

Abstract
Survival rates for patients following liver transplantation exceed 90% at 12 months and approach 70% at 10 years. Part 1 of this guideline has dealt with all aspects of liver transplantation up to the point of placement on the waiting list. Part 2 explains the organ allocation process, organ donation and organ type and how this influences the choice of recipient. After organ allocation, the transplant surgery and the critical early post-operative period are, of necessity, confined to the liver transplant unit. However, patients will eventually return to their referring secondary care centre with a requirement for ongoing supervision. Part 2 of this guideline concerns three key areas of post liver transplantation care for the non-transplant specialist: (1) overseeing immunosuppression, including interactions and adherence; (2) the transplanted organ and how to initiate investigation of organ dysfunction; and (3) careful oversight of other organ systems, including optimising renal function, cardiovascular health and the psychosocial impact. The crucial significance of this holistic approach becomes more obvious as time passes from the transplant, when patients should expect the responsibility for managing the increasing number of non-liver consequences to lie with primary and secondary care.
Keywords: liver transplantation, guideline
Introduction
Following successful liver transplant (LT), 12-month patient and graft survival rates in the UK exceed 90% and 80%, respectively.1 The 10-year survival approaches 70%, and transplant services have an ever-increasing population of long-term survivors.2 Kidney transplant services repatriate their transplant recipients to referrers soon after surgery, whereas liver services have historically been more cautious.3 However, as numbers increase, some aspects of post-operative care are being redistributed to referrers.
Part 2 of this two-part guideline examines:
Organ donation, organ allocation and organ types.
LT surgery and post-operative period.
How immunosuppression should be managed.
How the patient should be managed post-LT.
Transplant outcomes.
Organ donation, organ allocation and organ types
Organ donation
Figure 1 outlines the source of organs and their relative contributions.4–6
Figure 1.
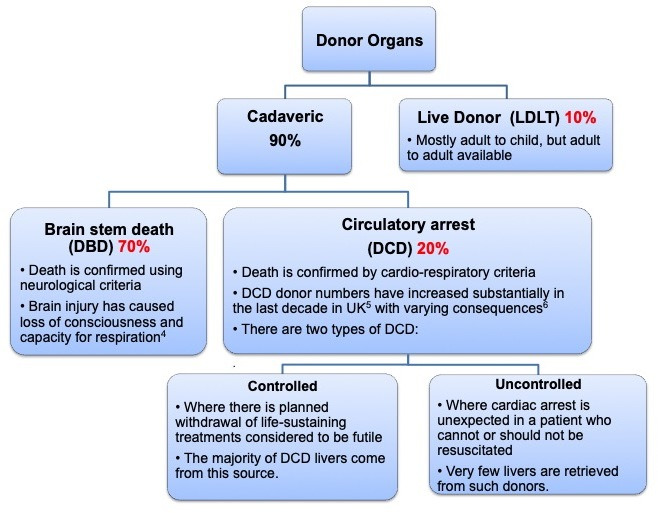
Sources of livers donated for transplantation. DBD, donor after brain death; DCD, donor after cardiac death; LDLT, live donor liver transplantation.
Organ allocation
Organ allocation has long been debated across many healthcare systems. Organs can be allocated according to ‘need’ (sickest first), ‘utility’ (best use of organ) or ‘benefit’ (combines need and utility). Most countries have adopted need as the main criterion. The UK recently agreed to use the Transplant Benefit Score (TBS) to allocate donor after brain death (DBD) livers, and it is likely that donor after cardiac death (DCD) livers will follow the same process. TBS contains 21 donor and recipient variables, including donor age, cause of death, body mass index (BMI), diabetes, recipient’s indication for transplant, creatinine, sodium, bilirubin, albumin, waiting time, maximum tumour size and number of tumours. The National Liver Offering Scheme ensures a complete de-linking between organ retrieval and allocation.7 Variant syndromes are allocated livers in proportion to the number on the waiting list.
Organ types
DCD grafts are usually whole livers but, if of sufficient quality, can be ‘split’ and transplanted into a child and adult. Partial grafts carry additional risks,8 so factors such as donor age, time on the intensive care unit and obesity will aid donor-team decision-making. All grafts risk transmission of malignancy and viruses so donor screening, transmission recognition and reporting facilitate accurate estimation of these risks.9
Liver transplantation surgery and the post-operative period
The recipient’s LT operation commences when the surgeon is assured of donor organ size, quality and anatomy. Hence, some recipients will experience a ‘false start’ if the organ quality is poor; however, if the organ is suitable, surgery will proceed (figure 2 outlines the order of surgery).
Figure 2.

Order of liver transplantation surgery. PSC, primary sclerosing cholangitis.
Figure 3 and online supplementary appendix 1 outline the post-LT complications. These can be broadly divided into immediate and early complications. Any major abdominal procedure carries a risk of bleeding and infection in the immediate post-operative period. The additional, more specific, surgical complications relate to the various vessel anastamoses (figure 2), including portal vein thrombosis, hepatic artery thrombosis and biliary leak or stricture. Live donor liver transplant (LDLT) and DCD allograft recipients are more prone to biliary and vascular complications. Hepatic artery stenosis and rare complications such as primary non-function may require re-graft,10 so all listed recipients are warned of this possibility. Conversely, portal vein thrombosis and biliary complications can usually be managed without the need for further surgery. These ‘immediate’ complications arise in the first few days and hence will all be managed in the liver transplant unit (LTU). Complications arising after the first week or so (see figure 3) include the ever-present risk of hepatic artery thrombosis, the emerging risk of organ rejection and diverse infections, including those related to graft transmission and immunosupression.
Figure 3.

Post-transplant complications. CMV, cytomegalovirus; EBV, Epstein-Barr virus.
flgastro-2019-101216supp001.pdf (53.1KB, pdf)
How should immunosuppression be managed in the clinic?
Most LT recipients require lifelong immunosuppression, although some develop ‘operational tolerance’ and can maintain graft health without immunosuppression.11 12 Maximum immunosuppression is required early post-transplant, when rejection risk is greatest. Frequently used agents are shown in online supplementary appendix 2. The most common regimens include13
flgastro-2019-101216supp002.pdf (51.7KB, pdf)
A calcineurin inhibitor (CNI) (usually tacrolimus) with or without corticosteroids.
