

Abstract
Background: Indonesia suffers growing health problems such as obesity, diabetes, and other metabolic syndromes with dietary habit as one of risk factors. To control the lipid and glycaemic profile, high fibre intake has been recommended. This study administered 400g/day vegetable intake with its fiber contents and observed the effects in lipid profile and glycaemic control.
Design: A parallel study of 30 pairs of menopausal women match paired in overweight, menopause, hyperlipidaemia, age, etc randomly divided into two groups (vegetable and control). The baseline data obtained from questionnaire and preliminary bloodwithdrawn of consented participants, then matched the characteristics included the results of lipid profile and glycated albumin. The administration was conducted for 21days by providing 400g/day of vegetable to the vegetable group subjects. Nutrition assessments were conducted at the baseline, middle, and final period. The data were analysed by using the unpaired and paired t-test.
Results: Significant results (p<0.05) were seen in biochemical variables in the lipid profile of total cholesterol, LDL cholesterol, and HDL cholesterol and body weight and BMI within the vegetable group. Significant results for the same variables were shown between vegetable and control group at the final data (p<0.05). The nutrition assessments result showed significances (p<0.05) within vegetable group and between two groups on the final data. After 21 days, significant decreases were found on the intakes of energy, lipids, carbohydrates (p<0.05), while vegetable intake and fiber intake showed significant increases (p<0.05).
Conclusion: These data suggest that maintaining a healthy diet of 400g/d vegetable can be effective in weight management and lipid profile control.
Significance for public health.
Growing health problems in Indonesia in non-communicable diseases increases awareness on how to prevent the diseases. Despite the government movements to improve healthy lifestyle habits by encouraging healthy movements for daily life, it doesn’t show any favorable impacts on Indonesian health, especially when non-communicable disease prevalence tends to increase years by years. One of the movement encouragements is to adapt more vegetable consumption in one’s daily life in the hope of improving the health quality of the people. However, there is limited number of studies on vegetable intake and its effects on health and also how it can be implemented on society. This study may be the first study on vegetable consumption and its effect on health in Indonesia, in the hope of its benefit to be adjusted on larger population in Indonesia.
Key words: Vegetable intake, body weight, hyperlipidemia, lipid profile, menopause
Introduction
Indonesia, like most countries, has been reported as having a high prevalence of overweight and obesity, especially in women1. According to Riskesdas (Basic Health Research), adult obesity in Indonesia has been increasing since the first national basic survey held in 2007, which made them more susceptible to lifestyle-related diseases.1 More than half of the major cause of death in Indonesia was caused by lifestyle-related diseases, which the highest three were stroke, heart diseases, and diabetes mellitus.1-4 These diseases are preventable by maintaining a healthy lifestyle, especially a balanced nutrition. At the previous study, it was found that the food habit of Jakarta’s stay-at-home women was to consume significant amounts of lipid sources, few vegetables, and few fibers.5
Higher fiber intake, especially from vegetables, is recommended to maintain a healthy lifestyle through dietary habits. Acting as glycemic and plasma lipid control that inhibits glucose absorption as layer on direct absorption, fiber can be a good way to modify diet in both diabetes prevention and treatment, with the goal of improving blood glucose levels control, lipid profiles, and blood pressure to reduce cardiovascular disease risk in diabetes patients.6-8 The risk of diabetes can be reduced by 33% increasing fiber intake.6 High intake of fruits, vegetables, and grains can increase the fiber intake.7
The Indonesian Ministry of Health recommends 300g/d of fruit and vegetable intake to be included in Indonesian food habits.9-12 These recommendations were carefully considered based on the Institute of Medicine and other agencies.13-15 Although higher fruit and vegetable intake daily has been suggested as a more efficient source of fiber intake, investigation in humans has been limited, especially in Indonesia. Many investigations have been conducted to identify beneficial combination of vegetables that has effects on health especially reducing cardiovascular diseases (CVD) risk and other lifestyle related diseases.6-8 As it is already clearly understood that vegetable intake has beneficial effects in controlling CVD, it is essential to assess its effect practically, since this will provide more direct evidence for better dietary guidelines. Therefore, this study was designed to prove the practical effects of recommended daily vegetable intake especially in controlling BMI, plasma lipids, and glycemia.
