

Abstract
Objectives:
To determine the proportion of well-appearing newborns screened for hypoglycemia; yield of specific screening criteria; and impact of screening on breastfeeding.
Study Design:
Retrospective study of well-appearing at-risk infants born ≥36 weeks’ gestation with blood glucose measurements obtained ≤72 hours of age.
Results:
Of 10,533 eligible well newborns, 48.7% were screened for hypoglycemia. Among tested infants, blood glucose <50 mg/dL occurred in 43% and 4.6% required intensive care for hypoglycemia. Blood glucose <50 mg/dL was associated with lower rates of exclusive breastfeeding (22% versus 65%, p <0.001). Infants screened due to late preterm birth were most frequently identified as hypoglycemic; the fewest abnormal values occurred among appropriate-weight, late term infants of non-diabetic mothers.
Conclusion:
Hypoglycemia risk criteria result in screening a large proportion of otherwise well newborns and negatively impact rates of exclusive breastfeeding. The risks and benefits of hypoglycemia screening recommendations should be urgently addressed.
INTRODUCTION
Screening for neonatal hypoglycemia is a common part of the care provided for otherwise well-appearing newborns. Based on American Academy of Pediatrics (AAP) recommendations, it has been estimated that ~30% of infants born >35 weeks’ gestation will be eligible for screening (1,2). Guidelines provided by the Pediatric Endocrine Society (PES) and the Academy of Breastfeeding Medicine include more at-risk criteria and would likely result in greater frequency of screening (3,4). Several criteria for an effective screening program, as developed for newborn state screening (5), remain controversial with respect to hypoglycemia screening. There is a lack of consensus regarding both risk criteria for screening and the threshold glucose levels that should define hypoglycemia and warrant intervention (6-8). Furthermore, a robust understanding is lacking with respect to the natural history of asymptomatic hypoglycemia, the implications of treating asymptomatic hypoglycemia among otherwise well term infants, and the impact of treatment on short and long-term outcomes (8). Despite existing uncertainties, neonatal providers are tasked with creating local protocols that establish standard of care at their respective institutions.
Quantifying the intended and unintended consequences of hypoglycemia screening is the first step in understanding the risk-benefit balance of this practice. In this study, we determined the frequency of hypoglycemia screening prompted by our local protocol; the proportion of infants who met specific thresholds for hypoglycemia in different risk groups; the proportion of initially well-appearing infants who required transfer to the neonatal intensive care unit (NICU) for hypoglycemia treatment; and the proportion of infants whose feeding was impacted by hypoglycemia screening and detection. We further explored how different definitions for at-risk weight-for-gestation impacted the number of infants identified for hypoglycemia screening.
METHODS
Study Design and Population:
This was a single center retrospective cohort study. Study infants were born from 01/01/2013 – 7/31/2015 with gestational age (GA) ≥36 0/7 weeks, birth weight (BW) ≥2,000 grams and admitted from the labor floor to postpartum floor for well newborn care. In our center, well newborns room-in with their mothers after birth. Infants admitted directly to the NICU for any reason were excluded. The study was approved by the Institutional Review Board at the University of Pennsylvania.
Setting:
Pennsylvania Hospital is the largest maternity center in Philadelphia, Pennsylvania with ~5,000 annual deliveries; an active high-risk maternal-fetal medicine service; and a 50-bed Level III NICU. Well-baby care is provided by in-house neonatology staff for ~80% of the infants and by community pediatricians for the remaining infants. The hospital was designated as a Baby-Friendly® Hospital in December 2015.
Hypoglycemia screening among well-babies:
Blood glucose (BG) was measured using point-of-care testing with Accu-check Inform II (Roche Diagnostics®, Germany) and was performed by postpartum nurses based on a local policy. Risk criteria for hypoglycemia screening included: BW <2,500 grams or ≥4,000 grams, BW <2,800 grams and GA ≥38 0/7 weeks (added July 2014), GA 36 0/7-6/7 weeks (late preterm), ≥41 0/7 weeks, infant of a pre-gestational or gestational diabetic mother, in-utero exposure to terbutaline or beta-blocker medications (9), or symptoms concerning for hypoglycemia (e.g. hypothermia, tachypnea or jitteriness). Standard newborn policy included skin-to-skin care and breastfeeding within 1 hour of birth. The BG screening schedule at minimum included: BG obtained 30 minutes after the first feed for all at-risk infants (within 2 hours after birth); and one additional pre-prandial BG. Infants with BW <2,500 grams, infants of diabetic mothers and late preterm infants underwent an extended screening evaluation that included BG tests every 12 hours until 36 hours of age. If the BG was lower than the appropriate threshold for age, it was checked prior to every feed until 2 normal BG values resulted. BG values included in the study were restricted to those obtained in the first 72 hours after birth.
Hypoglycemia definition and intervention:
The BG threshold for diagnosing hypoglycemia was <50 mg/dL. After 7/2014, the threshold was changed to <45 mg/dL at <4 hours of age and <50 mg/dL thereafter (10) to avoid capturing infants in the physiological nadir just after birth (1). The primary intervention for hypoglycemia was feeding as per mother’s choice (feeding at breast, feeding expressed breast milk, or feeding 15-20 ml of formula). For breastfeeding dyads, formula feeding was only recommended if hypoglycemia persisted despite breastmilk feeding. Mothers of infants receiving supplementation routinely received additional lactation support and were encouraged to pump or manually express breastmilk. If the BG was <20 mg/dL after feeding, or if hypoglycemia persisted despite two feedings, infants were transferred to the NICU for further evaluation and intravenous dextrose therapy.
