

Abstract
Background:
Despite many benefits of physical exercise to women during pregnancy, the majority of Saudi women do not engage in an adequate amount of activity because of common barriers such as fatigue, lack of motivation, and childcare. The purpose of this study was to estimate the proportion of Saudi women who get adequate exercise during pregnancy as well as to evaluate their knowledge of, attitude toward, and barriers to physical exercise during pregnancy.
Methods:
This study had a cross-sectional design. Data were collected retrospectively (average time: 1 year after the birth), using translated questionnaires (English to Arabic), from primary health care centers and from the Maternity and Children Hospital in Qassim, Saudi Arabia. Logistic regression was employed to assess the a priori correlates of adequate exercise during pregnancy (primary outcome).
Results:
The sample included 274 women, who had a mean age of 31.9 years. A majority of the women thought that physical exercise during pregnancy was necessary and had high knowledge levels (mean = 77; median = 75) about types and amount of physical activity. Less than half of the women were either walking (26%) or exercising (42%) adequately (i.e. ⩾150 min/week). Age (odds ratio: 1.79), number of pregnancies (odds ratio: 2.41), attitude toward exercise (odds ratio: 2.71), and self-rated health (odds ratio: 2.50) were significant correlates of adequate exercise during pregnancy. Among those who reported no physical exercise during pregnancy (n = 68), the following barriers were most common: tiredness (25.0%), fear (18.1%), dislike of exercise (16.7%), and lack of information (16.7%).
Conclusion:
For Saudi women, interventions are needed during pre-natal checkups to promote and maintain adequate physical activity levels during pregnancy.
Keywords: exercise, physical activity, pregnancy, women
The American Congress of Obstetricians and Gynecologists1 recommends that pregnant women exercise moderately for 150 min or more per week. Regardless of the physical fitness level, it is advised that exercise should be consistent, non-strenuous, and of mild to moderate intensity among pregnant women.1 Scientific evidence has shown that exercise during pregnancy has potential benefits to the mother and the baby.2–5 The foremost maternal physical health benefits include improving muscular strength, diminishing back pain, preventing excessive weight gain, lowering risk of developing gestational hypertension and diabetes, and reducing lower limb edema as well as urinary incontinence. Potential fetal health benefits include promoting fetal growth, enhancing fetal cardiac autonomic control, and improving neurological and mental development. In addition, regular physical exercise during pregnancy could reduce medical interventions during labor, such as cesarean sections, as well as alleviate pain and discomfort during labor.
Since most women fail to meet the recommendation for exercise during pregnancy, several studies have examined barriers to exercise.6–8 In those studies, intrapersonal factors, such as pregnancy-related symptoms, time constraints, and lack of motivation, were the most consistently cited barriers to exercise. However, interpersonal (e.g. social support) and environmental (e.g. lack of resources, weather) factors were also notable barriers. There was some variation in reported barriers across other demographic and lifestyle characteristics.6 For example, those with lower socio-economic status were more likely to report “lack of resources” than those with a higher status. Also, women who had exercise routines prior to pregnancy reported fewer barriers than those without previous routines.9
Data showed that the fertility rate among Saudi women was 2.58 in 2015 (rank 76).10 Early studies stated that Saudi women reported the desire to have large families.11 Further, available data on women in Saudi Arabia suggest that physical exercise is generally uncommon. It was reported that 75% of women have a sedentary lifestyle,12 but physical exercise during pregnancy among Saudi women has not yet been reported. Since physical exercise is not part of the culture in general,13 we hypothesized that the knowledge about the recommendations for exercise during pregnancy would be low and that there may be misconceptions that exercise during pregnancy poses health risks to the mother and the baby.
Therefore, the study objectives were to estimate the proportion of Saudi women who report an adequate amount of physical exercise during pregnancy as well as to identify significant correlates of adequate exercise. We hypothesized that the amount of time spent engaging in exercise would be low in this population; hence, we aimed to evaluate knowledge of, attitude toward, and barriers to physical exercise during pregnancy as well.
