

Supplemental Digital Content is available in the text
Keywords: emergency service, frequent user, hospital, risk factor
Abstract
Emergency department (ED) crowding is a public health burden that impedes the provision of high-quality emergency care and is related to poor outcomes. Frequent ED visits are known to contribute to ED crowding. This study aimed to identify frequent ED users’ characteristics and risk factors related to frequent ED visits.
A retrospective observational study was conducted using ED-based data derived from adult patients at a university hospital. The main exposure variable was frequent ED visits, which were defined as ≥4 visits within 12 months (January 1–December 31, 2018). Characteristics and risk factors for frequent ED users were evaluated using stepwise regression analysis.
Within the study period, there were 36,932 ED visits involving 29,759 patients. Of these, 3031 (8.2%) visits were from 556 (1.9%) patients classified as frequent ED users. The independent risk factors for frequent ED visits were older patients (≥65 years); the winter season; daytime discharge from ED; patients with medical aid insurance; and patients designated as high acuity at their first visit. Patients with a malignant neoplasm, mental health disorder, alcohol-related liver disease, chronic kidney disease, or chronic obstructive pulmonary disease were associated with more frequent ED visits.
Frequent ED users comprised a significant proportion of total ED visits. Frequent ED users were more likely than occasional ED users to be in poorer health, older, or have a chronic disease or a mental health disorder.
1. Introduction
Emergency department (ED) crowding is a public health concern, especially in developed countries, as the number of visits to the ED have increased over the past decade.[1,2] ED crowding impedes the quality of emergency care, which leads to delays in definitive care and poor clinical outcomes.[3,4]
One possible explanation for ED crowding is frequent ED visits,[5] which are defined as repeated ED visits by the same patient over a period of time, commonly defined as ≥4 visits per year.[6,7] For various reasons, frequent ED users account for only 4.5% to 8.0% of total ED patients, but comprise between 21% and 28% of annual ED visits.[8] A previous study conducted in Korea reported that 3.1% of the total number of ED patients comprised frequent ED users who accounted for 14% of ED visits annually and 17.2% of the total medical costs from all ED visits.[9]
Frequent ED users are more likely to have poor physical health with chronic disease, resulting in high hospital admission rates and mortality compared with nonfrequent users.[10] Moreover, they absorb other available health care resources and increase medical costs unnecessarily.[11,12] Various interventions aimed at targeting these patients have been implemented, such as case management, individual care planning, prehospital diversion strategies to nonurgent care, and strengthening primary care.[5,13]
Frequent ED user characteristics, however, appear to be site-specific and are difficult to generalize. Identifying the characteristics of frequent ED users and designing appropriate related interventions are essential tasks to reducing the frequency of ED visits and improving associated health care outcomes. We hypothesized that frequent ED users made up a small percentage of ED users but comprised a significant proportion of total ED visits. This study aimed to analyze the characteristics of frequent ED users among adult patients visiting a tertiary university hospital and to identify risk factors affecting frequent ED visits.
2. Methods
2.1. Study design and setting
We conducted a retrospective observational study involving adult patients who had visited a local emergency medical center in 2018. Our research institute is a tertiary university hospital designated as a regional emergency medical center that provides critical care, with emergency physician staff available 24 hours a day. Approximately 45,000 patients visit this ED each year.
The data for analysis in this study were extracted from the National Emergency Department Information System (NEDIS). The NEDIS is an ED-based database built in 2003 and comprises information related to the medical care of patients visiting EDs throughout Korea. Quality management is undertaken by the National Emergency Medical Center, under the authority of the Ministry of Health and Welfare.
2.2. Study population
The study population comprised adult patients who had visited the ED of our research institute between January 1 and December 31, 2018.
2.3. Main outcomes
The primary outcome was to analyze the characteristics of the frequent ED users. The secondary outcome was to identify risk factors for frequent ED users.
