

Key Points
Ixazomib, dexamethasone, and rituximab (IDR) was associated with overall, major, and very good partial response rates of 96%, 77%, and 19%.
Responses to IDR were durable, with a median PFS of 40 months, and the safety profile was excellent with no grade 4 adverse events.
Abstract
Proteasome inhibition is a standard of care for the primary treatment of patients with Waldenström macroglobulinemia (WM). We present the long-term follow-up of a prospective, phase II clinical trial that evaluated the combination of ixazomib, dexamethasone, and rituximab (IDR) in 26 treatment-naive patients with WM. IDR was administered as 6 monthly induction cycles followed by 6 every-2-month maintenance cycles. The MYD88 L265P mutation was detected in all patients, and CXCR4 mutations were detected in 15 patients (58%). The median time to response (TTR) and time to major response (TTMR) were 2 and 6 months, respectively. Patients with and without CXCR4 mutations had median TTR of 3 months and 1 month, respectively (P = .003), and median TTMR of 10 months and 3 months, respectively (P = .31). The overall, major, and very good partial response (VGPR) rates were 96%, 77%, and 19%, respectively. The rate of VGPR in patients with and without CXCR4 mutations were 7% and 36%, respectively (P = .06). The median progression-free survival (PFS) was 40 months, the median duration of response (DOR) was 38 months, and the median time to next treatment (TTNT) was 40 months. PFS, DOR, and TTNT were not affected by CXCR4 mutational status. The safety profile was excellent with no grade 4 adverse events or deaths to date. IDR provides a safe and effective frontline treatment option for symptomatic patients with WM. This study was registered at www.clinicaltrials.gov as #NCT02400437.
Visual Abstract

Introduction
Proteasome inhibitors (PIs) have shown to be effective in the primary treatment of symptomatic patients with Waldenström macroglobulinemia (WM). Specifically, bortezomib- and carfilzomib-containing regimens have been associated with durable responses in patients with WM.1-4 However, toxicity remains an issue with PIs, as bortezomib has been associated with high rates of peripheral neuropathy, and carfilzomib can induce cardiac events, especially in the elderly.3,5
Approximately 30% to 40% of patients with WM harbor frameshift and/or nonsense somatic, activating CXCR4 mutations.6 CXCR4 mutations can adversely affect the response and survival outcomes to Bruton tyrosine kinase (BTK) inhibitors in some but not all patients with WM.7-9 It is possible that specific CXCR4 mutation subtypes (ie, nonsense vs frameshift) or the clonality level of these mutations could be at the center of this heterogeneity.10 Preclinical studies have also suggested that CXCR4 mutations could induce resistance to PIs, although the evidence has been inconsistent,11,12 and the impact of CXCR4 mutations on the outcomes of patients with WM treated with PIs is evolving.13,14
The oral PI ixazomib, in combination with dexamethasone and rituximab (IDR), has been shown to be safe and effective in patients with WM.15 IDR offers a competitive treatment option for patients with WM, given the ease of administration, high efficacy rate, and excellent safety profile. In this study, we present the long-term follow-up on the outcomes of previously untreated patients with WM treated with IDR. We evaluated clinical features as well as response and survival outcomes according to CXCR4 mutations status.
Methods
Trial design
This study was a single-center, investigator-initiated, single-arm, prospective phase II study. The Institutional Review Board of the Harvard/Dana-Farber Cancer Center granted study approval. The study was conducted in accordance with the Declaration of Helsinki. Takeda Pharmaceuticals, the manufacturer of ixazomib, provided drug free of charge and funds to carry on the research. Rituximab and dexamethasone were obtained commercially.
Participants
Eligible participants were adults older than 18 years old who had a clinicopathologic diagnosis of WM,16 were previously untreated, and met criteria for treatment initiation according to the Second International Workshop for Waldenström’s Macroglobulinemia guidelines.17 Other inclusion criteria were Eastern Cooperative Oncology Group performance status of 0 to 2, neutrophil count ≥1 × 103/μL, platelet count ≥75 × 103/μL, total bilirubin <1.5 times the upper limit of normal, alanine and aspartate aminotransferase <3 times the upper limit of normal, and creatinine clearance ≥30 mL/min. Exclusion criteria included, but were not limited to, any prior therapy for WM; active infection with HIV, hepatitis B, or hepatitis C; involvement of the central nervous system by WM; pregnant or lactating women; and any condition that could have affected the gastrointestinal absorption of ixazomib. Written informed consent was obtained from all participants prior to any research procedure.