Methods
Study design and sample
This was a cross-sectional study that included women who had given birth in the previous 2 years in the Qassim region. Qassim is one of the largest provinces in Saudi Arabia and has a population of roughly 1.4 million.14 The women were recruited from nine primary health care centers and from the Maternal and Children’s Hospital in Buraydah using a non-probabilistic sampling strategy. Data collection was done over a period of 8 weeks on the days that the well-baby clinics were conducted (multiple days per week), which provided the widest sample available of recently pregnant women. The inclusion criteria included being a resident of Qassim and having a child between the ages of 1 month and 2 years. However, women were excluded from the study if they reported any physical deficiency/disability that restricted their ability to perform physical exercise, which included having a high-risk pregnancy. With an estimate that 50% of pregnant women have knowledge and perform physical exercise, we calculated the sample size. With a power of 88%, a margin of error of 12%, and a confidence level of 95%, the minimal sample size required was 267. The study protocol was approved by the Medical Research Ethical Committee in Qassim University (#15/11/7).
Data collection and instrument
The researchers described the study’s purpose and procedures to each woman. Once eligibility was determined, each woman was given the informed consent form to sign. There were eight medical students involved in the data collection. Each of them completed the interviews with the women. The recall period between the pregnancy and the interview was on average 1 year and maximum 2 years. The interview was structured to assess demographic characteristics and medical history, knowledge about physical activity during pregnancy, performance of physical activity, and barriers to physical activity during pregnancy. The demographic and medical history section included questions about the participant’s age, her child’s age, marital status, educational level, occupation, number of pregnancies, number of children, attendance at antenatal visits, delivery method (vaginal versus cesarean), and self-rated health (poor, fair, good, very good, excellent). Questions on knowledge, attitude, and barriers to exercise were derived from validated questionnaires;7,15 questions were translated from English to Arabic and back translated by a different person to ensure accuracy of the content. The validated Arabic version of the International Physical Activity Questionnaire (IPAQ) was used to assess physical activity.16 The entire questionnaire was pre-tested on a population sample similar to that included in the study prior to the data collection period.
Data analysis
The variables were checked for accuracy before the analysis was undertaken. First, descriptive statistics for the whole sample were generated as follows: frequency for categorical variables and mean and standard deviation (SD) for continuous variables. Knowledge of the physical activity score during pregnancy was calculated (scale: 0–100), and indices of central tendency were analyzed for the summary score. The knowledge score was categorized as either “low” or “high” based on the median split. Total minutes of physical activity and minutes of walking, per week, were calculated for each participant. Based on self-reported calculations, women were classified as having either adequate or inadequate activity. Demographic and lifestyle factors were compared between those with adequate and inadequate activity. A chi-square test was used to compare the categorical variables, and t tests, for continuous variables. Logistic regression was employed to assess the correlates of adequate activity. The adjusted model included the following covariates: age, education, occupation, number of pregnancies, delivery mode, knowledge score, attitude toward necessity, and self-rated health. Covariates were selected a priori based on the literature review, and all covariates were entered into the model simultaneously. Model adequacy was checked with a Hosmer–Lemeshow test. Odds ratios and the associated 95% confidence intervals for variables in the final model were reported. All tests were two sided with an alpha level of 0.05, and the analyses were carried out with SPSS version 22.
Results
Participants included 274 women who had been pregnant within the previous 2 years. We approached 326 women; 1 was excluded because she had polio, 49 refused to participate, and 2 did not complete the form after the informed consent. Thus, we had a response rate of 84% (274/326; Figure 1). Participants had a mean age of 31.9 years (median = 31; range = 18–51), and the mean age of their most recently born child was 12.8 months (median = 12; range = 1–24). A majority of the women were married (70.4%), 56.7% had a college education, and 55.8% were housewives. A majority of the women attended pre-natal appointments (82.5%), and 66.4% had a vaginal delivery during childbirth. The mean number of pregnancies per woman was 3.5 (median =3; range = 1–12), and the mean number of children per woman was 3.1 (median = 3; range = 1–9; Table 1). The principal sources of information on physical exercise were the Internet, television, doctors, and books/magazines. A majority of the women (86%) reported that exercise during pregnancy was necessary. The mean score for knowledge about exercise during pregnancy was 77.7 (SD = 9.7; median = 75.0; range = 40–95).