Materials and Methods
The study was conducted started from September 2017 to February 2018 with overweight menopausal women who were selected from 27 community health centres in 4 districts in southern areas of Jakarta. The study protocol and procedures were approved by the Ethical Committee of the Faculty of Medicine, Universitas Indonesia (Approval number No891/UN2.F1/ETIK/2017), conducted in accordance with the Helsinki Declaration of the World Medical Association. Written informed consent was obtained from all the participants in the study starting from the first screening process.
The first screening step was reviewing the data from community health centers and selecting overweight women. Next, 334 overweight women (BMI >25k g/m2) were approached, informed about the study, and asked to participate. Participants who agreed were provided with written informed consent form and returned the form to the researchers signed. Researchers measured their anthropometric status once again and assessed their basic data. Based on inclusion criteria of those who were overweight, menopausal, stay-at-home women with normal levels of activity, with exclusion criteria if they received psychological or pharmacological treatment, suffered from liver cirrhosis, nephritic syndrome, hyperthyroid, and steroid treatment, infectious diseases, and diabetes. After passing the first screening, the second screening measured their cholesterol and glucose level by simple peripheral tests. Inclusion criteria at the second screening step were subjects with high cholesterol (>200 mg/dL) and prediabetic glucose level (140 mg/dL – 199 mg/dL). After passing the second screening, at the last screening blood was withdrawn from 108 subjects to analysis their lipid profile and glycaemic albumin. After obtaining the analysis results, there were 60 eligible subjects assigned to one of two parallel group, in 1:1 ratio, 30 subjects for the vegetable group and 30 subjects for the control group (Figure 1).
Study design
This study was a parallel study comprising 21 days in which participants who had their blood drawn at the beginning of the study as the baseline data, would be treated as the vegetable group and the control group, and would have their blood drawn at the end of study as the final data. The blood withdrawn was analysed for the subjects’ biochemical variables, lipid profile and glycated albumin. Glycated albumin was used to describe the glucose value based on albumin turn over, in 1-2 weeks, which is much shorter than erythrocyte, resulted in easier treatment monitoring.16 Lipid profile analysis of total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides was conducted.
Diet
Four hundred grams of vegetables were provided in two plastic boxes with one packet each of mayonnaise and dressing, traditional peanut sauce and chili sauce which they could use according to their preferences. These vegetables were weighed before cooking. For the cooking process, blanching method was used to maintain the maximum nutritional value of the vegetables. The vegetables were divided into two packs, each with 200 grams of vegetables and had on average 150 kcal per 400 g vegetables. The vegetable group were given 400 g/day, while control group was given nutrition education. The subjects in the vegetable group were asked to maintain their usual dietary habits, only with the addition to include our 400 g/day vegetables in their diet. As for the activities, both groups were asked to maintain their usual daily activities. The vegetables were delivered daily to each subject in the vegetable group, while the control group were visited twice a week to recall their dietary intake and to receive nutrition education. The nutrition education was conducted in every visit to all control group subject for 14 days. The nutrition education was emphasized on the importance of consuming recommended daily vegetable and fruit intake, of 400 g a day, the same amount as vegetable pack provided for vegetable group. The material provided was one brochure of “Tumpeng Gizi Seimbang”, the promotion of Indonesian daily balance nutrition in a form of pyramid with local name.
Nutrition intake estimation
The nutrition assessment with 3 day 24 hour recall method were implemented three times; baseline, middle week, and final. The nutrition assessment were conducted by nutritionists who had at least one year experience monitoring and supervising study. Energy, protein, lipids, carbohydrates, fiber, and vegetable intake were obtained from each nutrition assessment. The fiber and vegetable intake included all intake during the study, including the 400 g vegetables we provided for the vegetable group.
