

ABSTRACT
The coronavirus disease 2019 (COVID-19) pandemic due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has challenged health-care systems and physicians worldwide to attempt to provide the best care to their patients with an evolving understanding of this unique pathogen. This disease and its worldwide impact have sparked tremendous interest in the epidemiology, pathogenesis, and clinical consequences of COVID-19. This accumulating body of evidence has centered around case series and often empiric therapies as controlled trials are just getting underway. What is clear is that patients appear to be at higher risk for thrombotic disease states including acute coronary syndrome (ACS), venous thromboembolism (VTE) such as deep vein thrombosis (DVT) or pulmonary embolism (PE), or stroke. Patients with underlying cardiovascular disease are also at higher risk for morbidity and mortality if infected. These patients are commonly treated with anticoagulation and/or antiplatelet medications and less commonly thrombolysis during hospitalization, potentially with great benefit but the management of these medications can be difficult in potentially critically ill patients.
In an effort to align practice patterns across a large health system (Jefferson Health 2,622 staffed inpatient beds and 319 intensive care unit (ICU) beds across 14 facilities), a task force was assembled to address the utilization of anti-thrombotic and anti-platelet therapy in COVID-19 positive or suspected patients. The task force incorporated experts in Cardiology, Vascular Medicine, Hematology, Vascular Surgery, Pharmacy, and Vascular Neurology. Current guidelines, consensus documents, and policy documents from specialty organizations were used to formulate health system recommendations.
Objective
Our goal is to provide guidance to the utilization of antithrombotic and antiplatelet therapies in patients with known or suspected COVID-19.
KEYWORDS: COVID-19, anti-coagulation, anti-platelet, thrombosis, acute coronary syndrome, venous thromboembolism, stroke, peripheral arterial disease, left ventricular assist device, extracorporeal membrane oxygenation
Background
Coronavirus 2019 (COVID-19) due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a global pandemic with over 4.3 million confirmed cases worldwide and over 297,000 deaths as of 15 May 2020. Currently, the United States leads all countries with over 1.3 million confirmed cases and over 82,000 deaths [1]. Disease severity ranges from asymptomatic to critical illness resulting in fatality. Early studies revealed an increased prevalence of acute cardiovascular events leading to a higher risk of mortality [2–5]. COVID-19 patients may present with hemodynamic instability and increased biomarkers of cardiac injury, specifically troponin and B-Type Natriuretic Peptide. This may be due to an acute coronary syndrome (ACS), myocarditis, Type 2 myocardial infarction, coronary vasospasm, or stress-induced cardiomyopathy. The specificity of these biomarkers in this setting is uncertain. Additionally, markedly elevated D-dimer levels are associated with severe illness and high mortality. This has been postulated to be due to micro thrombosis but alternatively may be due to disseminated intravascular coagulation (DIC) secondary to an increased inflammatory state. Patients also appear at higher risk of venous thromboembolism (VTE) due to critical illness, immobility, and inflammation.
Managing patients acute antiplatelet and anticoagulant regimens can be difficult without clear consensus on diagnosis and treatment. Many patients are on antiplatelet and anticoagulants for preexisting conditions when they present to the hospital and thus the balance of further ischemic/thrombotic events vs. bleeding events must be weighed. The margin of error appears to be narrower in patients with multi-system failure where fluctuating organ function can impact drug metabolism.
We aim to provide guidance for the management of various clinical scenarios encountered in COVID-19 infected patients recognizing that these recommendations may change given the rapidly evolving understanding of COVID-19 pathophysiology.
Clinical scenarios
Acute coronary syndrome (ACS)
The diagnosis of ACS in the COVID-19 patient can be challenging given that patients often have elevated troponin levels. Biomarkers are nonspecific measures of cardiac injury and may represent a myriad of cardiac conditions including myocardial ischemia secondary to either plaque rupture or demand ischemia,, myocarditis, stress cardiomyopathy, or coronary spasm. In order to assist with diagnosis and treatment, it is important to take into consideration the patient’s clinical presentation, electrocardiogram (ECG), and point of care ultrasound to evaluate ventricular wall motion. Typically, with ACS there is a characteristic rise and fall in troponins which represents myocardial tissue necrosis due to hypoperfusion, as opposed to myocarditis which can often lead to elevated but relatively stable troponin levels that represent ongoing myocardial inflammation and injury. A recent report demonstrated that ST-elevation myocardial infarction (STEMI) activation is down 38% in the United States [6] with growing concern that patients do not seek immediate medical attention due to fear of exposure to COVID-19 leading to missed events.
We recommend in all patients with concern for ACS, non-enteric coated aspirin 162–325 mg should be given immediately if no contraindication exists followed by daily low dose aspirin (81 mg) indefinitely. P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel) should be considered in these patients with guidance from cardiology with a length of therapy for 1 year in most patients [7–9]. For patients on anticoagulation prior to ACS, triple therapy should be used for the shortest duration possible. A regimen of a direct oral anticoagulant (DOAC) with clopidogrel with short duration of aspirin is now considered the standard of care and triple therapy with warfarin should be avoided [10–15].
STEMI specific management
All STEMI patients should receive standard medical therapy including full dose aspirin, high-intensity statin, unfractionated heparin (UFH), and nitrates for chest pain if hemodynamics allow. There has been considerable discussion regarding best practices for patients who present with STEMI in the COVID-19 era with the debate over fibrinolytic therapy versus primary percutaneous coronary intervention (PCI). Based on early experience out of Peking Union Medical College Hospital in China, it was recommended that all STEMIs be treated with thrombolytic therapy given its efficacy and ease of administration and to limit health-care worker exposure [16]. In the United states, approximately 13% of STEMIs prior to the COVID-19 era had fibrinolytic reperfusion strategies due to the inability to access hospitals with PCI capabilities within 120 minutes [17]. To ensure staff safety, there can be considerable system delays in patients who present with STEMI and have concern for COVID-19. These delays may cause patients to no longer receive standard of care primary PCI within the designated door to balloon time of 90 minutes, and the mortality benefit of primary PCI may no longer be significant compared to fibrinolytic therapy [18]. Finally, there is concern about transmission of infection from patient to staff and resources needed for these patients that fibrinolytic therapy may be considered in the COVID-19 patient population [19].
