

Abstract
Introduction:
The da Vinci® X hybrid systems (Intuitive Surgical®, Sunnyvale CA) provides standard sites recommendations for port placement during robotic surgery; including that for colorectal procedures. The author's encountered challenges while adhering to the provided instructions, such as clash of instruments and arms and need for additional ports, and hence to overcome these challenges attempted a few innovative technical modifications. The surgical results as well as merits of the revised Indian (Manipal) port placement with single docking technique are presented here.
Methods:
Twenty patients underwent robotic rectal resection at the Department of Surgical Oncology and Robotic Surgery, Manipal Comprehensive Cancer Centre, Bengaluru, India, between December 2017 and June 2018. A randomised controlled study was conducted to compare the two techniques. Ten patients were operated using hybrid da Vinci® ‘X’ system using the manufacturer's recommendations and 10 by the modified Indian (Manipal) port placement with a single docking technique.
Result and Conclusions:
The Indian (Manipal) modifications of port placements are optimal for colorectal procedures such as low anterior resection as well as for ultralow anterior resections. The intraoperative parameters compared between the recommendations of the Intuitive® (da Vinci® systems) and attempted modifications demonstrated statistically significant advantages with the use of the revised techniques. The improvements offered by this modification include no additional requirements of ports or staplers, lesser clash amongst instruments as well as arms, better mobilisation of splenic flexure amongst others.
Keywords: Indian (Manipal) port placement technique, port placement, rectal cancer, robotic rectal resection, single docking
INTRODUCTION
The robotic surgical systems offer several advantages such as a camera with three-dimensional views of the operating field, 10 times magnification and freedom of articulation and rotation.[1] The ease and comfort of robotic consoles also enhances surgeons performances and allows the surgical team to perform the procedure with lesser fatigability.[2] The da Vinci® X hybrid systems (Intuitive Surgical®, Sunnyvale CA) are approved for the use in colorectal surgery. The safety, feasibility, technique and post-operative outcomes of robotic-assisted surgery for rectal cancer procedures already established in previous studies.[3] Standardised sites for port placements during robotic surgery of colorectal anterior, low and ultralow anterior resections are recommended by the manufacturers. Conventional recommendations for the rectosigmoid region include; oblique linear ports along the line of mesenteric attachment and linear horizontal ports for the low and ultralow anterior resections, depending on the target anatomy. Previously, studies have commented on the performance of port placements for single docking for S system[4] and Si system;[5] however, there is very limited literature about performance for port placement for the hybrid “X” system.
The Department of Surgical Oncology and Robotic Surgery, Manipal Comprehensive Cancer Centre is the first centre in India to procure and treat patients using the hybrid X system. The authors encountered certain challenges while adhering to the instructions on the procedure card provided by the manufacturers such as clash of instruments and arms and need for additional ports, and hence attempted innovative modifications; the Indian (Manipal) port placement to overcome these issues.
METHODS
A randomised controlled study was conducted comparing the innovative Indian (Manipal) port placement technique with the manufacturer's recommendations. Between December 2017 and June 2018, 20 patients reporting to the department of surgical oncology and robotic surgery Manipal hospitals with carcinoma rectum and indications for robotic surgical interventions were included in the study. Written consent was sought from willing patients after a detailed and thorough explanation of the process. Patients also included post-chemoradiation as well as upfront surgical candidates. Patients who required abdominoperineal resections and paediatric cases were excluded from this study. All 20 procedures were performed by the same operating team headed by an experienced robotic colorectal surgeon.
Procedures involving robotic low anterior and ultralow anterior resections were performed. Ten patients were operated according to the manufacturer's recommendation and 10 by the modified Indian (Manipal) port placement with single docking technique.
The manufacturer's procedure card for the da Vinci® X systems recommends linear horizontal port placement, for the low and ultralow anterior resections [Figure 1a][6] For the Xi system targeting the rectosigmoid region, in the orientation of the long axis of mesentery oblique linear port placement was recommended [Figure 1b].[7] The procedure card also recommended dual docking for approaching another quadrant of the abdomen. The operating team encountered the enlisted challenges while following the procedure card [Table 1].
Figure 1.

(a) Intuitive Port placement (Clinical Specialty Guide, X), (b) Intuitive port placement (Clinical Specialty Guide – Xi system)
Table 1.
