

ABSTRACT
Objective:
To investigate parameters of lung function and respiratory muscle strength in different stages of Parkinson’s disease (PD), as well as to determine their correlation with motor function and quality of life.
Methods:
This was a cross-sectional study conducted at a referral center for PD in the city of Recife, Brazil. Respiratory muscle strength and lung function, as well as their relationship with motor function and quality of life, were evaluated in patients with PD, stratified by the level of severity, and were compared with the data obtained for a control group. After confirming the normality of data distribution, we performed one-way ANOVA with a post hoc t-test.
Results:
The sample comprised 66 individuals, in two groups: PD (n = 49) and control (n = 17). All of the parameters investigated showed inverse correlations with PD severity, and there were significant differences among the levels of severity, as well as between the PD and control groups, in terms of the MIP, MEP, FVC, FEV1, and FEF25-75%. The lung function parameters also showed moderate to weak inverse correlations with bradykinesia and rigidity. On a quality of life questionnaire, the total score and mobility domain score both presented a moderate inverse correlation with FVC, FEV1, PEF, and MEP.
Conclusions:
Respiratory muscle strength and some lung function parameters are impaired from the early stages of PD onward, bradykinesia and rigidity being the cardinal signs that correlate most strongly with impairment of those parameters. Such alterations negatively affect the quality of life of patients with PD.
Keywords: Parkinson disease, Respiratory mechanics, Maximum respiratory pressures, Quality of life
RESUMO
Objetivo:
Investigar a repercussão de parâmetros de função pulmonar e de força muscular respiratória nos diversos estágios da doença de Parkinson (DP) e suas correlações com a funcionalidade e a qualidade de vida desses pacientes.
Métodos:
Estudo de corte transversal realizado em um serviço de referência para DP em Recife (PE). Foram avaliadas a força muscular respiratória e a função pulmonar, assim como suas relações com a funcionalidade e a qualidade de vida, em pacientes com DP estratificados por gravidade da DP e comparados a um grupo controle. Após a verificação da normalidade da amostra, foi realizada one-way ANOVA e teste t post hoc.
Resultados:
A amostra foi composta por 66 indivíduos, sendo 49 no grupo DP e 17 no grupo controle. Houve reduções nos parâmetros investigados com a progressão da doença, em comparação com o grupo controle, sendo encontradas diferenças significativas em PImáx, PEmáx, CVF, VEF1 e FEF25-75% em todos os estágios da DP. Houve correlações inversas (de fraca a moderada) de alguns parâmetros estudados com bradicinesia e rigidez. Os escores totais do questionário de qualidade de vida e de seu domínio mobilidade apresentaram moderada correlação inversa com CVF, VEF1, PFE e PEmáx.
Conclusões:
A força muscular respiratória e alguns parâmetros de função pulmonar encontram-se reduzidos desde os estágios iniciais da DP, sendo a bradicinesia e a rigidez os sinais cardinais mais correlacionados ao prejuízo desses parâmetros. Essas alterações repercutem negativamente na qualidade de vida desses pacientes.
Descritores: Doença de Parkinson, Mecânica respiratória, Pressões respiratórias máximas, Qualidade de vida
INTRODUCTION
Respiratory dysfunction is the leading cause of death among individuals with Parkinson’s disease (PD) and can be caused by respiratory muscle stiffness and postural dysfunction, as well as changes in upper airway muscle activation and coordination. 1
As the disease progresses, lung function decreases in most patients, thus increasing the severity of PD. 2 , 3 Reduced lung function has been attributed to muscle stiffness and postural changes (including hyperkyphosis), which limit chest expansion and result in reduced lung volumes and restrictive lung disease. 4
Although pulmonary dysfunction is a common and potentially serious complication in PD patients, respiratory symptoms are rare. This might be due to the fact that patients with PD generally have a sedentary lifestyle; that is, they are unable to complete enough physical exertion to induce respiratory adaptations that might promote respiratory dysfunction. 5 , 6 Therefore, it is important to assess respiratory muscle strength and lung function, as well as their impact on motor function, in patients with PD in order to implement therapeutic interventions aimed at improving respiratory muscle strength, lung function, and quality of life. 7 , 8
The objective of the present study was to investigate parameters of lung function and respiratory muscle strength in different stages of PD, as well as to determine their correlation with motor function and quality of life.