Statistical analysis
The analyses were conducted with paired and unpaired t-test using Microsoft Excel Software 2013.
Figure 1.
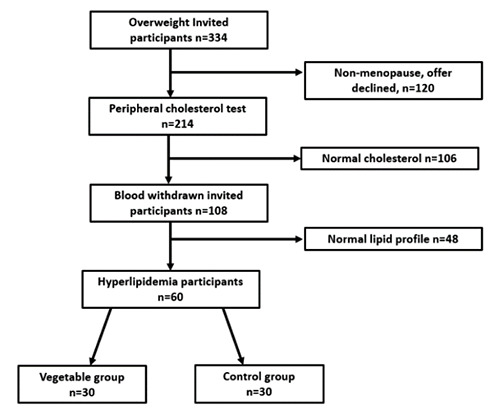
The subject recruitment process.
Results
A total of 13 subjects from the 60 subjects dropped out of the study; thus 47 women (24 in the vegetable group and 23 in the control group) completed the follow up and the study, respectively. Reasons for dropping out included personal reasons, refusing blood withdrawal at the end of the study, and exclusion due to incomplete records. The results for the 47 subjects who completed the follow-up were analyzed. Table 1 shows the characteristic and biochemical parameters of the subjects by group (vegetable n=24, control n=23). There is no significant difference in baseline values between the vegetable group and the control group. All subjects were overweight, and their biochemical values were match paired.
The final data of the vegetable group and the control group are shown in Table 1. The vegetable group shows significant differences within the group in weight, BMI, total cholesterol, LDL cholesterol, and HDL cholesterol (P<0.05). In the vegetable group, weight, BMI, total cholesterol, LDL cholesterol, and HDL cholesterol were significantly reduced at final data compared with baseline data. These was not found in the control group (P>0.05). There were no statistical differences in glycated albumin and triglycerides value between the vegetable and control groups or changes in these values during the 21-day study period (p<0.05).
Table 2 shows energy and nutrient intakes of both groups at baseline and final. Within the vegetable group, energy, lipids, carbohydrate, fiber, and vegetable intake show the significant differences (p<0.05), except protein intake (p>0.05). There is no significant difference with the control group (p>0.05). At the final data of the nutrition assessment, the vegetable group and the control group show significant differences p<0.05), except for protein intake (p>0.05) (Figure 2).
Discussion
The study involved the real implementation of 400 g/day vegetable intake in Indonesians, since there is the recommendation, of 300-500 g vegetables per day (3-5 servings) for children and young adolescents, and 400-600 g vegetables per day (4-6 servings) for adults, from the government but the actual implementation has not yet been observed.9-12 This recommendation was observed based the WHO recommendation of vegetable and fruit intake as part of healthy diet to reduce non-communicable disease risk and maintaining healthy lifestyle, which is about 250 g vegetables and 150 g fruit.15 The Indonesian government has adopted this recommendation as part of The Healthy Society Movement, which is known as Gerakan Masyarakat Sehat, or GERMAS in Indonesian, with the main dietary movement is about eating more vegetable and fruit as part of daily dietary habit with the recommendation of 300-500 g/day by promoting that fruit and vegetables contribute as vitamin and minerals, antioxidants, and fiber sources.9-12
Figure 2.
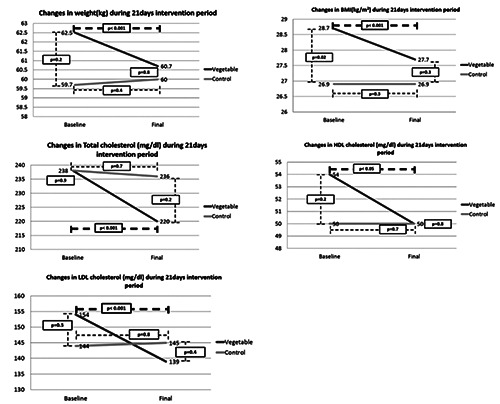
Changes in parameters that show significances (p<0.05).