2.4. Variables and measurements
The main exposure variable was frequent ED visits. Thresholds of ED visit numbers have varied across studies; therefore, we defined frequent ED visits as ≥4 ED visits within 12 months, which was the most commonly reported definition.[6,7] We collected information from the NEDIS database on age, sex, type of insurance, date of onset, date of ED visit and discharge, disease category (either medical problem or injury), type of ED visit (walk-in, ambulance, or other vehicle), level of acuity, initial mental status, and vital signs at ED visit, and primary diagnosis at each ED visit. The date of the visit and discharge were categorized as either during the day (between 0900 and 1800) or at night (between 1800 and 0900). We assessed the level of acuity based on the Korean Triage and Acuity Scale (KTAS) categories. The KTAS was developed in 2012 and has been implemented in all Korean emergency medical centers since 2016.[14,15] There are 5 KTAS levels ranging from level 1, which represents a critically ill patient requiring immediate medical attention, to level 5, which represents a nonurgent patient. Patients designated as KTAS levels 1 to 3 are presumed to need urgent care. The primary diagnosis was classified according to the 7th edition of the Korean Standard Classification of Disease and Cause of Death (KCD-7).[16]
2.5. Statistical analysis
Categorical variables were expressed as counts and proportions, and continuous variables were expressed as medians and interquartile ranges (IQRs). A Pearson χ2 test for categorical variables and a Wilcoxon rank sum test for continuous variables were used to compare characteristics between the frequent and occasional ED users. To evaluate independent risk factors affecting frequent ED visits, adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated using forward stepwise regression analysis at a significance level of <0.05, which has been used in previous studies.[17] All statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC).
2.6. Ethics statement
Informed consent was waived as this was a retrospective database study. This study was approved by the Institutional Review Board of Chungbuk National University Hospital (IRB No. 2019-07-017).
3. Results
A total of 47,876 ED visits were recorded in 2018. Frequent adult ED users accounted for 1.9% (556 patients) of total ED users (29,759 patients). Among the 36,932 adult patient visits, frequent ED visits accounted for 8.2% (3031 visits) (Fig. 1). In the pediatric population, frequent ED users accounted for 1.2% (106/9116 patients) and frequent ED visits accounted for 4.7% (512/10,944 visits). Compared with adult ED users, pediatric ED users were more likely to attend (61.0%) and be discharged from the ED (66.5%) during the night time than adult ED users (53.4% and 59.6%, respectively) and triaged as a low acuity level at the first visit (all P < .01) (see Tables E1 and E2, Supplemental Content, which demonstrated the characteristics of pediatric and adult ED users at the first visit and the ten most frequent diagnoses among frequent and occasional ED users in the pediatric patients).
Figure 1.
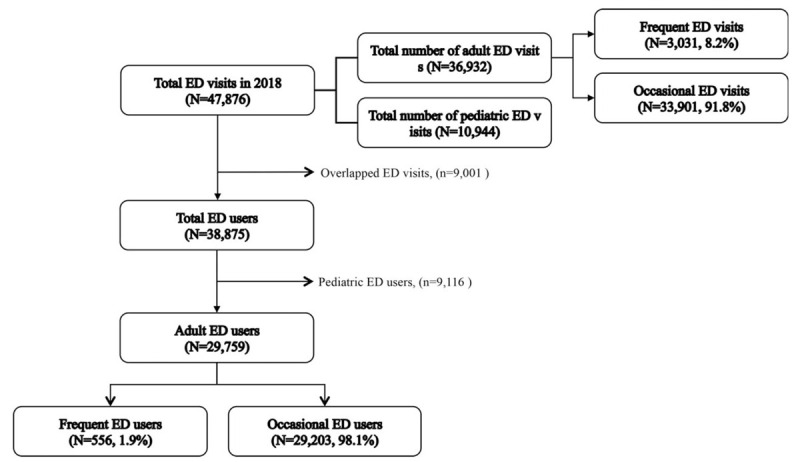
Study population. ED = emergency department.