A CNI with an antimetabolite (azathioprine or mycophenolate mofetil) with or without corticosteroids.
Mycophenolate and corticosteroids.
Immunosuppression is associated with significant side effects, which may be related to immunosuppression itself (such as increased risk of some cancers and infections) or drug-specific side effects (such as steroid-associated osteopenia or CNI-associated renal impairment) as in table 1. Golden rules for managing immunosuppression are outlined below, and the LTU’s pharmacist is an additional important resource.
Table 1.
Major side effects of commonly used immunosuppression
| Immunosuppressant | Side effects |
| Calcineurin inhibitors | Renal impairment Infections (viral, bacterial and fungal) increased risk Hyperuricaemia Gout Hypertension Hypercholesterolaemia Glucose intolerance Hypomagnesaemia Hyperkalaemia Headaches/migraines Insomnia Tremor Hirsuitism Gum hypertrophy |
| Mycophenolate | Diarrhoea Leucopenia Teratogenic (should be avoided by mother prior to and during pregnancy and male patients planning to father children. Men should use condoms during treatment and for at least 90 days after cessation of treatment. Female partners should also use a highly effective method of contraception for this duration.) Infections (viral, bacterial and fungal) |
| Corticosteroids | Sodium retention Fluid retention Potassium depletion Infections (viral, bacterial and fungal) Hypertension Carbohydrate intolerance and diabetes mellitus Cushingoid facies Growth retardation Menstrual irregularities Ophthalmological issues, for example, cataracts, glaucoma Osteoporosis and increased fracture risk, aseptic necrosis of femoral head Myopathy Muscle weakness Increased bruising Skin thinning/acne Altered mood Headaches Peptic ulceration Pancreatitis |
| mTORi | Infections (viral, bacterial and fungal) Thrombocytopenia and leucopenia Impaired wound healing Lymphocoele Rash Menstrual disorders Interstitial lung disease Hyperlipidaemia Proteinuria Possible increased risk of hepatic artery thrombosis Infections (viral, bacterial and fungal) Hepatotoxicity Bone marrow suppression |
mTORi, mTOR inhibitor.
Golden rules with immunosuppressants
Always use the same brand of CNI and do not interchange.
CNI and mTOR inhibitor (mTORi) doses should be informed by the use of therapeutic drug monitoring (TDM).
Target trough whole blood levels for the stable recipient are usually between 3 and 8 ng/L for tacrolimus and between 80 and 100 μg/L for cyclosporin.
For ‘trough’ CNI drug levels, ensure that the patient has not taken their drug on the morning of the blood test.
Always check any new prescriptions for potential drug–drug interactions.
The development of side effects does not necessarily equate with over-immunosuppression.
Immunosuppression regimens
Immunosuppression regimens vary considerably between units and individuals. The choice of immunosuppressive regimen is dependent on many factors, including
Time after transplant. Induction regimens (not included in these guidelines) use antilymphocytes agents and interleukin-2 receptor blockade: with increasing time after transplantation, the immunosuppressive burden can be reduced. Sirolimus (mTORi) is deferred for 3 months as it impairs wound healing and risks hepatic artery thrombosis.14
Indication for transplant. Many LTUs use long-term corticosteroids in autoimmune conditions,15 whereas high-dose steroids promote viral replication in active hepatitis C virus (HCV) infection.
Acute and/or chronic rejection episodes.
History or risk of cancer. mTORi may reduce the risk of some de novo cancers.
Complications of previous immunosuppression therapy.
Wish of recipient or partner to conceive and/or breast feed (mycophenolate and mTORi are teratogenic).
Renal impairment. For those with pre-transplant renal impairment, drug regimens with reduced CNI exposure may be appropriate.
Comorbid diseases. Diabetes mellitus or significant osteopenia is exacerbated by steroids. Azathioprine is frequently used in patients with inflammatory bowel diseaserequiring LT for primary sclerosing cholangitis (PSC).
There are few prospective, large-scale trials comparing different immunosuppressive regimens and these mostly focus on relatively short-term outcomes (<1 year), so the evidence base for immunosuppression is often based on retrospective analysis and clinical experience.
Pharmacokinetics and pharmacodynamics of immunosuppressants
TDM is used to adjust the dose of some drugs, especially CNI and mTORi. Usually, trough levels are used to direct therapy with higher target levels in the earlier post-operative period. TDM 2 hours after ingestion has been advocated for ciclosporin but is rarely used.16 TDM for mycophenolate has been advocated but is not used in routine practice.17
Drug metabolism is affected by many factors, including preparation and formulation, whether the medication is taken with food, co-morbid disease (including replicating HCV), intercurrent infections (especially diarrhoea or vomiting), change in liver function, use of other drugs (including herbal remedies) and genetic factors (such as CYP3A5 isoenzymes for CNI and thiopurine methyltransferase for azathioprine).
There are different preparations of the commonly prescribed agents available and different preparations with different pharmacodynamic profiles. For example, different preparations of tacrolimus are licensed for once daily or twice daily dosing and generic preparations that do not all have bioequivalence. Prolonged-release tacrolimus may be more cost-effective than two times per day release and may be associated with better outcomes.18 The MHRA has advised that the growing number of oral tacrolimus products available increases the potential for inadvertent switching between products, which has been associated with toxicity and graft rejection.19 Similar considerations apply to formulations of ciclosporin. Therefore, to ensure maintenance of therapeutic response when a patient is stabilised on a particular brand, oral tacrolimus products should be prescribed and dispensed by brand name only. If a prescriber considers that switching a patient to a different brand of oral tacrolimus would be of benefit, the change requires careful supervision and therapeutic monitoring by an appropriate specialist. There is some evidence that a significant variation in trough levels may be associated with a worse outcome.20 21 Similarly, mycophenolate sodium and mycophenolate mofetil are not interchangeable.
Adherence post LT
The rate of non-adherence to immunosuppression regimes approaches 40% in some studies22 (although non-adherence definitions are inconsistent across studies). Reasons for non-adherence vary between age groups and include side-effect profiles, perceived harm, changes to physical appearance and psychological distress. At all clinic visits, non-adherence should be considered and discussed with patients and their family, ideally by the specialist pharmacist.23
How should the patient be managed after LT?
