

Abstract
Carpal tunnel syndrome (CTS) represents the most common entrapment neuropathy of the upper extremity. Intermittent CTS has been reported in the surgical literature and usually, related to masses associated to flexor tendons. We describe a patient with an intrasynovial lipoma involving the deep flexor of the middle finger causing intermittent CTS and snapping on flexion–extension.
Keywords: Intrasynovial, Lipoma
Sommario
La sindrome del tunnel carpale (CTS) rappresenta la neuropatia da intrappolamento più comune dell’arto superiore. La CTS intermittente è stata riportata nella letteratura chirurgica e, di solito, in relazione alle masse associate ai tendini flessori. Descriviamo un paziente con un lipoma intrasinoviale che coinvolge il flessore profondo del dito medio che causa CTS intermittente e che si spezza sull’estensione della flessione.
Introduction
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy affecting between 2.7 and 5.8% of the population, more often females (3–1), and particularly frequent after the 5th decade [1.] It is characterised by pain, paraesthesia and numbness in the territory of innervation of the median nerve (1st to 3rd fingers and the radial aspect of the 4th finger). CTS may result from a wide variety of causes including repetitive traumatic stress, hormonal and metabolic changes, masses (ganglion cysts, tumours, accessory muscles) [2].
Case report
A 26-year-old man right-handed manual labourer presenting intermittent pain in his dominant wrist. There was no history of trauma and past medical history was unremarkable.
On clinical examination, intermittent paraesthesia along median nerve distribution and snapping of the wrist on movement (flexion and extension) of the middle finger. Imaging assessment of the wrist was requested to characterise the source of patient’s symptoms.
On MRI, the carpal tunnel was unremarkable with normal course and morphology of the median nerve. Distal to the carpal tunnel, at the level of the 3rd metacarpal, an intrasynovial lesion likely lipomatous was noted related to the tendon of the deep flexor of the middle finger, oedema of the surrounding soft tissues was also present (Fig. 1). Normal appearance of the flexor tendons and of the adipose tissue in the carpal tunnel, no evidence of ulnar nor radial bursitis.
Fig. 1.
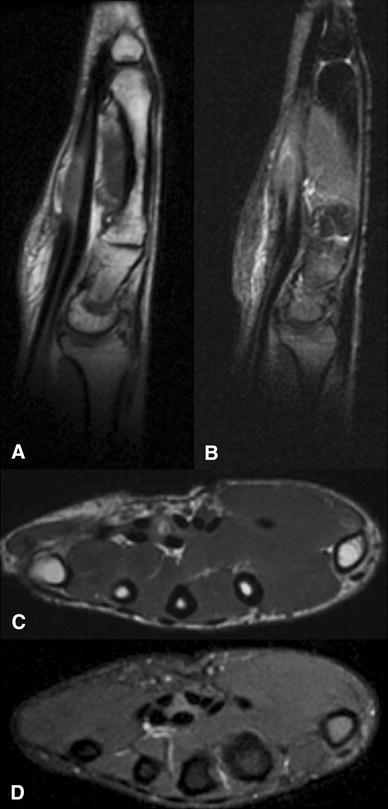
MRI sagittal PD (a) and PDFS (b) and axial T1(c) and PDFS (d) showing the lipomatous lesion closely related to the deep flexor of the middle finger tendon just distal to the carpal tunnel
Correlation with dynamic ultrasound was performed. Flexion of the middle finger with consequent snapping of the wrist was exacerbating neuropathic pain in the hand and wrist area, prompt resolution of the symptoms was observed with finger extension. The ultrasonographic features were characterised by sliding of the synovial lipoma underneath the flexor retinaculum into the carpal tunnel during middle finger flexion (Figs. 2, 3). The CTS was secondary to intermittent increased pressure in the carpal tunnel.
Fig. 2.