Definitions for at-risk weight-for-gestation:
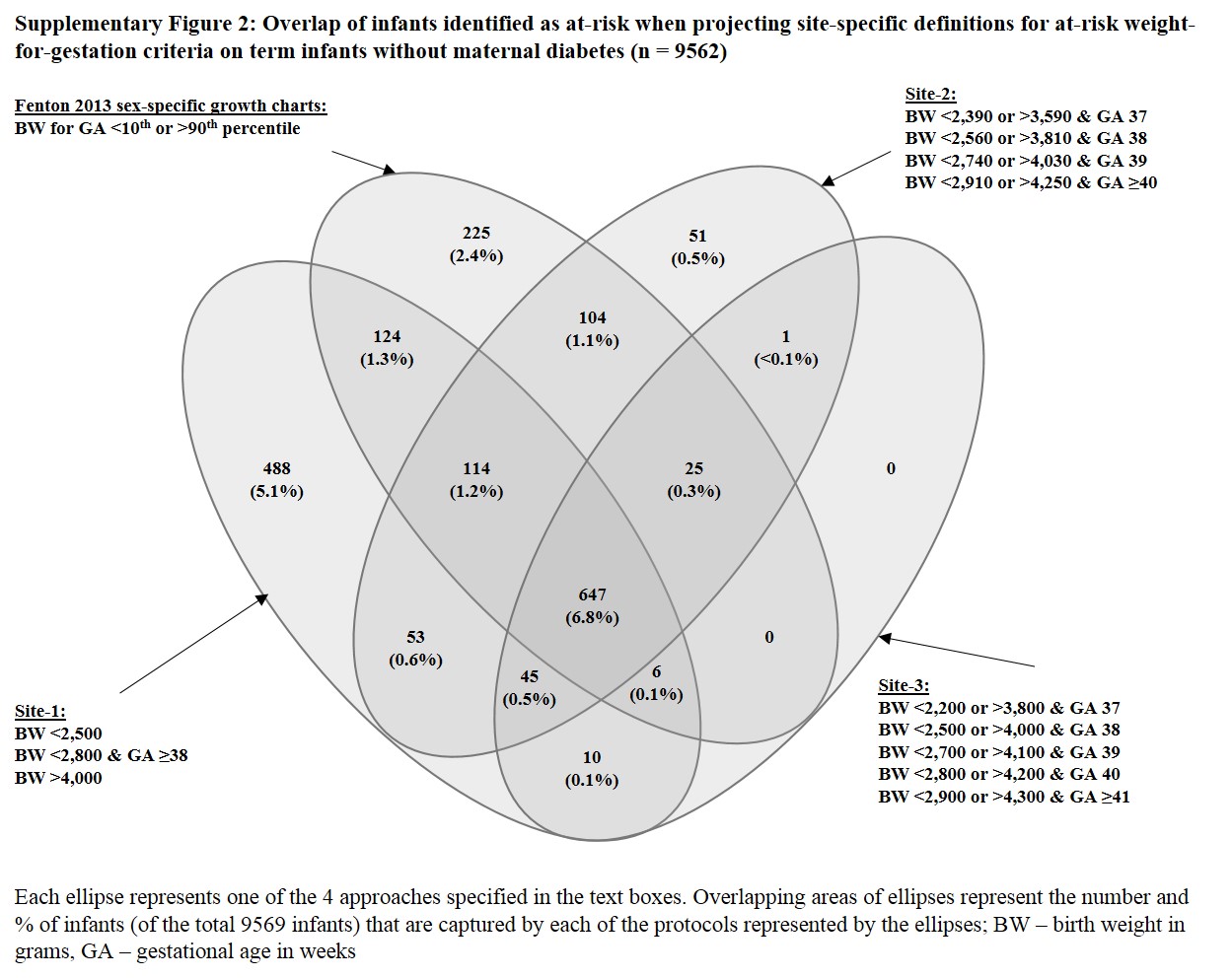
To explore the impact of different weight-for-gestation criteria used for hypoglycemia screening, we restricted the study cohort to infants born ≥37 weeks’ gestation to mothers without diabetes. We then applied definitions to identify at-risk infants for hypoglycemia screening used by three academic birth centers: Pennsylvania Hospital (Site-1), Massachusetts General Hospital, Boston, MA (Site-2) and Oregon Health and Science University, Portland, OR (Site-3) (Supplementary Table 1). Additionally, we applied the 10th and 90th percentile of weight-for-gestation from the 2013 Fenton growth charts (https://www.peditools.org/fenton2013/index.php), to identify infants who would meet criteria of small- and large-for-gestation when using sex-specific growth charts.
