

Abstract
In recent years, women and girls are increasing their sport participation, and female sports are becoming more challenging. While more women and girls are participating in sports, there is still a lack of information about gender-specific lesions. We will therefore evaluate gender differences in sports injuries, analyzing the five sports and sporting activities that are most widespread in the western world: running, soccer, basketball, water sports, and winter sports. The ability to make correct ultrasonographic diagnoses in sports injuries is improving as the technology is advancing. Ultrasonography demonstrates tissue structure with two-dimensional grayscale images, while blood flow can be visualized with color and power Doppler. Furthermore, ultrasonography is the preferred imaging modality for studying soft-tissue lesions dynamically. High-quality diagnostic ultrasound cannot be performed without the knowledge of the underlying clinical background, and an understanding of gender-specific injuries and mechanisms of injuries is therefore important for assessing proper diagnostic and treatment guidelines tailored to phenotypic differences in professional and amateur athletes between male and female.
Keywords: Sports injuries, Musculoskeletal ultrasound, Gender differences
Introduction
In recent years, women and girls are increasing their sport participation, sports fans are becoming more interested in women’s sports, and female sports are becoming more challenging [1, 2]. While more women and girls are participating in sports than ever before and sports fans are becoming more interested in women’s sports, there is still a lack of information about gender-specific lesions and patterns of injuries in athletes, which have for a long time been assumed to be more sport specific than gender specific [3]. In the past, most of the literature on women’s sports lesions focused on gymnastic injuries since gymnastics was generally regarded as a “female sport.” Nowadays, this kind of differentiation is no longer valid as women frequently perform “men’s sports” (such as soccer or rugby). This de-differentiation in sports gender has created the urgency for new studies and reviews on the gender differences in all sports.
In the past, male athletes have been reported to have a higher risk of severe sports-related injuries than female athletes [4, 5]. We should therefore consider whether women are better at dealing with pain. Eighty percent of women get period pain at some point in their lives, and therefore a large majority of women have developed strong coping mechanisms to deal with this regular pain, so the short-term pain they feel when running a race will fade in comparison [6]. Therefore, when discussing gender differences in sports lesions, it is crucial to analyze the different lesions in relation to the specific sporting activity and to focus on “minor injuries” and “overuse lesions” [7]. A more in-depth analysis will be carried out on injury mechanisms and imaging modalities, with a special focus on ultrasound and its field of application.
We will therefore evaluate gender differences in sports injuries, analyzing the five sports and sporting activities that are most widespread in the western world: running, soccer, basketball, water sports, and winter sports.
Running
Unsurprisingly and in agreement with previous reviews on the topic, the majority (> 70%) of running injuries occur at or below the knee (Figs. 1, 2). This is true for both men and women [8] in the top 10 running injuries, identifiable by specific pathology, supporting this finding.
Fig. 1.

Patellar tendinopathy. The sagittal B-mode ultrasound panoramic image shows an enlarged tendon with loss of echogenicity (arrows)
Fig. 2.

Jumper’s knee. The echo color Doppler image shows hypoechogenicity, with a heterogeneous structure (arrows) (a) and diffuse hyperemia of the deep insertional part of the patellar tendon (arrows) (b)
However, although the most commonly injured sites in men and women are the same, the proportions for each site differ. The main difference is that women have a larger proportion of knee injuries (40% of all injuries) relative to men, who experience a similar proportion of knee (31%) and ankle–foot (26%) injuries. The third highest proportion of injury was at the shank (16%). These data indicate that 70% of all reported injuries were at or below the knee. The hip and thigh regions accounted for 14% of injuries. The remaining injuries (other, 15%) were of unclear location, occurred in the upper extremities, or resulted from illness [9].
The two most common running injuries are patellofemoral pain syndrome (PFPS) and Achilles tendinopathy (AT) (Fig. 3) [10], which is in agreement with the majority of reports on the prevalence of musculoskeletal injury in runners [11].
Fig. 3.
