

Abstract
Educational attainment is often considered the most important protective factor against cognitive impairment and dementia, yet significant variation in early educational experiences exists among midlife and older US adults. We used prospective data from the Health and Retirement Study (HRS) along with information on respondents’ early educational experiences collected in the 2015 and 2017 HRS Life History Mail Survey to examine whether school context, educational content, and academic ability were associated with trajectories of cognitive functioning and whether educational attainment explains this relationship. We restricted our sample to age-eligible HRS Life History Mail Survey respondents who provided data on cognitive functioning at least once during 1998–2014 and attended primary school or higher (n = 9,565 respondents providing 62,037 person-period observations). Estimates from linear mixed models revealed that school context, educational content, and academic ability were significantly associated with level of cognitive functioning but not rate of cognitive decline. Educational attainment explained 9%–55% of the association between these early educational experiences and level of cognitive functioning; however, all relationships remained statistically significant. Our results suggest that educational experiences that span childhood and adolescence are independently related to level of cognitive functioning decades later.
Keywords: dementia, life course, prospective study, school context, school segregation
Abbreviations
- AHEAD
Asset and Health Dynamics Among the Oldest Old
- CI
confidence interval
- CODA
Children of the Depression
- HRS
Health and Retirement Study
- LHMS
Life History Mail Survey
Educational attainment, typically operationalized as years of schooling or degrees attained, is one of the strongest predictors of cognitive functioning among older adults and perhaps the most important protective factor against cognitive impairment and dementia (1–5). With increasing educational attainment, older adults report higher levels of cognitive functioning but similar rates of cognitive decline (6, 7). Some argue that education exerts its impact on cognitive functioning by increasing the number of synapses or the extent of vascularization within the brain, thereby creating cognitive reserve (7). Cognitive reserve allows individuals to more effectively cope with increased brain pathology, resulting in the delayed onset of clinical symptoms of cognitive impairment (6, 8).
The concept of cognitive reserve focuses on how environments and activities shape cognitive efficiency, capacity, and/or flexibility throughout the life course (9). Yet, by operationalizing education as attainment, important aspects of education that occur earlier in the life course—such as school context, educational content, and academic ability—are overlooked (10). These early educational experiences might relate to later life cognitive functioning not only via educational attainment but also via exposure to educational environments and opportunities that uniquely build (or do not build) cognitive reserve. For example, Glymour et al. (11) found that individuals who lived in states that mandated a longer school year performed better on memory tests decades later. Crowe et al. (12) likewise found that among community-dwelling Alabama residents aged 65 years and older, length of school term was associated with better cognitive performance.
School resources and context—as measured by per-pupil funding, student-teacher ratio, and school segregation—are also related to cognitive functioning. Using a composite measure of educational quality that included self-reported indicators of school context and administrative records of school-term length, school days attended, and classroom size, researchers found that higher educational quality was associated with better cognitive functioning and a slower rate of cognitive decline among older black Manhattan residents (13). Among a community sample of Baltimore residents 50 years of age or older, attending a racially mixed school was associated with better cognitive performance than attending a racially segregated school, although school segregation had no relationship to cognitive decline (14).
Taken together, these studies suggest there are important aspects of education beyond attainment that could expand our understanding of how education protects against poor cognitive functioning and, by extension, dementia. To date, our knowledge of the relationship between early educational experiences and cognitive functioning is based on data from a handful of community-based samples or data from non-Hispanic whites who did not attend college, neither of which reflect the early educational experiences of all US older adults.
Our study addresses this key limitation by using recently released retrospective data on childhood school context, educational content, and academic ability among a nationally representative sample of midlife and older adults. Given improvements in school context and educational content within the US educational system over the course of the 20th century (15–18), we also examine whether early educational experiences differentially relate to cognitive functioning across cohorts. Our study is important because dementia prevalence appears to be declining in the United States, possibly due to increasing levels of educational attainment (19–21), but significant variation in early educational experiences across cohorts might also be driving recent trends.
We sought answers to 3 questions. First, does school context, educational content, and academic ability directly relate to level and decline of cognitive functioning? Second, to what extent does educational attainment explain this relationship? Third, do these relationships vary by cohort?
METHODS
Data and sample
We used data from the Health and Retirement Study (HRS), a nationally representative, longitudinal study of US adults over age 50 years (22). Since 1992, the HRS has conducted core interviews with age-eligible respondents and their spouses approximately every 2 years. In 2015, HRS collected information on respondents’ residential and schooling history and other childhood events through a Life History Mail Survey (LHMS). The HRS-LHMS was initially sent to 11,256 HRS respondents and their spouses from the 2014 core interview who were not selected for the 2015 Consumption and Activities Mail Survey and who completed their most recent core interview in English. Just over half of contacted individuals (n = 6,481; 58%) responded. In 2017, an additional 5,174 HRS respondents who were part of the 2015 Consumption and Activities Mail Survey sample, were still alive in 2017, and had completed their 2016 core interview by early March 2017, were mailed a LHMS. Their response rate was 74% (n = 3,844). A total of 10,325 HRS respondents have completed the HRS-LHMS as of 2017.