Data sources:
Clinical and laboratory data were obtained from electronic medical records captured by hospital databases. Mother’s preference for feeding infant at admission and newborn feeding data were obtained by manual chart review of 1,119 randomly-selected infants (10.6% of the study cohort) using the following strata: 557 (25%) infants from those who were screened for hypoglycemia and had at least one BG <50 mg/dL, 292 (10%) infants from those who were screened for hypoglycemia but had no BG <50 mg/dL, and 270 (5%) infants from those who were not screened for hypoglycemia. Data from these infants were then extrapolated to the respective strata to determine feeding intent at admission and feeding type at discharge.
Data analysis:
Proportion, mean or median are presented as appropriate for describing frequency of screening, results and clinical outcomes. Comparisons between groups were assessed by using χ2 tests for categorical variables, and t tests or the Mann-Whitney test for continuous variables. A p-value <0.05 was considered statistically significant. All data analyses were conducted using Stata 14 (StataCorp, College Station, TX).
RESULTS
Indications and outcomes of hypoglycemia screening:
During the study period, 11,285 infants were born with GA ≥36 0/7 weeks and BW ≥2,000 grams. After excluding 752 infants admitted to the NICU immediately after birth, 10,533 infants remained with their mothers and were included in the study (Supplementary Figure 1). Of these infants, 5,140 (48.8%), had a BG test in the first 72 hours after birth with 4,718 (91.8%) infants tested within 4 hours of birth. A total of 23,463 BG tests were reported with a median of 3 tests per infants (interquartile range 2-5). NICU admission from the postpartum floors occurred in 529 infants; 235 (4.6%) admissions were for hypoglycemia management and 294 (5.7%) admissions were for other reasons. Prevalence of risk criteria and comparison between screened and unscreened infants are shown in Table 1. Other than the risk criteria of “BW <2,800 grams and GA ≥38 weeks”, which was added to the protocol later in the study period (July 2014), 99% of infants meeting criteria for hypoglycemia screening had a BG recorded. Screened infants were more likely to be delivered by cesarean section or to be born to mothers of black race, with high body mass index or with the diagnosis of hypertension.
Table 1.
Maternal and infant characteristics for study infants
| Characteristic, n (%) | Total n = 10,533 |
BG obtained n = 5,140 |
No BG obtained1 n = 5,393 |
p-value |
|---|---|---|---|---|
| Maternal age ≥35 years | 2,316 (22.0) | 1,182 (23.0) | 1,134 (21.0) | 0.02 |
| Race | ||||
| • Black | 3,141 (29.8) | 1,704 (33.2) | 1,437 (26.6) | <0.001 |
| • White | 4,843 (46.0) | 2,224 (43.3) | 2,619 (48.6) | |
| • Other | 2,549 (24.2) | 1,212 (23.6) | 1,337 (24.8) | |
| Maternal Hypertension | 822 (7.8) | 462 (9.0) | 360 (6.7) | <0.001 |
| Maternal Body Mass Index | ||||
| • <25 | 1,196 (11.4) | 550 (10.7) | 646 (12.0) | <0.001 |
| • 25 to <30 | 3,582 (34.0) | 1,608 (31.3) | 1,974 (36.6) | |
| • ≥30 | 4,467 (42.4) | 2,286 (44.5) | 2,181 (40.4) | |
| • Undocumented | 1,288 (12.2) | 696 (13.5) | 592 (11.0) | |
| Cesarean section | 3,438 (32.6) | 1,989 (38.7) | 1,449 (26.9) | <0.001 |
| Male | 5,358 (50.9) | 2,823 (54.9) | 2,535 (47.0) | <0.001 |
| NICU admissions (all indications) | 549 (5.2) | 529 (10.3) | 20 (0.4) | <0.001 |
| Frequency of hypoglycemia risk criteria | ||||
| BW <2,500 grams | 372 (3.5) | 368 (7.2) | 4 (0.1) | <0.001 |
| BW <2,800 grams and GA ≥38 0/7 weeks2 | 520 (4.9) | 335 (6.5) | 185 (3.4) | <0.001 |
| BW >4,000 grams | 854 (8.1) | 852 (16.6) | 2 (0.04) | <0.001 |
| GA (weeks) | ||||
| • 36 0/7 to 36 6/7 | 368 (3.5) | 363 (7.1) | 5 (0.1) | <0.001 |
| • 37 0/7 to 40 6/7 | 9,134 (86.7) | 3,767 (73.3) | 5,367 (99.5) | |
| • ≥41 0/7 | 1,031 (9.8) | 1,010 (19.6) | 21 (0.4) | |
| Maternal Diabetes | 621 (5.9) | 613 (11.9) | 8 (0.1) | <0.001 |
No BG obtained contains 53 infants with BG obtained after 72 hours of age
Excludes infants with BW <2,500 grams. Risk criteria added in 2014; BG – blood glucose, BW – birth weight, GA – gestational age, NICU – neonatal intensive care unit
We found male infants significantly more likely to be screened. To explore this further, we stratified risk factors by sex (Table 2). While overall BW criteria identify ~22% of both male and female infants, male infants were more likely to meet criteria of BW ≥4,000 grams as compared to female infants [384/2,823 (13.6%) vs 189/2,317 (8.2%), p <0.001], and female infants were more likely to meet criteria for BW <2,500 grams [315/2,317 (13.5%) vs 224/2,823 (7.9%), p <0.001]. More male infants were screened for other indications.
Table 2.