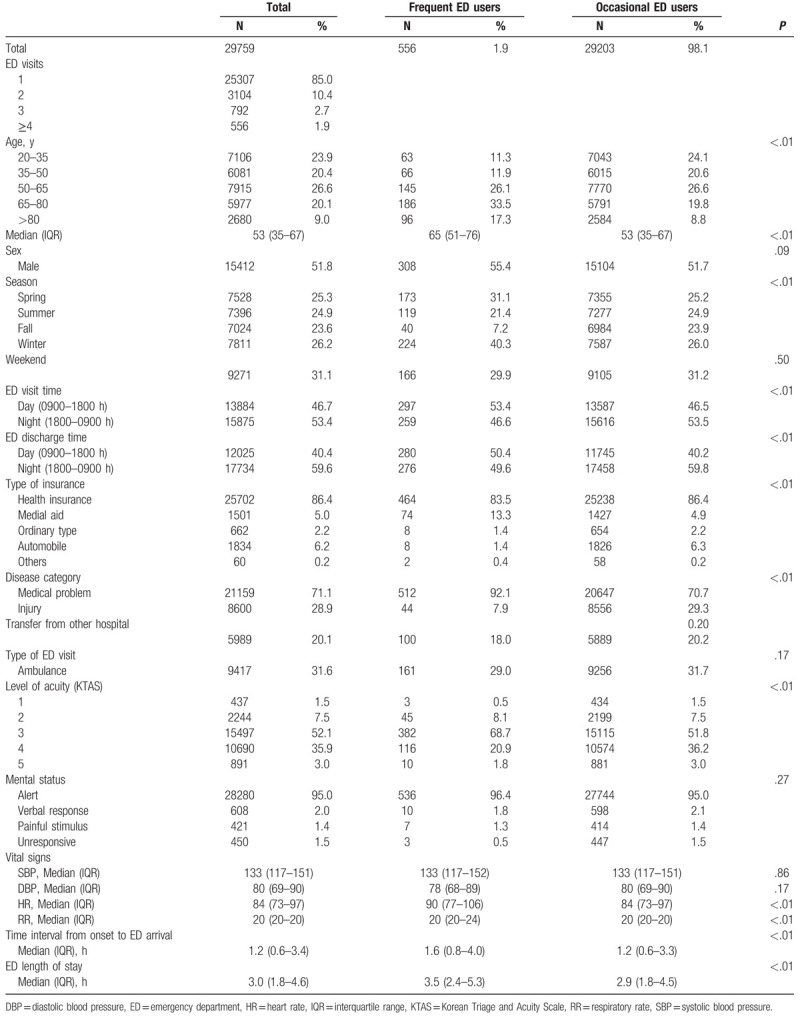
Table 1 shows the demographic characteristics of the adult ED users. Among frequent users, the proportion of patients aged 65 to 80 years (33.5%) and >80 years (17.3%) was higher than among occasional ED users (19.8% and 8.8%, respectively, all P < .01). Frequent ED users were more likely to attend (53.4%) and be discharged from the ED (46.5%) during the day (vs 46.5% and 40.2% in occasional users, respectively, all P < .01). Most patients in both groups had public insurance coverage; however, a higher percentage of frequent ED users had medical aid insurance (13.3% vs 4.9%, P < .01). A KTAS level of 3 was found to be most common in both patient groups, and time intervals from onset to ED arrival and ED length of stay were longer among frequent ED users (all P < .01).
Table 1.
Demographics of frequent and occasional ED users at the first visit.
The distribution of primary diagnoses at the first visit is outlined in Table 2. Malignant neoplasm of the liver and intrahepatic bile ducts was the most observed diagnosis among frequent ED users, whereas among occasional ED users, gastroenteritis and colitis/disease of the intestine (unspecified) was the most frequent primary diagnosis. Alcohol-related liver disease, malignant neoplasm of the bronchus and lung, malignant neoplasm of the stomach, chronic kidney disease, and chronic obstructive pulmonary disease were ranked among the 10 most frequent primary diagnoses for frequent ED users but not among the occasional ED users. In the pediatric population, the 4 most frequent primary diagnoses for frequent and occasional ED users were acute upper respiratory infections, gastroenteritis and colitis/disease of the intestine (unspecified), other and unspecified convulsions, and fever (unspecified) (see Table E2, Supplemental Content, which demonstrated the ten most frequent diagnoses among frequent and occasional ED users in the pediatric patients).
Table 2.
The 10 most frequent primary diagnoses among frequent and occasional ED users at the first visit.
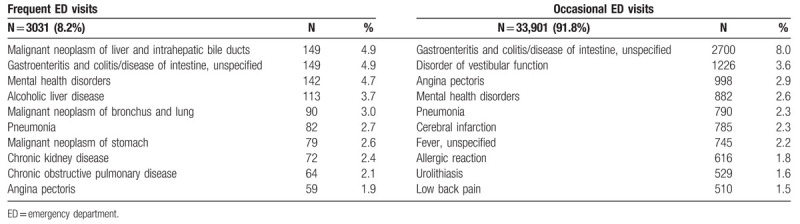
Figure 2A depicts the association between the level of acuity at initial presentation and frequent ED visits. Patients designated as KTAS 3 attended the ED most frequently. Figure 2B shows that older age was associated with increased ED visits.