In this study we tried to give 400 g/day of vegetable, which can be considered as fostering a new dietary habit for Indonesians, including higher amount of salad using mayonnaise, dressings and traditional dressing, peanut sauce and chili sauce. Although there is a recommendation to consume certain amount of vegetables to maintain healthy-lifestyle, the national survey Basic Health Research conducted by the government showed that 98% of Indonesians do not have the dietary habit of eating vegetables.1 This means that almost all Indonesians do not include vegetable in their daily dietary habit and through this study, a new simple dietary habit was introduced.
We developed 8 daily menus of vegetable combinations to serve 400 g/day of vegetables, with their preferred dressings. Then we used these in a 21-day cycle. Indonesians consumed vegetables by boiling and serving them with traditional dressings such as peanut sauce, coconut flakes, brown sugar sauce, etc, dipping it in chili sauce and cane sugar sauce, or stir-frying like in Chinese cuisine. The other cooking method was putting the vegetables in soup, either clear soup or coconut milk soup. Vegetables are commonly used in Indonesian cuisine. However, economic development has changed people’s food habit. They tended to eat easily prepared food and tasty items such as fried foods. These also influences people to buy meat products more than vegetables and there is a new food culture of foreign fast foods has fascinated the Indonesians, which has made vegetable intake decreased greatly. In this situation, people should adapt better habits, which are simple and easily adapted to daily life.
The subjects were stay at home housewives with some knowledge about nutrition. The subjects understood that vegetables are good for their health. However, they tended not to maintain a certain amount of vegetable servings as their daily food habit and they had no idea of what an ideal serving looks like. The study period of intervention was 21 days, which was considered a better period for the turnover rate of glycated albumin which is 2-3 weeks and its effects on lipid profiles.16 There was such a decrease found in the study. We also found significant changes in lipid profiles, specifically in controlling total cholesterol, LDL cholesterol, and HDL cholesterol levels. Significant differences were found in body weight and BMI of the subjects, which suggests that thesecan be controlled by high level vegetable intake.
To control body weight, some studies shows that diets resulted on lower carbohydrate intake includes protein from vegetables and oil can significantly reduce LDL cholesterol levels, which can contribute in reducing CVD risk.17-24 In reducing CVD risk, studies show that diet rich in composition of fruit and vegetables has beneficial effects on metabolic syndromes by reducing LDL cholesterol levels.17-21 Diets such as Mediterranean diet which focus on carbohydrate and protein sources from legumes and soy, are associated with reduction of coronary artery disease progression, weight loss, and LDL cholesterol level.19,20 The diet would affect on HDL Choylesterol level as the lipid intake reduced, which low level will be a concern. CVD risk is best expected to be reduced by lowering LDL choleysterol level without repressing HDL cholesterol level.17-21 Lower triglyceride concentrations are observed with low carbohydrate intake, which might reflected lower glycemic load and gluten.22-24 However, despite showing slight reduction in triglyceride concentration, there was no significant differences found in triglyceride concentrations in this study.
The vegetable group subjects were provided with 400 g vegetables delivered to their home every day. Every delivery, the subjects were asked to keep their vegetable wastes if any and return the wastes to researchers to be weighed. The vegetable intake reached 99% of 400 g/d at the final data, leaving wastes of only 1%. The intake had the tendency to increase by the end of the study, since the subjects were forming new dietary habits during our study. According to the nutrition assessment results, there were significant decreases in energy intake, lipid intake, and carbohydrate intake, and significant increases in fiber and vegetable intake.
Table 1.