Distribution of risk criteria among male and female screened infants (n = 5,140)
| Risk categories | Male n = 2,823 |
Female n = 2,317 |
p-value |
|---|---|---|---|
| Non-overlapping risk categories, n (%) | |||
| Maternal Diabetes | 333 (11.8) | 280 (12.1) | 0.06 |
| GA criteria for infants of non-diabetic mothers | 691 (24.5) | 633 (27.3) | |
| BW criteria for term infants of non-diabetic mothers | 608 (21.5) | 504 (21.8) | |
| Term infants of non-diabetic mothers with appropriate BW | 1,191 (42.2) | 900 (38.8) | |
| Individual risk categories, n (%) | |||
| Maternal Diabetes | 333 (11.8) | 280 (12.1) | 0.75 |
| GA criteria for infants of non-diabetic mothers | 691 (24.5) | 633 (27.3) | 0.02 |
| • 36 0/7 to 36 6/7 weeks | 171/691 (24.7) | 167/633 (26.4) | 0.40 |
| • ≥41 0/7 weeks | 520/691 (75.3) | 466/633 (73.6) | |
| BW criteria for term infants of non-diabetic mothers | 608 (21.5) | 504 (21.8) | 0.85 |
| • BW <2,500 grams or <2,800 grams and GA ≥38 0/7 weeks | 224/608 (36.8) | 315/504 (62.5) | <0.001 |
| • BW ≥4,000 grams | 384/608 (63.2) | 189/504 (37.5) | |
| Term infants of non-diabetic mothers with appropriate BW | 1,191 (42.2) | 900 (38.8) | 0.02 |
BW – birth weight, GA – gestational age
Table 3 shows the distribution of risk factors among infants who were screened, the severity of hypoglycemia based on lowest BG, and proportion requiring NICU admission for hypoglycemia. Infants of diabetic mothers compared to infants without maternal diabetes were more likely to have BG <50 mg/dL (52.2% vs. 42.1%, p <0.001) and require NICU admission for hypoglycemia management (9.5% vs. 3.9%, p <0.001). Among infants born to non-diabetic mothers, those born at 36 weeks were more likely than those born 37-41 weeks to require NICU admission for hypoglycemia (10.4% vs. 3.4%, p <0.001). Among all infants, the highest proportion of screened infants (19.9%) consisted of those born at 37 0/7 – 40 6/7 weeks with appropriate birthweight and non-diabetic mothers. These infants were screened due to maternal terbutaline or beta-blocker administration or non-specific physical exam abnormalities (e.g., hypothermia, jitteriness), and had the smallest proportion (2.5%) of infants requiring NICU admission for hypoglycemia treatment. Details of infants admitted to the NICU are shown in Supplementary Table 2. None of the infants admitted to NICU for hypoglycemia had seizures or apnea. Most admitted received IV dextrose (75%) for an average duration of 41 hours and remained in the NICU for a median of 2 days. Six infants were diagnosed with a cause for hypoglycemia other than transitional physiology (3 attributed to underlying syndrome and 3 with suspected persistent hyperinsulinism).
Table 3.
Indications and outcomes of hypoglycemia screening among study infants
| Risk Categories | Screened, n | Lowest BG obtained1, n (%) | NICU transfer1, n (%) | ||
|---|---|---|---|---|---|
| All BG ≥50 mg/dL | BG 36-49 mg/dL | BG ≤35 mg/dL | |||
| Infants born to women without diabetes and GA 36 0/7 to 36 6/7 weeks | |||||
| BW <2,500 grams | 112 | 28 (25.0) | 64 (57.1) | 20 (17.9) | 15 (13.4) |
| BW ≥2,500 grams | 226 | 73 (32.3) | 126 (55.8) | 27 (11.9) | 20 (8.8) |
| Infants born to women without diabetes and GA 37 0/7 to 40 6/7 weeks | |||||
| BW <2,500 grams, or BW <2,800 grams and GA ≥38 0/7 weeks | 539 | 253 (46.9) | 240 (44.5) | 46 (8.5) | 32 (5.9) |
| Appropriate BW | 2,091 | 1,312 (62.7) | 659 (31.5) | 120 (5.7) | 52 (2.5) |
| • Maternal terbutaline/beta-blocker | 144 | 84 (58.3) | 49 (34.1) | 11 (7.6) | 4 (2.8) |
| BW ≥4,000 grams | 573 | 304 (53.1) | 213 (37.2) | 56 (9.8) | 28 (4.9) |
| Infants born to women without diabetes and GA ≥41 0/7 weeks | |||||
| BW <2,800 grams | 10 | 6 (60.0) | 3 (30.0) | 1 (10.0) | 1 (10.0) |
| Appropriate BW | 788 | 527 (66.9) | 221 (28.0) | 40 (5.1) | 22 (2.8) |
| BW ≥4,000 grams | 188 | 118 (62.8) | 61 (32.4) | 9 (4.8) | 7 (3.7) |
| Infants born to women with diabetes and GA 36 0/7 to 36 6/7 weeks | |||||
| BW <2,500 grams | 3 | 1 (33.3) | 2 (66.7) | 0 | 1 (33.3%) |
| BW ≥2,500 grams | 22 | 6 (27.2) | 8 (36.4) | 8 (36.4) | 3 (13.6) |
| Infants born to women with diabetes and GA 37 0/7 to 40 6/7 weeks | |||||
| BW <2,500 grams, or BW <2,800 grams and GA ≥38 0/7 weeks | 39 | 19 (48.7) | 14 (35.9) | 6 (15.4) | 5 (12.8) |
| Appropriate BW | 445 | 223 (50.1) | 171 (38.4) | 51 (11.5) | 35 (7.9) |
| BW ≥4,000 grams | 80 | 28 (35.0) | 38 (47.5) | 14 (17.5) | 14 (17.5) |
| Infants born to women with diabetes and GA ≥41 0/7 weeks2 | |||||