Interventions
Treatment protocol consisted of 4 mg ixazomib and 20 mg dexamethasone orally on days 1, 8, and 15, and 375 mg/m2 rituximab IV on day 1. The protocol was administered for 6 4-week induction cycles followed by 6 8-week maintenance cycles, for a total of 12 cycles. Rituximab was held for the first 2 induction cycles of therapy to minimize the risk of IgM flare. Patients proceeded to receive maintenance if they had had at least minor response or clinical benefit from induction. Herpes zoster prophylaxis and proton pump inhibitors or H2 blockers were administered throughout IDR therapy. Prophylactic use of plasmapheresis before the administration of rituximab was recommended for patients with serum IgM levels >4000 mg/dL. Baseline studies included complete blood counts, comprehensive metabolic panel, serum IgM and β2-microglobulin levels, serum protein electrophoresis (SPEP), bone marrow biopsy and aspiration, and computed tomography (CT) scans of the chest, abdomen, and pelvis with IV contrast. Efficacy and toxicity were assessed on the first day of each cycle, starting at cycle 2, and thereafter, every 12 weeks for 3 years after a patient had completed therapy. If extramedullary disease was present at baseline, bone marrow biopsy and aspiration and CT scans were performed at the interphase (between the end of induction and the start of maintenance) and at the end of maintenance. MYD88 and CXCR4 mutational status was determined using DNA isolated from CD19-selected bone marrow cells as previously described.6,18 TP53 mutations were evaluated in unsorted bone marrow samples using the Rapid Heme Panel, a clinically validated next-generation sequencing platform.19
Outcomes
Response determinations were made using consensus criteria adapted from the Third International Workshop for Waldenström’s Macroglobulinemia.20 Briefly, minor response was defined as a decrease in serum IgM level of ≥25% but <50% when compared with baseline. Partial response (PR) was defined as a decrease of ≥50% but <90%. Very good partial response (VGPR) was defined as a decrease of ≥90% or serum IgM level normalization but with persistence of a detectable IgM monoclonal paraprotein in SPEP. Complete response was defined as normalization of serum IgM, SPEP, CT scans, and bone marrow biopsy. Overall response was defined as minor response or better, and major response was defined as PR or better. Time to response (TTR) was defined as the time from treatment initiation until at least minor response was attained, and time to major response (TTMR) was defined as the time from treatment initiation until at least PR was attained. Adverse events were graded according to the Common Terminology Criteria for Adverse Events, version 4.03.21 Progression-free survival (PFS) was defined as the time from treatment initiation until the last follow-up, progression, or death from any cause. Duration of response (DOR) was defined as the time from attainment of response until the last follow-up, progression, or death from any cause. Time to next treatment (TTNT) was defined as the time from the last dose of IDR until initiation of the next line of therapy. Overall survival was defined as the time from treatment initiation until the last follow-up or death from any cause. The primary objective of the study was determination of VGPR or better. Secondary objectives were determination of overall response, major response rate, PFS, safety and tolerability of IDR, as well as the impact of CXCR4 mutations on response and survival outcomes.
Statistical methods
Sample size was estimated assuming an expected VGPR or better of 40% and a minimal acceptable VGPR rate of 18%, with α of 0.05 and power of 80%, on the basis of assumptions derived from previous published experience with PIs. The Wilcoxon rank-sum test was used to compare independent continuous variables, the Fisher’s exact test was used for independent categorical variables, and the Student t test was used for dependent continuous variables. Confidence intervals (CI) of proportions were estimated using the Clopper-Pearson method. The Kaplan-Meier method for incomplete observations was used to estimate time to event distributions, which were compared using the log-rank test. P < .05 were considered statistically significant. All graphics and calculations were obtained using STATA version 15.1 (StataCorp LP, College Station, TX).
Results
Patients’ characteristics
Between 4 May 2015 and 2 May 2016, a total of 27 patients were considered for the study, and 26 patients started study therapy (Figure 1). One patient was excluded before study therapy because of a diagnosis of diffuse large B-cell lymphoma. At the time of this report, all patients have stopped study therapy and have completed the mandatory follow-up for this study. All patients had MYD88 L265P mutations. Fifteen patients (58%) had a CXCR4 mutation, of which 10 had nonsense mutations (5 had R338X, 4 had S338X, and 1 had G336X) and 5 had frameshift mutations (T318fs, L326fs, K327fs, S347fs, and H350fs). The patients’ baseline characteristics are shown in Table 1. CXCR4 mutated patients had higher median serum IgM levels and were less likely to present with lymphadenopathy than patients without CXCR4 mutations. No significant differences in the patients’ characteristics were detected between patients with nonsense and frameshift CXCR4 mutations (P > .05 for all variables).