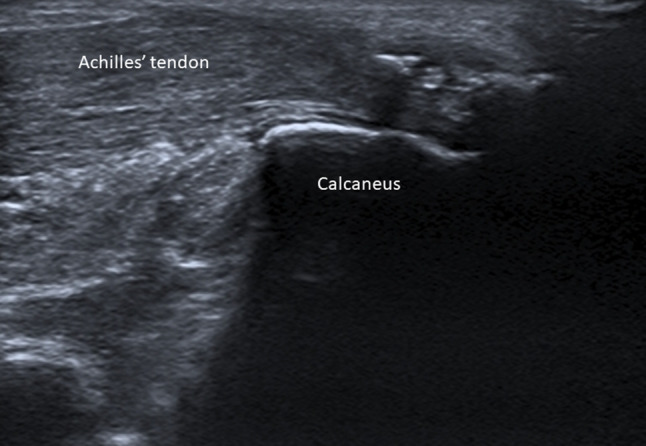
Achilles tendon tendinopathy. Sonography shows a larger and wider Achilles tendon, with calcifications and loss of normal echogenicity
The proportion of PFPS is far in excess of AT in females and may reflect a gender bias due to women having more knee injuries. Similarly, men have a greater proportion of ankle–foot injuries relative to women, which may indicate that the proportion of AT injuries, as well as plantar fascitis (Fig. 4) [12], is male biased [13]. In marathon runners, males have a greater risk of hamstring and calf (Fig. 5) injuries than females [14].
Fig. 4.

Plantar fasciitis. The B-mode ultrasound image shows plantar fascia hypoechoic with loss of fibrillar pattern (caliper)
Fig. 5.

Tears to the medial head of the gastrocnemius (tennis leg). The longitudinal sonogram shows hematoma with thin walls interposed between the gastrocnemius and the aponeurosis
This finding is particularly interesting since sprains and strains of the ankle, as well as ligament and stress fractures, are more frequent in women and female patients, with fractures occurring at an average age below the overall mean [15].
The proportion of specific pathologies will also be influenced by the variability in time to recover from different running injuries and the likelihood of reoccurrence, as well as the fact that females seem more predisposed to injuries sustained in long-distance running [16]. In extreme situations, sports-related rhabdomyolysis is a rare but severe potential complication in extreme running [17].
Ultrasound allows detection and localization of the lesions, helps clarify the stage and severity of the injuries, and aids clinicians to tailor management plans. Two-dimensional grayscale, color, and power Doppler provide high-resolution imaging of superficial muscles, tendons, ligaments, and other important structures in running-related injuries. A panoramic view yields a wider vision of the whole lesion. Dynamic sonographic examination demonstrates the interactions between the injured tissue and the surrounding structures. Ultrasound-guided aspiration of the hematoma in the injured soft tissue can be performed. Therefore, ultrasound is the gold standard imaging modality in runners’ injuries.
Soccer
Football (soccer) is the most popular sport worldwide and is associated with a high injury risk, according to data of the United States National Collegiate Athletic Association (NCAA).
Engaging hundreds of millions of participants each year in a physically demanding contact sport, soccer causes injuries ranging from common and benign low-grade muscle strains to potentially career-ending ligamentous injuries.
The overall injury rate in NCAA women’s soccer is 7.3 per 1000 athlete exposures (games and practices combined), and soccer players are nearly three times more likely to be injured in a game (14.4 injuries per 1000 athlete exposures) than in practice (5.0 injuries per 1000 athlete exposures). Ligament sprains (25.7%) (Figs. 6, 7), followed by muscle strains (21.5%) (Fig. 8), contusions (15.9%), and concussions (9.2%), are the most common types of injuries.
Fig. 6.