Figure 2.
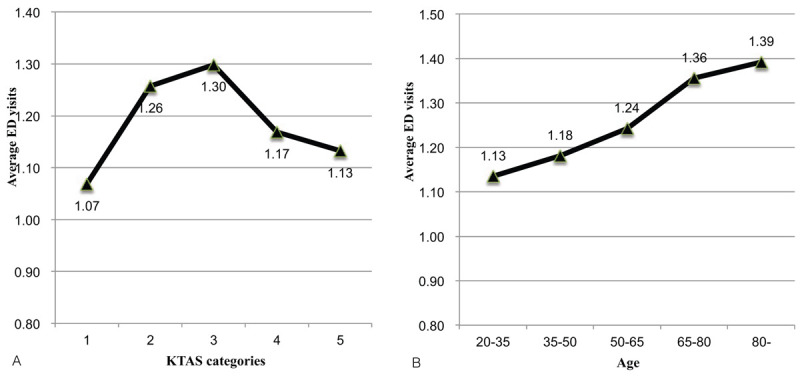
(A) Average ED visit rate according to Korean Triage and Acuity Scale (KTAS 1–5). (B) Age (in years). ED = emergency department.
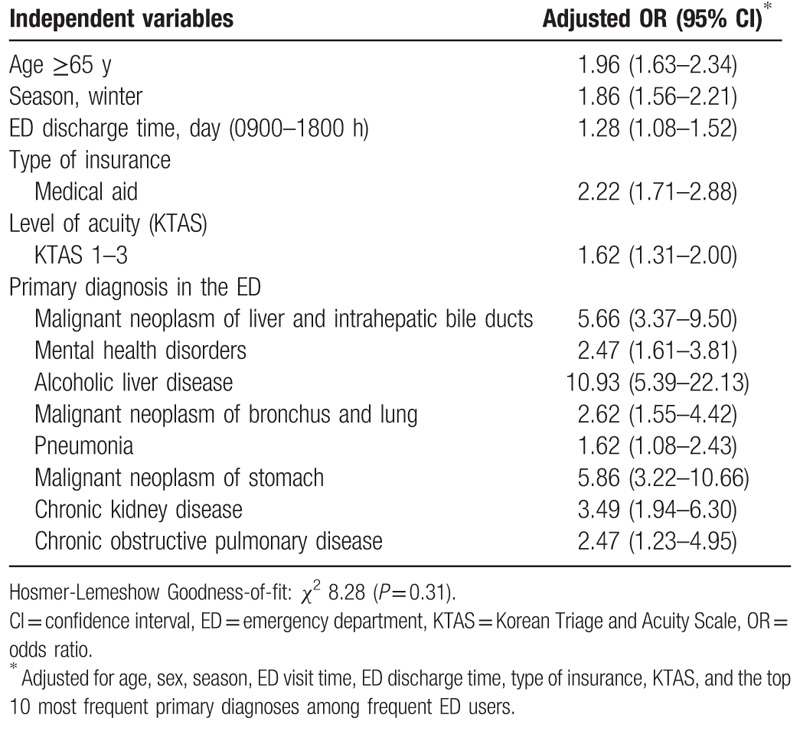
A multivariate logistic regression analysis was used to evaluate independent risk factors concerning frequent ED users (Table 3). Factors such as being >65 years’ old, being discharged from ED during the daytime, patients with medical aid insurance, and patients with KTAS 1 to 3 at the first visit were identified as independent risk factors among frequent ED users. Among the primary diagnoses at the first visit, malignant neoplasm, mental health disorders, alcohol-related liver disease, chronic kidney disease, and chronic obstructive pulmonary disease were significantly associated with visiting the ED more frequently.
Table 3.
Risk factors of ED frequent users.