We restricted our sample to age-eligible HRS-LHMS respondents (n = 9,706) who provided data on cognitive functioning at least once between 1998 and 2014 (n = 9,615) and attended at least primary school (n = 9,565). This resulted in an analytical sample of 9,565 respondents providing 62,037 person-period observations (mean number of observations = 6.5). Approximately 36% of the sample had missing data on at least 1 of the independent variables or covariates; item nonresponse ranged from <1% (educational attainment) to 14.8% (learning problem). Because we used the imputed cognition variables provided by HRS, there were no missing data on the dependent variable. To address item nonresponse, we employed multiple imputation.
Due to LHMS eligibility requirements and the timing of its administration, the HRS-LHMS sample is younger, less cognitively impaired, and more highly educated than the HRS sample overall (see Web Table 1).
Measures
Dependent variable.
HRS uses a modified version of the Telephone Instrument for Cognitive Status (TICS) to assess cognitive function both in face-to-face interviews and by telephone. We constructed a total cognitive function score by summing scores across the following tests of memory and mental status: 1) an immediate word-recall test in which respondents are read a list of 10 common nouns and are immediately asked to recall as many words as they can (10 points); 2) a delayed recall test, occurring approximately 5 minutes later, of the same 10 words (10 points); 3) a serial 7’s subtraction test requiring respondents to subtract 7 (from 100) 5 times (5 points); 4) a backward counting test requiring respondents to count backwards as quickly as possible for 10 continuous numbers from the number 20 (2 points if correct on first attempt, 1 point if correct on second attempt); 5) naming the day of the week and the date (4 points); 6) naming the President and Vice President (2 points); and 7) identifying 2 objects, “scissors” and “cactus” (2 points). We assigned full points on the naming and object identification tests for respondents under age 65 years who were not asked these questions. These tests do not differentiate impairment in younger populations because adults under age 65 typically provide correct answers to all naming questions. The total cognitive function score was normally distributed, and values ranged from 0 to 35.
Educational experiences.
Measures of academic ability, school context, and educational content come from the LHMS. We classified respondents as having a learning problem if, during elementary school, they were told by a professional that they had a problem learning any of 4 subject matters (i.e., reading, writing, mathematics, speaking/language) or they were diagnosed with attention deficit hyperactivity disorder, dyslexia, or another learning disorder. Respondents self-assessed their reading and math ability at age 10 years in comparison with other children in their class (1 = much better, 2 = better, 3 = average, 4 = worse, 5 = much worse). We classified respondents as having attended a majority-minority elementary school if most students in their school were black, Hispanic, or another nonwhite race/ethnicity. Respondents reported on their high-school curriculum, which we classified as 1) did not attend high school, 2) vocational or general education, and 3) college preparatory. We also classified respondents as being involved in language or creative arts in high school if they had studied a foreign language, played a musical instrument, took singing lessons/sang in a choir, learned ballet or dance, or learned to paint or draw. Finally, in the core HRS interview, respondents reported whether they lived in a rural area most of the time they were in school.
Educational attainment.
We classified respondents as having completed 1) less than a high-school diploma, 2) General Educational Development certificate or high-school diploma, 3) some college, or 4) a bachelor’s degree or higher. Other specifications of educational attainment yielded similar results.
Covariates.
To account for childhood factors that could confound the relationship between educational experiences and cognitive functioning, we included parent’s education measured as the highest year of schooling completed by either parent, the number of books in the childhood home (1 = none or few, 2 = 1 shelf, 3 = 1 bookcase, 4 = 2 bookcases, 5 = more than 2 bookcases), and self-reported childhood health (1 = excellent, 2 = very good, 3 = good, 4 = fair, 5 = poor). Adjustment for other measures of childhood socioeconomic status—including self-reported family socioeconomic status, father’s unemployment status, and residential moves due to financial difficulties—did not alter our overall findings but did increase multicollinearity. We therefore did not retain these indicators in our models. Demographic covariates included self-reported race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and other race/ethnicity), birth cohort (Asset and Health Dynamics Among the Oldest Old (AHEAD)/Children of the Depression (CODA) (≤1930), HRS/War Babies (1931–1947), or Early and Mid Baby Boomers (1948–1959)), sex (male or female), and whether they completed the LHMS on their own or with assistance.
Statistical analysis
To address item nonresponse, we imputed data on the independent variables and covariates using the mi impute command with chained equations in Stata, version 14 (StataCorp LP, College Station, TX). Imputation models included all analytical variables as well as variables not included in our analysis that were theoretically related to item nonresponse or the analytical variables (e.g., region of birth, childhood moves, attending preschool) (23). We produced 20 data sets as recommended by Graham et al. (24). Analyses were replicated across the 20 data sets and combined using mi estimate.