Following discharge after LT, patients are reviewed weekly by their LTU. In many LTU’s, the surgical team supervises the first 3 months post surgery. Depending on the complexity of surgery, distance to travel and post-operative complications, patients can expect to be ‘weaned off’ their weekly transplant clinic visit as care is increasingly shared with their local hospital (see box 1).
Box 1. Management of post liver transplant (LT) patient in the clinic.
General
Careful drug history to ensure no new renal toxins have been started.
Adherence.
Careful blood pressure (BP) monitoring aiming for a systolic BP of <140 mm Hg and a diastolic BP of <85 mm Hg. Home monitoring may be necessary.
BMI monitoring, monitoring weight in non-obese and advice on weight reduction in obese patients.
Abnormal liver function tests (LFT)
Check medications, including herbal remedies.
Ultrasound liver for space-occupying lesion and biliary anastamotic stricture, and Doppler of hepatic artery and portal vein for patency.
Viral hepatitis screen to include hepatitis A, B, C and E; cytomegalovirus (CMV); and Epstein-Barr virus (EBV).
Consider liver biopsy (disease recurrence or rejection).
Renal dysfunction
Close monitoring is necessary.
Mycophenolate mofetil use enables CNI dose reduction.
Seek help from multidisciplines, especially diabetologists and nephrologists.
Seek help early as, once lost, renal function tends not to recover.
Cardiovascular disease
Statins are safe and appropriate.
Continue CNI but minimise use of statins with cyclosporin, and in patients on sirolimus, carefully monitor lipids.
Use of cardiovascular risk scores such as QRISK .
Post-transplant diabetes
Ensure close control with regular evaluation.
Effective management of glucose control.
No particular advantage of one antidiabetic drug over another.
Rapid minimisation of steroids if safe.
Hypertension
Careful choice of antihypertensive, always check drug–drug interactions.
First line: calcium channel blockers, such as amlodipine, reduce systemic vascular resistance and improve renal blood flow with minimal side effects and no interactions with CNI.
β-Blockers are safe and widely used.
Drugs that block the renin–angiotensin system, such as ACE inhibitors and angiotensin-receptor blockers, are best avoided in the early post-operative period when plasma renin activity is low and can exacerbate the hyperkalaemia seen with CNIs. The renin–angiotensin system does recover later in the post-transplant period, and then these drugs can be useful.
Diuretics can damage renal function and are best avoided.
Dyslipidaemia
Aggressive management is necessary.
Dietary interventions have little effect on dyslipidaemia.
Long-term corticosteroid use can also contribute to hyperlipidaemia, so attempting to minimise corticosteroid use long-term is appropriate.
Sirolimus is associated with high rates of dyslipidaemia.
Statins are usually safe, efficacious and well tolerated post-LT.
Pravastatin and atorvostatin appear effective, have little significant interactions with CNI and are well tolerated.
Hypertriglyceridemia with normal cholesterol levels is also common post-LT.
Obesity
Advice and education of patient and family on the waiting list prior to surgery.
Early resumption of advice and weight supervision post surgery.
Diet education is critical at the early stage, and exercise becomes possible once wounds have healed.
Minimise length of steroid use in obese recipients.
Place similar emphasis on dangers of weight gain as is placed on the other core issues (including rejection and infection) in the early post-transplant period.
All options, including surgical and medical solutions, are possible in the post-LT patient, as per standard protocols.
Smoking
All patients should be rigorously questioned over tobacco use.
Patients should be actively and repeatedly encouraged to stop smoking.
Use of nicotine patches safe pre-LT and post-LT.
Careful education of patients in how to identify early signs of head and neck cancer in this group.
Osteoporosis
All patients with chronic liver disease should have a bone densitometry scan, regardless of whether they are being assessed for transplantation.
Minimise corticosteroid and heparin use and avoid loop diuretics as these drugs promote osteoporosis.
Optimise calcium and vitamin D intake.
Maintain weight-bearing exercise.
Consider rrepeat bone densitometry scan at 12 months post-transplant.
Prevention and treatment should be consistent with national guidance.
Note that bisphosphonates are both safe and effective post-transplant.
Alcohol
Check for alcohol use post-LT.
Ensure addiction services are being used, where appropriate.
Facilitate honest and open discussions with patient and family over alcohol, drug and tobacco use.
Cancer
Transplant recipients should avoid sun exposure, wear a hat and use factor 50 sunscreen.
Patients should participate in national screening programmes (cervical, breast and bowel).
Patients must be told to seek urgent dermatological opinion if skin changes are noticed, and every recipient should have a total skin review (head to toe) annually, to look for moles, basal cell carcinoma and other skin tumours (annual ‘MOT’).
Specific questions on smoking should be asked at every clinic review and appropriate advice provided.
Post-LT survival has been steadily rising for the last 20 years.24 Improved surgical expertise, better patient selection and better immunosuppression have contributed, such that non-liver causes such as malignancy (22%), cardiovascular disease (11%), infection (9%) and renal failure (6%) are the leading causes of mortality 1 year post surgery.25 Beyond 12 months, the metabolic syndrome emerges as being of increasing relevance to recipients.
Graft dysfunction
Most LT recipients return to their referrers outpatients with normal or stable LFTs. Any variance should be investigated thoroughly (table 2) to include a check of adherence, any new medication and an ultrasound scan (with Doppler). Further investigation of graft dysfunction for infection, rejection and disease recurrence will likely take place at the LTU and are outlined further:
Table 2.
Cause of graft dysfunction following liver transplantation
| Causes of abnormal liver function tests (LFT) post-transplant | |
| Parenchymal | Rejection, infection or disease recurrence |
| Drugs | Antibiotics or immunosuppression |
| Biliary | Stricture, leak or stones |
| Malignancy | Primary or secondary |
LFT, Liver Function Test.
Rejection
Rejection should be considered if liver biochemistry deteriorates post-LT. The classification of liver allograft rejection has recently been revised by the Banff Working Group26 (see online supplementary appendix 3). The most common form is T cell-mediated rejection where symptoms include fever, fatigue, jaundice and liver tenderness, which may occur with a rising transaminase and, possibly, leucocytosis. A biopsy is usually mandatory (see online supplementary appendix 3 for interpretation and management) and should be forwarded to the LTU as accurate interpretation is critical. Antibody-mediated rejection is rare and a detailed discussion is beyond the scope of this review. Chronic rejection (also termed ‘ductopenic’ rejection) typically occurs several months or more post-LT and is potentially reversible, so a liver biopsy with expert interpretation is mandatory.
flgastro-2019-101216supp003.pdf (52.6KB, pdf)
Infection
CMV infection usually occurs in a virus-naïve recipient receiving an organ from a previously infected donor. In such instances, the recipient will receive 6 months of oral valgancyclovir as prophylaxis. CMV infection causes fever, fatigue and gastrointestinal symptoms with neutropenia and positive CMV PCR.