4. Discussion
This retrospective study, conducted in 1 regional medical center, showed that frequent ED users accounted for 1.9% of all ED patients and 8.2% of total ED visits. Although frequent ED users comprised a small percentage of all ED users, they accounted for a significant proportion of ED visits. However, our results showed a smaller number of frequent ED users than that reported in previous studies.[8,9] This study was conducted at a single medical center and, as our research institute is a tertiary hospital, it may have been a barrier to frequent ED users. This situation may have resulted in an underestimation in terms of the number of frequent ED visits shown in our study.
Frequent ED users were more likely to be older, to have medical aid insurance coverage, and to have been discharged from the ED during the day. Frequent ED users tended to be more unwell than occasional ED users and were more likely to have a chronic illness or mental health disorder and be designated as high acuity at the first visit.
There was a trend for the number of ED visits to increase according to age, and patients aged ≥65 years were identified as more likely to attend the ED more frequently. Previous studies have reported mixed results concerning patient age; however, a systematic review that compared 5 different international health care systems showed that being >65 years’ old was an independent risk factor for ED frequent visits.[18] In total, >50% of frequent ED users in our study attended and were discharged from the ED during the day, which is consistent with findings from a previous study.[19]
In our study, patients with a high acuity level (KTAS 1–3) at the first visit were significantly associated with frequent ED visits. Although some patients attended the ED multiple times for low acuity complaints, most previous studies have reported that frequent users were often unwell due to chronic illnesses that are associated with higher hospital admission rates and greater mortality.[10,20] However, there has been marked heterogeneity reported in the predominant types of complaints of frequent ED users across regions.[18,21]
We found that exacerbations of chronic illnesses (eg, malignant neoplasms, alcohol-related liver disease, chronic kidney disease, and chronic obstructive pulmonary disease) and mental health issues were significant risk factors among frequent ED users. However, pediatric patients, unlike adults, show different characteristics and contributions to ED crowding. Although delay of admission is regarded as a major contribution to adult ED crowding, patient volume is recognized as a greater determinant of pediatric ED crowding.[22] Pediatric patients tended to visit the ED for low acuity complaints such as respiratory and gastrointestinal disorder, and fever, which were consistent with previous studies.[23,24] Because of these different characteristics, the intervention strategies should be distinct. Therefore, this study was intended to be limited to adult patients.
Most ED users had public insurance coverage; however, a high proportion of patients with medical aid coverage have been found to be among those who attend the ED more frequently.[6,8,25] These patients have been reported not only to have poor physical health, but also to have a low socioeconomic status (SES).[26] Because they appear to use the ED as an alternative to other sources of primary care, they are likely to use multiple medical resources, including the ED, to address their unmet healthcare needs.[21,27]
In this study, the winter season was identified as an independent risk factor for frequent ED visits. Among frequent ED users, 40.3% had visited the ED during the winter period. However, few studies have addressed seasonal variation in ED visits. One Australian study reported that frequent ED users were less likely to visit the ED during the summer due to warmer temperatures and fewer respiratory problems.[28] It is generally known that ED usage increases in winter.[29] Considering that most of the frequent ED users in our study had poor physical health and chronic illnesses, it can be surmised that they were not receiving appropriate medical care during the winter season.
The characteristics of frequent ED users are diverse, and previous studies have reported on the effectiveness of various strategies to reduce ED visits. One of the most commonly used strategies has involved the use of case management and individual care plans, which involve integrated care coordination of a multidisciplinary team between the hospital and the local community. This type of intervention is needed to specifically meet an individual's health needs and effectively reduce ED costs and decrease ED visits, particularly for vulnerable patient groups.[5,30] Addressing only 1 factor contributing to frequent ED visits was ineffective at reducing the number of ED visits; therefore, all strategies should be based on a systematic approach involving thorough preparation. Further research is needed to establish appropriate interventions and assess their effectiveness on ED use in regard to frequent adult users of the ED, and our research institute intends to engage in such research.
4.1. Limitations
This study had several limitations. First, it is a retrospective observational study. However, we tried to minimize systematic errors by using an ED-based database, which is under the authority of the Ministry of Health and Welfare in Korea and is used for quality control at the National Emergency Medical Center. And this study restricted the target population to adult patients in consideration of showing diverse clinical characteristics according to different age groups. Second, it was a single-center study and the research, in terms of ED utilization, was site-specific; therefore, it is difficult to generalize the results of our study to other regions. However, its findings are worthwhile to consider as a basis for strategies to reduce the burden on the ED through identifying the characteristics of community-based patients visiting the ED. Third, because of constraints in the ED-based database used in this study, we could not evaluate the association between frequent ED visits and SES-related variables such as income, education, and deprivation index.