Characteristic and biochemical parameters of the subjects by group.
| Vegetable n=24 | Control n=23 | |||
|---|---|---|---|---|
| Variable | Baseline | Final | Baseline | Final |
| Age (years) | 55 ± 3.2 | 55 ± 3,2 | 55.8 ± 3.2 | 55.8 ± 3.2 |
| Height (cm) | 147.5 ± 5.7 | 147.5 ± 5,7 | 149 ± 4.5 | 149 ± 4.5 |
| Weight (kg) | 62.5 ± 7 | 60.3 ± 7* | 59.7 ± 6.4 | 59.9 ± 6.4 |
| BMI (kg/m2) | 28.7 ± 2.6 | 27.7 ± 2.6* | 26.9 ± 2.7 | 26.9 ± 2.7 |
| Glycated albumin (%) | 13.6 ± 1.6 | 13.5 ± 1.7 | 13.6 ± 2 | 13.6 ± 1.8 |
| Total cholesterol (mg/dL) | 238 ± 36.5 | 220 ± 33.5* | 238 ± 37.6 | 236 ± 44.2 |
| LDL cholesterol (mg/dL) | 154 ± 28 | 139 ± 24.5* | 144 ± 30 | 145 ± 32 |
| HDL cholesterol (mg/dL) | 54 ± 11.6 | 50 ± 9* | 50 ± 6.2 | 50 ± 6.1 |
| Triglyceride (mg/dL) | 135 ± 51.8 | 131 ± 69 | 157 ± 74 | 141 ± 68.8 |
*Significant within the same group; values are mean ± SD.
Table 2.
Energy and nutrient intakes of both groups at baseline and final.
| Vegetable n=24 | Control n=23 | |||||
|---|---|---|---|---|---|---|
| Baseline | 14 days | Final | Baseline | 14 days | Final | |
| Energy (kcal/day) | 2055 ± 321 | 1615 ± 176 | 1607 ± 128* | 2005 ± 380 | 1943 ± 248 | 2009 ± 332° |
| Protein (g/d) | 57 ± 14 | 46 ± 14 | 49 ± 12 | 56 ± 18 | 53 ± 17 | 51 ± 14 |
| Lipids (g/d) | 89 ± 29 | 70 ± 19 | 69 ± 24* | 97 ± 30 | 83 ± 25 | 86 ± 27° |
| Carbohydrate (g/d) | 260 ± 39 | 205 ± 64 | 201 ± 52* | 239 ± 54 | 258 ± 32 | 264 ± 41° |
| Fiber (g/d) | 9.5 ± 3 | 21 ± 3 | 23 ± 4* | 11 ± 3 | 10 ± 2 | 10 ± 3° |
| Vegetable intake (g/d) | 83 ± 27 | 387 ± 11 | 393 ± 5* | 85 ± 11 | 88 ± 17 | 94 ± 30° |
*Significant within the same group
°significant on final vegetable and control; values are mean ± SD.