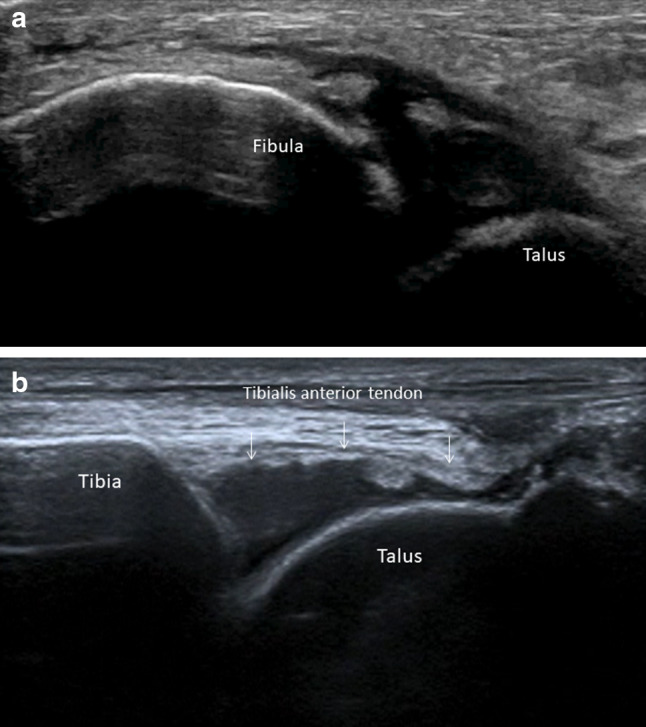
Ankle acute sprain. Sonography shows a complete tear of the anterior talofibular ligament, with absence of the ligament, allowing the effusion to reach the subcutaneous tissue (a), and joint effusion (arrows) (b)
Fig. 7.
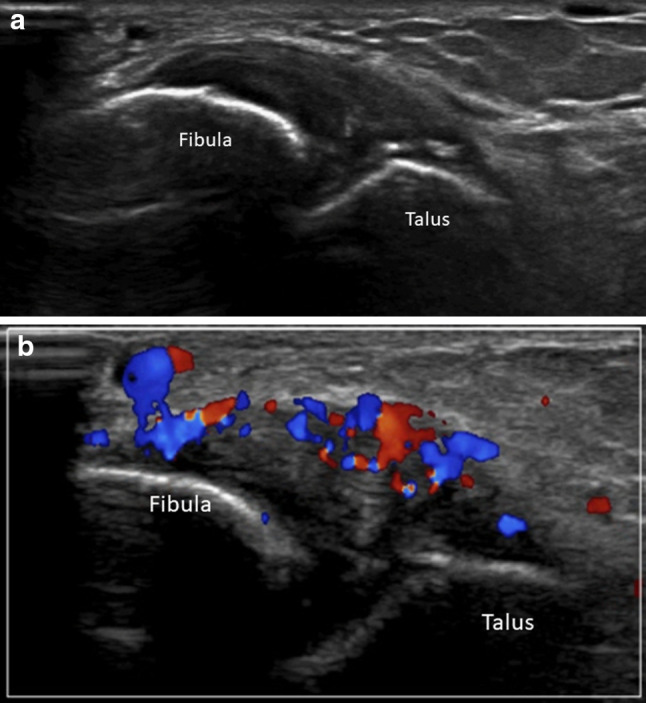
Ankle chronic sprain. Sonography shows an anterior talofibular ligament that is swollen, hypoechoic (a), and hyperemic upon color Doppler examination (b)
Fig. 8.

Rectus femoris myoaponeurotic lesion. The longitudinal (a) and axial (b) images show the central lamina surrounded by hematoma (caliper). Color Doppler shows no vascularization within the lesion (c)
Ligament sprains of the lateral ankle (12.8%), concussions (9.2%), quadriceps (thigh) muscle strains (7.0%) [18], and hamstring muscle strains (4.8%) are the most common specific types of injury in women’s soccer [19].
There are many kinds of kicking, but a kick can always be broken down into six basic phases: approach, foot plant, swing-limb loading, hip flexion and knee extension, ball contact, and follow-through. The hamstring musculature is particularly prone to injury especially when sprinting and limb loading.
The knee joint is often affected, and lesions of the anterior cruciate ligament are the most important and severe injuries. Several studies have found female players to be more susceptible to knee injury, anterior cruciate ligament (ACL) injury in particular, compared to their male counterparts. Female players have a two to three times higher ACL injury risk compared to males. Females also tend to sustain their ACL injury at a younger age than males [20].