Figure 1.
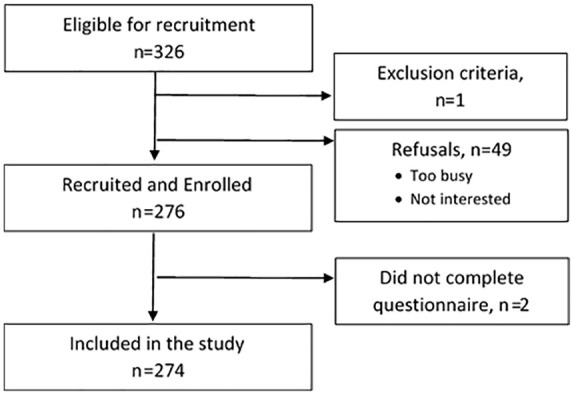
Flowchart for recruitment and enrollment into the study among recently pregnant women in Qassim, Saudi Arabia.
Table 1.
Demographic characteristics of 274 recently pregnant women in Qassim, Saudi Arabia.
| Variable | N | % |
|---|---|---|
| Age (years) | ||
| ⩽30 | 123 | 44.9 |
| >30 | 151 | 55.1 |
| Education | ||
| <Secondary | 105 | 38.3 |
| ⩾College | 169 | 61.7 |
| Occupation | ||
| Employed | 119 | 43.4 |
| Unemployed | 155 | 56.6 |
| Number of pregnancies | ||
| 1 | 50 | 18.2 |
| ⩾2 | 224 | 81.8 |
| Number of children | ||
| 1 | 68 | 24.8 |
| ⩾2 | 202 | 73.7 |
| Child age in months | 12.7 | 7.5 |
| Antenatal appointment | ||
| Yes | 226 | 82.5 |
| No | 47 | 17.2 |
| Delivery mode | ||
| Vaginal | 182 | 66.4 |
| C-section | 92 | 33.6 |
| Knowledge | ||
| <75: low | 131 | 47.8 |
| ⩾75: high | 143 | 52.2 |
| Is it necessary | ||
| Yes | 234 | 85.4 |
| No | 38 | 13.9 |
| Self-health | ||
| Excellent | 127 | 46.4 |
| Good–Very good | 111 | 40.5 |
| Poor–Fair | 36 | 13.1 |
More than half of the women (75%) reported engaging in exercise during their most recent pregnancy; however, only a portion of those women reported an adequate amount of time spent exercising (116/274 = 42%; Figure 2). Among the adequately active women (n = 116), the average minutes of exercise per day was 65.4 min (SD = 35.75). Walking was the most commonly reported type of exercise. Among women who walked adequately (72/274 = 26%), the average minutes of walking per day was 48.8 minutes (SD = 31.32). Among those who reported no physical exercise during pregnancy (n = 68), the following barriers were identified: tiredness (25.0%), dislike of exercise (16.7%), busy schedule (9.7%), childcare (13.9%), fear (18.1%), and lack of information (16.7%).
Figure 2.

Self-reported physical exercise during pregnancy among 274 recently pregnant women in Qassim, Saudi Arabia.
Univariate associations showed that attitude (i.e. exercise is necessary) and self-rated health were associated with adequate activity levels (Table 2). Among women who were adequately active, 93.0% reported that exercise during pregnancy was necessary compared with 80.9% of inactive women. Among women who were adequately active, 55.2% reported excellent health, 35.3% reported good to very good health, and 9.5% reported fair to poor health compared with 39.9%, 44.3%, and 15.8%, respectively, among inactive women.
Table 2.