| Appropriate BW | 15 | 8 (53.3) | 6 (40.0) | 1 (6.7) | 0 |
| BW ≥4,000 grams | 9 | 8 (88.9) | 1 (11.1) | 0 | 0 |
| Total | 5,140 | 2,914 (56.7) | 1,827 (35.5) | 399 (7.8) | 235 (4.6) |
Percentages represent frequency of infants per total screened infants in each risk category (row percentages)
No infants with low birth weight and GA over 41 weeks were identified among diabetic mothers; BG – blood glucose, BW – birth weight, GA – gestational age, NICU – neonatal intensive care unit
Impact of hypoglycemia screening on infant feeding during hospitalization:
We extrapolated feeding data obtained for a random sample of 1,119 infants to the full study cohort, to assess the impact of hypoglycemia screening and management on newborn feeding (Table 4). Maternal feeding intention differed between those whose infants were screened and those whose infants were not screened. Among mothers who planned to breastfeed exclusively, infant BG <50 mg/dL was significantly associated with formula supplementation (22.6% vs. 65.5%, p <0.001). Among mothers who planned to breastfeed exclusively, infants who had all BG ≥50 mg/dL were also more likely to be fed with formula compared to unscreened infants (56% vs 65%, p <0.001).
Table 4.
Feeding choices and outcome in infants categorized by hypoglycemia screening and results1
| Group 1 Lowest BG <50 mg/dL |
Group 2 Lowest BG ≥50 mg/dL |
Group 3 No BG obtained |
p-value 1 vs 3 |
p-value 1 vs 2 |
p-value 2 vs 3 |
|
|---|---|---|---|---|---|---|
| Maternal feeding intention at admission, n |
2,226 | 2,914 | 5,393 | |||
| Breastfeed2, n (%) | 1,606 (72.1) | 2,156 (74.0) | 4,056 (75.2) | 0.01 | 0.001 | 0.04 |
| Formula feed, n (%) | 324 (14.6) | 468 (16.1) | 759 (14.1) | |||
| Both, n (%) | 244 (11.0) | 250 (8.6) | 478 (8.9) | |||
| Undocumented, n (%) | 52 (2.3) | 40 (1.4) | 100 (1.9) | |||
| Mothers with intention to exclusively breastfeed2, n |
1,606 | 2,156 | 4,056 | |||
| In-hospital infant feeds | ||||||
| Breastfed exclusively, n (%) | 363 (22.6) | 1,208 (56.0) | 2,658 (65.5) | <0.001 | <0.001 | <0.001 |
| Any formula use, n (%) | 1,203 (74.9) | 888 (41.2) | 1,278 (31.5) | |||
| Undocumented, n (%) | 40 (2.5) | 60 (2.8) | 120 (3.0) |
Data obtained in a random sub-sample of 1,119 infants and extrapolated to full cohort
Comparing proportion of women planning to exclusively breastfeed vs. any other mode of feed across the 3 groups presents the following p values: Group 1 vs. 3: 0.005, Group 1 vs. 2: 0.14, Group 2 vs. 3: 0.22; BG – blood glucose
Impact of different weight-for-gestation screening criteria:
For this comparison we included 9,569 infants from the study cohort who were born ≥37 0/7 weeks’ gestation to non-diabetic mothers. The weight-for-gestation criteria used for screening at three birth centers (Supplementary Table 1) and sex-specific <10th and >90th weight-for-gestation percentiles from Fenton charts were applied to these infants. The four approaches identified different infants for screening (Supplementary Figure 2). Site-1 criteria would identify the largest number of infants as at-risk (1,487, 15.5%), followed by Fenton chart percentiles (1,245, 13.0%), Site-2 (1,040, 10.9%) and Site-3 (734, 7.7%). Overall, 1,893 (19.8%) infants would be identified for screening by at least one approach and 647 (6.8%) infants by all four approaches. Infants identified for screening by only one approach but not by the others were: Site-1 (488, 5.1%), Fenton charts (225, 2.4%) and Site-2 (51, 0.5%). All infants screened at Site 3 would be captured by at least one of the other approaches.
DISCUSSION
At our high-risk maternity center, we found that screening for risk of hypoglycemia had a significant and potentially negative impact on a large proportion of otherwise well-appearing newborns. Nearly half of all newborns healthy enough at birth to room-in with their mothers were screened for hypoglycemia in the first 72 hours after birth. Identification of hypoglycemia as well as the process of screening itself was associated with increased formula feeding and decreased exclusive breastfeeding. Furthermore, we found that local variation in the definitions of small-for-gestational age and large-for-gestational age could lead to substantial differences in which newborns were tested for hypoglycemia. This study raises two immediate clinical questions. First, can we safely screen fewer infants? Second, can we address the unintended negative impact on breastfeeding identified in this study?