The reason why ACL injuries are more frequent in female athletes, in soccer but also in other sports, is probably due to biomechanical behavior, with females having a more than five times higher relative risk of valgus collapse at the end of the jump [21].
Magnetic resonance (MR) remains the primary diagnostic imaging tool for severe knee lesions. Ultrasound obviously proves to be very useful for a wide range of lesions affecting muscles, tendons, and ligaments [22].
Swimming and water sports
There is a global consensus that swimming is the most secure way of training the whole body with minimal risk of injuries, much lower than that in other sports. It is generally true, but we must not forget that minimizing is not the same as erasing any possible risks.
Not many studies exist on the incidence of swimming injuries, and only a minority of studies evaluate gender influence. Independently from their gender, swimmers most commonly present clinically with pain at the shoulder, back, and knee.
The few studies available show that swimming has a statistically significant gender difference in the pattern of injury. More specifically, female swimmers had more back/neck, shoulder, hip, knee, and foot injuries than their male counterparts [23].
The shoulders are frequently injured in competitive swimming. The incidence of shoulder pain is related to the level of competition and is by far the most frequent chronic injury in swimmers. It is a musculoskeletal condition that results in symptoms in the area of the anterior lateral aspect of the shoulder. Generally, the symptoms are confined to the subacromial region and are due to overuse, with pathologies of the rotator cuff and long head of the biceps and subcoracoid or subacromial-subdeltoid bursitis [24], which are best evaluated by ultrasound [25] (Fig. 9).
Fig. 9.
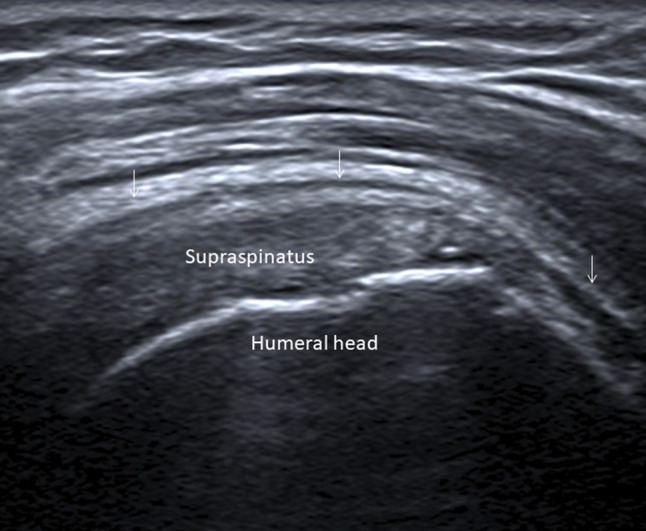
Subacromial bursitis and rotator cuff tendinopathy in a young male elite swimmer with a painful right shoulder (arrows)
Basketball
Basketball has evolved over time from a generally noncontact sport to a sport with greater body contact, thus leading, in all age groups and both genders, to an increase in injury frequency. Injuries can be both acute and chronic. Injuries in basketball evolved from a relatively high prevalence of chronic lesions in the past to a higher percentage of acute lesions now, due to both a better training pattern (lowering the rate of chronic overuse lesions) and greater body contact (increasing the rate of acute lesions).
The most common injury site is the ankle, followed by the knee, lower back, and upper extremities. There are no relevant gender differences in ankle lesions, while gender differences are rather important in knee injuries.
In an interesting retrospective study from the Institute for Integrated Sports Medicine of Keio University in Tokyo, Japan, there was a higher proportion of female players presenting with a knee injury, compared with male players (50.4% vs. 41.7%), and a lower proportion of female players presenting with an upper extremity injury (5.1% vs. 9.7%). The proportion of anterior cruciate ligament injury in the 10–19-year-old age group was higher among female players than among male players (45.9% vs. 22.1%). Conversely, the proportions of Osgood–Schlatter disease in the 10–19-year-old age group and jumper’s knee (patellar and femoral tendinopathy) in the 20–29-year-old age group were higher among male players than among female players (12.5% vs. 1.8% and 14.6% vs. 3.7%, respectively). However, the proportions of other injuries did not differ significantly between male and female players, which is surprising since many would assume that ligament lesions of the ankle would be more frequent in female athletes [26].