During the first 6 months post-LT, opportunistic infections such as those caused by Aspergillus can appear, and latent infections such as those caused by Mycobacterium tuberculosis may be reactivated.
Beyond 6 months, immunosuppression is frequently reduced, so infections then align with those seen in the non-immunosuppressed population. In addition, post-LT prophylactic agents such as co-trimoxazole, valganciclovir and isoniazid usually stop between 3 and 6 months post-LT and should be considered if new infections appear.
Chronic hepatitis E is under-recognised and should be considered in any LT recipient developing graft dysfunction. A positive hepatitis E PCR may require ribavirin treatment.27
Disease recurrence
Following LT, disease recurrence frequently occurs:
Hepatitis B requires ongoing viral suppression.
Untreated hepatitis C requires clearance post LT.
Non alcoholic steatohepatitis (NASH) can return, especially if obesity, hypertension, hypercholesterolaemia and diabetes control worsen post-LT.
Alcohol-related liver disease—addiction services and open discussion with patient.
PBC recurrence is found in up to 50% at 5 years. Ursodeoxycholic acid (URSO) is often used, but there is limited experience with obeticholic acid.
PSC recurs in up to 70% at 5 years; there is no effective treatment, although ursodeoxycholic acid (UDCA) is sometimes used.
Renal dysfunction
The cumulative incidence of end-stage renal failure (ESRF) post-LT was 4% in Fisher’s series at 10 years,28 while the frequency of chronic kidney disease at this time, approaches 25%.29 The longer the follow-up, the more renal dysfunction occurs, and this is associated with substantial cardiovascular mortality and morbidity. Poor pre-operation renal function, along with type 2 diabetes, hypertension and CNIs, are the major determinants of declining post-transplant renal function.29
Cardiovascular disease
Despite careful evaluation pre-surgery, cardiovascular risk increases post-LT. The proportion of transplant recipients with pre-existing metabolic syndrome is increasing as the population’s median BMI rises.30 A recent retrospective study from the USA identified a new cardiovascular disease within 8 years of surgery in almost a third of all LT recipients.31 Significant risk factors included age, diabetes, smoking, hypertension, estimated glomerular filtration rate (eGFR) of <60 mL/min/1.73 m2 and prior cardiovascular disease. Careful attention to risk factors and lifestyle is important in all recipients.
Post-transplant development of diabetes mellitus
Post-transplant diabetes mellitus (PTDM) increases the risk of infection and cardiovascular events, and decreases graft and recipient survival as well as quality of life (QOL).32 Risk factors for development of PTDM include HCV infection, male gender, corticosteroid use, pre-LT diabetes and CNI (tacrolimus>ciclosporin).
Post-transplant systemic hypertension
Pre-LT, arterial hypertension is rare, but most recipients develop hypertension following LT.33 Corticosteroids and CNIs are largely responsible.34
Post-transplant development of dyslipidaemia
Patients requiring lipid-lowering agents pre-LT should continue after surgery. Advanced liver disease lowers cholesterol levels because of impaired hepatic synthesis and esterification; however, patients with cholestatic liver disease may have high serum cholesterol levels if the liver synthetic function is preserved.35 Hyperlipidaemia is more frequent with ciclosporin than tacrolimus.36
Obesity
Obesity occurs in almost half of LT recipients in some series.37 Virtually all of those obese pretransplant remain so, and in those who were normal weight pre-LT, a third will become obese. Important factors include improved appetite and corticosteroid use, coupled with the reversal of cirrhosis, effectively removing the associated catabolic state. The cardiovascular mortality and morbidity rise, along with renal disease and non alcoholic fatty liver disease (NAFLD), in the recipient’s graft.38
Post-transplant smoking
Up to a quarter of patients in centres around the world will be regularly smoking tobacco at the time of their LT.39 While the European Association for the Study of the Liver (EASL) recommends abstinence before listing, UK transplant centres do not take an ‘absolutist’ view.40 Cigarette smoking promotes fibrosis in hepatitis C, PBC and alcohol-related liver disease (ArLD) and probably increases the likelihood of hepatoma developing . The data on graft and recipient survival are conflicting with respect to tobacco smoking, but cardiovascular disease is certainly more prevalent.41
Osteoporosis
Inadequate bone density is very common in the end-stage liver disease population.42 More advanced chronic liver disease and cholestatic liver diseases are associated with more advanced bone loss. Within the first 12 months after LT, bone density rapidly deteriorates, predisposing to fractures.43
Post-transplant alcohol use and misuse
All LT candidates are questioned over alcohol use, regardless of indication. Depending on definitions used, up to a quarter of patients transplanted for ArLD return to potential harmful consumption levels, and twice that many will return to some sort of alcohol use.44 45 When significant relapse occurs after LT, the rate of graft damage rises, as does mortality.
For patients transplanted for non-ArLD indications, standard advice to maintain alcohol intake below 14 units/week is appropriate.
Cancer
The risk of malignancy, particularly skin cancers and lymphoma, rises in LT recipients.46 Cancer of the lung, head, neck and colon are more common, whereas prostate and breast cancers have a similar prevalence to age-matched and sex-matched controls.
Post-transplant lymphoproliferative disorder is usually EBV driven and usually occurs in the first 12 months post-LT. While classical symptoms of fever, night sweats and weight loss are seen, they can sometimes be more subtle. Therapy is initiated by reducing immunosuppression combined with standard chemotherapy techniques.
Online supplementary appendix 4 displays a specimen outpatient proforma.
flgastro-2019-101216supp004.pdf (70.2KB, pdf)
Outcomes of LT
This section examines patient (table 3) and organ (table 4) survival, as well as other outcome parameters, such as QOL, return to employment and psychosexual outcomes.
Table 3.