Screening fewer infants may be addressed by altering the criteria for screening. Although the risk factors for hypoglycemia screening differ among national recommendations (1,3,4), every risk category in our local protocol resulted in the identification of some infants who met thresholds for hypoglycemia and some infants who required transfer to the NICU for persistent hypoglycemia. However, we observed that the “efficiency” of risk categories varied (Table 3). More than half of the infants screened for late preterm gestation and maternal diabetes had at least one BG <50 mg/dL and ~10% required NICU admission. In contrast, infants screened for gestation ≥41 0/7 weeks with appropriate weight-for-gestation and infants born 37 0/7 – 40 6/7 weeks with appropriate weight-for-gestation, screened due to maternal beta-blocker exposures or clinical symptoms, yielded many fewer infants with low BG results. The PES (but not AAP) recommends screening for post term infants (1,3). By local consensus, our center defines this as infants born after 41 0/7 weeks (rather than 42 0/7 weeks) gestation. If the 757 infants who were born at ≥41 0/7 −41 6/7 weeks without additional risk factors were eliminated from our local screening criteria, the rate of screening among well-appearing infants would decline from 48.8% to 41.6%. Term infants screened on the basis of in-utero maternal medication exposure, or symptoms suspicious for hypoglycemia, comprised the largest screened group. The majority of these infants have all BG ≥50 mg/dL, although 2.5% of these infants ultimately required NICU admission for persistent hypoglycemia. It remains unclear whether the small proportion of infants in each of these risk categories who were identified as hypoglycemic – including the 2-3% that ultimately required NICU admission for persistent hypoglycemia - would still be identified, or harmed from lack of identification and treatment.
We found that male infants were more frequently identified as at-risk for hypoglycemia per our local protocol (Tables 1 and 2). This difference was largely driven by the greater number of male term infants screened for clinical symptoms. Male infants have greater prevalence of morbidity and mortality than female infants (11), and our finding of a higher testing prevalence in male infants may simply represent a greater frequency of clinical instability. Notably, more male infants at our center met the criteria of BW ≥4,000 grams, unsurprisingly as male infants are larger than female infants of the same gestation on sex-specific growth charts (12). Prior studies that identified BW and GA criteria for hypoglycemia did not use sex-specific values (13). We observed that using sex-independent criteria will impact which infants are screened, differentially flagging male and female infants as large or small for GA (Table 2). Although the incidence of hypoglycemia has been reported to vary little with birth weight thresholds compared to the use of growth charts (14), the impact on screening varied 2-fold (7.7-15.5%) (Supplementary Figure 2). Leveraging electronic medical records to consistently identify at-risk infants based on sex-specific growth charts may reduce variation in screening across sites.
In-hospital formula supplementation is a predictor for early breastfeeding cessation with a potential loss of the health benefits associated with exclusive breastfeeding (15,16). Our center supports continued breastfeeding among infants with hypoglycemia, providing breast pumps and lactation consultation as well as instruction in and support for hand-expression, and offers outpatient lactation consultation after hospital discharge. Yet we found that among women with the intention to exclusively breastfeed, only 22% did so when their infant had a BG <50 mg/dL anytime in the first 72 hours of age. Furthermore, hypoglycemia screening itself (in the absence of a BG <50 mg/dL) was associated with a small increase in formula supplementation compared to infants who were not screened (Table 4). Such findings would not surprise our local nursing staff. While hypoglycemia has not consistently been cited as a driver for in-hospital newborn formula supplementation (17-19), a survey of nurses caring for well neonates at our center identified hypoglycemia as a major indication for formula supplementation among breastfeeding dyads (20). Infants screened for hypoglycemia often have other risk factors known to be associated with early breastfeeding cessation, such as maternal obesity and birth by cesarean section (21) (Table 1), that may have contributed to this finding. It is also possible that screening raises concern with the mother that breastfeeding does not provide adequate nutrition to her infant. Identifying dyads at particularly high risk for formula supplementation and concretely addressing the subliminal messaging that may be present in hypoglycemia screening are likely important steps for in-hospital lactation support.
Interventions have been reported that aim to limit formula supplementation for asymptomatic hypoglycemia among breastfeeding dyads. A randomized, placebo-controlled trial of dextrose gel administration for neonatal hypoglycemia found that the use of dextrose gel did not impact the total volume of in-hospital formula use but was associated with lower frequency of formula use and higher rates (87% vs 96%) of exclusive breastfeeding at 2 weeks of age (22). Donor breast milk may also be used to supplement the breastfed newborn with hypoglycemia. Each of these alternative interventions come at a cost (23,24), and it remains unclear whether use of such approaches after birth will result in longer overall duration of breastfeeding after discharge from the birth hospital. As a result of this study, our center now offers mothers the choice of feeding donor milk or formula if mother’s own milk requires supplementation for hypoglycemia (20). The impact of this change is an area of active study.