We used linear mixed models to account for repeated observations of cognitive functioning and varying numbers of observations per person (25). Age represents time, and it was centered at 65 years, the mean age of respondents across the period of investigation. We interacted all independent variables and covariates with age to examine their influence on the rate of change in cognitive functioning. Linear mixed models included a random-intercept assumed to be normally distributed with mean zero and independent of within-person error and all model covariates. Linear mixed models were estimated using mixed in Stata, version 14 (StataCorp LP). We used person-level weights from the respondents’ last core interview to account for the complex sampling design. Unweighted analyses yielded similar results.
We fitted 2 models. Model 1 estimated the relationship between early educational experiences and trajectories of cognitive functioning after adjustment for childhood and demographic confounders. Model 2 estimated the relationship between early educational experiences and trajectories of cognitive functioning after inclusion of educational attainment.
Before fitting our models, we plotted mean cognitive functioning by age across cohorts (Figure 1) and determined that a linear specification of age fit the data best, which we confirmed in an unconditional linear mixed model. Cognitive functioning was highest at younger ages and declined with age. Mean plots also revealed significant cohort differences in cognitive functioning.
Figure 1.
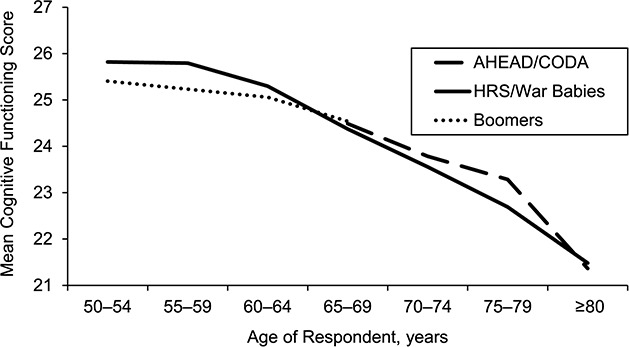
Mean cognitive functioning according to age and cohort, Health and Retirement Study Life History Mail Survey Sample, United States, 1998–2014. Weighted estimates (person-period observations = 62,037; number of respondents = 9,565). Asset and Health Dynamics Among the Oldest Old/Children of the Depression (AHEAD/CODA) cohort born ≤1930; Health and Retirement Study (HRS)/War Babies cohort born 1931–1947; Baby Boomer cohort born 1948–1959.
RESULTS
Sample characteristics
Table 1 presents sample characteristics for the full sample and by birth cohort. Most respondents were white (84.3%), and over 56% were women. On average, respondents’ most educated parent completed 11.6 years of school, they reported from 1 shelf to 1 bookcase of books in their childhood home (mean = 2.4; standard error, 0.02), and they rated their childhood health as very good to excellent (mean = 1.7; standard error, 0.01). Respondents generally rated their reading and math ability as between “average” to “better than their classmates” (mean = 2.4 and 2.6, respectively). Only 14.4% reported a learning problem. Approximately 14% ever attended a majority-minority elementary school, 73.7% were involved in language or creative arts in high school, and about two-thirds were enrolled in vocational or general education curriculum (65.4%). More than half completed some college or more.
Table 1.
Sample Characteristics According to Birth Cohort, Weighted Estimates, Health and Retirement Study Life History Mail Survey Sample, United States, 1998–2014
| Measure | Full (n = 9,565) | AHEAD/CODA (n = 782) | HRS/War Babies (n= 4,479) | Baby Boomers (n = 4,304) | ||||
|---|---|---|---|---|---|---|---|---|
| % | Mean (SE) | % | Mean (SE) | % | Mean (SE) | % | Mean (SE) | |
| Demographics | ||||||||
| Race/ethnicity | ||||||||
| Non-Hispanic white | 84.3 | 90.7 | 86.6 | 81.9 | ||||
| Non-Hispanic back | 8.4 | 5.1 | 7.4 | 9.6 | ||||
| Latino | 4.6 | 3.0 | 3.9 | 5.2 | ||||
| Other | 2.7 | 1.2 | 2.1 | 3.3 | ||||
| Female | 56.2 | 67.0 | 56.1 | 55.1 | ||||
| Proxy interview, LHMS | 6.1 | 21.5 | 7.3 | 3.4 | ||||
| Childhood and family experiences | ||||||||
| Parent’s education, years | 11.6 (0.04) | 9.6 (0.13) | 11.0 (0.06) | 12.3 (0.06) | ||||
| Number of books in the homea | 2.4 (0.02) | 1.9 (0.04) | 2.1 (0.02) | 2.7 (0.02) | ||||
| Self-rated health in childhoodb | 1.7 (0.01) | 1.8 (0.04) | 1.7 (0.02) | 1.6 (0.02) | ||||
| Educational experiences | ||||||||
| Learning problem | 14.4 | 9.4 | 11.5 | 17.3 | ||||
| Reading ability compared with peersc | 2.4 (0.01) | 2.3 (0.03) | 2.4 (0.02) | 2.4 (0.02) | ||||
| Math ability compared with peersc | 2.6 (0.01) | 2.5 (0.03) | 2.6 (0.02) | 2.6 (0.02) | ||||
| Attended majority-minority elementary school | 13.8 | 8.0 | 12.0 | 16.0 | ||||
| Involved in language or creative arts | 73.7 | 64.0 | 70.7 | 77.1 | ||||
| High-school curriculum | ||||||||
| Never attended high school | 3.3 | 9.4 | 4.4 | 1.8 | ||||
| Vocational or general education | 65.4 | 69.1 | 67.0 | 63.8 | ||||
| College preparatory | 31.3 | 21.5 | 28.6 | 34.4 | ||||
| Lived in rural area during school | 43.0 | 46.3 | 46.1 | 40.3 | ||||
| Educational attainment | ||||||||
| Less than high school | 8.6 | 17.1 | 11.4 | 5.5 | ||||
| High-school graduate or GED | 32.8 | 37.6 | 37.6 | 28.5 | ||||
| Some college | 26.8 | 21.1 | 23.1 | 30.4 | ||||
| College or more | 31.8 | 24.2 | 27.9 | 35.6 | ||||
Abbreviations: AHEAD/CODA, Asset and Health Dynamics Among the Oldest Old/Children of the Depression; GED, General Educational Development; HRS, Health and Retirement Study; LHMS, Life History Mail Survey; SE, standard error.