METHODS
This was a cross-sectional study conducted at the Federal University of Pernambuco Hospital das Clínicas Neurology Outpatient Clinic, located in the city of Recife, Brazil. The study was conducted under the auspices of the Pro-Parkinson Outreach Program, which is a referral program for patients with PD. The study was approved by the local research ethics committee (Protocol no. 49958315.2.0000.5208).
Patients routinely followed at the outpatient clinic were personally invited to participate in the study. The convenience sample consisted of patients clinically diagnosed with idiopathic PD in accordance with the Brazilian National Ministry of Health criteria 9 and healthy individuals. Participants were divided into two groups: PD and control.
The criteria for inclusion in the PD group were as follows: having been diagnosed with PD in accordance with the original Hoehn and Yahr (H&Y) scale 10 and having no cognitive impairment, as assessed by the Mini-Mental State Examination. 11 , 12 The exclusion criteria were as follows: being under 40 years of age; being over 80 years of age; having a history of lung disease; having undergone thoracic surgery; having undergone surgery (deep brain stimulation or stereotactic surgery) to treat PD symptoms; and failing to complete all of the tests. The control group comprised healthy adults in the 55- to 80-year age bracket. Smokers and former smokers were excluded from the study.
Respiratory muscle strength parameters (MIP and MEP) were assessed with a digital manometer (MVD 300; Globalmed, Porto Alegre, Brazil), in accordance with international guidelines, 13 being expressed in cmH2O. Three maneuvers were performed for each test, the best of the three being selected for analysis. Predicted values and percent predicted values were calculated from the equations provided by Pessoa et al. 14
Spirometry was performed with a portable spirometer (EasyOne; ndd Medical Technologies, Zurich, Switzerland), in accordance with international guidelines. 15 The following parameters were measured: FVC, FEV1, FEV1/FVC, FEF25-75%, and PEF. Results were expressed as absolute values, predicted values, and percent predicted values, in accordance with Pereira et al. 16
Motor function was assessed with subscale III of the Unified Parkinson’s Disease Rating Scale (UPDRS-III) while patients were in an “on” state (i.e., using levodopa). UPDRS-III consists of 14 items (items 18-31) that can be scored as 0-4 based on severity. 17 The UPDRS was developed in 1987 18 and is widely used in order to monitor disease progression and drug treatment efficacy. It assesses signs, symptoms, and certain activities by self-report and clinical observation. It consists of 42 items divided into four parts: I) mentation, behavior and mood; II) activities of daily living; III) motor examination; and IV) complications of therapy. Individual item scores range from 0 (normality) to 4 (disabling disease). 17 , 18 Each subscale can be administered separately; answers to UPDRS-III are clinically assessed by a health professional.
Quality of life was assessed with the 39-item Parkinson’s Disease Questionnaire (PDQ-39), which was adapted for use in Brazil in 2005, at the University of Oxford Department of Public Health and Primary Care Health Services Research Unit (in Oxford, UK). 19 The PDQ-39 is divided into 8 domains, total scores ranging from 0 to 100. A lower score translates to a better perceived quality of life. The total score and mobility domain score were correlated with lung function and respiratory muscle strength parameters.
The Shapiro-Wilk test was used in order to ascertain the normality of datasets. One-way ANOVA and a post hoc t-test were used in order to compare the groups. Pearson’s correlation coefficient was used in order to measure the relationship among functional variables, symptoms of PD, and quality of life, being expressed as r and %r2. Values of r = 0.10-0.39 (0-15%) indicated a weak correlation, values of r = 0.40-0.69 (15-50%) indicated a moderate correlation, and values of r = 0.70-1.00 (50-100%) indicated a strong correlation, in accordance with the classification proposed by Dancey and Reidy. 20 All statistical analyses were performed with the Predictive Analytics Software package for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA), values of p < 0.05 being considered significant.
RESULTS
A total of 89 individuals (70 PD patients and 19 controls) were recruited. Of those, 23 (21 PD patients and 2 controls) were excluded. Therefore, the final sample consisted of 66 individuals (49 PD patients and 17 controls; Figure 1). Because only 3 patients with H&Y stage 4 PD completed all of the tests, the PD group was subdivided as follows: patients with H&Y stage 1 PD (the H&Y1 group), patients with H&Y stage 2 PD (the H&Y2 group), and patients with H&Y stage 3/4 PD (the H&Y3/4 group; Table 1).
Figure 1. Flow chart of the data collection process.