Figure 1.

CONSORT diagram. The patient excluded was found to have diffuse large B-cell lymphoma at screening.
Table 1.
Patients’ characteristics per CXCR4 mutational status
| Characteristic | Patient population (N = 26) | CXCR4 mutated (n = 15) | CXCR4 wild type (n = 11) | P |
|---|---|---|---|---|
| Age at treatment initiation, median (range), y | 65 (46-82) | 65 (46-77) | 68 (54-82) | .46 |
| Age at treatment initiation >65 y, n (%) | 12 (46) | 6 (40) | 6 (55) | .69 |
| Hemoglobin level, median (range), g/dL | 10.2 (6.9-13.2) | 10.6 (6.9-11.6) | 9.8 (7.7-12) | .69 |
| Hemoglobin level ≤11.5 g/dL, n (%) | 21 (81) | 11 (73) | 10 (91) | .35 |
| Platelet count, median (range), × 103/μL | 211.5 (77-420) | 160 (77-346) | 243 (82-420) | .23 |
| Platelet count ≤100 × 103/μL, n (%) | 4 (15) | 3 (20) | 1 (9) | .61 |
| Serum β2-microglobulin level, median (range), mg/L | 3.95 (1.8-10.8) | 3.7 (2-4.8) | 5.3 (1.8-10.8) | .23 |
| Serum β2-microglobulin level >3 mg/L, n (%) | 20 (77) | 10 (67) | 10 (91) | .20 |
| Serum IgM level, median (range), mg/dL | 5074.5 (653-7650) | 5586 (1310-7650) | 4,040 (653-7350) | .005 |
| Serum IgM level ≥7000 mg/dL, n (%) | 2 (8) | 1 (7) | 1 (9) | 1.00 |
| Percentage of bone marrow involvement, median (range) | 55 (5-95) | 55 (5-95) | 52.5 (20-90) | .60 |
| Bone marrow involvement ≥60%, n (%) | 10 (38) | 6 (40) | 4 (36) | 1.00 |
| Lymphadenopathy ≥1.5 cm, n (%) | 14 (54) | 5 (33) | 8 (82) | .02 |
| Splenomegaly ≥15 cm, n (%) | 3 (12) | 1 (6) | 2 (18) | .56 |
| IPSSWM, n (%) | ||||
| Low risk | 5 (19) | 4 (27) | 1 (9) | .38 |
| Intermediate risk | 11 (42) | 6 (40) | 3 (27) | |
| High risk | 10 (38) | 5 (33) | 7 (64) |
IPSSWM, International Prognostic Scoring System for Waldenström Macroglobulinemia.
TTR
Median TTR was 2 months (95% CI, 1-2 months), and the median time to major response TTMR was 6 months (95% CI, 4-15 months). Patients with CXCR4 mutations had statistically longer median TTR when compared with patients without CXCR4 mutations (3 vs 1 month, respectively; P = .003; Figure 2A). No other factors evaluated (ie, age at treatment initiation, hemoglobin levels, platelet counts, serum IgM levels, serum β2-microglobulin levels, bone marrow involvement, presence of lymphadenopathy or splenomegaly, and International Prognostic Scoring System for Waldenström Macroglobulinemia) were associated with TTR (P > .05 for all variables). The median TTR in patients with nonsense and frameshift CXCR4 mutations were 4 and 2 months, respectively (P = .31). Patients with CXCR4 mutations had a median TTMR of 10 months vs 3 months in patients without CXCR4 mutations (P = .31; Figure 2B). The median TTMR in patients with nonsense and frameshift CXCR4 mutations were 12 and 6 months, respectively (P = .41). None of the evaluated factors were associated with TTMR (P > .05 for all variables).
Figure 2.
