per 5 mmHg higher, 95% CI 0.755–0.957, p = 0.007), as well as in the overall cohort after adjusting for SCAI CS stage (adjusted OR 0.913 per 5 mmHg, 95% CI 0.838–0.994, p = 0.035). The association between mMAP24 and hospital mortality persisted after excluding patients with an admission diagnosis of sepsis (adjusted OR 0.873, 95% CI 0.794–0.960, p = 0.0052). The association between mMAP24 and hospital mortality was present in patients without sepsis (adjusted OR 0.873, 95% CI 0.794–0.960, p = 0.0052). The optimal mMAP24 cutoff for predicting hospital mortality was 65.2 mmHg in patients with ACS and 70.0 mmHg in patients with HF. Hospital mortality varied as a function of mMAP24 and the maximum number of vasopressors during the first 24 h and the peak VIS during the first 24 h (Fig. 3). In subgroups of patients with and without a diagnosis of hypertension, there was no association between mMAP24 and the incidence of severe AKI (p = 0.83) (Supplemental Figures 4A and 4B).
Fig. 2.
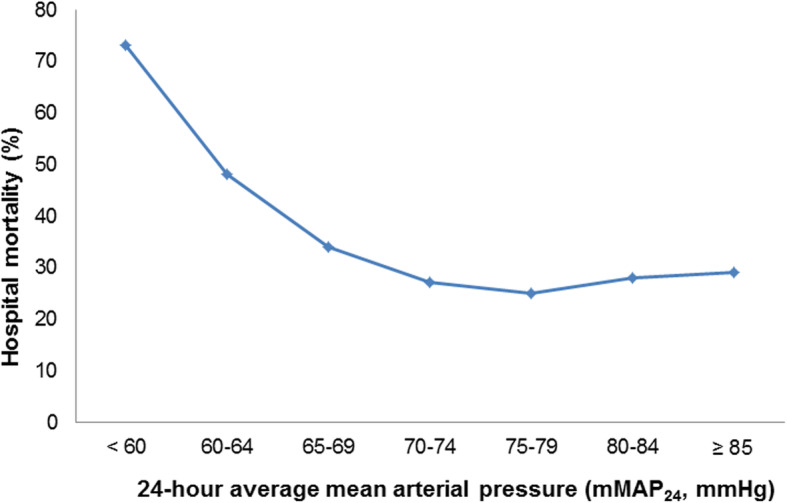
Hospital mortality as a function of the average mean arterial pressure in the first 24 h of cardiac intensive care unit (CICU) admission (mMAP24)
Fig. 3.

Hospital mortality as a function of 24-h average mean arterial pressure (mMAP24) and vasoactive infusion score (VIS)
After multivariable adjustment, mMAP24 remained inversely associated with hospital mortality (adjusted OR 0.89 per 5 mmHg higher mMAP24, 95% CI 0.82–0.97, p = 0.01, Table 2). Patients with a mMAP24 < 65 mmHg were at higher risk of hospital mortality (adjusted OR 2.05, 95% CI 1.38–3.02, p < 0.001), with no difference between patients with mMAP24 65–75 mmHg and mMAP24 ≥ 75 mmHg (p = 0.77).
Table 2.