Patient survival times post liver transplant, depending on age of recipient (source eltr.org24)
| Age of recipient (years) | 1-year survival (%) | 5-year survival (%) | 10-year survival (%) | 20-year survival (%) |
| 18–45 | 84 | 75 | 66 | 50 |
| 46–60 | 83 | 70 | 59 | 36 |
| 60–70 | 80 | 65 | 49 | 21 |
Table 4.
Graft survival over time for first transplant, second transplant and third transplant (source eltr.org24)
| Graft number | 1-year survival (%) | 5-year survival (%) | 10-year survival (%) | 20-year survival (%) |
| First | 79 | 66 | 55 | 36 |
| Second | 58 | 46 | 36 | 22 |
| Third | 53 | 42 | 33 | 27 |
Patient outcomes
Patient survival times (table 3) reported in the European Liver Transplant Registry (ELTR) show that survival depends on the indication and the age of the recipient. However, there is a cohort effect, and long-term patient and graft survival has been steadily improving over the last 20 years.
Graft outcomes
Graft survival times (table 4) reported in the ELTR demonstrate that re-grafts do not last as long as the first organ transplanted.
Psychosocial outcomes following LT
Quality of life
Assessing successful outcomes following LT has historically focused on survival rates for both the patient and graft. More recently, with ever improving ‘hard’ outcomes, it is becoming recognised that measures of a successful LT should include aspects of Quality of Life (QOL).47 48 Evaluation of outcomes according to QOL following LT are limited due to the lack of a standardised framework for evaluation and data collection; the generic health assessment questionnaires are the most widely published (Short Form 36 and the Hospital Anxiety and Depression Score) but are limited by their lack of disease-specific elements.49
Generic heath-related quality of life (HR-QOL) improves following LT, and improvements are similar to outcomes in kidney, heart and lung transplant recipients; however, HR-QOL scores fail to return to that of sex-matched and age-matched healthy individuals.50 Improvements are most marked in the first 2 years following LT, with positive changes in psychological, physical, social, personal and overall health perceptions.51 Assessment of anxiety and depression, specifically, shows a decline in the longer term, reported for 2 years after LT, secondary to concerns regarding disease recurrence and accruement of comorbidities accentuated by immunosuppression use. Conversely, improvements in physical functioning and overall life satisfaction scores appear more sustained over time.51
Employment
LT recipients who return to work have a significantly better QOL compared with those who are unemployed. The percentage of recipients who return to work varies from 26% to 57% and is dependent on time from LT and disease aetiology.52 53
Sexual function and pregnancy
Sexual function and fertility improves following LT but does not reach that of healthy age-matched and sex-matched individuals with reports of decreased libido, difficulty in reaching orgasm, erectile dysfunction and reduced satisfaction.54–56 For men, erectile dysfunction usually improves post-LT but remains in some due to a combination of medication, comorbidities and depression.56 57 Sexual health in women has been less well studied; however, dysfunction following LT correlates with a reduction in QOL.56 Fertility can return as early as 1 month post-LT. Fertility should be discussed with all women of childbearing age following transplantation; pre-conception counselling and multidisciplinary management of the pregnancy will result in the best possible outcome. Pregnancy should be avoided for the first post-LT year due to its association with acute cellular rejection.58 59 Pregnancy following LT is associated with a live birth rate of 70% but with an increased risk of foetal loss, prematurityand low birth weight whilst the mother is more likely to develop hypertension, pre-eclampsia, gestational diabetes and graft dysfunction.58 59 Immunosupression should be continued throughout pregnancy with the exception of mycophenolate or sirolimus/everolimus, which are teratogenic.
Physical activity and diet post-LT
After LT, functional capacity improves, although exercise capacity remains lower than that of age-matched controls.60 Only 25% of recipients are physically active after LT, and more than two-thirds consume more than the recommended calorie intake.61 Data to support benefit in targeted exercise/nutritional programmes post-LT are emerging, although these have yet to demonstrate an impact on metabolic syndrome and cardiovascular morbidity and mortality.62 Obesity is a growing problem, with >30% being obese at 3 years, with older age at transplant and transplant for chronic as opposed to acute liver failure being risk factors.
Conclusions
Liver transplantation improves the quantity and quality of life of patients with advanced liver disease.
The number of organs available for liver transplantation has steadily increased over recent years and is associated with increasing numbers of long-term survivors.
After the first year, most patients will be cared for primarily by their local gastroenterologist/hepatologist.
Immunosuppression requires careful management to maximise protection from the immune system while minimising harm to other organs.
Early post-transplant complications include technical, infection and immunological issues.
With time, complications related to the metabolic syndrome and associated cardiovascular risks become increasingly prevalent.
Acknowledgments
Ms Lorna Tong and Mrs Elizabeth Crawshaw, expert patients, kindly read through the document and offered helpful criticism.