Despite the initial push for fibrinolytic therapy, there is hesitation with this strategy as it can lead to unnecessary use of thrombolytics in the case of ‘STEMI-mimicker,’ patients with COVID-19 who have non-obstructive coronary artery disease on coronary angiography despite STEMI on ECG [20,21]. The use of fibrinolytics in this population would lead to no clinical benefit and potential significant harm. Even in those patients who receive thrombolytics for STEMI, approximately 50% require rescue PCI and thus the benefit of thrombolytics seems to be low in patients where PCI can be performed. Due to these concerns, the current Society for Cardiovascular Angiography and Interventions (SCAI) consensus document suggests continuing primary PCI for STEMI patients as the treatment of choice with the use of fibrinolytic therapy only for selected lower-risk patients (those with inferior STEMI without RV involvement and those with lateral STEMI without hemodynamic compromise) [20]. The recommendation for primary PCI in the COVID-19 patient was reiterated in a consensus statement from SCAI, American College of Cardiology (ACC) and the American College of Emergency Physicians (ACEP) and a pharmacoinvasive approach should only be considered if primary PCI is not feasible [22]. We agree that primary PCI should remain standard of care if a patient is at a PCI capable hospital. The lack of familiarity with fibrinolytics dosing for many providers, their increased risk of significant bleeding, and the possibility of treating patients without coronary thrombosis makes this a less attractive first-line therapy. In patients with whom primary PCI is not possible due to access to a cardiac cath lab, we recommend a pharmacoinvasive approach with fibrinolytic therapy followed by transfer to a PCI capable hospital for possible intervention [23]. If PCI is performed, dual antiplatelet therapy with aspirin and P2Y12 should ideally be continued for 1 year.
Non-ST elevation myocardial infarction (NSTEMI) specific management
The diagnosis of type 1 NSTEMI (plaque rupture) is difficult in the COVID-19 era due to the elevated troponin levels in a significant proportion of patients [4]. The true incidence of type 1 myocardial infarctions is not well known and thus COVID-19 positive patients with elevated troponins should be risk stratified to determine the most appropriate management. All patients should receive medical therapy with full dose aspirin, high-intensity statin, parental anticoagulation (heparin or low molecular weight heparin (LMWH)), beta blocker if hemodynamics allow, and possible nitrate therapy if ongoing chest pain [7]. In patients undergoing early invasive strategy, we recommended using heparin over LMWH as an anticoagulant of choice due to the ability to titrate the medication and to measure the degree of anticoagulation in the cardiac catheterization lab with activated clotting times. Patients who are COVID-19 negative should be considered for early invasive therapy [20]. In patients who are COVID-19 positive or still under investigation, we recommend invasive strategy in patients who have GRACE score > 140 [24] or those with high-risk clinical features such as refractory chest pain, unstable arrhythmias, heart failure, or hemodynamic instability. In COVID-19 positive patients with low-risk NSTEMI, we recommend a delayed invasive approach and upfront medical management [7]. These patients receive less benefit from early-invasive primary PCI compared to high-risk NSTEMI. We believe that the risks of resource utilization, risk of virus transmission to hospital workers, and lack of definitive diagnosis is higher than the potential benefit of invasive angiography and potential PCI in this population. We recommend LMWH preferentially over UFH due to the ease of administration, lack of medication titration, and fewer lab draws that could lead health-care professionals to unnecessary exposures. In medically treated NSTEMI patients, aspirin (81 mg) with either clopidogrel (75 mg) or ticagrelor (90 mg BID) should be given if no contraindication exists. Prasugrel is not indicated for patients being treated medically for NSTEMI [25]. Consideration for outpatient testing and coronary angiography can be considered in these patients in the future once their infection has resolved in accordance with SCAI/ACC/ACEP recommendations [22].
Stable ischemic heart disease (SIHD)
Patients with COVID-19 may present on therapy from previous coronary intervention irrespective of their current hospital admission. Data is limited in this patient population, and we, therefore, rely on established guidelines for antiplatelet recommendations [8]. Patients with COVID-19 may have thrombocytopenia and other coagulopathies similar to DIC which can make the use of anti-platelet agents more challenging. It is important for providers to understand the indication for the patient’s antiplatelet therapy in SIHD as it can help guide therapy in those patients at higher bleeding risk. All patients with previous stent placement should be continued on single antiplatelet therapy regardless of indication unless at very high bleeding risk. In patients on therapy with platelet count > 50,000 mm3 and at a low risk of bleeding, we recommend continuing outpatient anti-platelet therapy for the duration recommended in the ACC/AHA guidelines [8]. In patients with a platelet count between 25,000 mm3 to 50,000 mm3 we recommend continuing aspirin therapy and if platelet count <25,000 mm3 discussion with cardiology regarding the ongoing benefits of aspirin therapy (i.e. location of stents, previous ischemic history, size of stents, timing of stent) with the risk of bleeding.
Atrial fibrillation/Atrial flutter
Acute and chronic respiratory illnesses are risk factors for atrial fibrillation [26,27]. COVID-19 patients, commonly present with shortness of breath secondary to viral pneumonia with critically ill patients progressing to acute respiratory distress syndrome (ARDS). Unfortunately, the rate of new atrial fibrillation in these patients is unknown. Management of patients with atrial fibrillation includes oral anticoagulation which is recommended for patients with CHA2DS2-VASc score of 2 or more in men or 3 or more in women as long as the benefit of anticoagulant outweighs the risk of bleeding [28]. In most scenarios, direct oral anticoagulants (dabigatran, rivaroxaban, apixaban, and edoxaban) are recommended over warfarin due to large randomized controlled trials showing non-inferiority or superiority for stroke reduction and superiority for bleeding risk in patients with non-valvular atrial fibrillation [29–32].
In the inpatient setting, there is less guidance on the initiation of anticoagulation for new onset atrial fibrillation and decisions to continue outpatient oral anticoagulation can be more difficult due to rapid fluctuations in clinical status, need for invasive procedures, and renal/liver function changes. The risk of endothelial damage, vascular inflammation, and vascular thrombosis appears heightened in severe COVID-19 patients and thus could pose an increased risk of arterial thrombosis in this patient population. The use of UFH or LMWH may be considered in patients with high potential stroke risk and new onset atrial fibrillation; however, heparin drips require constant monitoring and titration of dosing during hospitalization leading to increased nursing exposure to potential COVID-19 patients. In this group, therapeutic enoxaparin 1 mg/kg every 12 hours could be used instead of unfractionated heparin. Inpatient anticoagulation will be recommended for de novo AF based on the risks of benefits of the individual patients with men with CHA2DS2-VASc ≥2 and women ≥3 being most likely to benefit from anticoagulation. In this context, the annual stroke risks are between 5% and 10% in patients with CHA2DS2-VASc 5 or 6, and >10% in patients with CHA2DS2-VASc ≥7 [33]. We would recommend LMWH over heparin as long as Creatinine Clearance (CrCl) ≥ 30 and no need for invasive procedures.
In patients who are established on anticoagulation due to previous diagnosis of atrial fibrillation, continuing oral anticoagulation should be considered in patients at low risk of clinical decompensation or bleeding. In patients who are critically ill, we recommend holding outpatient oral anticoagulation and consideration of using a parenteral agent (heparin/LMWH). The risks and benefits of stroke vs. bleeding as well as duration of time without oral anticoagulation should be considered in all cases. For patients who do not have prohibitive bleeding risk and CHA2DS2-VASc score ≥ 5 or previous thromboembolic event, we would recommend a parental agent with LMWH considered first-line therapy if CrCl ≥ 30 [34]. Patients with mechanical heart valves and atrial fibrillation who require invasive procedures should be bridged with heparin or LMWH [33,35]. The ACC ManageAnticoag app can be used to help providers determine the need for anticoagulation interruption and bridging in case by case scenario (Figure 1).