Univariate associations between covariates and adequate activity during pregnancy among 274 recently pregnant women in Qassim, Saudi Arabia.
| Variable | Inadequate activity | Adequate activity | p value |
|---|---|---|---|
| Age (years) | |||
| ⩽30 | 41.1% (65) | 50.0% (58) | 0.145 |
| >30 | 58.9% (93) | 50.0% (56) | |
| Education | |||
| <Secondary | 39.9% (63) | 36.2% (42) | 0.537 |
| ⩾College | 60.1% (95) | 63.8% (74) | |
| Occupation | |||
| Employed | 35.4% (56) | 41.4% (48) | 0.317 |
| Unemployed | 64.6% (102) | 58.6% (68) | |
| Number of pregnancies | |||
| 1 | 20.9% (33) | 14.7% (17) | 0.187 |
| ⩾2 | 79.1% (125) | 85.3% (99) | |
| Delivery mode | |||
| Vaginal | 68.4% (108) | 63.8% (74) | 0.43 |
| C-section | 31.6% (50) | 36.2% (42) | |
| Knowledge | |||
| <75: low | 34.8% (55) | 39.7% (46) | 0.41 |
| ⩾75: high | 65.2% (103) | 60.3% (70) | |
| Is it necessary | |||
| Yes | 80.9% (127) | 93.0% (107) | 0.004 |
| No | 19.1% (30) | 7.0% (8) | |
| Self-health | |||
| Excellent | 39.9% (63) | 55.2% (64) | 0.03 |
| Good–Very good | 44.3% (70) | 35.3% (41) | |
| Poor–Fair | 15.8% (25) | 9.5% (11) | |
In the multivariate logistic model, age, number of pregnancies, attitude toward the necessity of exercise, and self-rated health were significantly associated with adequate time spent exercising during pregnancy (Table 3). Younger women (⩽30 years) were 1.7 times more likely to be adequately active than older women. Multiparous women (⩾2 pregnancies) were 2.4 times more likely to be adequately active. Women who reported they believed exercise was necessary were 2.7 times more likely to be adequately active. Women with excellent self-rated health were 2.5 times more likely to be adequately active compared to women who self-reported their health as fair to poor.
Table 3.
Adjusted logistic regression for the correlates of adequate physical exercise during pregnancy among 274 recently pregnant women in Qassim, Saudi Arabia.
| Variable | Odds ratio | 95% CI | p value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age (years) | ||||
| ⩽30 | 1.79 | 1.01 | 3.18 | 0.047 |
| >30 | Ref | |||
| Education | ||||
| <Secondary | Ref | |||
| ⩾College | 1.10 | 0.61 | 2.00 | 0.75 |
| Occupation | ||||
| Employed | Ref | |||
| Unemployed | 1.34 | 0.73 | 2.45 | 0.35 |
| Number of pregnancies | ||||
| 1 | Ref | |||
| ⩾2 | 2.41 | 1.13 | 5.14 | 0.02 |
| Delivery mode | ||||
| Vaginal | 1.34 | 0.78 | 2.31 | 0.29 |
| C-section | Ref | |||
| Knowledge | ||||
| <75: low | Ref | |||
| ⩾75: high | 1.34 | 0.79 | 2.29 | 0.28 |
| Is it necessary | ||||
| Yes | 2.71 | 1.20 | 6.13 | 0.02 |
| No | Ref | |||
| Self-health | ||||
| Excellent | 2.50 | 1.09 | 5.72 | 0.03 |
| Good–Very good | 1.27 | 0.55 | 2.94 | 0.58 |
| Poor–Fair | Ref | |||
CI: confidence interval.
Discussion
The study results showed that the majority of the women thought that physical exercise during pregnancy was necessary and had high knowledge about the appropriate types and amount of physical activity. Less than half of the women were either walking or exercising adequately (i.e. ⩾150 min/week). The study findings identified that age, number of pregnancies, attitude toward exercise, and self-rated health were significant correlates of adequate exercise during pregnancy. Self-reported barriers to exercise included personal barriers such as fatigue, time, childcare, and lack of information.
This study found that 42% reported exercising, 26% reported walking ⩾150 min per week, and walking was the most common form of exercise. These findings are consistent with previously published studies,8,17–19 although there is some variation across countries. A recent study from Brazil reported that 23% of women exercise during pregnancy and that nearly half of the women either reduce or stop exercising because of the pregnancy.20 A study from the United States showed that 29% exercised both before and during pregnancy, while an additional 4% initiated exercise during pregnancy.21 However, when we compare these estimates to the larger Saudi population, they are considered high. In a national survey, only 12% of the total Saudi population met the guidelines for physical exercise.12 Since a sedentary lifestyle is common outside of pregnancy, it is likely that women remain sedentary during pregnancy. Other studies show that women are more likely to decrease exercise time than they are to initiate exercise during pregnancy.22 There are two potential explanations for the findings: (a) either women in our sample overestimated the time that they spent exercising or (b) the high levels of knowledge/attitude reflect a true increase in exercise time during pregnancy.