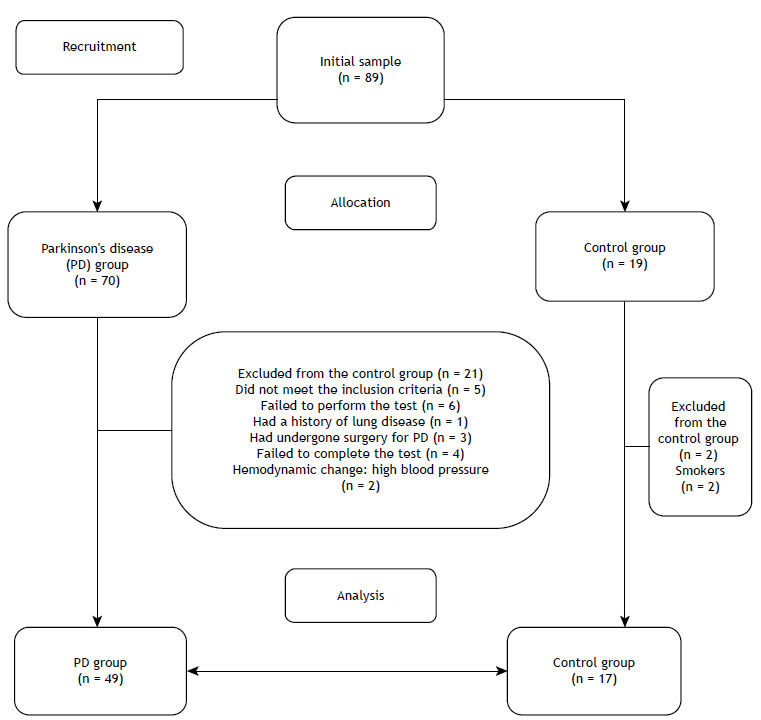
Table 1. Mean age, weight, height, and waist circumference, as well as their respective standard deviations, in controls and in patients at different stages of Parkinson’s disease.
| Variable | Controls | Parkinson’s disease | p* | ||
|---|---|---|---|---|---|
| H&Y1 | H&Y2 | H&Y3/4 | |||
| N = 17 (100%) | n = 17 (35%) | n = 19 (39%) | n = 13 (26%) | ||
| Age | 66 (6)** | 57 (9)** | 63 (8) | 67 (9)** | 0.006** |
| Weight | 68 (12) | 70 (9) | 73 (11) | 73 (8) | 0.53 |
| Height | 158 (6) | 162 (8) | 164 (10) | 163 (6) | 0.12 |
| WC | 99 (12) | 91 (12) | 97 (10) | 96 (12) | 0.24 |
H&Y: Hoehn and Yahr 10 ; H&Y1: patients with H&Y stage 1 Parkinson’s disease; H&Y2: patients with H&Y stage 2 Parkinson’s disease; H&Y3/4: patients with H&Y stage 3/4 Parkinson’s disease; and WC: waist circumference. *One-way ANOVA. **H&Y1 vs. controls and H&Y1 vs. H&Y3/4.
MIP and MEP were significantly and inversely correlated with PD severity, as well as being significantly lower in the PD group than in the control group (Table 2). Similarly, FEV1, PEF, and FEF25-75%, as well as percent predicted FVC, FEV1, PEF, and FEF25-75%, were significantly and inversely correlated with PD severity, as well as being significantly lower in the PD group than in the control group. The differences between the H&Y3/4 group and the remaining groups were all significant (Table 3).
Table 2. Mean maximal inspiratory and expiratory pressures (in cmH2O), as well as their corresponding standard deviations, in controls and in patients at different stages of Parkinson’s disease.