Figure 1.
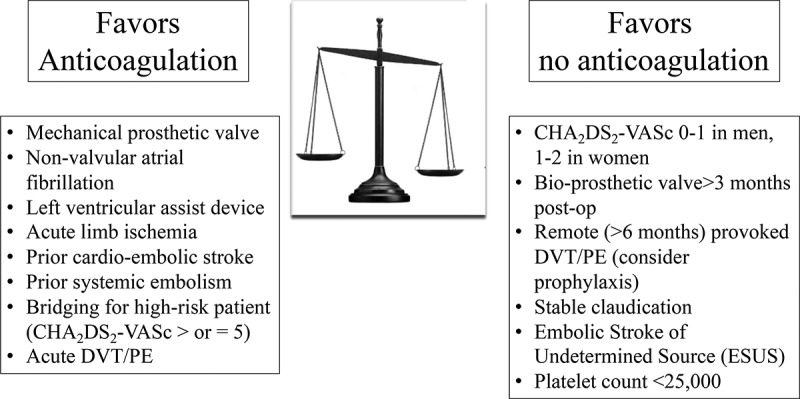
Risk factors to determine the need for therapeutic anticoagulation.
Prosthetic heart valves
Despite the concern for increased thrombotic risk in COVID-19 patients, there are no published reports of prosthetic valve thrombosis in this patient population. As such, we recommend anticoagulation in accordance with the latest ACC/AHA valvular guidelines. All patients with a mechanical heart valve should continue anticoagulation with a vitamin K antagonist (VKA) with their previously recommended goal international normalized ratio INR [36,37]. All patients with mechanical valve prostheses should also be continued on 81 mg aspirin daily [38], and it is reasonable for patients with bioprosthetic valve prostheses to be continued on ASA 81 mg daily [38]. Anticoagulation with DOACs should be avoided in patients with mechanical valve prostheses [39].
In patients on anticoagulation due to mechanical valve, anticoagulation should not be interrupted for low bleeding risk procedures. If, for a procedure, anticoagulation needs to be interrupted, then bridging with LMWH or heparin is reasonable for patients with mechanical mitral valve, mechanical aortic valve with risk factor(s) (atrial fibrillation, low EF, hypercoagulable state, or previous VTE), or older generation mechanical aortic valve [40]. We suggest that warfarin only be continued upfront in those patients who are not critically ill or at high bleeding risk. In all others, suggest transition to a parental agent with a bridge until warfarin can be resumed.
Stroke
Currently, the most common neurologic manifestations of COVID-19 that should prompt strong consideration of an acute cerebrovascular event include dizziness, headache, focal neurologic deficits, and encephalopathy [41]. In four early studies, ischemic and hemorrhagic stroke complicated COVID-19 infection in about 6% of patients at a median 10 days after symptom onset and the incidence, particularly of stroke due to large vessel occlusion, continues to rise in the United States [42–45]. In addition to common cardiovascular comorbidities in the elderly COVID-19 positive population, mechanisms for ischemic stroke in infected patients of all age groups include hypercoagulability from pro-inflammatory state, embolism from virus-related cardiac injury, and infection-induced disseminated intravascular coagulation. Intracerebral hemorrhage and hemorrhagic conversion of ischemic stroke may also occur due to possible coagulopathy, specifically thrombocytopenia, in the severely ill, fluctuating blood pressures due to viral-binding to ACE 2 receptors [46], and potential interactions between anticoagulants and medications now commonly used for COVID-19 patients (Table 1).
Table 1.
Investigative medications for COVID-19 positive patients and effect on DOAC concentration.
| Medication | Mechanism | Dabigatran | Apixaban | Edoxaban | Rivaroxaban |
|---|---|---|---|---|---|
| Hydroxy-chloroquine | None | - | - | - | - |
| Azithromycin | P-glycoprotein competition | ↑No dose adjustment recommended | ↑VTE:30 mg daily AF: No dose changes |
||
| Remdesivir | Reportedly CYP3A4 | ? | ? | ? | ? |
| Lopinavir/Ritonavir | CYP3A4 Inhibition/P-glycoprotein competition | ↑No dose adjustment recommended, however would avoid if possible | ↑↑50% dose reduction (do not use if patient requires 2.5 mg BID at baseline) | ↑↑Do not co-administer | ↑↑Do not co-administer |
| Tocilizumab | CYP3A4 Inducer (weak) | - | ↓No dose adjustment recommended | - | ↓No dose adjustment recommended |
| Sarilumab | CYP3A4 Inducer | - | ↓No dose adjustment recommended | - | ↓No dose adjustment recommended |
| Favipiravir | CYP2C8 | - | - | - | - |
| Nitazoxanide | Weak CYP2C9 | - | - | - | - |
| Tacrolimus | P-glycoprotein competition in-vitro | - | -/↑ | - | -/↑ |
| Camostat Mesilate | Unknown | ? | ? | ? | ? |
Non-contrast computed tomography (CT) head is the appropriate initial imaging in COVID-19 patients with neurologic symptoms particularly prior to initiation of antithrombotic agents. While most serum studies are not required prior to emergent IV-tPA use based on guidelines, it may be reasonable to await results of coagulation studies and complete blood count in critically ill COVID-19 suspected or positive patients prior to thrombolytic administration. Patients with large vessel occlusion remain eligible for endovascular therapy despite infection.
Antithrombotic recommendations for secondary prevention of stroke in the suspected or positive COVID-19 patient are currently unchanged from the general population assuming the absence of coagulopathy and prothrombotic state. For ischemic stroke due to small and large vessel atherosclerotic disease as well as embolic strokes of undetermined source, antiplatelet therapy with aspirin, clopidogrel, or aspirin/dipyridamole remains the appropriate first-line therapy [47,48]. Dual antiplatelet therapy should be reserved for symptomatic intracranial atherosclerotic disease [49], certain carotid cases, recent stenting, and patients with recent minor stroke or high-risk TIA [50].
Outcomes in available COVID-19 patient data do not suggest clear benefit over risk of therapeutic anticoagulation for primary stroke prevention. However, assuming low risk of hemorrhagic conversion, therapeutic anticoagulation with LMWH is frequently initiated for secondary stroke prevention in the critically ill with significantly elevated D-dimer and no other clear etiology of ischemic stroke. In addition to patients with atrial fibrillation, consider anticoagulation with UFH/LMWH, warfarin, or DOACs in patients with ischemic strokes that are embolic appearing with cardiac etiology, non-occlusive thrombi, recurrent ischemic strokes, atypical intracranial stenosis, venous sinus thrombosis, extracranial dissection with ischemia, and pro-thrombotic state [51]. Minimize the use of triple therapy to avoid intracranial hemorrhagic complications. The appropriate timeframe to initiate anticoagulation in the ischemic stroke patient remains heavily individualized based on age, comorbidities, stroke size and location, imaging characteristics, and medication choice. The decision to initiate antithrombotic therapy in COVID-19 positive patients with acute neurologic symptoms should be made in conjunction with a neurologist.