Footnotes
Contributors: There were 20 authors involved in the production of these two articles concerning liver transplantation. The original project was divided into an Introduction, nine sections and a Conclusion. From that original outline, the sections were written by writing groups and then collated. The nine sections were then divided into two halves for the purposes of publication, after discussion with the editor of Frontline Gastroenterology. Each contributor provided editing input to the project, as the manuscript went through its many iterations. The specific contribution/participation of each contributor are as follows: CM (consultant hepatologist in a DGH): senior author; initiated section divisions, collected manuscripts; contributed to writing by adding DGH aspects to all part 1 and management of the post-transplant patient section; edited all tables and oversaw the process; responsible for the overall content as guarantor. AC: consultant pharmacist; cowrote the section on immunosuppression agents in part 2 with JN and gave input to part 1, particularly with the ‘disease-specific considerations’ and where medication interactions can occur. MEC: consultant transplant hepatologist; coauthored the section on 'management of the patient on the waiting list' and then read both parts 1 and 2 of the final submission as an additional critique for all sections; critical role in the planning and acquisition of data for inclusion into the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. AH: consultant transplant hepatologist; coauthored the section on 'how to refer' and then drew up the tables and added valuable additional input, as well as rewrote participation for the sections when the original submission was too lengthy; critical role in planning, final manuscript editing and approval. SH: consultant histopathologist; wrote the section on cellular rejection in part 2; added valuable oversight in part 1, particularly as both parts were too lengthy and required significant reduction in word count. JH: consultant hepatologist in a DGH; wrote the section on transplant assessment and with KJ refined this section to focus on the DGH referrer, and also read both completed parts to provide the DGH perspective on these elements of liver transplantation and ensure focus was correct for that audience; critical role in planning and acquisition of data for inclusion into part 1 of the guideline, along with an evaluation of relevance to the project; editing and approval of parts 1 and 2 of the final manuscript. KJ: transplant coordinator; provided the section on the transplant coordinator and then gave critical input for aspects on process of organ selection, along with RP; critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. JL: consultant transplant hepatologist; coauthored the section on 'how to refer' and provided editorial input for part 2; critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. SM: consultant transplant hepatologist; coauthored the section on 'how to manage the patient on the waiting list'; brought together the coordinators' input with the transplant centre and the interaction with secondary care referring centre; provided insights from both sides of the secondary/tertiary care interaction and then edited the initial contribution of the section to a more manageable section; ensured relevance of the data collected for the project along with final manuscript editing and approval. KM: consultant transplant surgeon; contributed to the section in part 2 on transplant surgery and outcomes; also provided input in part 1 in the section on transplant assessment and previous surgery; critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. DM: consultant transplant surgeon; co-authored the section on transplant surgery with KM and post-transplant surgical complications; also provided input in part 1 in the section on transplant assessment and previous surgery; critical role in the planning and acquisition of data for inclusion in guideline, along with evaluation of relevance to the project; final manuscript editing and approval. JN: consultant transplant hepatologist; wrote the section on post-transplant Immunosuppression with the aid of AC; also contributed to part 1 in an editorial role, when he helped with the original concept; provided a critical role following the original guideline production and prior to its splitting into two halves (parts 1 and 2) and ensuring correct focus was maintained when the manuscript was reduced in size. RP: consultant transplant surgeon; wrote the section on organ allocation and donation; also made a significant contribution to the postoperative care and complications sections and the preop evaluation (part 1); critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. AP: liver pharmacist; contributed to part 2, immunosupression section, but also gave useful input into parts 1 and 2 from the point of view of medication and drug interactions, particularly with viral hepatitis treatment; critical role in evaluating data for inclusion in the guideline, along with maintaining relevance to the project; final manuscript editing and approval. WP: consultant in palliative care; authored the section on palliative care and transplantation in part 1; contributed in part 2 via proofreading and providing critical input; critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. LS: transplant coordinator; contributed to the section on how to refer a patient for liver transplant (part 1) and gave input into the section on organ allocation (part 2); critical role in the planning and acquisition of data for inclusion in the guideline, along with evaluation of relevance to the project; final manuscript editing and approval. KS: consultant transplant hepatologist; wrote the section on 'when to refer' in part 1, but also gave significant editorial input to the entire project, at the time of the section merge and subsequent division into two halves; critical role in planning and acquisition of data for inclusion into guideline, along with evaluation of relevance to project; final manuscript editing and approval. DTh and RW: consultant transplant hepatologists; coauthored the section on transplant outcomes; provided critical input into part 1 as well, with respect to the referral process; critical role in the planning and acquisition of data for inclusion in guideline, along with evaluation of relevance to the project; final manuscript editing and approval. DTr: consultant transplant hepatologist; coauthored the section on postoperative care and complications (non-surgical); also supported the entire process by helping the lead author with editing sections and discussion of tables and pictures and deciding on section inclusion, data relevance and final manuscript editing and approval.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Annual Report on Liver Transplantation 2015/2016 NHS Blood & Transplant. Available: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/5007/annual_liver_transplantation_report_2017.pdf