a 1 = none or few; 5 = 200 or more books.
b 1 = excellent; 5 = poor.
c 1 = much better; 5 = much worse.
Demographic differences across cohorts likely reflected a combination of selective mortality, demographic shifts, and changes in US schooling. For example, compared with the AHEAD/CODA cohort, fewer respondents in the Baby Boomer cohort were white or women. Baby Boomers were also more educated than the AHEAD/CODA cohort, more likely to have attended a majority-minority elementary school (16% vs. 8%), and more likely to have learned a foreign language or participated in creative arts (77.1% vs. 64%).
Linear mixed models
Table 2 presents results from the linear mixed models. Model 1 shows estimates for academic ability, school context, and educational content after adjustment for childhood and demographic confounders. At age 65 years, all early educational experiences were significantly associated with cognitive functioning. Respondents with a learning problem in elementary school scored 0.88 points lower on cognitive functioning at age 65 than those without a learning problem. Lower ratings on reading (b = −0.28, 95% confidence interval (CI): −0.36, −0.19) and math ability (b = −0.47, 95% CI: −0.56, −0.39) in elementary school, attending a majority-minority elementary school (b = −0.43, 95% CI: −0.81, −0.05), attending a school in a rural area versus an urban area (b = −0.45, 95% CI: −0.58, −0.32), and enrollment in vocational or general education curriculum in high school (b = −0.56, 95% CI: −0.71, −0.41) versus a college preparatory curriculum were associated with lower cognitive functioning at age 65 years. Involvement in language or creative arts in high school (b = 0.71, 95% CI: 0.54, 0.88) was associated with higher cognitive functioning at age 65. As respondents aged, their cognitive functioning declined by 0.15 points per year. Having a learning problem was associated with a faster rate of cognitive decline, but no other educational experience was associated with rate of cognitive decline.
Table 2.
Linear Mixed Models Predicting Cognitive Functioning by Educational Experiences, Weighted Estimates, Health and Retirement Study Life History Mail Survey Sample (n = 9,565)a,b, United States, 1998–2014
| Measurec | Model 1 | Model 2 | ||
|---|---|---|---|---|
| b | 95% CI | b | 95% CI | |
| At age 65 years | 26.84 | 26.47, 27.21 | 27.37 | 27.01, 27.74 |
| Learning problem | −0.88 | −1.12, −0.64 | −0.80 | −1.03, −0.56 |
| Reading ability compared with peersd | −0.28 | −0.36, −0.19 | −0.18 | −0.26, −0.09 |
| Math ability compared with peersd | −0.47 | −0.56, −0.39 | −0.42 | −0.50, −0.34 |
| Majority-minority elementary school | −0.43 | −0.81, −0.05 | −0.45 | −0.82, −0.08 |
| Language or creative arts | 0.71 | 0.54, 0.88 | 0.36 | 0.19, 0.53 |
| High-school curriculum | ||||
| Never attended high school | −2.04 | −2.50, −1.58 | −0.92 | −1.38, −0.47 |
| Vocational or general education | −0.56 | −0.71, −0.41 | −0.25 | −0.40, −0.11 |
| Lived in rural area during school | −0.45 | −0.58, −0.32 | −0.34 | −0.46, −0.21 |
| Educational attainment | ||||
| Less than high school | −3.16 | −3.46, −2.85 | ||
| High-school graduate or GED | −1.50 | −1.67, −1.33 | ||
| Some college | −0.81 | −0.98, −0.64 | ||
| Age, yearse | −0.150 | −0.180, −0.120 | −0.151 | −0.181, −0.122 |
| Learning problem × age | −0.022 | −0.040, −0.004 | −0.019 | −0.037, −0.002 |
| Reading ability compared with peers × aged | −0.001 | −0.007, 0.006 | 0.000 | −0.006, 0.007 |
| Math ability compared with peers × aged | 0.004 | −0.002, 0.011 | 0.004 | −0.002, 0.011 |
| Majority-minority elementary school × age | 0.017 | −0.012, 0.045 | 0.020 | −0.008, 0.048 |
| Language or creative arts × age | 0.007 | −0.006, 0.020 | 0.006 | −0.008, 0.019 |
| High-school curriculum | ||||
| Never attended high school × age | −0.019 | −0.051, 0.014 | −0.012 | −0.045, 0.022 |
| Vocational or general education × age | 0.002 | −0.010, 0.014 | 0.002 | −0.010, 0.015 |
| Lived in rural area during school × age | −0.008 | −0.018, 0.002 | −0.006 | −0.017, 0.004 |
| Educational attainment | ||||
| Less than high school × age | −0.014 | −0.038, 0.009 | ||
| High-school graduate or GED × age | −0.002 | −0.016, 0.012 | ||
| Some college × age | −0.011 | −0.025, 0.003 | ||
| Random intercept (at mean age) | 0.82 | 0.79, 0.84 | 0.77 | 0.75, 0.80 |
| Within-person error | 0.95 | 0.94, 0.96 | 0.95 | 0.94, 0.96 |
Abbreviations: CI, confidence interval; GED, General Educational Development.