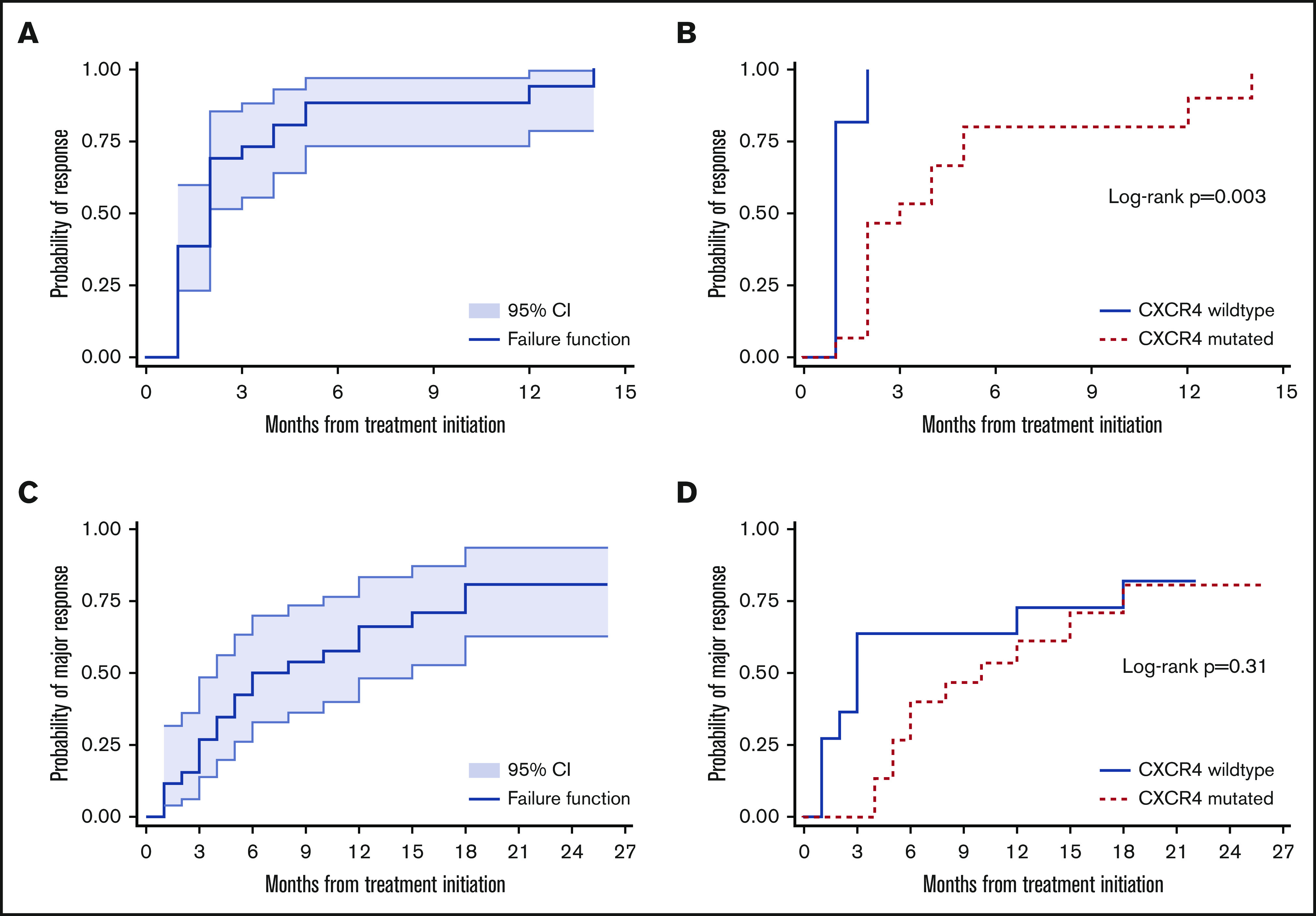
Kaplan-Meier estimates for TTR and TTMR. Kaplan-Meier estimates for TTR for the entire cohort (A) and according to CXCR4 mutational status (B). TTMR for the entire cohort (C) and according to CXCR4 mutational status (D) of 26 patients with WM treated with IDR.
Response to therapy
At best response, 5 patients (19%) attained VGPR, 15 (58%) attained PR, 5 (19%) attained minor response, and 1 (4%) had stable disease, for an ORR of 96% (95% CI, 80% to 100%) and a major response rate of 77% (95% CI, 56% to 91%). Categorical responses according to CXCR4 mutational status are shown in Figure 3. The VGPR rates in patients with and without CXCR4 mutations were 7% vs 36%, respectively (P = .06). None of the 10 patients with nonsense mutations, and only 1 of the 5 patients with frameshift CXCR4 mutations attained VGPR (P = .36). No other evaluated factor was associated with major response or VGPR rate (P > .05 for all variables).