This study found that age, number of pregnancies, attitude toward exercise, and self-rated health were significant correlates of adequate exercise during pregnancy. Other studies also identified education, income, not having other children in the home, exercise before pregnancy, and exercise guidance during pre-natal visits.22,23 The correlation between self-rated health and adequate exercise is a relevant one because self-rated health has been shown to be associated with psychological stress, objective health diagnosis, and body mass index among pregnant women.24,25 Since pregnant women are acutely aware of their health behavior as well as attending pre-natal care visits, it would be efficient for physicians to identify patients using self-rated health and to promote exercise as a way to improve this rating.
A comprehensive and theoretically driven review has outlined the most frequently reported barriers to physical exercise among pregnant women.6 Using the socio-ecological model, barriers were classified into intrapersonal (e.g. pregnancy-related symptoms, time constraints, lack of motivation) and interpersonal (e.g. lack of information, lack of support). Across the studies, intrapersonal barriers were most commonly cited.7–9 Examples included fatigue, nausea, physical pain, and bodily changes. The findings of the current study echo these same results; the barriers of fatigue, time, childcare, and lack of information were cited by 15%–25% of the women in the study. When future studies design interventions to target the barriers and help pregnant women increase physical exercise, pre-pregnancy exercise patterns should be considered.
The study’s strengths include an adequate sample size and previously validated assessment tools. However, the results of this study should be interpreted with a few limitations in mind. The study had a non-random sampling method, and data were collected at a single time point; hence, the sample may not be representative of the specified population of women. Also, we excluded women with any condition that would prevent them from exercising; therefore, study results are not generalizable for severely ill or disabled women. A degree of measurement error can be expected because of the self-reported data and the extended recall period, which on average was 1 year but maximum 2 years. Self-reported physical activity tends to be overestimated. The findings should be considered in light of these aforementioned limitations. However, we can observe that there is a striking difference in the level of awareness and knowledge about physical exercise during pregnancy between the proportion of women exercising adequately and those with inadequate activity. Therefore, we conclude that designing and implementing interventions to promote physical exercise during pregnancy is the appropriate next direction for researchers. We hypothesize that physical activity coaching, which includes goal setting and self-monitoring with a professional coach/trainer, be paired with pre-natal and post-natal visits. Coaching during this period around childbirth would not only keep women active but also help them to maintain appropriate weight levels throughout the process.
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Abeer A Alaglan  https://orcid.org/0000-0003-3919-4976
https://orcid.org/0000-0003-3919-4976
References
- 1. American College of Obstetricians and Gynecologists. Physical activity and exercise during pregnancy and the postpartum period. Obstet Gynecol 2015; 126(6): e135–e142. [DOI] [PubMed] [Google Scholar]
- 2. Barakat R, Perales M, Garatachea N, et al. Exercise during pregnancy. A narrative review asking: what do we know? Br J Sports Med 2015; 49(21): 1377–1381. [DOI] [PubMed] [Google Scholar]
- 3. Leite CF, do Nascimento SL, Helmo FR, et al. An overview of maternal and fetal short and long-term impact of physical activity during pregnancy. Arch Gynecol Obstet 2017; 295(2): 273–283. [DOI] [PubMed] [Google Scholar]
- 4. Perales M, Santos-Lozano A, Ruiz JR, et al. Benefits of aerobic or resistance training during pregnancy on maternal health and perinatal outcomes: a systematic review. Early Hum Dev 2016; 94: 43–48. [DOI] [PubMed] [Google Scholar]