a All models adjusted for sex, race/ethnicity, birth cohort, proxy interview, parents’ education, number of books in house during childhood, and self-reported health in childhood.
b Number of person-period observations = 62,037; mean number of observations = 6.5.
c Reference groups: college preparatory coursework (high-school curriculum), college or above (educational attainment).
d 1 = much better, 5 = much worse.
e Age centered at 65 years.
Model 2 shows estimates for educational experiences after inclusion of educational attainment. Educational attainment attenuated the regression coefficients for early educational experiences by about 9% (learning problem) to 55% (vocational/general education curriculum); however, all remained significantly associated with cognitive functioning at age 65. In addition, having a learning problem remained significantly associated with rate of cognitive decline.
Given selective mortality, demographic shifts, and changes in US schooling across cohorts, we refitted model 2 but modeled only how our variables of interest were related to level of cognitive functioning given that supplemental analysis confirmed that these variables were unrelated to cognitive decline across cohorts. In Table 3, fewer of the early educational experiences were significantly related to cognitive functioning among the AHEAD/CODA cohort than the HRS and more recent cohorts; however, the coefficients did not statistically differ across cohorts in post-hoc tests. Generally, indicators of academic ability were significantly associated with cognitive functioning across all cohorts. These patterns were also found in models that did not include educational attainment (results available upon request).
Table 3.
Cohort-Stratified Linear Mixed Modelsa Predicting Cognitive Functioning According to Educational Experiences, Weighted Estimates, Health and Retirement Study Life History Mail Survey Sample, United States, 1998–2014
| Measure | AHEAD/CODA b (n = 782) | HRS/War Babies c (n = 4,479) | Baby Boomers d (n = 4,304) | |||
|---|---|---|---|---|---|---|
| b | 95% CI | b | 95% CI | b | 95% CI | |
| At mean agee | 24.86 | 23.57, 26.15 | 27.26 | 26.77, 27.76 | 27.62 | 27.07, 28.17 |
| Learning problem | −0.83 | −1.61, −0.05 | −0.80 | −1.15, −0.46 | −0.64 | −0.93, −0.35 |
| Reading ability compared with peersf | −0.26 | −0.55, 0.03 | −0.18 | −0.29, −0.06 | −0.16 | −0.27, −0.04 |
| Math ability compared with peersf | −0.28 | −0.56, −0.00 | −0.50 | −0.61, −0.38 | −0.39 | −0.51, −0.28 |
| Majority-minority elementary school | 0.23 | −1.38, 1.83 | −0.36 | −0.93, 0.20 | −0.64 | −1.06, −0.21 |
| Language or creative arts | 0.23 | −0.35, 0.82 | 0.39 | 0.18, 0.61 | 0.31 | 0.05,0.57 |
| High-school curriculum | ||||||
| Never attended high school | −0.83 | −2.06, 0.41 | −1.20 | −1.77, −0.63 | −0.58 | −1.45, 0.29 |
| Vocational or general education | −0.12 | −0.63, 0.39 | −0.25 | −0.45, −0.05 | −0.31 | −0.52, −0.10 |
| Lived in rural area during school | −0.44 | −0.88, 0.01 | −0.38 | −0.55, −0.21 | −0.26 | −0.45, −0.07 |
| Educational attainment | ||||||
| Less than high school | −2.87 | −3.83, −1.91 | −3.23 | −3.62, −2.84 | −3.06 | −3.60, −2.51 |
| High-school graduate or GED | −0.66 | −1.23, −0.10 | −1.45 | −1.68, −1.21 | −1.65 | −1.91, −1.39 |
| Some college | −0.17 | −0.76, 0.41 | −0.80 | −1.03, −0.57 | −0.80 | −1.03, −0.56 |
| Age, yearse | −0.25 | −0.27, −0.24 | −0.15 | −0.16, −0.14 | −0.02 | −0.04, −0.01 |
| Random intercept (at mean age) | 0.88 | 0.81, 0.96 | 0.78 | 0.74, 0.81 | 0.73 | 0.69, 0.77 |
| Within-person error | 1.04 | 1.01, 1.07 | 0.97 | 0.95, 0.98 | 0.91 | 0.89, 0.93 |
Abbreviations: AHEAD/CODA, Asset and Health Dynamics Among the Oldest Old/Children of the Depression; CI, confidence interval; GED, General Educational Development; HRS, Health and Retirement Study.