A final issue that underlies the impact of hypoglycemia screening is the thresholds set for defining hypoglycemia. The level of BG at which intervention should be initiated remains controversial (2,6,8,25-27). Testing modalities are complicated by the frequent use of bedside point-of-care glucometers that are not designed to accurately detect low glucose levels in neonates (28). Table 3 shows a lower proportion of tested infants with a lowest BG <50 mg/dL vs. <36 mg/dL. Such data should be interpreted with caution. As our center policy is to intervene for BG <45-50 mg/dL, we cannot be certain how many more infants would experience lower BG levels if the threshold for intervention were set differently.
Our study provides detailed information on the impact of a common newborn screening practice as implemented at a single large maternity center. The study data may inform consideration of the differential yield of individual risk factors for hypoglycemia to assign more individualized risk assessments. Our observations may be broadly applicable as they reflect real-world care rather than care provided in intervention studies. However, it is a limitation that our observations will not be generalizable to centers with substantially different approaches to hypoglycemia screening and management. Further, our study is limited by incomplete information on the symptoms prompting screening and lack of follow-up breastfeeding information after discharge. It should be noted that our center modified our local protocol to define small for gestation criteria among term infants, and to change the threshold for intervention for infants <4 hours of age mid-way through the current study period. We showed previously that this change did not impact the total proportion of infants screened for hypoglycemia (10).
At our center, these results have prompted efforts to use electronic medical records to identify at-risk weight-for-gestation infants using sex-specific growth charts, to promote euthermia during neonatal transition, to require re-warming and feeding prior to BG testing in asymptomatic infants with low temperatures, and finally, to offer donor milk as a feeding option in infants with hypoglycemia-indicated supplementation (20).
The most important question raised by this study is a difficult one: have we done any good offering this medical intervention to nearly half of our well-appearing newborns? Pathological hypoglycemia as occurs in congenital hyperinsulinism or with inborn errors of metabolism can cause severe neurologic morbidity and even mortality (29). The effect of transitional hypoglycemia and the impact of intervening in asymptomatic hypoglycemia are less clear. Associations with school age performance, executive function and visual motor function have been reported in prospective cohort studies but the effect of interventions for transitional hypoglycemia and the thresholds at which such interventions are most protective remain unknown (2,25,27,30). Cornblath et al proposed operational thresholds for hypoglycemia intervention, noting that the optimal blood glucose level for intervention is likely distinct for each individual infant based on their glucose requirements and overall metabolic state (31). They further noted that in the absence of understanding individual needs, “all that can be proposed are pragmatic intervention thresholds that also provide a margin of safety”. We propose that such a ‘margin of safety’ should account for all of the impacts of hypoglycemia screening, including that of maternal-infant separation and impacts on breast feeding.
CONCLUSION
Blood glucose screening impacts a high proportion of newborns and decreases the proportion who are exclusively breastfed, yet key criteria for screening vary. A collaborative endeavor that brings together the expertise of the perinatal providers (including physicians, nurses, and lactation consultants) who take care of the vast number of healthy infants, pediatric endocrinologists who manage the more severe cases of glucose metabolic disorders, and input from parents, is urgently needed to determine the best management of newborn infants while minimizing unnecessary medical intervention.
Supplementary Material
{kind=link}
{kind=link}
Acknowledgments
FUNDING INFORMATION
This study was partly supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development Grant (Number - 1K23HD088753-01A1).
Funding source: Eunice Kennedy Shriver National Institute of Child Health and Human Development (1K23HD088753-01A1)
Abbreviations:
- BW
Birth weight
- GA
Gestational age
- AAP
American Academy of Pediatrics
- PES
Pediatric Endocrine Society
- IQR
Interquartile range
- NICU
Neonatal Intensive Care Unit
- BG
Blood Glucose
Footnotes
CONFLICT OF INTEREST
The authors have no conflicts of interest relevant to this article to disclose.
Supplementary information is available at JPER’s website.
REFERENCES
- (1).Committee on Fetus and Newborn, Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics 2011; 127: 575–579. [DOI] [PubMed] [Google Scholar]
- (2).McKinlay CJ, Alsweiler JM, Ansell JM, Anstice NS, Chase JG, Gamble GD, et al. Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years. N Engl J Med 2015; 373: 1507–1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (3).Thornton PS, Stanley CA, De Leon DD, Harris D, Haymond MW, Hussain K, et al. Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children. J Pediatr 2015; 167: 238–245. [DOI] [PubMed] [Google Scholar]