- 5. Blaize AN, Pearson KJ, Newcomer SC. Impact of maternal exercise during pregnancy on offspring chronic disease susceptibility. Exerc Sport Sci Rev 2015; 43(4): 198–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Coll CV, Domingues MR, Gonçalves H, et al. Perceived barriers to leisure-time physical activity during pregnancy: a literature review of quantitative and qualitative evidence. J Sci Med Sport 2017; 20(1): 17–25. [DOI] [PubMed] [Google Scholar]
- 7. Evenson KR, Moos MK, Carrier K, et al. Perceived barriers to physical activity among pregnant women. Matern Child Health J 2009; 13(3): 364–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Krans EE, Gearhart JG, Dubbert PM, et al. Pregnant women’s beliefs and influences regarding exercise during pregnancy. J Miss State Med Assoc 2005; 46(3): 67–73. [PubMed] [Google Scholar]
- 9. Pereira MA, Rifas-Shiman SL, Kleinman KP, et al. Predictors of change in physical activity during and after pregnancy: project viva. Am J Prev Med 2007; 32(4): 312–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. The World Bank. Fertility rate by country 2015, https://data.worldbank.org/indicator/SP.DYN.TFRT.IN/
- 11. Farrag O, Rahman M, Rahman J, et al. Attitude towards fertility control in the eastern province of Saudi Arabia. Saudi Medical Journal 1983; 4(2): 111–116. [Google Scholar]
- 12. El Bcheraoui C, Tuffaha M, Daoud F, et al. On your mark, get set, go: levels of physical activity in the Kingdom of Saudi Arabia, 2013. J Phys Act Health 2016; 13(2): 231–238. [DOI] [PubMed] [Google Scholar]
- 13. Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: a brief review. East Mediterr Health J 2004; 10(4–5): 663–670. [PubMed] [Google Scholar]
- 14. General authority for statistics. Kingdom of Saudi Arabia, https://www.stats.gov.sa/sites/default/files/en-qassim-pulation-by-gender-govnernorate-nationality_0.pdf
- 15. Chasan-Taber L, Schmidt MD, Roberts DE, et al. Development and validation of a Pregnancy Physical Activity Questionnaire. Med Sci Sports Exerc 2004; 36(10): 1750–1760. [DOI] [PubMed] [Google Scholar]
- 16. Helou K, El Helou N, Mahfouz M, et al. Validity and reliability of an adapted Arabic version of the long International Physical Activity Questionnaire. BMC Public Health 2017; 18(1): 49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Cioffi J, Schmied V, Dahlen H, et al. Physical activity in pregnancy: women’s perceptions, practices, and influencing factors. J Midwifery Womens Health 2010; 55(5): 455–461. [DOI] [PubMed] [Google Scholar]
- 18. Duncombe D, Wertheim EH, Skouteris H, et al. Factors related to exercise over the course of pregnancy including women’s beliefs about the safety of exercise during pregnancy. Midwifery 2009; 25(4): 430–438. [DOI] [PubMed] [Google Scholar]
- 19. Ribeiro CP, Milanez H. Knowledge, attitude and practice of women in Campinas, São Paulo, Brazil with respect to physical exercise in pregnancy: a descriptive study. Reprod Health 2011; 8: 31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Nascimento SL, Surita FG, Godoy AC, et al. Physical activity patterns and factors related to exercise during pregnancy: a cross sectional study. PLoS ONE 2015; 10(6): e0128953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Harris ST, Liu J, Wilcox S, et al. Exercise during pregnancy and its association with gestational weight gain. Matern Child Health J 2015; 19(3): 528–537. [DOI] [PubMed] [Google Scholar]
- 22. Nascimento SL, Surita FG, Cecatti JG. Physical exercise during pregnancy: a systematic review. Curr Opin Obstet Gynecol 2012; 24(6): 387–394. [DOI] [PubMed] [Google Scholar]
- 23. Gaston A, Cramp A. Exercise during pregnancy: a review of patterns and determinants. J Sci Med Sport 2011; 14(4): 299–305. [DOI] [PubMed] [Google Scholar]
- 24. Christian LM, Iams J, Porter K, et al. Self-rated health among pregnant women: associations with objective health indicators, psychological functioning, and serum inflammatory markers. Ann Behav Med 2013; 46(3): 295–309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Coussons-Read ME. “Thinking healthy” in pregnancy: a comment on Christian et al. Ann Behav Med 2013; 46(3): 258–259. [DOI] [PubMed] [Google Scholar]