| Variable | Controls | Parkinson’s disease | p* | ||
|---|---|---|---|---|---|
| H&Y1 | H&Y2 | H&Y3/4 | |||
| N = 17 (100%) | n = 17 (35%) | n = 19 (39%) | n = 13 (26%) | ||
| MIP | −78.65 (22) | −59.00 (21) | −60.95 (20) | −48.85 (18) | 0.001 |
| Predicted MIP | 70.04 (11) | 80.97 (11) | 80.65 (12) | 79.76 (11) | 0.02 |
| MIP, % predicted | 112 (27) | 72 (19) | 77 (25) | 61 (18) | < 0.0001 |
| MEP | 106.53 (34) | 85.76 (22) | 90.00 (21) | 73.69 (33) | 0.016 |
| Predicted MEP | 103.02 (24) | 112.64 (26) | 115.30 (21) | 111.19 (26) | 0.29 |
| MEP, % predicted | 105 (28) | 79 (22) | 81 (25) | 66 (26) | 0.0005 |
H&Y: Hoehn & Yahr 10 ; H&Y1: patients with H&Y stage 1 Parkinson’s disease; H&Y2: patients with H&Y stage 2 Parkinson’s disease; and H&Y3/4: patients with H&Y stage 3/4 Parkinson’s disease. *One-way ANOVA and post hoc t-test (least significant difference). MIP: H&Y1 vs. controls (p < 0.006); H&Y2 vs. controls (p < 0.011); and H&Y3/4 vs. controls (p < 0.001). Predicted MIP: H&Y1 vs. controls (p = 0.007); H&Y2 vs. controls (p = 0.007); and H&Y3/4 vs. controls (p = 0.02). MIP, % predicted: H&Y1 vs. controls (p < 0.0001); H&Y2 vs. controls (p < 0.0001); and H&Y3/4 vs. controls (p < 0.0001). MEP: H&Y1 vs. controls (p = 0.031) and H&Y3/4 vs. controls (p = 0.002). MEP, % predicted: H&Y1 vs. controls (p = 0.002); H&Y2 vs. controls (p = 0.003); and H&Y3/4 vs. controls (p < 0.001).
Table 3. Mean lung function parameters and their corresponding standard deviations in controls and in patients at different stages of Parkinson’s disease.
| Variable | Controls | Parkinson’s disease | p* | ||
|---|---|---|---|---|---|
| H&Y1 | H&Y2 | H&Y3/4 | |||
| N = 17 (100%) | n = 17 (35%) | n = 19 (39%) | n = 13 (26%) | ||
| FVC, L | 2.6 (0.6) | 2.9 (0.6) | 2.8 (1.0) | 2.2 (0.9) | 0.06 |
| FVC, % predicted | 88 (14) | 85 (12) | 79 (18) | 61 (22) | 0.0006 |
| FEV1, L | 2.1 (0.5) | 2.4 (0.5) | 2.2 (0.7) | 1.7 (0.7) | 0.01 |
| FEV1, % predicted | 90 (18) | 84 (14) | 79 (18) | 59 (20) | 0.0002 |
| FEV1/FVC | 79.3 (4.5) | 79.7 (5.3) | 78.9 (6.9) | 77.6 (4.3) | 0.91 |
| FEV1/FVC, % predicted | 100 (5) | 100 (7) | 100 (9) | 990 (18) | 0.97 |
| PEF, L | 5.0 (1.5) | 6.0 (1.8) | 4.8 (1.5) | 3.2 (1.6) | 0.0005 |
| PEF, % predicted | 68 (15) | 72 (19) | 56 (16) | 36 (14) | 0.0001 |
| FEF25-75% | 2.2 (0.8) | 2.5 (0.7) | 2.1 (0.7) | 1.5 (0.9) | 0.01 |
| FEF25-75 %, % predicted | 98 (40) | 98 (34) | 84 (29) | 61 (32) | 0.01 |
H&Y: Hoehn & Yahr 10 ; H&Y1: patients with H&Y stage 1 Parkinson’s disease; H&Y2: patients with H&Y stage 2 Parkinson’s disease; and H&Y3/4: patients with H&Y stage 3/4 Parkinson’s disease. *One-way ANOVA and post hoc t-test (least significant difference). FVC, % predicted: H&Y1 vs. H&Y3/4 (p < 0.001); H&Y2 vs. H&Y3/4 (p = 0.004); and H&Y3/4 vs. controls (p < 0.001). FEV1: H&Y1 vs. H&Y3/4 (p = 0.002) and H&Y2 vs. H&Y3/4 (p = 0.012). FEV1, % predicted: H&Y1 vs. H&Y3/4 (p < 0.001); H&Y2 vs. H&Y3/4 (p = 0.003); H&Y2 vs. controls (p = 0.05); and H&Y3/4 vs. controls (p < 0.001). PEF: H&Y1 vs. H&Y2 (p = 0.026); H&Y1 vs. H&Y3/4 (p < 0.001); H&Y2 vs. H&Y3/4 (p = 0.008); and H&Y3/4 vs. controls (p = 0.004). PEF, % predicted: H&Y1 vs. H&Y2 (p = 0.003); H&Y1 vs. H&Y3/4 (p < 0.001); H&Y2 vs. H&Y3/4 (p = 0.001); H&Y2 vs. controls (p = 0.003); and H&Y3/4 vs. controls (p < 0,001). FEF25-75%: H&Y1 vs. H&Y3/4 (p = 0.001) and H&Y3/4 vs. controls (p = 0.0043). FEF25-75%, % predicted: H&Y1 vs. H&Y3/4 (p = 0.003) and H&Y3/4 vs. controls (p = 0.003).