Challenges encountered while adhering to manufacturers recommendations
| 1. External clash of Arms |
| 2. Clash of instruments suggesting need for additional ports |
| 3. Difficulty in mobilisation of the splenic flexure of colon |
| 4. Restricted arm movements |
| 5. Difficulty in firing the staplers intracorporeally (especially in ultralow anterior resections) due to acute angle of the stapler with the long axis of the rectum |
| 6. Stapler fulcrum directly abutting the iliac vessels , increasing the risk of major iatrogenic vascular injury [Figure 2] |
| Need of >2 staplers for complete rectal transactions |
Figure 2.

Stapler fulcrum directly on the iliac vessels
The hybrid X system lacks the overhead boom, rendering the procedure card with instructions similar to that of Xi system, of limited utility. To overcome the aforementioned challenges, the authors made innovative modifications to the port placement technique. The Indian (Manipal) technique involves single docking with port hopping [Figure 3a and b]. The docking positions of the patient cart for the colorectal surgeries were also suitably modified.
Figure 3.

(a) Diagrammatic representation (b) Clinical image of the innovative Indian (Manipal) port placement technique
Modifications
The patients were started on a liquid diet 2 days before the surgery. After administering general anaesthesia, patients were placed in Trendelenburg position (more than 15°) with height as low as possible. Careful strapping was performed, and a small bolster was positioned below the sacrum. The operating table was given a slight right tilt. Ports were placed according to the modified Indian (Manipal) technique [Figure 3b] after painting and draping. The Veress technique was adopted for insufflation. The OptiView trocar with the camera was introduced in the right lateral position to the umbilicus, roughly at the edge of a square of approximately 4 cm in length with umbilicus being the midpoint. R 1 was introduced in the subumbilical line at approximately 6 to 8 cm from the midline. R 2 was positioned to the left of the midline just besides the falciform ligament. R 3 was positioned in the right suprapubic region, lateral to the lateral umbilical ligament around 3 cm above the pubic symphysis. R 2’ was at the line of the camera port in the left abdominal quadrant around 8 cm from the midline. R 3’ was around 3 cm above and right lateral to the anterior superior iliac spine. A minimum of 6–8 cm distance between the two ports was ensured to avoid crowding of the ports.
In the initial part of inferior mesenteric artery identification and ligation and the splenic flexure mobilisation, R 1, R 2 and R 3 ports were used while R 3’ can be optionally used as an assistant port for bowel retraction as well as traction [Figure 4a].
Figure 4.

(a) R 3’ port used for retraction of the duodenum. (b) R 2 port providing traction to the rectum for the pelvic phase of dissection
During the latter part of the pelvic dissection, R 1 remained at the same position, while R 2 moved to R 2’ and R 3 to R 3'. R 3 could now be changed to assistant 12 mm port for firing the stapler at a much better and safer angle. R 2’ could now be used to give lateral traction on the rectum with a umbilical tape which facilitates dissection for the total mesorectal excision (TME) [Figure 4b]. The position of docking from central or side as recommended by the manufacturers is modified to Centro-Side. This facilitated entire dissection and avoided additional port and dual docking with just port hopping.
On an average the following observations were made with the Indian (Manipal) technique; the total operative time was around 200 min, with around 25–30 min required for docking time and remaining for the console time. Blood loss was around 50–80 ml. Liquid diet was administered to the patients from the 2nd day and the first flatus occurred on the 2nd day as well. The patients recuperated uneventfully and were discharged around the 7th day postoperatively.
RESULTS
In order to study the impact of this innovative modification over the conventional recommendation, the authors divided 20 cases equally and devised four main parameters for comparison. The intraoperative parameters evaluated between the two port placements techniques included external clash of arms, internal clash of instruments, requirements of additional ports and additional staplers for rectal transaction. Statistical analysis included the use of Chi-square tests and independent sample t-tests. P < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 21.0 software (IBM Corp., Armonk, NY).