- (4).Wight N, Marinelli KA, Academy of Breastfeeding Medicine. ABM clinical protocol# 1: guidelines for blood glucose monitoring and treatment of hypoglycemia in term and late-preterm neonates, revised 2014. Breastfeeding Medicine 2014; 9: 173–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (5).Andermann A, Blancquaert I, Beauchamp S, Déry V. Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bull World Health Organ 2008; 86: 317–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (6).Adamkin DH, Polin RA. Imperfect Advice: Neonatal Hypoglycemia. J Pediatr 2016; 176: 195–196. [DOI] [PubMed] [Google Scholar]
- (7).Adamkin DH. Neonatal hypoglycemia. Curr Opin Pediatr 2016; 28: 150–155. [DOI] [PubMed] [Google Scholar]
- (8).Thornton PS. Neonates at risk for hypoglycemia: associated neurological outcomes. J Pediatr 2016; 170: 343–344. [DOI] [PubMed] [Google Scholar]
- (9).Bateman BT, Patorno E, Desai RJ, Seely EW, Mogun H, Maeda A, et al. Late Pregnancy beta Blocker Exposure and Risks of Neonatal Hypoglycemia and Bradycardia. Pediatrics 2016; 138: 10.1542/peds.2016-0731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (10).Dhudasia MB, Mukhopadhyay S, Wade KC, Puopolo KM. Impact of Neonatal Hypoglycemia Screening in the Well Baby Nursery and Trends in Neonatal Intensive Care Unit Admissions. Pediatrics 2018; 142 (1 Meeting Abstract): DOI: 10.1542/peds.142.1_MeetingAbstract.554. [DOI] [Google Scholar]
- (11).Zhao D, Zou L, Lei X, Zhang Y. Gender differences in infant mortality and neonatal morbidity in mixed-gender twins. Scientific reports 2017; 7: 8736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (12).Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC pediatrics 2013; 13: 59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (13).Lubchenco LO, Bard H. Incidence of hypoglycemia in newborn infants classified by birth weight and gestational age. Pediatrics 1971;47: 831–838. [PubMed] [Google Scholar]
- (14).Harris DL, Weston PJ, Harding JE. Incidence of neonatal hypoglycemia in babies identified as at risk. J Pediatr 2012; 161: 787–791. [DOI] [PubMed] [Google Scholar]
- (15).Chantry CJ, Dewey KG, Peerson JM, Wagner EA, Nommsen-Rivers LA. In-hospital formula use increases early breastfeeding cessation among first-time mothers intending to exclusively breastfeed. J Pediatr 2014; 164: 1339–45.e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (16).Ip S, Chung M, Raman G, Chew P, Magula N, DeVine D, et al. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep) 2007; 153: 1–186. [PMC free article] [PubMed] [Google Scholar]
- (17).Gagnon AJ, Leduc G, Waghorn K, Yang H, Platt RW. In-hospital formula supplementation of healthy breastfeeding newborns. J Hum Lact 2005; 21: 397–405. [DOI] [PubMed] [Google Scholar]
- (18).Temple Newhook J, Newhook LA, Midodzi WK, Murphy Goodridge J, Burrage L, Gill N, et al. Determinants of Nonmedically Indicated In-Hospital Supplementation of Infants Whose Birthing Parents Intended to Exclusively Breastfeed. J Hum Lact 2017; 33: 278–284. [DOI] [PubMed] [Google Scholar]
- (19).Kair LR, Flaherman VJ. Donor Milk or Formula: A Qualitative Study of Postpartum Mothers of Healthy Newborns. J Hum Lact 2017; 33: 710–716. [DOI] [PubMed] [Google Scholar]
- (20).Ferrarello D, Froh EB, Hinson TD, Spatz DL. Nurses' Views on Using Pasteurized Donor Human Milk for Hypoglycemic Term Infants. MCN Am J Matern Child Nurs 2019; 44: 157–163. [DOI] [PubMed] [Google Scholar]
- (21).Wojcicki JM. Maternal prepregnancy body mass index and initiation and duration of breastfeeding: a review of the literature. J Womens Health (Larchmt) 2011; 20: 341–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (22).Harris DL, Weston PJ, Signal M, Chase JG, Harding JE. Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): a randomised, double-blind, placebo-controlled trial. Lancet 2013; 382: 2077–2083. [DOI] [PubMed] [Google Scholar]
- (23).Sen S, Benjamin C, Riley J, Heleba A, Drouin K, Gregory K, et al. Donor milk utilization for healthy infants: Experience at a single academic center. Breastfeeding Medicine 2018; 13: 28–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (24).Solimano A, Kwan E, Osiovich H, Dyer R, Elango R. Dextrose gels for neonatal transitional hypoglycemia: What are we giving our babies? Paediatrics & child health 2019; 24 :115–118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (25).McKinlay CJD, Alsweiler JM, Anstice NS, Burakevych N, Chakraborty A, Chase JG, et al. Association of Neonatal Glycemia With Neurodevelopmental Outcomes at 4.5 Years. JAMA Pediatr 2017; 171: 972–983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (26).Lucas A, Morley R, Cole TJ. Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia. BMJ 1988; 297: 1304–1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (27).Tin W, Brunskill G, Kelly T, Fritz S. 15-Year Follow-Up of Recurrent “Hypoglycemia” in Preterm Infants. Pediatrics 2012; 130 :e1497–503. [DOI] [PubMed] [Google Scholar]
- (28).Ho HT, Yeung WK, Young BW. Evaluation of “point of care” devices in the measurement of low blood glucose in neonatal practice. Arch Dis Child Fetal Neonatal Ed 2004; 89: F356–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (29).Traill Z, Squier M, Anslow P. Brain imaging in neonatal hypoglycaemia. Arch Dis Child Fetal Neonatal Ed 1998;79: F145–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (30).Kaiser JR, Bai S, Gibson N, Holland G, Lin TM, Swearingen CJ, et al. Association between transient newborn hypoglycemia and fourth-grade achievement test proficiency: a population-based study. JAMA pediatrics 2015; 169: 913–921. [DOI] [PubMed] [Google Scholar]
- (31).Cornblath M, Hawdon JM, Williams AF, Aynsley-Green A, Ward-Platt MP, Schwartz R, et al. Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds. Pediatrics 2000; 105 :1141–1145. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.