a All models adjusted for sex, race/ethnicity, birth cohort, proxy interview, parents’ education, number of books in house during childhood, and self-reported health in childhood. Reference groups: college preparatory coursework (high-school curriculum), college or above (educational attainment).
b AHEAD/CODA cohort born ≤1930; person-period observations = 6,625; mean number of observations = 8.5.
c HRS/War Babies cohort born 1931–1947; person-period observations = 37,363; mean number of observations = 8.3.
d Baby Boomer cohort born 1948–1959; person-period observations = 18,049; mean number of observations = 4.2.
e Age centered at mean age of cohort in years (AHEAD/CODA = 79; HRS/War Babies = 66; Boomers = 57).
f 1 = much better, 5 = much worse.
Supplemental analysis
We estimated the natural direct effects of educational experiences on trajectories of cognitive functioning under the assumption that these relationships were similar across levels of educational attainment (Web Figure 1, available at https://academic.oup.com/aje) (26). To test this assumption, we stratified by educational attainment and refitted our model. Overall, we did not find evidence that our models violated this assumption.
DISCUSSION
Recent studies in high-income countries document declining prevalence and incidence of dementia, driven in part by historical increases in educational attainment (19–21, 27, 28). Some speculate that declines in dementia might reverse or diminish among younger cohorts given near universal high-school completion (29, 30). Such speculation, however, is undergirded by an overreliance on educational attainment as the sole measure of education, leaving other aspects of education—including context, content, and ability—unexamined. This omission is particularly concerning given that educational policies and allocation of school funding have resulted in vastly different educational experiences across US cohorts and racial/ethnic groups (15, 16). Few studies have examined how these early educational experiences shape cognitive functioning, and those that have often relied on selective samples with limited generalizability. Our study used a nationally representative sample of midlife and older US adults to examine whether school context, educational content, and academic ability were related to cognitive functioning and decline, and whether educational attainment fully or partially explained these relationships.
We found that these early educational experiences were all significantly related to level of cognitive functioning but not to cognitive decline (with the exception of having a learning problem). Educational attainment explained about 9%–55% of the association between individual indicators of context, content, and ability and level of cognitive functioning. Importantly, all of these early educational experiences remained significant after accounting for educational attainment, suggesting that exposure to early educational advantages might build cognitive reserve important for maintaining cognitive functioning later in life independent from educational attainment.
In cohort-stratified analysis, the size of the coefficients for context and content were larger (and significant) for midlife and older adults born after 1940 than for those born prior to 1941; however, these coefficients did not statistically differ across cohorts, perhaps due to the small size of the AHEAD/CODA cohort. Indicators of academic ability, in general, were significantly associated with level of cognitive functioning across all cohorts. These cohort differences are suggestive and might be related to sociohistorical changes occurring within the education system that were more likely to affect younger versus older cohorts, including the desegregation of public schools, the 1958 National Defense Education Act, and the Great Society Programs (15–17).
Older adults who attended rural or majority-minority elementary schools reported lower levels of cognitive functioning than those who attended urban or predominantly white elementary schools. School context indicators were unrelated to cognitive decline. Similar findings were documented in a community-based sample of older black adults living in Baltimore; attending desegregated schools resulted in higher levels of cognitive functioning but had no relationship to cognitive decline (14). Historical data on rural schooling is sparse (31), and recent studies examining the role of early educational experiences on cognitive functioning have either not included rural/urban indicators or did not investigate their independent effects (12, 13). Our study suggests that this aspect of school context might be an important predictor of cognitive functioning in older adulthood.
Prior work suggests that music instruction and learning a foreign language are associated with reduced risk for mild cognitive impairment and higher levels of cognitive functioning (32). Similarly, our results indicate that older adults who took a foreign language course or participated in creative arts during high school reported higher cognitive functioning, whereas those who enrolled in vocational or general education curriculum instead of college preparatory courses in high school had lower cognitive functioning. The 1958 National Defense Education Act invested $1 billion dollars over 7 years (equivalent to $8.8 billion in 2019 dollars) to improve education in the fields of science, mathematics, and foreign language (17). Respondents attending high school after 1958 would have benefited directly from such an investment, and this could be one reason that educational content was significantly associated with cognitive functioning among the younger, but not older, cohorts.