As in soccer, there is a higher proportion of female than male basketball players presenting with ACL injury, and therefore MR is obviously the primary imaging modality for assessing major knee trauma. Interestingly, there is a higher proportion of male than female basketball players presenting with Osgood–Schlatter disease and jumper’s knee, both of which can be well assessed by ultrasound.
Winter sports
The development of winter sports has resulted in improvements in materials and responses to stresses. Technology has provided lightweight and increasingly ergonomic equipment that enhances performance and attempts to improve safety. These technological developments have led to changes in the injury patterns associated with winter sports.
To understand common contemporary injuries, we must remember the differences between the two most common groups of winter sports. Alpine skiing and snowboarding can be grouped together since they are based on power performance with the heels blocked on the boots, while Telemark skiing (which permits turning with a free-heel lift) and Nordic (cross-country/endurance) skiing have completely different patterns of activation and thus of injury.
Alpine skiing and snowboarding
Injury rates in skiers and snowboarders are at a very high level relative to the hours spent sporting. Injury rates in skiers and snowboarders fluctuated over time but currently remain higher in snowboarders than in skiers. Wrist, shoulder, and ankle injuries are more common among snowboarders, while knee ligament injuries are surprisingly more common in skiers.
Injured snowboarders were significantly younger, less experienced, and more likely to be female than injured skiers or male snowboarders [27].
Stener lesion of the ulnar collateral ligament of the thumb [28] obviously occurs far more often in skiers (Fig. 10). Interestingly, there exist statistically significant confounder-corrected correlations between sex and rupture site, as well as between trauma intensity and rupture site: Mid-substance tears occur more frequently in women, whereas men tend to suffer from distal ligament or bony avulsions. Compared to women, men suffer more frequently from distal ligament or bony avulsions. The higher the velocity involved in the trauma mechanism, the more probable it is that the tear will occur distally, but velocity alone seems not to be sufficient to explain the difference: There seems to be some sex-specific variable that, by itself, has some meaningful influence on rupture site [29].
Fig. 10.

Stener lesion. Full-thickness tear of the ulnar collateral ligament of the metacarpophalangeal joint of the thumb with retraction of the proximal stump. The adductor aponeurosis (arrows) is interposed between the ruptured ulnar collateral ligaments
Cross-country skiing
Cross-country skiing is one of the sports in which gender differences were studied first [30]. Cross-country skiing is an endurance sport requiring a range of skiing techniques to cover various types of terrain efficiently, although cross-country skiers have the lowest rates of injury relative to other endurance sports (long-distance running, swimming, cycling, orienteering) and winter Olympic athletes [31]. There are two distinct cross-country ski styles, skating and classic, each with subtechniques, making it difficult to do an exact statistical analysis of the lesion in relation to the trauma mechanism [32]. The main difference between genders seems to be a greater number of overuse injuries in the posterior thigh in male than in female athletes, whereas females have a greater risk of overuse injuries to the ankle [33]. Since muscle strain is the single most frequent lesion type in cross-country skiers, ultrasound proves to be of great value in the diagnosis and follow-up of injured athletes of both genders.
Conclusions
The ability to make correct ultrasonographic diagnoses in sports injuries is improving as advancing technology allows for high-resolution images in contemporary medical ultrasound. Ultrasonography demonstrates tissue structure with two-dimensional grayscale images. Blood flow in the tissue can be rapidly depicted with color and power Doppler techniques. Furthermore, ultrasonography is the preferred imaging modality for studying soft-tissue lesions dynamically [34, 35]. With high-resolution images afforded by ultrasonography, injuries of the muscle, tendon, ligament, bursa, bony structure, cartilage, and subcutaneous tissue can be accurately diagnosed.
High-quality diagnostic ultrasound cannot be performed without knowledge of the underlying clinical background, and an understanding of gender-specific injuries and mechanisms of injuries is therefore important for assessing proper diagnostic and treatment guidelines tailored to phenotypic differences in professional and amateur athletes between male and female.