5. Conclusions
Frequent ED users accounted for a significant proportion of total ED visits despite their small numbers. Frequent ED users were more likely to be older and have poor physical health status with chronic illness or mental health issues. With better understanding of the characteristics of frequent ED users, necessary multidisciplinary interventions to be designed are more likely to reduce repeated ED utilization and improve associated outcomes.
Acknowledgments
The authors thank all the staff members of the Emergency Medicine Department of Chungbuk National University Hospital for their assistance in collecting the data. We would like to thank Editage (www.editage.co.kr) for editing and reviewing this manuscript for English language.
Author contributions
Conceptualization: Lee JH, Park GJ. Methodology: Park GJ, Kim SC. Formal analysis: Lee JH, Park GJ. Investigation: Lee JH. Data curation: Park GJ, Kim H, Lee SW. Writing – original draft preparation: Lee JH, Park GJ. Writing – reviewing and editing: Park GJ, Kim SC, Kim H, Lee SW
Supplementary Material
Supplementary Material
Footnotes
Abbreviations: AOR = Adjusted odds ratio, CI = Confidence interval, ED = Emergency department, IQR = Interquartile range, KTAS = Korean Triage and Acuity Scale, NEDIS = National Emergency Department Information System, SES = Socioeconomic status.
How to cite this article: Lee JH, Park GJ, Kim SC, Kim H, Lee SW. Characteristics of frequent adult emergency department users: A Korean tertiary hospital observational study. Medicine. 2020;99:18(e20123).
The authors report no conflicts of interest.
This study was supported by a research grant from the Chungbuk National University Hospital in 2019.
Supplemental Digital Content is available for this article.
The data that support the findings of this study are available from a third party, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are available from the authors upon reasonable request and with permission of the third party.
References
- [1].Pines JM, Hilton JA, Weber EJ, et al. International perspectives on emergency department crowding. Acad Emerg Med 2011;18:1358–70. [DOI] [PubMed] [Google Scholar]
- [2].Berchet C. Emergency care services: trends, drivers and interventions to manage the demand, OECD Health Working Papers, No. 83. Paris, France: OECD Publishing; 2015. [Google Scholar]
- [3].Trzeciak S, Rivers EP. Emergency department overcrowding in the United States: an emerging threat to patient safety and public health. Emerg Med J 2003;20:402–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Hoot NR, Aronsky D. Systematic review of emergency department crowding: causes, effects, and solutions. Ann Emerg Med 2008;52:126–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Van den Heede K, Van de Voorde C. Interventions to reduce emergency department utilisation: a review of reviews. Health Policy 2016;120:1337–49. [DOI] [PubMed] [Google Scholar]
- [6].Hunt KA, Weber EJ, Showstack JA, et al. Characteristics of frequent users of emergency departments. Ann Emerg Med 2006;48:1–8. [DOI] [PubMed] [Google Scholar]
- [7].Bieler G, Paroz S, Faouzi M, et al. Social and medical vulnerability factors of emergency department frequent users in a universal health insurance system. Acad Emerg Med 2012;19:63–8. [DOI] [PubMed] [Google Scholar]
- [8].LaCalle E, Rabin E. Frequent users of emergency departments: the myths, the data, and the policy implications. Ann Emerg Med 2010;56:42–8. [DOI] [PubMed] [Google Scholar]
- [9].Woo JH, Grinspan Z, Shapiro J, et al. Frequent users of hospital emergency departments in Korea characterized by claims data from the National Health Insurance: a cross sectional study. PLoS One 2016;11:e0147450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Moe J, Kirkland S, Ospina MB, et al. Mortality, admission rates and outpatient use among frequent users of emergency departments: a systematic review. Emerg Med J 2016;33:230–6. [DOI] [PubMed] [Google Scholar]
- [11].Cook LJ, Knight S, Junkins EP, Jr, et al. Repeat patients to the emergency department in a statewide database. Acad Emerg Med 2004;11:256–63. [DOI] [PubMed] [Google Scholar]