Having a learning problem and poorer self-assessments of reading and math ability were independently associated with lower levels of cognitive functioning, regardless of cohort. Few studies have examined academic ability as a predictor of cognitive functioning, although a recent Swedish study found that individuals reporting better academic grades at age 12 years had higher cognitive functioning and slower cognitive decline from ages 45 to 70 years (33). Although we could not assess academic grades, we found similar relationships using measures of academic ability. Thus, educational experiences that enhance early academic performance might also have long-term implications for cognitive functioning.
Limitations
Our study includes several limitations. First, early educational experiences were self-reported and retrospective, potentially leading to measurement error. The HRS-LHMS used a life history calendar method, however, which reduces recall bias and increases accuracy (34). Our findings also align with prior work using administrative data, suggesting that if measurement bias exists its impact is likely minimal (12, 13, 33). Second, given that our sample was relatively healthier and more cognitively intact than the full HRS sample, we might have underestimated the association between early educational experiences and cognitive functioning and decline as well as cohort differences in these relationships. Third, the HRS-LHMS included a limited number of early educational experiences. Other aspects of education—including teacher experience, classroom size, and per-pupil spending—could also be related to cognitive functioning.
Last, while researchers assume that education is preventive against cognitive decline, an alternative explanation is that unobserved confounders, including genetic endowments, might determine both attainment and cognitive functioning. We cannot account for the potential influence of heritability in our models and thus cannot rule out this alternative explanation. The amount of variation explained by heritability, however, is often less than or comparable to the amount of variation explained by environment and also dependent on environment (e.g., school context) (35, 36). Moreover, our results show a relationship between school context—an exposure which is theoretically exogenous—and level of cognitive functioning.
Conclusion
Education might change brain structure and increase cognitive reserve (7, 8). Some argue that such changes occur early in the life course, before most studies of cognitive decline commence (37). Given the dominant use of educational attainment to operationalize education, it is not entirely clear when education exerts its effects, but our findings suggest that certain aspects of education that occur as early as primary school have lasting impacts on cognitive functioning, independent of educational attainment. While some speculate that after 8 years of education, maximum cognitive reserve is reached and little benefit is gained from additional education (6), our results suggest that educational experiences that span childhood and adolescence are related to cognitive functioning decades later.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Department of Health Promotion, Education, and Behavior, Arnold School of Public Health, University of South Carolina, Columbia, South Carolina (Katrina M. Walsemann); and Leonard Davis School of Gerontology, University of Southern California, Los Angeles, California (Jennifer A. Ailshire).
This work was funded by the National Institute on Aging (grants P30AG059294 and P30AG043073).
Earlier versions of this study were presented at the 2018 Annual Scientific Meeting of the Gerontological Society of America, November 14–18, 2018, Boston, Massachusetts; and the 2019 Annual Meeting of the Population Association of America, April 10–13, 2019, Austin, Texas.
The views expressed in this paper are those of the authors and not necessarily those of any funding body. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest: none declared.
REFERENCES
- 1. Alley D, Suthers K, Crimmins E. Education and cognitive decline in older Americans: results from the AHEAD sample. Res Aging. 2007;29(1):73–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Reuser M, Willekens FJ, Bonneux L. Higher education delays and shortens cognitive impairment. A multistate life table analysis of the US Health and Retirement Study. Eur J Epidemiol. 2011;26(5):395–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wilson RS, Hebert LE, Scherr PA, et al. Educational attainment and cognitive decline in old age. Neurology. 2009;72(5):460–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Zahodne LB, Glymour MM, Sparks C, et al. Education does not slow cognitive decline with aging: 12-year evidence from the Victoria Longitudinal Study. J Int Neuropsychol Soc. 2011;17(6):1039–1046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Schneeweis N, Skirbekk V, Winter-Ebmer R. Does education improve cognitive performance four decades after school completion? Demography. 2014;51(2):619–643. [DOI] [PubMed] [Google Scholar]
- 6. Lenehan ME, Summers MJ, Saunders NL, et al. Relationship between education and age-related cognitive decline: a review of recent research. Psychogeriatrics. 2015;15(2):154–162. [DOI] [PubMed] [Google Scholar]
- 7. Beydoun MA, Beydoun HA, Gamaldo AA, et al. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014;14(1):643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Mungas D, Gavett B, Fletcher E, et al. Education amplifies brain atrophy effect on cognitive decline: implications for cognitive reserve. Neurobiol Aging. 2018;68:142–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Barulli D, Stern Y. Efficiency, capacity, compensation, maintenance, plasticity: emerging concepts in cognitive reserve. Trends Cogn Sci. 2013;17(10):502–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Walsemann KM, Gee GC, Ro A. Educational attainment in the context of social inequality: new directions for research on education and health. Am Behav Sci. 2013;57(8):1082–1104. [Google Scholar]