These results may be caused by the high portion size of added vegetable in the daily dietary habit. Energy intake, lipid intake and carbohydrate intake were reduced by including 400 g/day of vegetables compared with having no added vegetable at all in previous daily food habit. There are studies which suggested that meal intake was reduced by eating a double portion of salad; eating a large portion of vegetable is an effective strategy for increasing satiety and reducing overall energy intake.25-29 Adding large portions of low energy dense salad decreased meal energy intake by 11-12% by increasing fullness while adding few calories, so that intake is reduced during the entire meal.28,29 Other studies have shown similar effects on meal energy intake by adding a fixed preload of low-energy-dense soup or fruit and have examined such factors as food type, macronutrient, energy, and food volume.26,27 Eventually, calorie intake reduction has an effect on body weight loss rather than metabolic changes.29-31
Furthermore, the amount of vegetable could provide fiber, which contributed to lowering cholesterol levels and is expected to reduce the risk of CVD.32,33 In addition to the other reasons, LDL cholesterol reduction was probably caused by lower saturated fat intake, which has beneficial effect in reducing insulin resistance and chronic inflammation and contributes to lower risk of CVD.32,33 Another study of lowfat dairy diets emphasizing higher intake of fruits and vegetables shows an associated improvement of the serum lipid profile.34
Vegetables are nutrient-dense foods, have dietary fibers which can increase cholecystokinin responses, a hormone responsible for food satiety and slowing down gastric emptying process. Insulin sensitizing potential of leafy vegetables is suggested as adjuvants for oral hypoglycemic drugs.35,36 These features of vegetables have been used in designing low glycemic response food products. It was suggested that diet mainly in vegetables consumptions without changing in regular dietary habit, has similar features as low-fat foods consumption, the ability to maintain low glycemic response that enhance satiety, insulin sensitivity, and low postprandial insulin secretion.37 After 400 g/day of vegetables intake, there is no significant result found on glycated albumin. This may lead to the suggestion of weight control might has more influence in insulin resistance than the vegetable itself. Another study found that unless there is favorable effect on body weight, diets of fruit and vegetable would have indirect control in insulin resistance.38 The nutrition education to the control group was also to emphasize the importance of eating 400 g/day vegetables as recommended, with one brochure of daily balance nutrition as tools. This one brochure was intended to make the subjects had easier understanding towards daily food consumption with the goal to encourage dietary habit of increase their daily vegetable intake. By this nutrition education, the control group managed to increase vegetable intake by 10 g/day. There is no significance difference found at the final, indicating by nutrition education itself for 21 days would not be enough to change dietary habit. Longer periods of nutrition education would have better results in metabolic syndrome control, which may take months to see the effects.37
The limitation of this study is its limited length: there might be more beneficial effects on longer study periods. There was no significant difference in glycated albumin levels, which suggested that a longer period of study may have control on blood glucose level. Another limitation is that daily visit must be done to provide the subjects with vegetable packs, which the subjects might feel constantly reminded to consume the vegetable packs. Further study on daily consumption of 400 g per day effects on glycemic response in the subject is recommended. Another recommendation for future study is whether the 400 g per day vegetable consumption per day has similar outcome on overweight women in younger age (non-menopausal).
Conclusions
In conclusion, the results of this study show how common overweight and obesity problem associated with metabolic syndrome. This study can present a confirmation on preventing lifestyle-related disease, especially CVD, by practical dietary recommendation. High vegetable diet is an effective dietary habit option for people suffers from overweight and a high lipid profile, with controlling body weight and lipid profiles as the final goal. Better strategies for health and nutrition education particularly in community should be be directed carefully for the better implementation of recommended dietary guidelines.
Acknowledgments
We gratefully thank all supporting staffs such as the research assitants, all health community centers and their staffs, the subjects of our study, the research group of Kewpie, and Prof. Andrew Durkin of Indiana Bloomington University, USA, for his generous help of the article English proof-reading.