- [12].Sun BC, Burstin HR, Brennan TA. Predictors and outcomes of frequent emergency department users. Acad Emerg Med 2003;10:320–8. [DOI] [PubMed] [Google Scholar]
- [13].Moe J, Kirkland SW, Rawe E, et al. Effectiveness of interventions to decrease emergency department visits by adult frequent users: a systematic review. Acad Emerg Med 2017;24:40–52. [DOI] [PubMed] [Google Scholar]
- [14].Ryu JH, Min MK, Lee DS, et al. Changes in relative importance of the 5-level triage system, Korean Triage and Acuity Scale, for the disposition of emergency patients induced by forced reduction in its level number: a multi-center registry-based retrospective cohort study. J Korean Med Sci 2019;34:e114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Park JB, Lee J, Kim YJ, et al. Reliability of Korean Triage and Acuity Scale: interrater agreement between two experienced nurses by real-time triage and analysis of influencing factors to disagreement of triage levels. J Korean Med Sci 2019;34:e189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16]. Statistics Korea. Korean Standard Classification of Diseases and Causes of Death (KCD-7) Daejeon: Statistics Korea; 2016. Available at: https://kssc.kostat.go.kr:8443/ksscNew_web/ekssc/main/main.do Updated 2016. Accessed August 10, 2019. [Google Scholar]
- [17].Chiu Y, Racine-Hemmings F, Dufour I, et al. Statistical tools used for analyses of frequent users of emergency department: a scoping review. BMJ Open 2019;9:e027750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Soril LJ, Leggett LE, Lorenzetti DL, et al. Characteristics of frequent users of the emergency department in the general adult population: a systematic review of international healthcare systems. Health Policy 2016;120:452–61. [DOI] [PubMed] [Google Scholar]
- [19].Slankamenac K, Zehnder M, Langner TO, et al. Recurrent emergency department users: two categories with different risk profiles. J Clin Med 2019;8:333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Salazar A, Bardes I, Juan A, et al. High mortality rates from medical problems of frequent emergency department users at a university hospital tertiary care centre. Eur J Emerg Med 2005;12:2–5. [DOI] [PubMed] [Google Scholar]
- [21].Krieg C, Hudon C, Chouinard MC, et al. Individual predictors of frequent emergency department use: a scoping review. BMC Health Serv Res 2016;16:594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Seguin J, Osmanlliu E, Zhang X, et al. Frequent users of the pediatric emergency department. CJEM 2018;20:401–8. [DOI] [PubMed] [Google Scholar]
- [23].Kim BS, Kim JY, Choi SH, et al. Understanding the characteristics of recurrent visits to the emergency department by paediatric patients: a retrospective observational study conducted at three tertiary hospitals in Korea. BMJ Open 2018;8:e018208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Neuman MI, Alpern ER, Hall M, et al. Characteristics of recurrent utilization in pediatric emergency departments. Pediatrics 2014;134:e1025–31. [DOI] [PubMed] [Google Scholar]
- [25].Zuckerman S, Shen Y-C. Characteristics of occasional and frequent emergency department users: do insurance coverage and access to care matter? Med Care 2004. 176–82. [DOI] [PubMed] [Google Scholar]
- [26].Lucas RH, Sanford SM. An analysis of frequent users of emergency care at an urban university hospital. Ann Emerg Med 1998;32:563–8. [DOI] [PubMed] [Google Scholar]
- [27].Giannouchos TV, Kum HC, Foster MJ, et al. Characteristics and predictors of adult frequent emergency department users in the United States: a systematic literature review. J Eval Clin Pract 2019;25:420–33. [DOI] [PubMed] [Google Scholar]
- [28].Kirby SE, Dennis SM, Jayasinghe UW, et al. Frequent emergency attenders: is there a better way? Aust Health Rev 2011;35:462–7. [DOI] [PubMed] [Google Scholar]
- [29]. Care Quality Commission. Under pressure: safely managing increased demand in emergency departments. May 2018. Available at: https://www.cqc.org.uk/sites/default/files/20180716_underpressure-winterpressures.pdf Updated 2018. Accessed August 15, 2019. [Google Scholar]
- [30].Althaus F, Paroz S, Hugli O, et al. Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Ann Emerg Med 2011;58:41–52. e42. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.