Peripheral arterial disease (PAD)
Stable, chronic PAD
Peripheral arterial disease is a common cardiovascular disorder that is highly under-recognized with significant cardiovascular morbidity, mortality, and quality of life impairment. In patients with symptomatic peripheral arterial disease, anti-platelet medication with either aspirin (75–325 mg per day) or clopidogrel (75 mg per day) is recommended as first-line therapy [52]. The use of dual anti-platelet therapy is beneficial only in those patients who have undergone revascularization [52]. Patients should remain on these medications throughout their hospitalization unless high bleeding risk.
Acute limb ischemia
Acute limb ischemia (ALI) is associated with significant morbidity and mortality and is defined as <2 weeks of severe hypoperfusion of the limb characterized by features of pain, pallor, pulselessness, poikilothermia, paresthesias, and paralysis [53]. Patients who present to the hospital with ALI should be emergently evaluated to assess limb viability and systemically anticoagulated with heparin unless contraindicated. In early single-center retrospective studies, the incidence of ALI in COVID-19 patients appears to be higher than the general public and includes patients with no traditional risk factors [54,55]. The success of revascularization was also decreased felt to be secondary to the virus-induced hypercoagulable state [54].
In patients with COVID-19, it is important to remain hypervigilant for signs and symptoms of ALI. Emergent consultation with vascular surgery should be obtained and early initiation of parental anticoagulation is paramount due to the hypercoagulable state observed in some patients. We suggest that patients undergo limb salvage procedures in accordance with standardized guidelines due to the high risk of morbidity and mortality without acute intervention. Acro-ischemia has been described in patients who are critically ill with COVID-19 pneumonia and, despite treatment with LMWH, there was no clinical improvement and there was a high rate of mortality [56]. In these patients, a palliative approach should be considered.
Venous thromboembolism (VTE)
Recent data suggests a high rate of VTE in the hospitalized, critically ill COVID-19 patient [57,58]. The mechanism by which these patients are developing VTE at significant rates have been hypothesized including immobility, severe inflammatory response, and coagulopathy including DIC. Decision algorithms of testing patients for asymptomatic and symptomatic VTE as well as treatment of VTE are not well defined. Patients should be risk stratified (high, intermediate, or low risk) on presentation to help guide therapy [59,60].
For COVID-19 patients who present with or develop acute VTE during hospitalization, we recommend treating with anticoagulation if no contraindication exists. For all patients with symptomatic PE, we recommend activating the pulmonary embolism response team (PERT) to provide interdisciplinary care and make individualized decisions based on the patient’s clinical status, co-morbidities, and hospital factors [60,61]. In patients with high-risk PE, we recommend systemic or catheter-directed thrombolysis in patients with low bleeding risk or those who deteriorate after initial anticoagulation (i.e. development of worsening hypoxia, tachycardia, RV failure) [60,62,63]. In patients at high bleeding risk, the use of catheter-directed mechanical thrombolysis or surgical removal should be considered in consultation with the PERT team [64].
In the intermediate-risk patient, debate remains over the best treatment. Risk calculators such as the PESI or BOVA score can help further risk stratify these patients to help guide therapy [65,66]. Anticoagulation remains the mainstay of treatment for this population and we suggest the use of parental anticoagulation with heparin or enoxaparin instead of a DOAC due to potential decompensation [60,67,68]. Enoxaparin is preferred if CrCl is ≥ 30. The use of catheter-directed thrombolysis or thrombectomy for intermediate-risk PE should be made on a case by case basis with guidance from the PERT team. Due to the risk of infectivity, there should be a higher threshold to perform invasive procedures that have not been shown to improve mortality [64]. Once patients have stabilized, we recommend the use of DOAC over the use of warfarin or LMWH therapy [60,62].
In the low-risk patient, we recommend treatment with a DOAC without the need of parental anticoagulation (apixaban or rivaroxaban) to avoid increasing length of stay.
The use of inferior vena cava filters should not be considered for routine use and only considered in those patients who have absolute contraindications for anticoagulation with clinically relevant VTE [62]. In a patient who requires an IVC filter, anticoagulation should still be restarted once the bleeding risk has passed.
VTE prophylaxis
The incidence of thrombotic complications in critically ill COVID-19 patients in the ICU has been shown to be at least 25–40% in observational studies [57,58]. This increased rate of thrombotic complications appears to be related to a hypercoagulable state similar to DIC or thrombotic microangiopathy yet with unique differences including the appearance of a positive lupus anticoagulant in patients [51,69,70]. In order to attempt to decrease the rates of thrombotic complications, preventative measures should be used whenever possible [71]. Heparin, enoxaparin, and fondaparinux are all recommended for VTE prophylaxis by the American College of Chest Physicians [72]. One retrospective study of critically ill COVID-19 patients with D-dimers > 6x ULN compared UFH or LMWH plus antiviral therapy versus no pharmacologic prophylaxis plus antiviral therapy. The combination therapy of pharmacologic plus antiviral group had a significantly decreased 28-day mortality [73]. LMWH was preferentially used in this study due to its previously reported anti-inflammatory effect. Another retrospective trial in critically ill patients in China confirmed lower mortality in those patients who were treated with pharmacologic prophylaxis, yet stated that Asian populations have a low incidence of VTE and thus higher doses of anticoagulation may be necessary in other populations [74].
There remains concern throughout the medical community that in the most critically ill patients, pharmacologic prophylaxis is not enough to reduce the risk of thrombosis. A French cohort of ICU patients on pharmacologic prophylaxis found a high prevalence of thrombotic complications including PE, stroke, circuit clotting of continuous renal replacement therapy or extracorporeal membrane oxygenation (ECMO) with minimal bleeding risk suggesting the need for higher doses of prophylactic anticoagulation in this patient population [70]. In another retrospective study, mechanically vented patients were found to have a significantly decreased risk of mortality if treated with full-dose anticoagulation compared to those not on anticoagulation, yet this mortality benefit was not seen in all COVID-19 patients admitted to the hospital [75]. The use of higher dose thromboprophylaxis or full-dose anticoagulation is currently being investigated in multiple randomized control trials (NCT04372589, NCT04367831, NCT04345949, and NCT04366960).
We recommend that all patients on admission be assessed for the risk of VTE. For patients with platelet counts greater than 25,000, we recommend using pharmacologic prophylaxis for all COVID-19 positive patients if no contraindication exists. While anecdotal and retrospective data may support higher doses of pharmacologic prophylaxis in critically ill patients, there is considerable risk of bleeding in these populations and thus without higher-level evidence, we remain hesitant to adopt these practices. As such, we continue to recommend standard dose pharmacologic prophylaxis with an understanding that our recommendations may change as data continues to evolve.