- 2. Neuberger J. Liver transplantation in the United Kingdom. Liver Transpl 2016;22:1129–35. 10.1002/lt.24462 [DOI] [PubMed] [Google Scholar]
- 3. Adult kidney transplant Service-NHS England. Available: https://www.england.nhs.uk/wp./service-spec-adult-kidney-transplant- service.pdf
- 4. A code of practice for the diagnosis and confirmation of death. Available: www.aomrc.org.uk/reports-guidance/./code-practice-diagnosis- confirmation-death/
- 5. Donation after circulatory death. Available: https://www.odt.nhs.uk/deceased-donation/best-practice-guidance/donation-after-circulatory-death/
- 6. Callaghan CJ, Charman SC, van der Muerlen JHP, et al. Outcomes of transplantation of livers from donation after circulatory death donors in the UK: a cohort study. Available: http://bmjopen.bmj.com/ content/3/9/e003287 [DOI] [PMC free article] [PubMed]
- 7. The new National Liver Offering Scheme What’s changing and how it will affect you. Available: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/7892/national-liver-offering-roadshow-presentation.pdf
- 8. Collett D, Friend PJ, Watson CJE. Factors associated with short- and long-term liver graft survival in the United Kingdom: development of a UK donor liver index. Transplantation 2017;101:786–92. 10.1097/TP.0000000000001576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Len O, Garzoni C, Lumbreras C, et al. Recommendations for screening of donor and recipient prior to solid organ transplantation and to minimize transmission of donor-derived infections. Clin Microbiol Infect 2014;20:10–18. 10.1111/1469-0691.12557 [DOI] [PubMed] [Google Scholar]
- 10. Marudanayagam R, Shanmugam V, Sandhu B, et al. Liver retransplantation in adults: a single-centre, 25-year experience. HPB 2010;12:217–24. 10.1111/j.1477-2574.2010.00162.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Fine RN. Tolerance in solid-organ transplant. Exp Clin Transplant 2016;14:1–5. [PubMed] [Google Scholar]
- 12. Clavien P-A, Muller X, de Oliveira ML, et al. Can immunosuppression be stopped after liver transplantation? Lancet Gastroenterol Hepatol 2017;2:531–7. 10.1016/S2468-1253(16)30208-4 [DOI] [PubMed] [Google Scholar]
- 13. Neuberger J. An update on liver transplantation: a critical review. J Autoimmun 2016;66:51–9. 10.1016/j.jaut.2015.08.021 [DOI] [PubMed] [Google Scholar]
- 14. Ventura-Aguiar P, Campistol JM, Diekmann F. Safety of mTOR inhibitors in adult solid organ transplantation. Expert Opin Drug Saf 2016;15:303–19. 10.1517/14740338.2016.1132698 [DOI] [PubMed] [Google Scholar]
- 15. Montano-Loza AJ, Bhanji RA, Wasilenko S, et al. Systematic review: recurrent autoimmune liver diseases after liver transplantation. Aliment Pharmacol Ther 2017;45:485–500. 10.1111/apt.13894 [DOI] [PubMed] [Google Scholar]
- 16. Kim KH, Lee SG, Lee YJ, et al. Suitable whole blood levels 2 hours after neoral in liver transplant patients: experiences at a single center. Transplant Proc 2006;38:2971–3. 10.1016/j.transproceed.2006.08.148 [DOI] [PubMed] [Google Scholar]
- 17. Kaltenborn A, Schrem H. Mycophenolate mofetil in liver transplantation: a review. Ann Transplant 2013;18:685–96. 10.12659/AOT.889299 [DOI] [PubMed] [Google Scholar]
- 18. Muduma G, Odeyemi I, Pollock RF. A cost-utility analysis of prolonged-release tacrolimus relative to immediate-release tacrolimus and ciclosporin in liver transplant recipients in the UK. J Med Econ 2016;19:995–1002. 10.1080/13696998.2016.1189921 [DOI] [PubMed] [Google Scholar]
- 19.https://www.gov.uk/drug-safety-update/oral-tacrolimus-products-prescribe-and-dispense-by-brand-name-only-to-minimise-the-risk-of-inadvertent-switching-between-products-which-has-been-associated-with-reports-of-toxicity-and-graft-rejection
- 20. Shemesh E, Bucuvalas JC, Anand R, et al. The medication level variability index (MLVI) predicts poor liver transplant outcomes: a prospective multi-site study. Am J Transplant 2017;17:2668–78. 10.1111/ajt.14276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Neuberger JM, Bechstein WO, Kuypers DRJ, et al. Practical recommendations for long-term management of modifiable risks in kidney and liver transplant recipients: a guidance report and clinical checklist by the consensus on managing modifiable risk in transplantation (commit) group. Transplantation 2017;101:S1–56. 10.1097/TP.0000000000001651 [DOI] [PubMed] [Google Scholar]
- 22. Morrissey PE, Flynn ML, Lin S. Medication noncompliance and its implications in transplant recipients. Drugs 2007;67:1463–81. 10.2165/00003495-200767100-00007 [DOI] [PubMed] [Google Scholar]
- 23. Rebafka A. Medication adherence after renal Transplantation-a review of the literature. J Ren Care 2016;42:239–56. 10.1111/jorc.12181 [DOI] [PubMed] [Google Scholar]
- 24. European liver transplant registry. Available: http://www.eltr.org
- 25. Watt KDS, Pedersen RA, Kremers WK, et al. Evolution of causes and risk factors for mortality post-liver transplant: results of the NIDDK long-term follow-up study. Am J Transplant 2010;10:1420–7. 10.1111/j.1600-6143.2010.03126.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Demetris AJ, Bellamy C, Hübscher SG, et al. 2016 comprehensive update of the Banff Working group on liver allograft pathology: introduction of antibody-mediated rejection. Am J Transplant 2016;16:2816–35. 10.1111/ajt.13909 [DOI] [PubMed] [Google Scholar]
- 27. Aggarwal A, Perumpail RB, Tummala S, et al. Hepatitis E virus infection in the liver transplant recipients: clinical presentation and management. World J Hepatol 2016;8:117–22. 10.4254/wjh.v8.i2.117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Fisher NC, Nightingale PG, Gunson BK, et al. Chronic renal failure following liver transplantation. Transplantation 1998;66:59–66. 10.1097/00007890-199807150-00010 [DOI] [PubMed] [Google Scholar]
- 29. Solà E, Ginès P. Chronic kidney disease: a major concern in liver transplantation in the XXI century. J Hepatol 2014;61:196–7. 10.1016/j.jhep.2014.05.011 [DOI] [PubMed] [Google Scholar]
- 30. Laish I, Braun M, Mor E, et al. Metabolic syndrome in liver transplant recipients: prevalence, risk factors, and association with cardiovascular events. Liver Transpl 2011;17:15–22. 10.1002/lt.22198 [DOI] [PubMed] [Google Scholar]
- 31. Fussner LA, Heimbach JK, Fan C, et al. Cardiovascular disease after liver transplantation: when, what, and who is at risk. Liver Transpl 2015;21:889–96. 10.1002/lt.24137 [DOI] [PubMed] [Google Scholar]
- 32. Baid S, Cosimi AB, Farrell ML, et al. Posttransplant diabetes mellitus in liver transplant recipients: risk factors, temporal relationship with hepatitis C virus allograft hepatitis, and impact on mortality. Transplantation 2001;72:1066–72. 10.1097/00007890-200109270-00015 [DOI] [PubMed] [Google Scholar]