Predictors of hospital mortality on multivariable regression. Only predictors with p < 0.1 are shown. Additional predictors with p ≥ 0.1 included in the model were white race, noninvasive ventilator use, creatinine, hemoglobin, PAC, RBC transfusion, respiratory failure, HF, and sepsis. Final model validation AUC 0.80
| Variable | Adjusted OR | 95% CI | p value |
|---|---|---|---|
| APACHE-IV predicted mortality | 3.61 | 1.81–7.22 | < 0.001 |
| Cardiac arrest | 3.11 | 2.21–4.36 | < 0.001 |
| Dialysis during CICU admission | 2.64 | 1.68–4.14 | < 0.001 |
| mMAP24 < 65 mmHg | 2.05 | 1.38–3.02 | < 0.001 |
| Charlson Comorbidity Index | 1.07 | 1.01–1.14 | 0.03 |
| Age (per year) | 1.03 | 1.02–1.04 | < 0.001 |
| Peak vasoactive infusion score (VIS) during first 24 h | 1.01 | 1.01–1.02 | < 0.001 |
| IABP | 0.64 | 0.44–0.92 | 0.02 |
Abbreviations: APACHE Acute Physiology and Chronic Health Evaluation, IABP intra-aortic balloon pump, mMAP24 average mean arterial pressure (MAP) in the first 24 h
Discussion
In this retrospective study of a large tertiary CICU patient population with CS, we demonstrate that mMAP24 is inversely associated with CICU and hospital mortality after adjusting for illness severity and CICU therapies, including patients with common CICU diagnoses such as ACS, HF, and CA. These data suggest that mMAP24 is an independent predictor of hospital mortality in CS patients across subgroups, even when accounting for vasopressor requirements. The association between mMAP24 and hospital mortality remained even after adjustment for the SCAI shock stage, suggesting that the importance of mMAP24 extends beyond initial shock severity alone. Patients who were able to maintain a MAP above 65 mmHg had lower hospital mortality; similar results were seen among patients with ACS, whereas unexpectedly patients with HF seemed to have better outcomes at a MAP above 70 mmHg. Among patients with a MAP below 65 mmHg, hospital mortality increased in proportion to the severity of hypotension, and patients with the most severe hypotension were at highest risk of mortality. We observed a threshold effect, such that patients with progressively higher mMAP24 above these levels did not have further decreases in mortality. The prevalence of non-cardiovascular organ failure and severe AKI was higher among patients with lower MAP, potentially explaining why these patients had higher mortality. Notably, not all patients who had an admission diagnosis of CS received vasopressors, mechanical circulatory support, or had manifest hypoperfusion on CICU admission, suggesting that some patients had resolved CS. These data suggest that maintaining MAP goals lower than 65 mmHg may not be adequate to preserve organ perfusion. However, targeting MAP goals higher than 65 mmHg may potentially expose patients to added hazards from the known adverse effects of vasoactive drugs without definite benefit. We did not observe a difference in MAP thresholds in patients with a pre-existing history of hypertension, and our findings do not suggest that a higher MAP is preferentially associated with any decrease in mortality or end-organ injury among this subgroup of patients.
Evidence-based therapies available to patients with CS remain limited, and much of the critical care strategies in the CICU have been extrapolated from other non-CS populations [3]. The optimal MAP goal in patients with CS has not been well defined. Current strategies are based on evidence from patients with other forms of circulatory shock, particularly patients with sepsis whose physiology is entirely different from CS due to the presence of a low diastolic blood pressure from vasoplegia which drives down the MAP [7, 18]. The SEPSISPAM trial compared a vasopressor strategy targeting MAP of 80–85 mmHg to a target of 65–70 mmHg in patients with septic shock and found no difference in death or AKI at 28 days despite more arrhythmias in the higher MAP arm; patients with chronic hypertension maintained at the higher MAP target were less likely to suffer from AKI [7]. By contrast, a recent multicenter randomized controlled trial of patients 65 years and older who were admitted to the ICU with septic shock demonstrated that permissive hypotension (MAP 60–65 mmHg) reduced vasopressor exposure without increasing the risk of mortality or AKI (including patients with and without hypertension) [9]. The findings of our study indirectly support the safety of a lower MAP target (i.e., 65–70 mmHg) in CS patients, but did not show a benefit of higher MAP targets among patients with a history of hypertension. Evidence supports the use of vasopressors such as norepinephrine that have a lower rate of cardiovascular adverse events, including increased myocardial oxygen demand, ischemia, arrhythmias, and mortality [1, 14]. In general, increasing doses of vasoactive agents increase the risk of cardiovascular adverse events and are associated with higher mortality, and current recommendations suggest the lowest effective dose necessary to achieve a target MAP [3, 14]. We observed a strong independent association between higher vasopressor doses based on VIS24 and higher hospital mortality.