Enoxaparin is the preferred agent for patients with a CrCl ≥ 30 ml/min. For those with impaired renal function, heparin can be used as an alternative agent with a dosing regimen based on patient weight. For heparin dosing, patients <50 kg use 5,000 units q12 hours, for patients 50–120 kg we recommend 5,000 units Q8 hours, for >120 kg we recommend 7,500 units Q8 hours. For enoxaparin dosing, we recommend 30 mg Qday for those <40 kg, 40 mg Qday for patients 40–120 kg, and 40 mg twice a day for patients >120 kg. We recommend mechanical prophylaxis in addition to pharmacologic prophylaxis for all ICU patients without contraindication. For patients that are unable to be on pharmacologic prophylaxis due to low platelets or active bleeding we recommend mechanical prophylaxis (Figure 2).
Figure 2.

Venn diagram illustrating the overlap in patient risk factors and co-morbidities to determine the type of anticoagulation.
Critically ill patients who survive to discharge are still at increased risk of thromboembolic events [76]. Given that thromboembolic events seem to be elevated in the COVID-19 population, this risk may be even higher. We recommend that all patients be assessed for VTE risk at discharge for consideration of extended VTE prophylaxis. Multiple studies pre-COVID-19 have shown the benefit of extended prophylaxis for high-risk patients following discharge. The decreased incidence of thrombotic events is at the expense of a slight increase in bleeding. Multiple agents have shown efficacy with extended prophylaxis including enoxaparin, rivaroxaban, and betrixaban [77–79]. We recommend that patients should be risk assessed for VTE and bleeding on discharge for extended prophylaxis using the IMPROVED for VTE and IMPROVE Bleeding risk indices [80–83]. The patient should have a creatinine clearance and liver function panel in addition to platelet count (>25,000 mm3) prior to the initiation of extended prophylaxis. We preferentially recommend rivaroxaban 10 mg daily for 6 weeks for extended prophylaxis. Enoxaparin 40 mg Qday subcutaneously can be used as an alternative agent if the CrCl ≥ 30 ml/min. If patients are unable to receive pharmacologic prophylaxis, we recommend knee high compression stockings (15–20 or 20–30 mmHg) and encourage ambulation. Patients should be educated on the symptoms and signs of DVT/PE and report such events to their primary care provider.
Disseminated intravascular coagulation (DIC)
DIC can be seen in hospitalized patients with severe illness [84]. It can accompany the acute respiratory failure and multi-organ failure from COVID-19 and is associated with poor prognosis [85]. Yet, further studies suggest that while similar to DIC, the coagulopathy of COVID-19 has distinct features with only mild thrombocytopenia and normal fibrinogen levels early in the course [2,86]. There also appear to be similarities to thrombotic microangiopathy with elevated LDH and ferritin levels [87]. These coagulation abnormalities appear to promote the hypercoagulable hypothesis of COVID-19 which has been further suggested by autopsy reports showing micro thrombosis of the lungs and various other organs [69].
The optimal initial approach to DIC or DIC like coagulopathy is to treat underlying causes, and in this case to support O2 and CO2 exchange, metabolic functions, and possibly use anti-viral agents and anti-cytokine release syndrome agents. Clinically, close attention for these patients should be directed to unexpected bleeding or thrombosis. In addition to clinical monitoring, lab tests to monitor for the development and progression of DIC are the CBC, PT and aPTT, and fibrinogen. Serial comparisons of the labs are essential as the development of DIC during hospitalization is a poor prognostic indicator [85]. D-dimer, while not specific for DIC has also been shown independently to be a predictor of morbidity and mortality when significantly elevated [2,85,86].
Despite the incidence of DIC being a poor prognostic indicator, the treatment of these patients remains the previous standard of care. In accordance with the guidance from the International Society of Thrombosis and Hemostasis (ISTH), these patients should be treated with prophylactic dose enoxaparin if no contraindication exists [88]. There is no role for therapeutic anticoagulation in DIC, in the absence of an acute thrombotic event.
While bleeding in COVID-19 patients remains less common than thrombosis, bleeding risk increases as the platelet count goes below 50,000 mm3, the PT and PTT rise to > 1.4 X ULN, or when fibrinogen falls below 100 mg/dl. There is no role for giving blood products to correct lab abnormalities in the absence of bleeding [89]. If bleeding occurs, blood product(s) should be given to replace the depleted components. Factor VIIa and prothrombin complex concentrate use are discouraged, as the risk of serious thrombosis is high.
Drug–drug interactions
In the COVID-19 era, there is an influx of drugs aimed to improve patient’s morbidity and mortality. The only FDA approved therapy at this time for COVID-19 is remdesivir, and there remains over 100 pharmacological trials on clinical-trials.gov attempting to find further treatment for this disease [90]. The effect of these medications on anti-platelet agents and anticoagulants is important for the individualized patient and the prescriber. Pathways that are most important for identifying drug–drug interactions appear mediated via cytochrome P450 (CYP450) and/or transporter permeability glycoprotein (P-gp). The most common medications being used include hydroxychloroquine/chloroquine, azithromycin, remdesivir, lopinavir/ritonavir, and tocilizumab which may affect the efficacy of antiplatelets and anticoagulants.
P2Y12 inhibitors are commonly used in a wide spectrum of cardiovascular disease states as described above. Their interactions with treatments for COVID-19 are not well known and rely on package inserts and anecdotal experience. The only medication with significant known interactions with P2Y12 inhibitors is lopinavir/ritonavir, a protease inhibitor previously used for the treatment of HIV. Early studies in patients with COVID-19 have found no decrease in morbidity or mortality with this medication combination [91], yet ongoing trials continue to look at the impact of this combination on patients with COVID-19. It is a known inhibitor of CYP3A4 metabolism and has significant effects on clopidogrel and ticagrelor, yet no significant effect on prasugrel. Inhibition of CYP3A4 in patients taking clopidogrel can decrease its efficacy; however, inhibition of CYP3A4 leads to increased effects of ticagrelor and thus neither is recommended to be administered in patients on lopinavir/ritonavir [92,93].