- 33. Canzanello VJ, Textor SC, Taler SJ, et al. Late hypertension after liver transplantation: a comparison of cyclosporine and tacrolimus (FK 506). Liver Transpl Surg 1998;4:328–34. 10.1002/lt.500040404 [DOI] [PubMed] [Google Scholar]
- 34. Luca LD, Westbrook R, Tsochatzis EA. Metabolic and cardiovascular complications in the liver transplant recipient. Ann Gastroenterol 2015;28:183–92. [PMC free article] [PubMed] [Google Scholar]
- 35. Kobashigawa JA, Kasiske BL. Hyperlipidemia in solid organ transplantation. Transplantation 1997;63:331–8. 10.1097/00007890-199702150-00001 [DOI] [PubMed] [Google Scholar]
- 36. Charco R, Cantarell C, Vargas V, et al. Serum cholesterol changes in long-term survivors of liver transplantation: a comparison between cyclosporine and tacrolimus therapy. Liver Transpl Surg 1999;5:204–8. 10.1002/lt.500050303 [DOI] [PubMed] [Google Scholar]
- 37. Perito ER, Glidden D, Roberts JP, et al. Overweight and obesity in pediatric liver transplant recipients: prevalence and predictors before and after transplant, United network for organ sharing data, 1987-2010. Pediatr Transplant 2012;16:41–9. 10.1111/j.1399-3046.2011.01598.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Dare AJ, Plank LD, Phillips ARJ, et al. Additive effect of pretransplant obesity, diabetes, and cardiovascular risk factors on outcomes after liver transplantation. Liver Transpl 2014;20:281–90. 10.1002/lt.23818 [DOI] [PubMed] [Google Scholar]
- 39. Ehlers SL, Rodrigue JR, Widows MR, et al. Tobacco use before and after liver transplantation: a single center survey and implications for clinical practice and research. Liver Transpl 2004;10:412–7. 10.1002/lt.20087 [DOI] [PubMed] [Google Scholar]
- 40. European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu EASL clinical practice guidelines: liver transplantation. J Hepatol 2016;64:433–85. 10.1016/j.jhep.2015.10.006 [DOI] [PubMed] [Google Scholar]
- 41. Ursic-Bedoya J, Donnadieu-Rigole H, Faure S, et al. Alcohol use and smoking after liver transplantation; complications and prevention. Best Pract Res Clin Gastroenterol 2017;31:181–5. 10.1016/j.bpg.2017.03.005 [DOI] [PubMed] [Google Scholar]
- 42. Ninkovic M, Love SA, Tom B, et al. High prevalence of osteoporosis in patients with chronic liver disease prior to liver transplantation. Calcif Tissue Int 2001;69:321–6. 10.1007/s00223-001-2028-4 [DOI] [PubMed] [Google Scholar]
- 43. Monegal A, Navasa M, Guañabens N, et al. Bone disease after liver transplantation: a long-term prospective study of bone mass changes, hormonal status and histomorphometric characteristics. Osteoporos Int 2001;12:484–92. 10.1007/s001980170094 [DOI] [PubMed] [Google Scholar]
- 44. DiMartini A, Dew MA, Day N, et al. Trajectories of alcohol consumption following liver transplantation. Am J Transplant 2010;10:2305–12. 10.1111/j.1600-6143.2010.03232.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Dew MA, DiMartini AF, Steel J, et al. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transpl 2008;14:159–72. 10.1002/lt.21278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Schrem H, Kurok M, Kaltenborn A, et al. Incidence and long-term risk of de novo malignancies after liver transplantation with implications for prevention and detection. Liver Transpl 2013;19:1252–61. 10.1002/lt.23722 [DOI] [PubMed] [Google Scholar]
- 47. Parmar A, Vandriel SM, Ng VL. Health-Related quality of life after pediatric liver transplantation: a systematic review. Liver Transpl 2017;23:361–74. 10.1002/lt.24696 [DOI] [PubMed] [Google Scholar]
- 48. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995;273:59–65. [PubMed] [Google Scholar]
- 49. Jay CL, Butt Z, Ladner DP, et al. A review of quality of life instruments used in liver transplantation. J Hepatol 2009;51:949–59. 10.1016/j.jhep.2009.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. De Bona M, Ponton P, Ermani M, et al. The impact of liver disease and medical complications on quality of life and psychological distress before and after liver transplantation. J Hepatol 2000;33:609–15. 10.1034/j.1600-0641.2000.033004609.x [DOI] [PubMed] [Google Scholar]
- 51. Ruppert K, Kuo S, DiMartini A, et al. In a 12-year study, sustainability of quality of life benefits after liver transplantation varies with pretransplantation diagnosis. Gastroenterology 2010;139:1619–29. 10.1053/j.gastro.2010.06.043 [DOI] [PubMed] [Google Scholar]
- 52. Aberg F, Höckerstedt K, Roine RP, et al. Influence of liver-disease etiology on long-term quality of life and employment after liver transplantation. Clin Transplant 2012;26:729–35. 10.1111/j.1399-0012.2012.01597.x [DOI] [PubMed] [Google Scholar]
- 53. Huda A, Newcomer R, Harrington C, et al. High rate of unemployment after liver transplantation: analysis of the United network for organ sharing database. Liver Transpl 2012;18:89–99. 10.1002/lt.22408 [DOI] [PubMed] [Google Scholar]
- 54. Ho JK, Ko HH, Schaeffer DF, et al. Sexual health after orthotopic liver transplantation. Liver Transpl 2006;12:1478–84. 10.1002/lt.20831 [DOI] [PubMed] [Google Scholar]
- 55. Heneghan MA, Selzner M, Yoshida EM, et al. Pregnancy and sexual function in liver transplantation. J Hepatol 2008;49:507–19. 10.1016/j.jhep.2008.07.011 [DOI] [PubMed] [Google Scholar]
- 56. Sorrell JH, Brown JR. Sexual functioning in patients with end-stage liver disease before and after transplantation. Liver Transpl 2006;12:1473–7. 10.1002/lt.20812 [DOI] [PubMed] [Google Scholar]
- 57. Madersbacher S, Ludvik G, Stulnig T, et al. The impact of liver transplantation on endocrine status in men. Clin Endocrinol 1996;44:461–6. 10.1046/j.1365-2265.1996.698519.x [DOI] [PubMed] [Google Scholar]
- 58. Armenti VT. Pregnancy after liver transplantation. Liver Transpl 2012;18:619–20. 10.1002/lt.23446 [DOI] [PubMed] [Google Scholar]
- 59. Westbrook RH, Yeoman AD, Agarwal K, et al. Outcomes of pregnancy following liver transplantation: the King's College Hospital experience. Liver Transpl 2015;21:1153–9. 10.1002/lt.24182 [DOI] [PubMed] [Google Scholar]
- 60. Beyer N, Aadahl M, Strange B, et al. Improved physical performance after orthotopic liver transplantation. Liver Transpl Surg 1999;5:301–9. 10.1002/lt.500050406 [DOI] [PubMed] [Google Scholar]
- 61. Painter P, Krasnoff J, Paul SM, et al. Physical activity and health-related quality of life in liver transplant recipients. Liver Transpl 2001;7:213–9. 10.1053/jlts.2001.22184 [DOI] [PubMed] [Google Scholar]
- 62. Krasnoff JB, Vintro AQ, Ascher NL, et al. A randomized trial of exercise and dietary counseling after liver transplantation. Am J Transplant 2006;6:1896–905. 10.1111/j.1600-6143.2006.01391.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
flgastro-2019-101216supp001.pdf (53.1KB, pdf)
flgastro-2019-101216supp002.pdf (51.7KB, pdf)
flgastro-2019-101216supp003.pdf (52.6KB, pdf)
flgastro-2019-101216supp004.pdf (70.2KB, pdf)