Some of the lung function parameters were significantly correlated with bradykinesia and rigidity. Bradykinesia showed a statistically significant moderate inverse correlation with FEV1 and significant but weak inverse correlations with FVC, PEF, and FEF25-75%. Rigidity showed significant but weak inverse correlations with FVC and PEF. With regard to motor function, UPDRS-III scores showed significant but weak inverse correlations with FEF25-75%, PEF, and MEP (Table 4).
Table 4. Correlation of lung function and respiratory muscle strength parameters with cardinal signs and Unified Parkinson’s Disease Rating Scale subscale III (motor examination) scores in patients with Parkinson’s disease.
| Variable | Cardinal signs, r (r2, %) | Motor function, r (r2, %) | ||
|---|---|---|---|---|
| Tremor at rest | Rigidity | Bradykinesia | UPDRS III | |
| FVC | 0.05 (0.25) | −0.29 (8.4)* | −0.35 (12.2)* | −0.23 (5.2) |
| FEV1 | 0.12 (1.4) | −0.27 (7.2) | −0.41 (16.8)* | −0.25 (6.2) |
| FEV1/FVC | 0.17 (2.8) | 0.13 (1.6) | −0.10 (1.0) | -0.002 (0.0004) |
| PEF | −0.03 (0.09) | −0.35 (12.2)* | −0.37 (13.6)* | −0.31 (9.6)* |
| FEF25-75% | 0.08 (0.64) | −0.25 (6.2) | −0.39 (15.2)* | −0.32 (10.2)* |
| MIP | −0.04 (0.14) | 0.07 (0.4) | 0.15 (2.25) | 0.15 (2.2) |
| MEP | −0.03 (0.09) | −0.18 (3.2) | −0.25 (6.2) | −0.32 (10.2)* |
UPDRS-III: subscale III of the Unified Parkinson’s Disease Rating Scale. *Pearson’s correlation; p < 0.05.
Total PDQ-39 scores and PDQ-39 mobility domain scores showed significant moderate inverse correlations with FVC, FEV1, PEF, and MEP (Table 5).
Table 5. Correlation of lung function and respiratory muscle strength parameters with quality-of-life questionnaire scores in patients with Parkinson’s disease.
| Variable | Quality of life | |
|---|---|---|
| PDQ-39, r (r2, %) | PDQ-39 mobility domain, r (r2, %) | |
| FVC | −0.39 (15.2)* | −0.38 (14.4)* |
| FEV1 | −0.36 (12.9)* | −0.36 (12.9)* |
| FEV1/FVC | 0.20 (4.0) | 0.17 (2.8) |
| PEF | −0.31 (9.6)* | −0.30 (9)* |
| FEF25-75% | −0.19 (3.6) | −0.22 (4.8) |
| MIP | 0.24 (5.7) | 0.27 (7.2) |
| MEP | −0.42 (17.64)* | −0.37 (13.6)* |
PDQ-39: 39-item Parkinson’s Disease Questionnaire. *Pearson’s correlation; p < 0.05.