Many CS patients are already maximally vasoconstricted due to cardiac pump failure, and further increasing afterload with vasopressors may be deleterious, particularly when targeting higher MAP goals [3]. In the distinct high-risk subgroup of patients with CA, which is commonly associated with abnormal cerebral blood flow autoregulation, retrospective evidence suggests that maintenance of a higher MAP may be considered to improve cerebral perfusion and neurological outcomes [6]. However, randomized controlled trials of higher MAP targets (80 or 85 to 100 mmHg) have not shown an improvement in neurological outcomes when compared to a target of 65 mmHg [18, 19]. Likewise, we did not observe a different MAP threshold for patients with CA and CS in our study. The use of higher vasopressor doses to achieve a higher target MAP after CA poses a risk of increasing the arrhythmia burden, which may be particularly harmful in CA patients with an arrhythmic substrate. As a result, current society guidelines for patients with septic shock or CA recommend MAP targets of 65–70 mmHg [6, 20].
It is crucial to note that the observed association between outcomes and mMAP24 demonstrated in our retrospective observational study is not the same as testing specific MAP goals for titrating vasopressor therapy in CS patients. We could not determine the MAP goals used by the treatment team, and therefore, we could not distinguish patients who had low MAP due to failure to achieve a prescribed MAP goal from those in whom a lower MAP was successfully targeted. Besides, patients with lower MAP had more severe illness by all relevant metrics and did not receive as many supportive cardiovascular procedures; we could not exclude the possibility that these patient-specific factors drove the adverse outcomes as opposed to the lower MAP itself. Importantly, CS patients may preferentially benefit from tailored vasopressor and inotropic support guided by hemodynamic data, such as those derived from a pulmonary artery catheter, rather than a “one-size-fits-all” approach [3]. Nonetheless, our data clearly show that an inability to maintain MAP ≥ 65 mmHg during the first 24 h after CICU admission is associated with adverse outcomes in CICU patients with CS.
Limitations
This retrospective cohort study has a number of inherent limitations, including the potential for unmeasured confounders and missing data to have influenced the results. This single-center cohort may not fully represent the general patient population with CS. The mMAP24 values included both invasive and noninvasive MAP measurements, but we could not determine which MAP measurements were made using each method, and mMAP24 potentially included a mixture of both. Admission diagnoses are based on ICD-9 coding and may underrepresent the number of patients with CS and associated comorbidities. The inclusion of a mixed CICU population without available hemodynamic or echocardiographic data implies that some patients may have had non-cardiogenic or mixed cardiogenic-septic shock states. MAP data is limited to the first 24 h of CICU admission, so this study cannot evaluate the association between patient outcomes and MAP beyond 24 h. For this reason, we specifically focused on organ failure occurring during the first 24 h of CICU admission and cannot comment on later development of organ failure. Detailed data regarding vasopressor doses over time could potentially provide additional indication of illness severity in the context of mMAP24; unfortunately, these data were not available. Patients with mMAP24 < 65 mmHg were less likely to undergo PCI; the reasons for this are likely multifactorial and largely dependent on clinical factors and contraindications (e.g., severe shock, renal injury, or concern for cerebral anoxia). Unfortunately, our retrospective dataset cannot account for these clinical decisions. In addition, we could not determine the incidence of relevant cardiovascular adverse events attributable to vasopressor and inotrope therapy. Due to lack of data availability, we could not account for patient-level variables before CICU admission, including specific diagnostic or therapeutic interventions which took place before CICU admission.
Conclusions
There was an inverse correlation between mMAP in the first 24 h and hospital mortality among patients with CS admitted to the CICU. Patients with a MAP below 65 mmHg during the first 24 h after CICU admission had an increased risk of mortality. These findings provide indirect support for a MAP target of 65 mmHg for most CICU patients with CS. Further prospective research should evaluate which, if any, MAP goals are optimal for patients with specific hemodynamic or etiologic subtypes of CS.
Supplementary information
Additional file 1: Supplemental Figure 1. Patient flow diagram describing inclusion/exclusion criteria and patient groups. Supplemental Figure 2AB. Hospital mortality as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with acute coronary syndrome (A) or heart failure (B). Supplemental Figure 3AB. Hospital mortality and incidence of severe acute kidney injury (AKI) as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with (A) and without (B) cardiac arrest. Supplemental Figure 4AB. Hospital mortality and incidence of severe acute kidney injury (AKI) as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with (A) and without (B) a pre-admission diagnosis of hypertension. Supplemental Figure 5. Hospital mortality as a function of the 24-hour average mean arterial pressure (mMAP24), among patients age 65 and older. Supplemental Figure 6. Mean values of systolic (circles), diastolic (arrows), and mean (diamonds) blood pressure over the first 1, 6, and 24 hours of the CICU stay.