External clash of arms was observed on an average only 4.9 times using the Indian (Manipal) modifications in comparison to 7.7 times with the manufacturer's recommendations [Graph 1]. The use of the modifications resulted in statistically significant P = 0.013 using Chi-square test. Internal clash of instruments was 9 times with the recommendations and only 6.8 times with the modifications with a P = 0.04 [Graph 1]. The most striking result of the modification was the complete omission of any requirements of additional ports in the completion of the entire procedure. Additional ports were always required with the manufacturer's recommendations; however, there was absolutely no requirement with the modification [Graph 2]. Two or more additional staplers were required for rectal transaction in 70% of cases performed according to the manufacturer's recommendations but only 20% cases by the Indian (Manipal) technique [Graph 2]; which was a statistically significant improvement with a P= 0.0029 (independent sample t-test).
Graph 1.
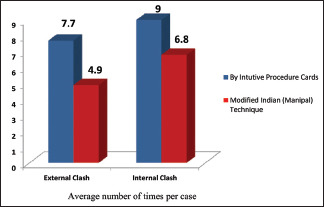
The intra operative parameters compared between the two port placements techniques
Graph 2.

Need for additional instrumentation compared between the two port placements techniques
DISCUSSION
The manufacturer's procedure card for the da Vinci® systems is instructive and helpful albeit with aforementioned challenges. The Indian (Manipal) modification comprises of a set of innovative variations designed to overcome these issues. Several similar instances of operating teams attempting amendments to the manufacturer's instructions are documented in the literature.[1,3,4,5]
Mégevand et al.[5] attempted single docking in 83 patients and their findings concurred with the present study in terms of reduced operating time and maximised advantages of robotic approaches; however, the point of difference is that no separate port for assistant was required in the present study. Similar to the present study, Jafari and Stamos also employed the Veress needle for insufflations of the abdomen and the optical trocar for gaining visual access to the abdomen; as described in book by Ross et al. (2015).[8] D'Annibale et al.[9] and Hellan et al.[10] used initially three arms for mobilisation of the splenic flexure in the first step and later introduced the fourth arm for TME whereas four arms are employed from the initial phase in the Indian (Manipal) technique. Baek and Kim, as described in book by Obais V (2017);[11] compared the hybrid technique that incorporates laparoscopic and robotic techniques for colonic and pelvic regions respectively with the total robotic technique that combines both the phases into a single robotic technique and is similar to the present study and obtained comparable operative outcomes including operating times. Cui et al.[12] used a novel procedure for removing the specimen through anus instead of separate incision; although abdominal incision was preferred in the Indian (Manipal) technique; still the operative parameters such as operating time, amount of blood loss and post-operative convalescence time were similar. The operating time of the Indian (Manipal) technique is was about 200 min and was lesser than the series of cases reported by Choi et al.[4] which was about 300 min. Hellan et al.[10] also remarked about the same challenges the surgical team in the present study observed; that the docking procedure, patient positioning and collisions between arms and arms and instruments prolong the operation time. Halabi et al.[13] also noted that repeated docking and undocking of the robot is often needed when using the robot to perform surgical procedure in different compartments in the abdominal cavity, result in prolonged operating time and delayed conversion in case of massive bleeding.
Operating time, estimated blood loss, reduction in hospital stay and bowel function recovery observed in the present study were similar to observations of Bandar et al.[2] who studied the scope of robotic surgery in colorectal cancers. Although the Indian (Manipal) technique employs innovative modification for colorectal robotic surgery several other authors have also attempted modifications form the procedure card, these include Chang et al.,[14] Cestari et al.,[15] and Jain[16] who attempted simplifying the process, patient positioning and port placement for various other application of the da Vinci X system.
CONCLUSIONS
The Indian (Manipal) modifications of port placements have demonstrated several improvements over conventional recommendations for the colorectal procedures such as low anterior resection and ultralow anterior resections. The most notable advantages are that it is a single docking technique with no additional requirements of ports or staplers, lesser clash amongst instruments and arms, better and safer angles for stapler firing, better splenic flexure mobilisation. All expected quadrants required to be exposed for these surgeries are better addressed with these modifications.
In terms of procedures such as abdominoperineal resections, anterior resections and left hemicolectomy also, the same port technique and docking can be used with or without the need for conversion of R3 to assistant port.