DISCUSSION
In the present study, maximal respiratory pressures decreased with the progression of PD, with significant differences between controls and patients with PD at all levels of disease severity. This finding demonstrates that maximum respiratory pressures are lower in patients with PD than in individuals without the disease, regardless of disease severity. Specific PD features might play a larger role in this process than do aging-related losses. In patients with PD, respiratory muscle weakness might be due to progressively reduced chest wall motion and, consequently, reduced tidal volume. 21 Therefore, reduced MIP and MEP values might be related to the inherent characteristics of PD, including postural changes (increased kyphosis), thoracic spine stiffness, and rib cage stiffness, all of which result in decreased muscle flexibility and control. 22 , 23 Chest muscle rigidity, bradykinesia, and tremors can severely compromise breathing in patients with PD. 22 , 24
Parasympathetic hyperactivity results in impaired respiratory physiology and, consequently, airway smooth muscle constriction. 25 Patients with neuromuscular disease present with altered activity in the respiratory centers, as evidenced by impaired activation and coordination of the muscles that control central airway function. 26 , 27 Therefore, our findings are consistent with those of Seccombe et al., 28 who found that MIP and MEP were below the normal range in 68% and 79% of patients, respectively. Sathyaprabha et al. 29 found that respiratory muscle strength was significantly lower in individuals with PD than in those without the disease. They found an improvement in MIP and MEP in PD patients receiving levodopa in comparison with those not receiving the drug. These findings are consistent with those of Weiner et al. 30
In the present study, certain lung function parameters (FVC, FEV1, FEF25-75%, and PEF) decreased significantly as PD progressed. Patients with PD typically present with restrictive lung disease, the most common changes being reduced tidal volume, reduced minute volume, and reduced inspiratory flow. These changes are related to respiratory muscle stiffness and hypokinesia, which are characteristic signs of PD. 6 , 28 , 29
Although respiratory symptoms are rare in the early stages of PD, there have been reports of changes in lung function and respiratory mechanics in patients with PD. 18 , 26 , 29 Possible explanations for reduced lung volume and capacity include the following: impaired upper airway muscle function affecting airflow resistance and causing flow oscillation 27 ; diaphragmatic flutter 30 ; and reduced MEP. 31
Significant inverse correlations were found between UPDRS-III scores and the following lung function parameters: FVC, FEV1, PEF, and FEF25-75%. A worse motor function (i.e., a higher UPDRS-III score) translates to lower FVC, FEV1, PEF, and FEF25-75%. The respiratory system of patients with PD is likely affected by impaired motor function, with reduced thoracic motion resulting in postural misalignment and osteoarticular degeneration, both of which affect respiratory mechanics. 32 Significantly increased motor symptoms, including bradykinesia and rigidity, which worsen when patients are off levodopa, have been shown to be associated with reduced lung function and impaired respiratory mechanics. 33 , 34 Our findings are consistent with those of a study in which a strong inverse correlation was found between PEF and PDQ-39 scores in patients with PD. 34
With regard to quality of life, total PDQ-39 scores and PDQ-39 mobility domain scores showed moderate inverse correlations with FVC, FEV1, PEF, and MEP. As the disease progresses, motor changes negatively affect patient physical, mental, emotional, and socioeconomic status, resulting in poor perceived quality of life. In addition, impaired mobility leads to social isolation and reduced activities of daily living, with progressive worsening of pulmonary complications. 35
Although it is important to determine the impact that changes in lung function and respiratory mechanics have on the quality of life of patients with PD, few studies have addressed this issue, further studies therefore being required.
Footnotes