Compliance with ethical standards
Conflict of interest
CB is consultant for Bracco Imaging Italia and Doc Congress. The other authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Bibel S (2012) NCAA women’s basketball overnight rating up over last year. https://tvbythenumbers.zap2it.com/2012/04/04/ncaa-womens-basketballovernight-rating-up-over-last-year/127494/. Accessed 28 Dec 2017
- 2.Antil JH, Burton E, Robinson M. Exploring the challenges facing female athletes as endorsers. J Brand Strat. 2012;1:292–307. [Google Scholar]
- 3.Aaltonen S, Karjalainen H, Heinonen A, Parkkari J, Kujala UM. Prevention of sports injuries: systematic review of randomized controlled trials. Arch Intern Med. 2007;167:1585–1592. doi: 10.1001/archinte.167.15.1585. [DOI] [PubMed] [Google Scholar]
- 4.Conn JM, Annest JL, Gilchrist J. Sports and recreation related injury episodes in the US population, 1997–99. Inj Prevent. 2003;9:117–123. doi: 10.1136/ip.9.2.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dempsey RL, Layde PM, Laud PW, Guse CE, Hargarten SW. Incidence of sports and recreation related injuries resulting in hospitalization in Wisconsin in 2000. Inj Prevent. 2005;11:91–96. doi: 10.1136/ip.2004.006205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Perry J. Performing under pressure. NY: Routledge; 2020. [Google Scholar]
- 7.Post EG, Biese KM, Schaefer DA. Sports specific associations and specialization and sex with overuse injury in young athletes sports. Health. 2019;12:36–42. doi: 10.1177/1941738119886855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Francis P, Whatman C, Johnson MJ. The proportion of lower limb running injuries by gender, anatomical location and specific pathology. Sports Sci Med. 2019;18:21–31. [PMC free article] [PubMed] [Google Scholar]
- 9.Kluitenberg B, van Middelkoop M, Diercks R, van der Worp H. What are the differences in injury proportions between different populations of runners? A systematic review and meta-analysis. Sports Med. 2015;45:1143–1161. doi: 10.1007/s40279-015-0331-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Draghi F, Cocco G, Lomoro P, Bortolotto C, Schiavone C. Non-rotator cuff calcific tendinopathy: ultrasonographic diagnosis and treatment. J Ultrasound. 2019 doi: 10.1007/s40477-019-00393-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lopes AD, Hespanhol Junior LC, Yeung SS, Costa LO. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012;42:891–905. doi: 10.1007/BF03262301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Draghi F, Gitto S, Bortolotto C, Draghi AG, Ori BG. Imaging of plantar fascia disorders: findings on plain radiography, ultrasound and magnetic resonance imaging. Insights Imaging. 2017;8:69–78. doi: 10.1007/s13244-016-0533-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nielsen RO, Ronnow L, Rasmussen S, Lind M. A prospective study on time to recovery in 254 injured novice runners. PLoS One. 2014;9:e99877. doi: 10.1371/journal.pone.0099877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Satterthwaite P, Norton R, Larmer P, Robinson E. Risk factors for injuries and other health problems sustained in a marathon. Br J Sports Med. 1999;33:22–26. doi: 10.1136/bjsm.33.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Powell JW, Barber-Foss KD. Sex-related injury patterns among selected high school sports. Am J Sports Med. 2000;28:385–391. doi: 10.1177/03635465000280031801. [DOI] [PubMed] [Google Scholar]
- 16.Zingg MA, Rüst CA, Rosemann T, Lepers R, Knechtle B. Runners in their forties dominate ultra-marathons from 50 to 3100 miles. Clinics (Sao Paulo) 2014;69:203–211. doi: 10.6061/clinics/2014(03)11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Clarkson PM. Exertional rhabdomyolysis and acute renal failure in marathon runners. Sports Med. 2007;37:361–363. doi: 10.2165/00007256-200737040-00022. [DOI] [PubMed] [Google Scholar]