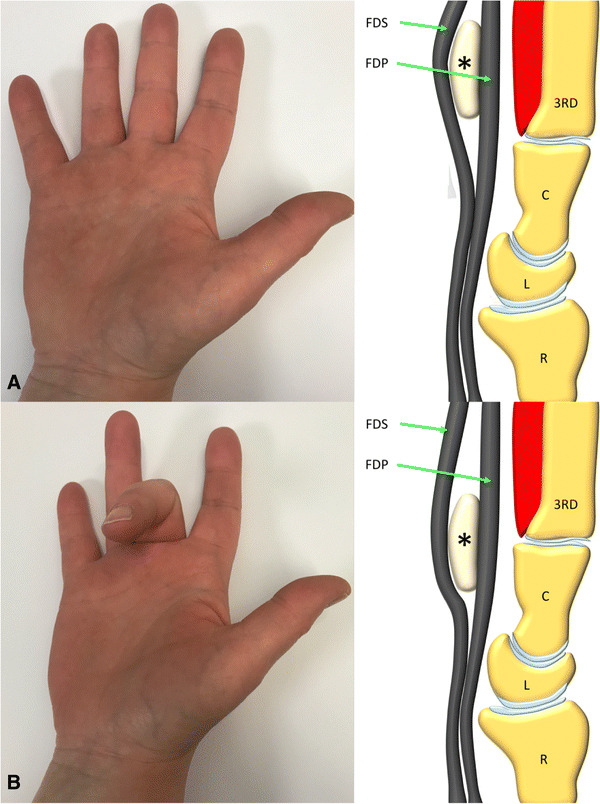
Diagrammatic representation showing movement to the lipoma (*) between the flexor tendons on flexion and extension of the middle finger. FDS (flexor digitorum superficialis), FDP flexor digitorum profundus, C capitate, L lunate, R radius
Fig. 3.
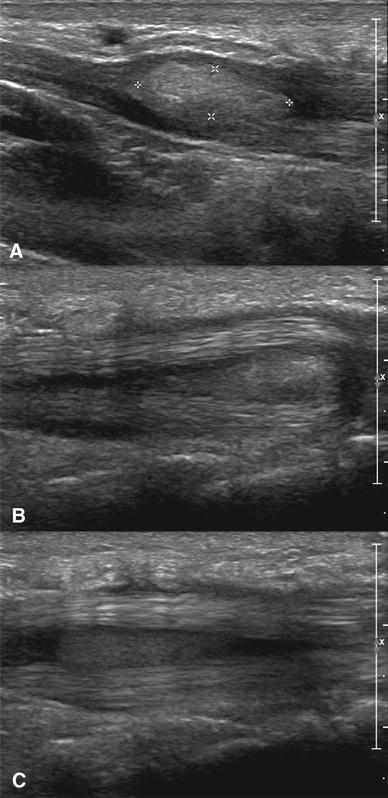
Longitudinal ultrasound images a–c showing movement to the lipoma between the flexor tendons on flexion and extension of the middle finger
Subsequently, surgical treatment was planned and the lipomatous tumour was removed. Histology was consistent with a benign intrasynovial spindle cell lipoma (Fig. 4). At the postoperative clinical examination, complete resolution of patient’s symptoms with complete functional recovery was noticed.
Fig. 4.
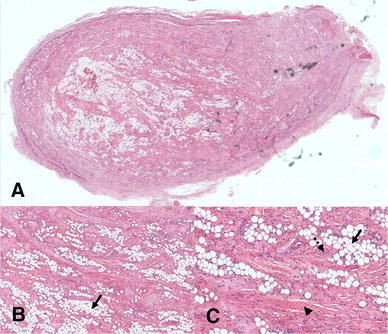
At low magnification the tumour is well circumscribed and contains fat and spindle cells in a collagenised stroma. a Higher magnification shows the tumour to be composed of an mixture of mature adipocytes(arrow) and spindle cells (arrow head) embedded in a stroma that contains wavy collagen fibres
Discussion
Several different causes of CTS have been described both in the orthopaedic in the radiological literature. The electrophysiological analysis represents the gold standard, and nerve conduction alterations in combination with the clinical findings are diagnostic, consequently prompt surgical release is performed to prevent the effects of chronic denervation [2].
On MRI, the carpal tunnel is better evaluated on the axial plane. Two features are suggestive for CTS: in particular the enlargement of the median nerve in the proximal carpal tunnel at the level of the pisiform and flattening of the nerve at the level of the hamate (distal carpal tunnel) with bowing of the flexor retinaculum these findings might be associated with intrasubstance changes in the nerve. Sensitivity and specificity of these criteria are low, and the main role of MRI is in detecting masses (ganglion cysts, tumours, accessory muscles, anatomical variants of the median nerve, bony deformities) and traumatic/osteoarthritic-related changes [3, 4].