Despite advances in DOACs for reducing systemic thromboembolism and systemic bleeding compared to warfarin, DOACs have drug–drug interactions that must be considered in all patients. CYP3A4 is important for the metabolism of apixaban (20–25%) and rivaroxaban (18%) with no significant effect on dabigatran and edoxaban while P-gp is an important mediator for apixaban, dabigatran, and rivaroxaban. The FDA recommends avoiding concurrent use of apixaban and rivaroxaban with inducers of P-gp or CYP3A4 [94]. There is limited data on the in vivo effects of these medications with DOAC concentrations and unless explicitly known we do not have recommendations regarding avoiding or dose changes of these medications. Table 1 summarizes the interactions between the investigational drugs and commonly prescribed DOACs. Further drug–drug interactions between DOACs and commonly used medications can be found in the EHRA practical guidelines [95]. Hydroxychloroquine, used primarily in auto-immune disease, has not been found to interact with CYP3A4 or P-glycoprotein. Azithromycin is an inhibitor of P-gp and thus could increase the serum concentration of dabigatran especially in conjunction with other cardiac P-gp inhibitors such as amiodarone. It is not recommended to decrease dabigatran dosing. However, patients on edoxaban should only be prescribed the 30 mg dose for VTE. Lopinavir/ritonavir is known strong inhibitors of both CYP3A4 and P-glycoprotein and thus could have significant effects on the pharmacokinetics of all DOACs leading to increased concentration and potential bleeds. The European Heart Rhythm Association practical guidelines suggests that DOACs should not be given in patients taking ritonavir [95]. However, the package insert of apixaban recommends dose reduction by 50% and should not be co-administered if patient is on low dose apixaban (2.5 mg BID). We suggest to avoid DOACs in patients with whom lopinavir/ritonavir is being prescribed. Tocilizumab is known to decrease serum concentrations of CYP3A4 substrates and thus could decrease the effectiveness of apixaban or rivaroxaban. Finally, remdesivir has little pharmacokinetic data available although it is believed that there are no significant clinical interactions with CYP3A4 enzyme. (Table 2)
Table 2.
Takeaway points from paper.
| 1. COVID-19 patients have much in common with other critically ill patients where there may be a narrow margin for AC and APT of benefit (preventing thrombotic events) and risk (bleeding). |
| 2. The rationale for AC should be carefully examined in all inpatients, balancing risk and benefit. For example: a patient on AC with CHA2DS2-VASc of 1 for men and 2 for women. Point of care risk calculators and apps to assist in evaluating the risk and benefit should be used when available. |
| 3. In COVID-19 confirmed or expected patients, it is reasonable to continue outpatient anticoagulation unless they become critically ill in the ICU or if they have invasive procedures planned. |
| 4. If interrupted, bridging should not be offered in low risk thrombosis patients. |
| 5. Routine use of aspirin increases bleeding risk by as much as 50% and benefit should be carefully assessed. |
| 6. Prolonged DAPT beyond 6 months for elective stenting and beyond a year for ACS should be examined, balancing risk and benefit. |
| 7. Warfarin based triple therapy for patients with stenting and AF is inferior to DOAC based regimen with P2Y12 and short duration aspirin. |
| 8. Decision to bridge either with UFH or LMWH in a COVID-19 patient exposes nursing to a greater degree. This is not worthwhile in a low thrombotic risk patient. |
| 9. When there is the potential for significant drug-drug interactions, consultation with pharmacy is invaluable. |
| 10. Careful consideration is required in weighing the risks and benefits of any intervention not only to the COVID-19 confirmed or expected patient, but also to the health care workers who are directly involved in patient care. Special consideration should be given when possible to limiting health care worker exposure to COVID-19. |
Conclusions
COVID-19 has challenged our thinking about the management of critically ill patients. The mechanisms of this disease and its complications' continue to be elucidated. That being said the principles of managing these patients are built on the foundations of evidence-based medicine in severely ill patients. There is a narrow therapeutic index between prevention and treatment of venous and arterial thrombosis in these patients and the risk of bleeding. This document can be used to help guide providers to treat cardiovascular patients at high risk during this pandemic (Figure 2). Only by adhering to the principles of practicing what we know and maintaining openness to what we don’t can we stand up to the greatest challenge of our professional lives.
Acknowledgments
We want to acknowledge the following people who helped with formulation of our best practice initiative for our institution: David Fischman MD, Michael Savage MD, Alec Vishnevsky MD, Nicholas Ruggiero MD, Robert Watson MD, Mohammad Murtaza MD, Kartic Giri MD, Matthew Decaro MD, Gregary Marhefka MD, Rene Alvarez MD, Eduardo Rame MD, Howard Weitz MD, Yair Lev MD, Nawar Al Rawas MD, Hitoshi Hirose MD,PhD, Paul Dimuzio MD, Babak Abai MD, Dawn Salvatore MD, Christian Fidler MD, Lynda Thomson Pharm D, Steven McKenzie MD, Moshe Chasky MD, Michael Rotkowitz MD, Walter Kraft MD, Robert Perry MD, Laurence Needleman MD, Photi Galanis MD, Luis Eraso MD, Dina Orapallo CRNP, Heather Yenser CRNP.
Declaration of interest
The contents of the paper and the opinions expressed within are those of the authors, and it was the decision of the authors to submit the manuscript for publication.
The authors report no conflicts of interest for their manuscript.
Reviewer’s disclosures
A reviewer on this manuscript has disclosed that their institution has received research grants, and they have received honoraria for CME programs and consulting for companies developing novel antithrombotic therapies. The other peer reviewers on this manuscript have no other relevant financial relationships or otherwise to disclose.