Study carried out at the Ambulatório de Neurologia, Hospital das Clínicas, Universidade Federal de Pernambuco - UFPE - Recife (PE) Brasil.
Financial support: None.
REFERENCES
- 1.Monteiro L, Souza-Machado A, Pinho P, Sampaio M, Nóbrega AC, Melo A. Swallowing impairment and pulmonary dysfunction in Parkinson's disease the silent threats. J Neurol Sci. 2014;339(1-2):149–152. doi: 10.1016/j.jns.2014.02.004. [DOI] [PubMed] [Google Scholar]
- 2.Ferreira FV, Cielo CA, Trevisan ME. Respiratory, posture and vocals features in Parkinson's Disease theoretical considerations [Article in Portuguese]. Rev. CEFAC. 2011;13(3):534–540. doi: 10.1590/S1516-18462010005000135. [DOI] [Google Scholar]
- 3.Ramos ML, Neves DR, Lima VP, Orsini M, Machado D, Bastos VH. Analysis of pneumofunctional parameters in patients with Parkinson's disease pilot study [Article in Portuguese]. Rev Bras. Neurol. 2014;50(2):38–43. [Google Scholar]
- 4.Ferreira FV, Cielo CA, Trevisan ME. Respiratory muscle strength, body posture, vocal intensity and maximum phonation times in Parkinson Disease [Article in Portuguese] Rev. CEFAC. 2012;14(2):361–368. doi: 10.1590/S1516-18462010005000103. [DOI] [Google Scholar]
- 5.Sabaté M, Rodríguez M, Méndez E, Enríquez E, González I. Obstructive and restrictive pulmonary dysfunction increases disability in Parkinson disease. Arch Phys Med Rehabil. 1996;77(1):29–34. doi: 10.1016/S0003-9993(96)90216-6. [DOI] [PubMed] [Google Scholar]
- 6.Parreira VF, Guedes LU, Quintão DG, Silveira EP, Tomichs GM, Sampaio RF. Breathing pattern in Parkinson's disease patients and healthy elderly subjects [Article in Portuguese] Acta. Fisiatrica. 2003;10(2):61–66. [Google Scholar]
- 7.Fleck CS, Gerzson LR, Steidl EM, Hernandez NM. Characterization of functional capacity, cognitive level and respiratory muscle strength of elderly women with parkinsonian syndrome [Article in Portuguese] Estud Interdiscipl. Envelhec. 2014;19(1):109–121. [Google Scholar]
- 8.Sanches VS, Santos FM, Fernandes JM, Santos ML, Müller PT, Christofoletti G. Neurodegenerative disorders increase decline in respiratory muscle strength in older adults. Respir Care. 2014;59(12):1838–1845. doi: 10.4187/respcare.03063. [DOI] [PubMed] [Google Scholar]
- 9.Brasil . Portaria no. 228 de 10 de maio de 2010. Brasília: Ministério da Saúde; 2010. [Google Scholar]
- 10.Hoehn MM, Yahr MD. Parkinsonism onset, progression and mortality. Neurology. 1967;17(5):427–442. doi: 10.1212/wnl.17.5.427. [DOI] [PubMed] [Google Scholar]
- 11.Brucki SM, Rocha MS. Category fluency test effects of age, gender and education on total scores, clustering and switching in Brazilian Portuguese-speaking subjects. Braz J Med Biol Res. 2004;37(12):1771–1777. doi: 10.1590/S0100-879X2004001200002. [DOI] [PubMed] [Google Scholar]
- 12.Vitiello AP, Ciríaco JG, Takahashi DY, Nitrini R, Caramelli P. Brief cognitive evaluation of patients attended in a general neurological outpatient clinic [Article in Portuguese] Arq. Neuropsiquiatr. 2007;65(2A):299–303. doi: 10.1590/S0004-282X2007000200021. [DOI] [PubMed] [Google Scholar]
- 13.American Thoracic Society/European Respiratory Society ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624. doi: 10.1164/rccm.166.4.518. [DOI] [PubMed] [Google Scholar]
- 14.Pessoa IM, Houri M, Neto, Montemezzo D, Silva LA, Andrade AD, Parreira VF. Predictive equations for respiratory muscle strength according to international and Brazilian guidelines. Braz J Phys Ther. 2014;18(5):410–418. doi: 10.1590/bjpt-rbf.2014.0044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 16.Pereira CA, Sato T, Rodrigues SC. New reference values for forced spirometry in white adults in Brazil. J Bras Pneumol. 2007;33(4):397–406. doi: 10.1590/s1806-37132007000400008. [DOI] [PubMed] [Google Scholar]
- 17.Palmer JL, Coats MA, Roe CM, Hanko SM, Xiong C, Morris JC. Unified Parkinson's Disease Rating Scale-Motor Exam: inter-rater reliability of advanced practice nurse and neurologist assessments J Adv. Nurs. 2010;66(6):1382–1387. doi: 10.1111/j.1365-2648.2010.05313.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fahn S Elton RL, UPDRS Development Committee Fahn S, Marsden CD, Calne D, Goldstein M. Recent developments in Parkinson's disease. Florham Park [NJ, USA]: MacMillan Healthcare Information; 1987. Unified Parkinson's Disease Rating Scale; pp. 153–163. [Google Scholar]