This study is able to ascertain the benefits of modified port placements and docking position for the da Vinci® X system, which indeed would facilitate robotic colorectal surgeons achieve better competency and reduce the time duration with more effective results. Future studies by using the innovative Indian (Manipal) port placement with single docking technique will further establish its clinical efficiency.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Zawadzki M, Rząca M, Czarnecki R, Obuszko Z, Jacyna K, Stewart L, et al. Beginning robotic assisted colorectal surgery – It's harder than it looks! Wideochir Inne Tech Maloinwazyjne. 2014;9:562–8. doi: 10.5114/wiitm.2014.45494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bandar MH, Sabilah JA, Kim NK. The current scope of robotic surgery in colorectal cancer. Adv Robot Autom. 2015;S2:2. [Google Scholar]
- 3.Somashekhar SP, Ashwin KR, Rajashekhar J, Zaveri S. Prospective randomized study comparing robotic-assisted surgery with traditional laparotomy for rectal cancer-Indian study. Indian J Surg. 2015;77:788–94. doi: 10.1007/s12262-013-1003-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Choi DJ, Kim SH, Lee PJ, Kim J, Woo SU. Single-stage totally robotic dissection for rectal cancer surgery: Technique and short-term outcome in 50 consecutive patients. Dis Colon Rectum. 2009;52:1824–30. doi: 10.1007/DCR.0b013e3181b13536. [DOI] [PubMed] [Google Scholar]
- 5.Mégevand J, Rusconi A, Amboldi M, Lillo L, Lenisa L, et al. Totally robotic low anterior resection and left colectomy with systematic splenic flexure mobilization a single docking procedure for sigmoid and rectal cancer: Technical notes and results. JSM Surg Oncol Res. 2016;1:1003. [Google Scholar]
- 6.Intuitive Surgical® X Clinical Specialty Guide. [Last accessed on 2019 Mar 27]. Available from : https://wwwdavincisurgerycommunitycom/Clinical/General_Surgerytab1=CL .
- 7.Intuitive Surgical® Xi Clinical Specialty Guide. [Last accessed on 2019 Mar 27]. Available from: https://wwwdavincisurgerycommunitycom/Clinical/General_Surgerytab1=CL .
- 8.Ross HM, Lee S, Mutch M, Rivadeneira DE, Steele SR, editors. Minimally Invasive Approaches to Colon and Rectal Disease: Technique and Best Practices. New York: ©Springer, Science, Business Media; 2015. [Google Scholar]
- 9.D'Annibale A, Morpurgo E, Fiscon V, Trevisan P, Sovernigo G, Orsini C, et al. Robotic and laparoscopic surgery for treatment of colorectal diseases. Dis Colon Rectum. 2004;47:2162–8. doi: 10.1007/s10350-004-0711-z. [DOI] [PubMed] [Google Scholar]
- 10.Hellan M, Anderson C, Ellenhorn JD, Paz B, Pigazzi A. Short-term outcomes after robotic-assisted total mesorectal excision for rectal cancer. Ann Surg Oncol. 2007;14:3168–73. doi: 10.1245/s10434-007-9544-z. [DOI] [PubMed] [Google Scholar]
- 11.Obias V, editor. Robotic Colon and Rectal Surgery. Switzerland: ©Springer International Publishing; 2017. pp. 59–78. [Google Scholar]
- 12.Cui B, Lei S, Liu K, Yao H. Robotic low anterior resection plus transanal natural orifice specimen extraction in a patient with situs inversus totalis. BMC Surg. 2018;18:64. doi: 10.1186/s12893-018-0394-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Halabi WJ, Kang CY, Jafari MD, Nguyen VQ, Carmichael JC, Mills S, et al. Robotic-assisted colorectal surgery in the United States: A nationwide analysis of trends and outcomes. World J Surg. 2013;37:2782–90. doi: 10.1007/s00268-013-2024-7. [DOI] [PubMed] [Google Scholar]
- 14.Chang C, Steinberg Z, Shah A, Gundeti MS. Patient positioning and port placement for robot-assisted surgery. J Endourol. 2014;28:631–8. doi: 10.1089/end.2013.0733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cestari A, Buffi NM, Scapaticci E, Lughezzani G, Salonia A, Briganti A, et al. Simplifying patient positioning and port placement during robotic-assisted laparoscopic prostatectomy. Eur Urol. 2010;57:530–3. doi: 10.1016/j.eururo.2009.11.028. [DOI] [PubMed] [Google Scholar]
- 16.Jain M. Making robotic surgery easier and safer: A clinical review. WJLP. 2012;5:67–71. [Google Scholar]