Ultrasound (US) examination is a simple, cheap, non-invasive imaging technique for wrist disorders. US diagnostic criteria for CTS are basically two, morphologic (by loss of the normal honeycomb pattern with uniform hypo echogenicity of the nerve) and dimensional (cross-sectional area). However, morphologic changes cannot predict the residual function of the nerve and cross-sectional area depends more on the patient’s characteristics than on the nerve entrapment [5].
Therefore, dynamic ultrasound (DUS) criteria based on the assumption that the median nerve has a transverse sliding, this is radial to ulnar with fingers flexion and ulnar to radial with extension.
A limitation of this movement is associated with CTS, and also the degree of limitation is directly related to the severity of the nerve conduction impairment [6].
Trigger wrist/intermittent CTS is a rare entity and has been described in the literature mostly from a clinical/surgical point of view [4, 7–12]. In fact, static imaging has a marginal role and often no alterations of electrophysiology are detected. However, in presence of an intermittent CTS triggered by finger flexion symptoms are less definite, electrophysiology shows normal conduction of the nerve throughout the carpal tunnel and static imaging (MRI) shows a normal carpal tunnel with preserved innervation of distal muscles. MRI is useful to assess the presence of masses within and/or around (especially distal) the carpal tunnel.
Ultrasound although dependent on radiologist’s experience has an important role in the diagnostic assessment of this entity. Dynamic examination of flexor tendons as well as of the carpal tunnel can be performed. If an intrasynovial mass is detected, examination of every single superficial and deep tendon can be performed respectively with passive flexion of the intermediate and distal phalanx. Mobility of the medial nerve should be assessed.
In presence of symptoms involving the median nerve distribution US dynamic assessment should always be performed anytime and MRI is requested. This will improve the diagnostic accuracy in order to increase the reliability of imaging in CTS.
Elastography is being widely used with great potential in breast, thyroid, liver, musculoskeletal, prostate and gastrointestinal systems [13–16]. Cantisani et al. had shown that contrast enhanced ultrasound and elastography are effective tools for evaluation of nature of thyroid nodules with increased specificity [16]. The fibrotic component of a lesion can be assessed using acoustic structure quantification software on ultrasound which had shown promising results in patients with liver cirrhosis and fibrosis [15]. Contrast enhanced ultrasound in comparison to ultrasound helps to decipher additional information about the content of a soft tissue mass enabling one to more accurate target for biopsy [17.]
Disclosures
No financial disclosures.
Funding
No funding to declare.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Approval by an ethics committee was not applicable in this case report.
Informed consent
For this type of study formal consent is not required.
References
- 1.Hobby J (2008) Focus on Carpal tunnel syndrome. J Bone Jt Surg 1–2. 10.1302/0301-620X.90B6.21534
- 2.Dong Q, Jacobson JA, Jamadar DA, Gandikota G, Brandon C, Morag Y, et al (2012) Entrapment Neuropathies in the upper and lower limbs: anatomy and MRI features. Radiol Res Pract [Internet], pp 1–12. http://www.hindawi.com/journals/rrp/2012/230679/ [DOI] [PMC free article] [PubMed]
- 3.Jarvik JG, Yuen E, Haynor DR, Bradley CM, Fulton-Kehoe D, Smith-Weller T, et al (2002) MR nerve imaging in a prospective cohort of patients with suspected carpal tunnel syndrome. Neurology [Internet]. 58(11):1597–1602. http://www.neurology.org/content/58/11/1597.abstract [DOI] [PubMed]