References
- 1.World health Organization. Coronavirus Disease . (COVID-19) situation report - 116. 2019. [cited 2020 May 15]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200515-covid-19-sitrep-116.pdf?sfvrsn=8dd60956_2
- 2.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan China. Lancet. 2020;395(10223):497–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020. March 3. DOI: 10.1007/s00134-020-05991-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020. March 25. [published online]. DOI: 10.1001/jamacardio.2020.0950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020. March 27. [published online]. DOI: 10.1001/jamacardio.2020.1017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Garcia S, Albaghdadi MS, Meraj PM, et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J Am Coll Cardiol. 2020. DOI: 10.1016/j.jacc.2020.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014;64:e139–228. [DOI] [PubMed] [Google Scholar]
- 8.Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction, 2014 ACC/AHA guideline for the management of patients with non–ST-elevation acute coronary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. J Am Coll Cardiol. 2016;68:1082–1115.27036918 [Google Scholar]
- 9.Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J. 2018;39:213–254. [DOI] [PubMed] [Google Scholar]
- 10.Dewilde WJ, Oirbans T, Verheugt FW, et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet. 2013;381:1107–1115. [DOI] [PubMed] [Google Scholar]
- 11.Fiedler KA, Maeng M, Mehilli J, et al. Duration of triple therapy in patients requiring oral anticoagulation after drug-eluting stent implantation: the ISAR-TRIPLE trial. J Am Coll Cardiol. 2015;65:1619–1629. [DOI] [PubMed] [Google Scholar]
- 12.Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017;377:1513–1524. [DOI] [PubMed] [Google Scholar]
- 13.Gibson CM, Mehran R, Bode C, et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N Engl J Med. 2016;375:2423–2434. [DOI] [PubMed] [Google Scholar]
- 14.Lopes RD, Heizer G, Aronson R, et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med. 2019;380:1509–1524. [DOI] [PubMed] [Google Scholar]
- 15.Vranckx P, Valgimigli M, Eckardt L, et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): a randomised, open label, phase 3b study. Lancet. 2019;394:1335–1343. [DOI] [PubMed] [Google Scholar]
- 16.Zhi-Cheng J, Hua-Dong Z, Xiao-Wei Y, et al. on behalf of the COVID-19 & AMI committee of Peking Union Medical College Hospital, recommendations from the Peking Union Medical College Hospital for the management of acute myocardial infarction during the COVID-19 outbreak. Eur Heart J 2020. ehaa258. DOI: 10.1093/eurheartj/ehaa258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol. 2010;56:254–263. [DOI] [PubMed] [Google Scholar]
- 18.Nallamothu BK, Bates ER.. Percutaneous coronary intervention versus fibrinolytic therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol. 2003;92:824–826. [DOI] [PubMed] [Google Scholar]
- 19.Daniels MJ, Cohen MG, Bacry AA, et al. Reperfusion of STEMI in the COVID-19 era – business as usual? Circulation. 2020. April 13. [Epub ahead of print]. DOI: 10.1161/CIRCULATIONAHA.120.047122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Szerlip M, Anwaruddin S, Aronow HD, et al. Considerations for cardiac catheterization laboratory procedures during the COVID-19 pandemic: SCAI ELM perspectives. Catheter Cardiovasc Interv. Accessed 2020 March 25. [Epub 2020 Mar 24]. DOI: 10.1002/ccd.28887 [DOI] [PubMed] [Google Scholar]
- 21.Bangalore S, Sharma A, Slotwiner A, et al. ST-segment elevation in patients with Covid-19 — a case series. N Eng J Med. 2020. DOI: 10.1056/nejmc2009020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mahmud E, Dauerman HL, Welt FG, et al. Management of acute myocardial infarction during the COVID-19 pandemic. J Am Coll Cardiol. 2020. DOI: 10.1016/j.jacc.2020.04.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2013;61:e78–140. [DOI] [PubMed] [Google Scholar]
- 24.Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360:2165–2175. [DOI] [PubMed] [Google Scholar]
- 25.Roe MT, Armstrong PW, Fox KAA. et al.; TRIOLOGY ACS Investigators . Prasugrel versus clopidogrel for acute coronary syndrome without revascularization. N Eng J Med. 2012;367:1297–1309. [DOI] [PubMed] [Google Scholar]
- 26.Buch P, Friberg J, Scharling H, et al. Reduced lung function and risk of atrial fibrillation in the Copenhagen city heart study. Eur Respir J. 2003;21:1012–1016. [DOI] [PubMed] [Google Scholar]
- 27.Mortensen E, Metersky M, Atuegwu N, et al. New onset atrial fibrillation in patients hospitalized with pneumonia. Eur Respir J. 2019;54:OA3307. [Google Scholar]
- 28.January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. Circulation. 2019;140:e125–e151. [DOI] [PubMed] [Google Scholar]
- 29.Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. [DOI] [PubMed] [Google Scholar]
- 30.Patel MR, Mahaffey KW, Garrg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2010;365:883–891. [DOI] [PubMed] [Google Scholar]
- 31.Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–992. [DOI] [PubMed] [Google Scholar]
- 32.Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–2104. [DOI] [PubMed] [Google Scholar]
- 33.Doherty JU, Gluckman TJ, Hucker WJ, et al. 2017 ACC expert consensus decision pathway for periprocedural management of anticoagulation in patients with nonvalvular atrial fibrillation. J Am Coll Cardiol. 2017;69:871–898. [DOI] [PubMed] [Google Scholar]
- 34.Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med. 2015;373:823–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tomaselli GF, Mahaffey KW, Cuker A, et al. 2017 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American College of Cardiology Task Force on expert consensus decision pathways. J Am Coll Cardiol. 2017;70:3042–3067. [DOI] [PubMed] [Google Scholar]
- 36.Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014;63:e57–185. [DOI] [PubMed] [Google Scholar]
- 37.Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;70:252–289. [DOI] [PubMed] [Google Scholar]
- 38.Whitlock RP, Sun JC, Fremes SE, et al. Antithrombotic and thrombolytic therapy for valvular disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:e576s–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Eikelbloom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Eng J Med. 2013;369:1206–1214. [DOI] [PubMed] [Google Scholar]
- 40.Douketis JD, Spyropoulos AC, Spencer FA, et al. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Erratum. Chest. 2012;141:e326S–350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Powers SJ, Green AJ, Josephson A. The spectrum of neurologic disease in the severe acute respiratory syndrome coronavirus 2 pandemic infection. JAMA Neurol. 2020. DOI: 10.1001/jamaneurol.2020.1065 [DOI] [PubMed] [Google Scholar]
- 42.Li Y, Wang M. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study. SSRN Electron J. 2020. DOI: 10.2139/ssrn.3550025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Mao L, Wang M, Chen S, et al. Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. SSRN Electron J. 2020. DOI: 10.2139/ssrn.3544840 [DOI] [Google Scholar]
- 44.On Temporary emergency guidance to US stroke centers during the COVID-19 pandemic. Stroke. 2020. DOI: 10.1161/strokeaha.120.030023 [DOI] [Google Scholar]
- 45.Helms J. Correspondence: neurologic features insSevere SARS-CoV-2 infection. N Engl J Med. 2020. DOI: 10.1056/NEJMc2008597 [DOI] [PubMed] [Google Scholar]
- 46.Jin H, Hong C, Chen S, et al. Consensus for prevention and management of coronavirus disease 2019 (COVID-19) for neurologists. Stroke Vasc Neurol. 2020:svn-2020-000382. DOI: 10.1136/svn-2020-000382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hart RG, Sharma M, Mundl H, et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N Engl J Med. 2018;378:2191–2201. [DOI] [PubMed] [Google Scholar]
- 48.Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. [DOI] [PubMed] [Google Scholar]