- 18.Draghi F, Draghi AG, Gitto S. Myotendinous strains of the vastus lateralis as a result of sport-related trauma. J Sports Med Phys Fit. 2018;58:947–949. doi: 10.23736/S0022-4707.17.07304-2. [DOI] [PubMed] [Google Scholar]
- 19.www.stopsportsinjuries.org. Accessed 26 Jan 2020
- 20.Arendt EA, Agel J, Randall D. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34:86–92. [PMC free article] [PubMed] [Google Scholar]
- 21.Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–367. doi: 10.1177/0363546506293899. [DOI] [PubMed] [Google Scholar]
- 22.Depaoli R, Canepari E, Bortolotto C, Ferrozzi G. Morel-Lavallée lesion of the knee in a soccer player. J Ultrasound. 2015;18:87–89. doi: 10.1007/s40477-015-0157-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shapiro C. Swimming. In: Shamus E, Shamus J, editors. Sports injury prevention and rehabilitation. New York: McGraw-Hill; 2001. pp. 103–154. [Google Scholar]
- 24.Draghi F, Scudeller L, Draghi AG, Bortolotto C. Prevalence of subacromial-subdeltoid bursitis in shoulder pain: an ultrasonographic study. J Ultrasound. 2015;18:151–158. doi: 10.1007/s40477-015-0167-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kennedy JC, Hawkins RJ. Swimmer's shoulder. Phys Sportsmed. 1974;2:34–38. [Google Scholar]
- 26.Iro E, Iwamoto J, Matsumoto H. Sex-specific differences in injury types among basketball players. Open Access J Sports Med. 2015 doi: 10.2147/OAJSM.S73625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kim S, Endres NK, Ettinger CF, Shealy JE. Snowboarding injuries: trends over time and comparisons with alpine skiing injuries. Am J Sports Med. 2012;40:770–776. doi: 10.1177/0363546511433279. [DOI] [PubMed] [Google Scholar]
- 28.Draghi F, Gitto S, Bianchi S. Injuries to the collateral ligaments of the metacarpophalangeal and interphalangeal joints: sonographic appearance. J Ultrasound Med. 2018;37(9):2117–2133. doi: 10.1002/jum.14575. [DOI] [PubMed] [Google Scholar]
- 29.Boesmüller S, Huf W, Vierhapper M. The influence of sex and trauma impact on the rupture site of the ulnar collateral ligament of the thumb. PLoS One. 2017;12:e0181754. doi: 10.1371/journal.pone.0181754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sandelin J, Kiviluoto O, Santavirta S. Injuries of competitive skiers in Finland: a three-year survey. Annales Chirurgiae et Gynaecologiae. 1980;69:97–101. [PubMed] [Google Scholar]
- 31.Clarsen B, Bahr R, Heymans MW, et al. The prevalence and impact of overuse injuries in five norwegian sports: application of a new surveillance method. Scand J Med Sci Sport. 2014;25:323–330. doi: 10.1111/sms.12223. [DOI] [PubMed] [Google Scholar]
- 32.Marsland F, Lyons K, Anson J, Waddington G, Macintosh C, Chapman D. Identification of cross-country skiing movement patterns using micro-sensors. Sensors. 2012;12:5047–5066. doi: 10.3390/s120405047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ristolainen L, Heinonen A, Kettunen J. Gender differences in sports injuries a retrospective study on cross country skiers. J Sports Sci Med. 2009;8:443–451. [PMC free article] [PubMed] [Google Scholar]
- 34.Draghi F, Bortolotto C, Draghi AG, Gitto S. Intrasheath instability of the peroneal tendons: dynamic ultrasound imaging. J Ultrasound Med. 2018;37:2753–2758. doi: 10.1002/jum.14633. [DOI] [PubMed] [Google Scholar]
- 35.Draghi F, Gregoli B, Bortolotto C. Absence of elevation of fibular tendons during dorsal hyperflexion of the foot: a sign of loss of the calcaneofibular ligament. J Ultrasound Med. 2014;33:1307–1308. doi: 10.7863/ultra.33.7.1307. [DOI] [PubMed] [Google Scholar]