- 4.Kernohan JG, Benjamin A, Simpson D (1982) Trigger wrist due to anomalous flexor digitorum profundus muscle in association with fibroma of tendon sheath. Hand 14(1):59–60 [DOI] [PubMed]
- 5.Fowler JR, Gaughan JP, Ilyas AM. The sensitivity and specificity of ultrasound for the diagnosis of carpal tunnel syndrome: a meta-analysis. Clin Orthop Relat Res. 2011;469(4):1089–1094. doi: 10.1007/s11999-010-1637-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kuo TT, Lee MR, Liao YY, Chen JP, Hsu YW, Yeh CK. Assessment of median nerve mobility by ultrasound dynamic imaging for diagnosing carpal tunnel syndrome. PLoS ONE. 2016;11(1):1–16. doi: 10.1371/journal.pone.0147051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harris WR (1961) Trigger wrist with intermittent carpal tunnel syndrome. Can Med Assoc J [Internet]. 84(17):963. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1939529/ [PMC free article] [PubMed]
- 8.Brown LP, Coulson DB. Triggering at the carpal tunnel with incipient carpal-tunnel syndrome. Report of an unusual case. J Bone Jt Surgery. 1974;56(3):623–624. doi: 10.2106/00004623-197456030-00022. [DOI] [PubMed] [Google Scholar]
- 9.Iqbal QM. Triggering of the finger at the flexor retinaculum. Hand. 1982;14(1):53–55. doi: 10.1016/S0072-968X(82)80041-7. [DOI] [PubMed] [Google Scholar]
- 10.Imai S, Kodama N, Matsusue Y (2008) Intrasynovial lipoma causing trigger wrist and carpal tunnel syndrome. Scand J Plast Reconstr Surg Hand Surg [Internet] 42(6):328–330. 10.1080/02844310701282104 [DOI] [PubMed]
- 11.Patil AA, Bhandari P. True trigger wrist and carpal tunnel syndrome A. Case Rep Rev Lit. 2014;9(4):15–18. [Google Scholar]
- 12.Park I-J, Lee Y-M, Rhee S-K, Song S-W, Kim H, Choi K-B (2015) Trigger wrist. Clin Orthop Surg [Internet] 7(4):523–526 [DOI] [PMC free article] [PubMed]
- 13.Coran A, Di Maggio A, Rastrelli M, Alberioli E, Attar S, Ortolan P, Bortolanza C, Tosi A, Montesco MC, Bezzon E, Rossi CR, Stramare R. Core needle biopsy of soft tissue tumors, CEUS vs US guided: a pilot study. J Ultrasound. 2015;18(4):335–342. doi: 10.1007/s40477-015-0161-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cosgrove D, Piscaglia F, Bamber J, Bojunga J, Correas JM, Gilja OH, Klauser AS, Sporea I, Calliada F, Cantisani V, D’Onofrio M, Drakonaki EE, Fink M, Friedrich-Rust M, Fromageau J, Havre RF, Jenssen C, Ohlinger R, Săftoiu A, Schaefer F, Dietrich CF, EFSUMB EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: clinical applications. Ultraschall Med. 2013;34(3):238–253. doi: 10.1055/s-0033-1335375. [DOI] [PubMed] [Google Scholar]
- 15.Ricci P, Marigliano C, Cantisani V, Porfiri A, Marcantonio A, Lodise P, D’Ambrosio U, Labbadia G, Maggini E, Mancuso E, Panzironi G, Di Segni M, Furlan C, Masciangelo R, Taliani G. Ultrasound evaluation of liver fibrosis: preliminary experience with acoustic structure quantification (ASQ) software. Radiol Med. 2013;118(6):995–1010. doi: 10.1007/s11547-013-0940-0. [DOI] [PubMed] [Google Scholar]
- 16.Cantisani V, Consorti F, Guerrisi A, Guerrisi I, Ricci P, Di Segni M, Mancuso E, Scardella L, Milazzo F, D’Ambrosio F, Antonaci A. Prospective comparative evaluation of quantitative-elastosonography (Q-elastography) and contrast-enhanced ultrasound for the evaluation of thyroid nodules: preliminary experience. Eur J Radiol. 2013;82(11):1892–1898. doi: 10.1016/j.ejrad.2013.07.005. [DOI] [PubMed] [Google Scholar]
- 17.De Marchi A, Prever EBD, Cavallo F, Pozza S, Linari A, Lombardo P, Comandone A. Piana R8, Faletti C. Perfusion pattern and time of vascularisation with CEUS increase accuracy in differentiating between benign and malignant tumours in 216 musculoskeletal soft tissue masses. Eur J Radiol. 2015;84(1):142–150. doi: 10.1016/j.ejrad.2014.10.002. [DOI] [PubMed] [Google Scholar]