References
- 1.Ministry of Health Republic of Indonesia Research and Development Board. [National Report of Basic Health Research 2018].[Report in Indonesian]. Laporan Nasional Riskesdas: 2018. [Google Scholar]
- 2.Ministry of Health Republic of Indonesia. [Penyakit Jantung Penyebab Kematian Tertinggi, Kemenkes Ingatkan Cerdik].[in Indonesian]. Ministry of Health: 2017. Available from: http://www.depkes.go.id/pdf.php?id=17073100005 Indonesian [Google Scholar]
- 3.Ministry of Health Republic of Indonesia. [Tekan Angka Kematian Melalui Program Indonesia Sehat].[in Indonesian]. Ministry of Health: 2017. Available from: http://www.depkes.go.id/article/view/17061600003/tekan-angka-kematianmelalui-program-indonesia-sehat-dengan-pendekatan-keluarga.html Indonesian [Google Scholar]
- 4.Ministry of Health Directorate General for Diseases Control and Prevention. Kebijakan dan Startegi Pencegahan dan Pengendalian Stroke di Indonesia].[in Indonesian]. Ministry of Health: 2017. Available from: http://p2ptm.kemkes.go.id/uploads/VHcrbkVobjRzUDN3UCs4eUJ0dVBndz09/2017/10/Kebijakan_dan_Strategi_Pencegahan_dan_Pengendalian_Stroke_di_Indonesia_dr_Lily_Sriwahyuni_Sulistyowati_MM1.pdf Indonesia [Google Scholar]
- 5.Kartiko Sari I, Oktaviana D, Utari DM. A nutrition survey and food patterns in predominantly middle-income housewives in Jakarta. Asian J Diet 2019;1:4-11. [Google Scholar]
- 6.Schulze MB, Schulz M, Heidemann C, et al. Fiber and magnesium intake and incidence of type 2 diabetes: a prospective study and meta-analysis. Arch Intern Med 2007;167:956-65. [DOI] [PubMed] [Google Scholar]
- 7.American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010;33:S64-S71.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.InterAct Consortium. Dietary fibre and incidence of type 2 diabetes in eight European countries: the EPIC-InterAct Study and a meta-analysis of prospective studies. Diabetologia 2015;58:1394-408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ministry of Health Republic of Indonesia. [Guide for Nutrition Balance Government Act No 41 of 2014].[in Indonesian]. Peraturan Menteri Kesehatan Republik Indonesia Nomor 41 tahun 2014 tentang Pedoman Gizi Seimbang; 2014. [Google Scholar]
- 10.Ministry of Health Republic of Indonesia. [Recommended Dietary Allowance for Indonesian Health Minister Act No 75 of 2013].[in Indonesian]. Peraturan Menteri Kesehatan Republik Indonesia Nomor 75 Tahun 2013 tentang Angka Kecukupan Gizi yang Dianjurkan bagi Bangsa Indonesia; 2013. [Google Scholar]
- 11.Ministry of Health Republic of Indonesia. [The Book of Guide for GERMAS, Healthy Society Movement.]. Buku Panduan GERMAS, Gerakan Masyarakat Hidup Sehat; 2016. [Google Scholar]
- 12.The President of Republic of Indonesia. [The President Instructions No 1 of 2017 about Healthy Society Movement]. [in Indonesian]. Instruksi Presiden Republik Indonesia Nomor 1 Tahun 2017 tentang Gerakan Masyarakat Hidup Sehat; 2017. [Google Scholar]
- 13.Hardinsyah H, Riyadi H. [Kecukupan Energi, Protein, Lemak, dan Karbohidrat].[Article in Indonesian]. Proceedings National Congress “Widyakarya Nasional Pangan dan Gizi X”, November 2012, Jakarta. Available from: https://www.researchgate.net/publication/301749209_KECUKUPAN_ENERGI_PROTEIN_LEMAK_DAN_KARBOHIDRAT [Google Scholar]
- 14.Institute of Medicine. Dietary reference intake for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington (DC): The National Academies Press; 2005. [Google Scholar]
- 15.WHO. Diet nutrition and the prevention of chronic diseases. Geneva; WHO: 2003. Available from: http://www.who.int/elena/titles/fruit_vegetables_ncds/en/ [Google Scholar]
- 16.Koga M, Kasayama S. Clinical impact of glycated albumin as another glycemic control marker. Endocr J 2010;57:751-62. [DOI] [PubMed] [Google Scholar]
- 17.Altman DG, Schulz KF, Moher D, et al. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med 2001;134:663-94. [DOI] [PubMed] [Google Scholar]