- 11. Glymour MM, Kawachi I, Jencks CS, et al. Does childhood schooling affect old age memory or mental status? Using state schooling laws as natural experiments. J Epidemiol Community Health. 2008;62(6):532–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Crowe M, Clay OJ, Martin RC, et al. Indicators of childhood quality of education in relation to cognitive function in older adulthood. J Gerontol A Biol Sci Med Sci. 2013;68(2):198–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Sisco S, Gross AL, Shih RA, et al. The role of early-life educational quality and literacy in explaining racial disparities in cognition in late life. J Gerontol B Psychol Sci Soc Sci. 2015;70(4):557–567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Aiken-Morgan AT, Gamaldo AA, Sims RC, et al. Education desegregation and cognitive change in African American older adults. J Gerontol B Psychol Sci Soc Sci. 2015;70(3):348–356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Office of Vocational and Adult Education From There to Here: the Road to Reform of American High Schools. Washington, DC: US Department of Education; 2003. [Google Scholar]
- 16. Cottrol RJ, Diamond RT, Ware LB. Brown v. Board of Education: Caste, Culture, and the Constitution. Lawrence, KS: University Press of Kansas; 2003. [Google Scholar]
- 17. Flemming AS. The philosophy and objectives of the National Defense Education Act. Ann Am Acad Pol Soc Sci. 1960;327(1):132–138. [Google Scholar]
- 18. Fuller E, Pearson JB. Education in the States: Historical Development and Outlook. Washington, DC: Council of Chief State School Officers, National Education Association; 1969. [Google Scholar]
- 19. Langa KM, Larson EB, Crimmins EM, et al. A comparison of the prevalence of dementia in the United States in 2000 and 2012. JAMA Intern Med. 2017;177(1):51–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Satizabal CL, Beiser AS, Chouraki V, et al. Incidence of dementia over three decades in the Framingham Heart Study. N Engl J Med. 2016;374(6):523–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Freedman VA, Kasper JD, Spillman BC, et al. Short-term changes in the prevalence of probable dementia: an analysis of the 2011–2015 National Health and Aging Trends Study. J Gerontol B Psychol Sci Soc Sci. 2018;73(suppl 1):S48–S56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Sonnega A, Weir D. The Health and Retirement Study: a public data resource for research on aging. Open Health Data. 2014;2(1):e7. [Google Scholar]
- 23. Heeringa SG, West BT, Berglund PA. Applied Survey Data Analysis. 2nd ed. Boca Rotan, FL: Chapman & Hall/CRC Press; 2017. [Google Scholar]
- 24. Graham JW, Olchowski AE, Gilreath TD. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev Sci. 2007;8(3):206–213. [DOI] [PubMed] [Google Scholar]
- 25. Singer JD, Willet JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. New York, NY: Oxford University Press; 2003. [Google Scholar]
- 26. Petersen ML, Sinisi SE, van der Laan MJ. Estimation of direct causal effects. Epidemiology. 2006;17(3):276–284. [DOI] [PubMed] [Google Scholar]
- 27. Wu Y-T, Beiser AS, Breteler MM, et al. The changing prevalence and incidence of dementia over time—current evidence. Nat Rev Neurol. 2017;13(6):327–339. [DOI] [PubMed] [Google Scholar]
- 28. Prince M, Ali G-C, Guerchet M, et al. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimers Res Ther. 2016;8(1):23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. McFarland J, Cui J, Stark P. Trends in high school dropout and completion rates in the United States: 2014 In: National Center for Education Statistics. Washington DC: US Department of Education; 2018. [Google Scholar]
- 30. US Census Bureau Table A-2. Percent of people 25 years and over who have completed high school or college, by race, Hispanic origin, and sex: Selected years 1940 to 2017. https://www.census.gov/data/tables/2016/demo/education-attainment/cps-detailed-tables.html. Accessed December 12, 2019.
- 31. DeYoung AJ. The status of American rural education research: an integrated review and commentary. Rev Educ Res. 1987;57(2):123–148. [Google Scholar]
- 32. Wilson RS, Boyle PA, Yang J, et al. Early life instruction in foreign language and music and incidence of mild cognitive impairment. Neuropsychology. 2015;29(2):292–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Pudas S, Rönnlund M. School performance and educational attainment as early-life predictors of age-related memory decline: protective influences in later-born cohorts. J Gerontol B Psychol Sci Soc Sci. 2019;74(8):1357–1365. [DOI] [PubMed] [Google Scholar]
- 34. Axinn WG, Pearce LD, Ghimire D. Innovations in life history calendar applications. Soc Sci Res. 1999;28(3):243–264. [Google Scholar]
- 35. Lee JJ, Wedow R, Okbay A, et al. Gene discovery and polygenic prediction from a 1.1-million-person GWAS of educational attainment. Nat Genet. 2018;50(8):1112–1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Cook CJ, Fletcher JM. Can education rescue genetic liability for cognitive decline? Soc Sci Med. 2015;127:159–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Mayeda ER, Filshtein TJ, Tripodis Y, et al. Does selective survival before study enrolment attenuate estimated effects of education on rate of cognitive decline in older adults? A simulation approach for quantifying survival bias in life course epidemiology. Int J Epidemiol. 2018;47(5):1507–1517. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.