- 19.Lana RC, Álvares LMRS, Nasciutti-Prudente C, Goulart FRP, Teixeira-Salmela LF, Cardoso FE. Perception of quality of life in individuals with Parkinson's disease using the PDQ-39. Rev Bras Fisioter. 2007;11(5):397–402. doi: 10.1590/S1413-35552007000500011. [DOI] [Google Scholar]
- 20.Dancey C, Reidy J. Estatística sem matemática para psicologia: usando SPSS para Windows. 5. Porto Alegre: Artmed; 2006. [Google Scholar]
- 21.Frazão M, Cabral E, Lima I, Resqueti V, Florêncio R, Aliverti A. Assessment of the acute effects of different PEP levels on respiratory pattern and operational volumes in patients with Parkinson's disease. Respir Physiol Neurobiol. 2014;198:42–47. doi: 10.1016/j.resp.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 22.Cardoso SR, Pereira JS. Analysis of breathing function in Parkinson's disease [Article in Portuguese] Arq. Neuropsiquiatr. 2002;60(1):91–95. doi: 10.1590/S0004-282X2002000100016. [DOI] [PubMed] [Google Scholar]
- 23.Goulart F, Santos CC, Teixeira-Salmela LF, Cardoso F. Analysis of functional performance in patients with Parkinson's disease [Article in Portuguese] Acta. Fisiatrica. 2004;11(1):12–16. doi: 10.5935/0104-7795.20040001. [DOI] [Google Scholar]
- 24.Guedes LU, Rodrigues JM, Fernandes AA, Cardoso FE, Parreira VF. Respiratory changes in Parkinson's disease may be unrelated to dopaminergic dysfunction. Arq Neuropsiquiatr. 2012;70(11):847–851. doi: 10.1590/S0004-282X2012001100005. [DOI] [PubMed] [Google Scholar]
- 25.Mikaelee H, Yazdchi M, Ansarin K, Arami M. Pulmonary Function Tests Abnormalities In Parkinson Disease. Internet J Pulm Med. 2006;8(2):1–5. doi: 10.5580/e0f. [DOI] [Google Scholar]
- 26.De Pandis MF, Starace A, Stefanelli F, Marruzzo P, Meoli I, De Simone G. Modification of respiratory function parameters in patients with severe Parkinson's disease. Neurol Sci. 2002;23(2):S69–S70. doi: 10.1007/s100720200074. [DOI] [PubMed] [Google Scholar]
- 27.Vincken W, Elleker G, Cosio MG. Detection of upper airway muscle involvement in neuromuscular disorders using the flow-volume loop. Chest. 1986;90(1):52–57. doi: 10.1378/chest.90.1.52. [DOI] [PubMed] [Google Scholar]
- 28.Seccombe LM, Giddings HL, Rogers PG, Corbett AJ, Hayes MW, Peters MJ. Abnormal ventilatory control in Parkinson's disease--further evidence for non-motor dysfunction. Respir Physiol Neurobiol. 2011;179(2-3):300–304. doi: 10.1016/j.resp.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 29.Sathyaprabha TN, Kapavarapu PK, Thennarasu K, Raju TR. Pulmonary functions in Parkinson's disease. Indian J Chest Dis Allied Sci. 2005;47(4):251–257. [PubMed] [Google Scholar]
- 30.Weiner P, Inzelberg R, Davidovich A, Nisipeanu P, Magadle R, Berar-Yanay N. Respiratory muscle performance and the perception of dyspnea in Parkinson's disease. Can J Neurol Sci. 2002;29(1):68–72. doi: 10.1017/S031716710000175X. [DOI] [PubMed] [Google Scholar]
- 31.Wang Y, Shao WB, Gao L, Lu J, Gu H, Sun LH. Abnormal pulmonary function and respiratory muscle strength findings in Chinese patients with Parkinson's disease and multiple system atrophy--comparison with normal elderly. PLoS One. 2014;9(12):e116123. doi: 10.1371/journal.pone.0116123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Owolabi LF, Nagoda M, Babashani M. Pulmonary function tests in patients with Parkinson's disease A case-control study. Niger J Clin Pract. 2016;19(1):66–70. doi: 10.4103/1119-3077.173714. [DOI] [PubMed] [Google Scholar]
- 33.Estenne M, Hubert M, De Troyer A. Respiratory-muscle involvement in Parkinson's disease. New Eng J Med. 1984;311(23):1516–1517. doi: 10.1056/NEJM198412063112314. [DOI] [PubMed] [Google Scholar]
- 34.Yust-Katz S, Shitrit D, Melamed E, Djaldetti R. Respiratory distress an unrecognized non-motor phenomenon in patients with parkinsonism. J Neural Transm (Vienna) 2012;119(1):73–76. doi: 10.1007/s00702-011-0671-0. [DOI] [PubMed] [Google Scholar]
- 35.Lim A, Leow L, Huckabee ML, Frampton C, Anderson T. A pilot study of respiration and swallowing integration in Parkinson's disease "on" and "off" levodopa. Dysphagia. 2008;23(1):76–81. doi: 10.1007/s00455-007-9100-9. [DOI] [PubMed] [Google Scholar]