- 49.Chimowitz MI, Lynn MJ, Derdeyn CP, et al. Stenting versus aggressive medical therapy for intracranial arterial stenosis. N Engl J Med. 2011;365:993–1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. N Engl J Med. 2018;379:215–225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Zhang Y, Ziao M, Zhang S, et al. Coagulopathy and antiphospholipid antibodies in patients with COVID-19. N Engl J Med. 2020;382(17):e38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2017;123:e686–e725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Creager MA, Belkin M, Bluth EI, et al. 2012 ACCF/AHA/ACR/SCAI/SIR/STS/SVM/SVN/SVS key data elements and definitions for peripheral artherosclerotic vascular disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on clinical data standards (Writing committee to develop clinical data standards for peripheral atherosclerotic vascular disease). Circulation. 2012;125:395–467. [DOI] [PubMed] [Google Scholar]
- 54.Bellosta R, Luzzani L, Natalini G, et al. Acute limb ischemia in patients with COVID-19 pneumonia. J Vasc Surg. 2020. [EPub ahead of print]. DOI: 10.1016/j.jvs.2020.04.483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Perini P, Nabulsi B, Massoni CB, et al. Acute limb ischemia in two young, non-atherosclerotic patients with COVID-19. Lancet. 2020;395(10236):1546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Yan Z, Wei C, Meng X, et al. Clinical and coagulation characteristics of 7 patients with critical COVID-19 pneumonia and acro-ischemia. Chin J Haemtol. 2020;44. [Epub ahead of print]. DOI: 10.3760/cma.j..0253-2727.2020.0006 [DOI] [Google Scholar]
- 57.Cui S, Chen S, Li X, et al. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J Thromb Haemost;2020. Accepted Author Manuscript. DOI: 10.1111/jth.14830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020. DOI: 10.1016/j.thromres.2020.04.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Becattini C, Agnelli G, Lankeit M, et al. Acute pulmonary embolism: mortality prediction by the 2014 European Society of Cardiology risk stratification model. E Respir J. 2016;48:780–786. [DOI] [PubMed] [Google Scholar]
- 60.Konstantinides SV, Meyer G, Bacttini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41:543–603. [DOI] [PubMed] [Google Scholar]
- 61.Rosovsky R, Zhao K, Sista A, et al. Pulmonary embolism response teams: purpose, evidence for efficacy, and future research directions. Res Pract Thromb Haemost. 2019;3:315–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kearon C, Akl EA, Orenals J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. CHEST. 2016;149(2):315–352. [DOI] [PubMed] [Google Scholar]
- 63.Meyer G, Vicaut E, Danays T, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402–1411. [DOI] [PubMed] [Google Scholar]
- 64.Giri J, Sista AK, Weinberg I, et al. Interventional therapies for acute pulmonary embolism: current status and principles for the development of novel evidence: a scientific statement from the American Heart Association. Circulation. 2019;140:e774–e801. [DOI] [PubMed] [Google Scholar]
- 65.Aujesky D, Obrosky DS, Stone RA, et al. Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med. 2005;172(8):1041–1046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Bova C, Sanchez O, Prandoni P, et al. Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur Respir J. 2014;44:694–703. [DOI] [PubMed] [Google Scholar]
- 67.Witt DM, Bieuwlaat R, Clark NP, et al. American society of heamtology 2018 guidelines for management of venous thromboembolism: optimal management of anticoagulation therapy. Blood Adv. 2018;2:3257–3291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788–1830. [DOI] [PubMed] [Google Scholar]
- 69.Levi M, Thachil J, Iba T, et al. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Hematol. 2020. May 11. [Published online]. DOI: 10.1016/S2352-3026(20)30145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Helms J, Tacquard C, Severac F, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020. [Un-edited accepted proof]. DOI: 10.1007/s00134-020-06062-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Schünemann HJ, Cushman M, Burnett AE, et al. American society of hematology 2018 guidelines for management of venous thromboembolism: prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018;2(22):3198–3225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Kahn SR, Lim W, Dunn AS, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141:e195S- e226S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Yin S, Huang M, Li D, et al. Difference of coagulation features between severe pneumonia induced by SARS-CoV2 and non-SARS-CoV2. J Thromb Thrombolysis. 2020. DOI: 10.1007/s11239-020-02105-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Tang N, Bai H, Chen X, et al. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020;18(5):1094–1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Paranjjpe I, Fuster V, Lala A, et al. Association of treatment dose anticoagulation with in-hospital survival among hospitalized patients with COVID-19. J Am Coll Cardiol. 2020. [Epub ahead of print]. DOI: 10.1016/j.jacc.2020.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Dentali F, Mumoli N, Prisco D, et al. Efficacy and safety of extended thromboprophylaxis for medically ill patients. A meta-analysis of randomised controlled trials. Thromb Haemost. 2017;117:606–617. [DOI] [PubMed] [Google Scholar]
- 77.Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153:8–18. [DOI] [PubMed] [Google Scholar]
- 78.Cohen AT, Harrington RA, Goldhaber SZ, et al. Extended thromboprophylaxis with betrixaban in acutely Ill medical patients. N Engl J Med. 2016;375:534–544. [DOI] [PubMed] [Google Scholar]
- 79.Cohen AT, Spiro TE, Buller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368:513–523. [DOI] [PubMed] [Google Scholar]
- 80.Mahan CE, Burnett AE, Fletcher ML, et al. Extended thromboprophylaxis in the acutely ill medical patient after hospitalization – a paradigm shift in post-discharge thromboprophylaxis. Hosp Pract. 2018;46:1, 5–15. [DOI] [PubMed] [Google Scholar]
- 81.Gibson CM, Spyropoulos AC, Cohen AT, et al. The IMPROVEDD VTE risk score: incorporation of D-Dimer into the IMPROVE score to improve venous thromboembolism risk stratification. TH Open. 2017;1(1):e56–e65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Rosenberg DJ, Press A, Fishbein J, et al. External validation of the IMPROVE bleeding risk assessment model in medical patients. Thromb Haemost. 2016;116(3):530–536. [DOI] [PubMed] [Google Scholar]
- 83.Hostler DC, Marx ES, Moores LK, et al. Validation of the international medical prevention registry on venous thromboembolism bleeding risk score. Chest. 2016;149(2):372–379. [DOI] [PubMed] [Google Scholar]
- 84.Hunt BJ. Bleeding and coagulopathies in critical care. N Engl J Med. 2014;370:847–859. [DOI] [PubMed] [Google Scholar]
- 85.Tang N, Li D, Wang X, et al. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844–847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort. Lancet. 2020;395:1054–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Thachil J, Tang N, Gando S, et al. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J Thromb Haemost. 2020;18:1023–1026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Levi M, Toh CH, Thachil J, et al. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British committee for standards in haematology. Br J Haematol. 2009;145:24–33. [DOI] [PubMed] [Google Scholar]
- 90.Sanders JM, Monogue ML, Jodlowski TZ, et al. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. 2020. [Published online]. DOI: 10.1001/jama.2020.6019. [DOI] [PubMed] [Google Scholar]
- 91.Cao B, Wang Y, Wen D, et al. A trial of lopinavir-ritonavir in adults hospitalized with severe Covid-19. N Eng J Med. 2020;382(19):1787–1799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Prescribing information. Brilinta (ticagrelor). Wilmington, DE. AstraZeneca LP, 07/2011.
- 93.Marsousi N, Dalli Y, Fontana P, et al. Impact of booster antiretroviral therapy on the pharmacokinetics and efficacy of clopidogrel and prasugrel active metabolites. Clin Pharmacokinetic. 2018;57:1347–1354. [DOI] [PubMed] [Google Scholar]
- 94.Wiggins BS, Dixon DL, Neyens RR, et al. Select drug-drug interactions with direct oral anticoagulants: JACC review topic of the week. J Am Coll Cardiol. 2020;75:1341–1350. [DOI] [PubMed] [Google Scholar]
- 95.Steffel J, Verhamme P, Potpara TS, et al. The 2018 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. EHJ. 2018;39:1330–1393. [DOI] [PubMed] [Google Scholar]