Abbreviations
- ACS
Acute coronary syndrome
- AKI
Acute kidney injury
- CA
Cardiac arrest
- CICU
Cardiac intensive care unit
- CS
Cardiogenic shock
- HF
Heart failure
- MAP
Mean arterial pressure
- mMAP24
Average mean arterial pressure during first 24 h of CICU admission
Authors’ contributions
JCJ helped conceive of the study, designed the data analysis plan, acquired the data, performed the statistical analysis, and drafted the manuscript. BB helped conceive of the study, assisted with the analysis, and drafted the manuscript. MT, GWB, MRB, and KK contributed to the data analysis and drafting of the manuscript. All authors were involved in the data interpretation and manuscript revision for intellectual content. All authors have provided approval of the final manuscript.
Funding
None declared.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article and its supplementary materials.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Mayo Clinic (IRB # 16-000722) as posing minimal risk to patients and was performed under a waiver of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s13054-020-03217-6.
References
- 1.De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent J-L, et al. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362(9):779–789. doi: 10.1056/NEJMoa0907118. [DOI] [PubMed] [Google Scholar]
- 2.Berg DD, Bohula EA, van Diepen S, Katz JN, Alviar CL, Baird-Zars VM, Barnett CF, Barsness GW, Burke JA, Cremer PC, et al. Epidemiology of shock in contemporary cardiac intensive care units. Circ Cardiovasc Qual Outcomes. 2019;12(3):e005618. doi: 10.1161/CIRCOUTCOMES.119.005618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136(16):e232–e268. doi: 10.1161/CIR.0000000000000525. [DOI] [PubMed] [Google Scholar]
- 4.Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr, Ganiats TG, Holmes DR, Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;130(25):E344–E426. doi: 10.1161/CIR.0000000000000134. [DOI] [PubMed] [Google Scholar]
- 5.Werdan K, Russ M, Buerke M, Delle-Karth G, Geppert A, Schoendube FA. Cardiogenic shock due to myocardial infarction: diagnosis, monitoring and treatment a German-Austrian S3 guideline. Deutsches Arzteblatt International. 2012;109(19):343–U315. doi: 10.3238/arztebl.2012.0343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, Leary M, Meurer WJ, Peberdy MA, Thompson TM, et al. Part 8: post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S465–S482. doi: 10.1161/CIR.0000000000000262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Asfar P, Meziani F, Hamel J-F, Grelon F, Megarbane B, Anguel N, Mira J-P, Dequin P-F, Gergaud S, Weiss N, et al. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014;370(17):1583–1593. doi: 10.1056/NEJMoa1312173. [DOI] [PubMed] [Google Scholar]
- 8.Heart Outcomes Prevention Evaluation Study I. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000;342(3):145–153. doi: 10.1056/NEJM200001203420301. [DOI] [PubMed] [Google Scholar]
- 9.Lamontagne F, Richards-Belle A, Thomas K, Harrison DA, Sadique MZ, Grieve RD, Camsooksai J, Darnell R, Gordon AC, Henry D et al: Effect of reduced exposure to vasopressors on 90-day mortality in older critically ill patients with vasodilatory hypotension. JAMA. 2020;323(10):938–49. 10.1001/jama.2020.0930. Online ahead of print. [DOI] [PMC free article] [PubMed]
- 10.Jentzer JC, Bennett C, Wiley BM, Murphree DH, Keegan MT, Gajic O, Wright RS, Barsness GW: Predictive value of the sequential organ failure assessment score for mortality in a contemporary cardiac intensive care unit population. J Am Heart Assoc. 2018;7(6):e008169. 10.1161/JAHA.117.008169. [DOI] [PMC free article] [PubMed]
- 11.Jentzer JC, Murphree DH, Wiley B, Bennett C, Goldfarb M, Keegan MT, Murphy JG, Wright RS, Barsness GW. Comparison of mortality risk prediction among patients >/=70 versus <70 years of age in a cardiac intensive care unit. Am J Cardiol. 2018;122(10):1773–1778. doi: 10.1016/j.amjcard.2018.08.011. [DOI] [PubMed] [Google Scholar]