- 18.Mosca L, Mochari H, Christian A, et al. National study of women’s awareness, preventive action, and barriers to cardiovascular health. Circulation 2006;113:525-34. [DOI] [PubMed] [Google Scholar]
- 19.Esposito K, Marfella R, Ciotola M, et al. Effect of a mediterranean- style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA 2004;292:1440-6. [DOI] [PubMed] [Google Scholar]
- 20.Salas-Salvadó J, Bulló M, Babio N, et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care 2011;34:14-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Azadbakht L, Mirmiran P, Esmaillzadeh A, et al. Beneficial effects of a dietary approaches to stop hypertension eating plan on features of the metabolic syndrome. Diabetes Care 2005;28:2823-31. [DOI] [PubMed] [Google Scholar]
- 22.Reaven GM. The insulin resistance syndrome: definition and dietary approaches to treatment. Annu Rev Nutr 2005;25:391-406. [DOI] [PubMed] [Google Scholar]
- 23.Jenkins 25DJ, Kendall CW, Vidgen E, et al. High-protein diets in hyperlipidemia: effect of wheat gluten on serum lipids, uric acid, and renal function. Am J Clin Nutr 2001;74:57-63. [DOI] [PubMed] [Google Scholar]
- 24.Liu S, Manson JE, Stampfer MJ, et al. Dietary glycemic load assessed by food frequency questionnaire in relation to plasma high-density-lipoprotein cholesterol and fasting plasma triacylglycerols in postmenopausal women. Am J Clin Nutr 2001;73:560-6. [DOI] [PubMed] [Google Scholar]
- 25.Yao M, Roberts SB. Dietary energy density and weight regulation. Nutr Rev 2001;59:247-58. [DOI] [PubMed] [Google Scholar]
- 26.Flood JE, Rolls BJ. Soup preloads in a variety of forms reduce meal energy intake. Appetite 2007;49:626-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Flood-Obbagy JE, Rolls BJ. The effect of fruit in different forms on energy intake and satiety at a meal. Appetite 2009;52:416-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rolls BJ, Roe LS, Meengs JS. Salad and satiety: Energy density and portion size of a first-course salad affect energy intake at lunch. J Am Diet Assoc 2004;104:1570-6. [DOI] [PubMed] [Google Scholar]
- 29.Roe LS, Meengs JS, Rolls BJ. Salad and satiety. The effect of timing of salad consumption on meal energy intake. Appetite 2012;58:242-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Foster GD, Wyatt HR, Hill JO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med 2003;348:2082-90. [DOI] [PubMed] [Google Scholar]
- 31.Samaha FF, Iqbal N, Seshadri P, et al. A low-carbohydrate as compared with a low-fat diet in severe obesity. N Engl J Med 2003;348:2074-81. [DOI] [PubMed] [Google Scholar]
- 32.Anderson JW, Randles KM, Kendall CW, Jenkins DJ. Carbohydrate and fiber recommendations for individuals with diabetes: a quantitative assessment and metaanalysis of the evidence. J Am Coll Nutr 2004;23:5-17. [DOI] [PubMed] [Google Scholar]
- 33.Kennedy A, Martinez K, Chuang CC, et al. Saturated fatty acidmediated inflammation and insulin resistance in adipose tissue: mechanisms of action and implications. J Nutr 2009;139:1-4. [DOI] [PubMed] [Google Scholar]
- 34.Appel LJ, Sacks FM, Carey VJ, et al. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: results of the OmniHeart randomized trial. JAMA 2005;294:2455-64. [DOI] [PubMed] [Google Scholar]
- 35.Manchali S, Murthy KNC, Patil BS. Crucial facts about health benefits of popular cruciferous vegetables. J Functs Foods 2012;4:94-106. [Google Scholar]
- 36.Platel K, Srinivasan K. Plant foods in the management of diabetes mellitus: vegetables as potential hypoglycemic agents. Mol Nutr Food Res 1997;4:68-74. [DOI] [PubMed] [Google Scholar]
- 37.Imai S, Fukui M, Ozasa N, et al. Eating vegetables before carbohydrates improves postprandial glucose excursions. Diabet Med 2013;30:370-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Boeing H, Bechthold A, Bub A, et al. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr 2012;51:637-63. [DOI] [PMC free article] [PubMed] [Google Scholar]