- 12.Bennett CE, Wright RS, Jentzer J, Gajic O, Murphree DH, Murphy JG, Mankad SV, Wiley BM, Bell MR, Barsness GW. Severity of illness assessment with application of the APACHE IV predicted mortality and outcome trends analysis in an academic cardiac intensive care unit. J Crit Care. 2018;50:242–246. doi: 10.1016/j.jcrc.2018.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Herasevich V, Pickering BW, Dong Y, Peters SG, Gajic O. Informatics infrastructure for syndrome surveillance, decision support, reporting, and modeling of critical illness. Mayo Clin Proc. 2010;85(3):247–254. doi: 10.4065/mcp.2009.0479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jentzer JC, Wiley B, Bennett C, Murphree DH, Keegan MT, Kashani KB, Bell MR, Barsness GW. Temporal trends and clinical outcomes associated with vasopressor and inotrope use in the cardiac intensive care unit. Shock. 2020;53(4):452–459. doi: 10.1097/SHK.0000000000001390. [DOI] [PubMed] [Google Scholar]
- 15.Brueske B, Sidhu MS, Schulman-Marcus J, Kashani KB, Barsness GW, Jentzer JC. Hyperkalemia is associated with increased mortality among unselected cardiac intensive care unit patients. J Am Heart Assoc. 2019;8(7):e011814. doi: 10.1161/JAHA.118.011814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jentzer JC, Wiley B, Bennett C, Murphree DH, Keegan MT, Gajic O, Kashani KB, Barsness GW: Early noncardiovascular organ failure and mortality in the cardiac intensive care unit. Clin Cardiol. 2020;43(5):516–23. 10.1002/clc.23339. [DOI] [PMC free article] [PubMed]
- 17.Rocca WA, Yawn BP, St Sauver JL, Grossardt BR, Melton LJ., 3rd History of the Rochester Epidemiology Project: half a century of medical records linkage in a US population. Mayo Clin Proc. 2012;87(12):1202–1213. doi: 10.1016/j.mayocp.2012.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jakkula P, Pettila V, Skrifvars MB, Hastbacka J, Loisa P, Tiainen M, Wilkman E, Toppila J, Koskue T, Bendel S, et al. Targeting low-normal or high-normal mean arterial pressure after cardiac arrest and resuscitation: a randomised pilot trial. Intensive Care Med. 2018;44(12):2091–2101. doi: 10.1007/s00134-018-5446-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ameloot K, De Deyne C, Eertmans W, Ferdinande B, Dupont M, Palmers PJ, Petit T, Nuyens P, Maeremans J, Vundelinckx J, et al. Early goal-directed haemodynamic optimization of cerebral oxygenation in comatose survivors after cardiac arrest: the Neuroprotect post-cardiac arrest trial. Eur Heart J. 2019;40(22):1804–1814. doi: 10.1093/eurheartj/ehz120. [DOI] [PubMed] [Google Scholar]
- 20.Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi: 10.1007/s00134-017-4683-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Supplemental Figure 1. Patient flow diagram describing inclusion/exclusion criteria and patient groups. Supplemental Figure 2AB. Hospital mortality as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with acute coronary syndrome (A) or heart failure (B). Supplemental Figure 3AB. Hospital mortality and incidence of severe acute kidney injury (AKI) as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with (A) and without (B) cardiac arrest. Supplemental Figure 4AB. Hospital mortality and incidence of severe acute kidney injury (AKI) as a function of the 24-hour average mean arterial pressure (mMAP24), among patients with (A) and without (B) a pre-admission diagnosis of hypertension. Supplemental Figure 5. Hospital mortality as a function of the 24-hour average mean arterial pressure (mMAP24), among patients age 65 and older. Supplemental Figure 6. Mean values of systolic (circles), diastolic (arrows), and mean (diamonds) blood pressure over the first 1, 6, and 24 hours of the CICU stay.
Data Availability Statement
The dataset supporting the conclusions of this article is included within the article and its supplementary materials.