Figure 3.

Response rates of 26 patients with WM treated with IDR according to CXCR4 mutational status. Major response rates were 93% and 100% for patients with and without CXCR4 mutations, respectively.
At best response, median serum IgM level decreased from 5067 mg/dL (range, 653-7650 mg/dL) to 905 mg/dL (range, 69-5500 mg/dL; P < .001 when compared with baseline). In patients without CXCR4 mutations, median serum IgM decreased from 4040 mg/dL (range, 653-7350 mg/dL) to 563 mg/dL (range, 89-2663 mg/dL; P < .001). In CXCR4-mutated patients, median serum IgM decreased from 5586 mg/dL (range, 1310-7650 mg/dL) to 1121 mg/dL (range, 69-5500 mg/dL; P < .001). The median serum IgM reduction in patients with wildtype and mutated CXCR4 status was 81% (range, 41% to 98%) and 80% (range, 21% to 98%), respectively (P = .69). In patients with nonsense CXCR4 mutations, the median serum IgM decreased from 5710 mg/dL (range, 1310-7650 mg/dL) to 1513 mg/dL (range, 250-5500 mg/dL; P < .001). In patients with frameshift CXCR4 mutations, the median serum IgM decreased from 5201 mg/dL (range, 3562-5694 mg/dL) to 670 mg/dL (range, 69-3943 mg/dL; P = .003). The median serum IgM reduction in patients with nonsense and frameshift CXCR4 mutations was 67% (range, 21% to 90%) and 86% (range, 31% to 98%), respectively (P = .20).
Survival
With a median follow-up of 52 months (95% CI, 47-55), 14 patients experienced disease progression. The median PFS was 40 months (95% CI, 22 to not reached [NR]; Figure 4A). None of the 5 patients who attained VGPR have progressed. The median PFS for the 16 patients who attained PR was 39 months, and for the 6 patients who attained major response or stable disease was 22 months. The median PFS for patients with and without CXCR4 mutations were 40 months (95% CI, 22-53) and 36 months (95% CI, 17 to NR), respectively (P = .72; Figure 4B). There was no detectable difference in PFS between patients with nonsense and frameshift CXCR4 mutations (P = .90). The median DOR for the 25 patients who attained a response to IDR was 38 months (95% CI, 20 to NR; Figure 4C). The median DOR for patients with and without CXCR4 mutations were 38 months (95% CI, 20-54) and 35 months (95% CI, 16 to NR), respectively (P = .62; Figure 4D). There was no detectable difference in PFS between patients with nonsense and frameshift CXCR4 mutations (P = .80). Nine patients have received a subsequent therapy; 5 received BTK-containing regimens, 2 received venetoclax, 1 received bendamustine-containing regimens, and 1 received daratumumab. All patients responded to subsequent therapy. The median TTNT was 40 months (95% CI, 24 to NR; Figure 4E). The median TTNT for patients with and without CXCR4 mutations were 40 months (95% CI, 18 to NR) and NR, respectively (P = .73; Figure 4F). There was no detectable difference in PFS between patients with nonsense and frameshift CXCR4 mutations (P = .44). There have been no deaths, for an overall survival rate of 100% (95% CI, 87% to 100%).
Figure 4.

Kaplan-Meier estimates for PFS, DOR, and TTNT. Kaplan-Meier estimates for PFS for the entire cohort (A) and according to CXCR4 mutational status (B). DOR for the entire cohort (C) and according to CXCR4 mutational status (D). TTNT for the entire cohort (E) and according to CXCR4 mutational status (F) of 26 patients with WM treated with IDR.
Safety
There were no grade 4 adverse events. Grade 3 adverse events included infections (n = 2, unrelated to IDR), hyperglycemia (n = 2, because of dexamethasone), infusion reactions (n = 2, because of rituximab), and neuropathy (n = 1, because of diabetes). Twenty-one patients (81%) completed the 12 planned cycles of therapy. Of the 5 patients that stopped therapy earlier than planned, 3 did so because of suboptimal response or lack of clinical benefit, 1 because of progressive neuropathy that was considered to be related to uncontrolled diabetes, and 1 because of infections unrelated to study therapy. Rituximab was stopped early in 2 patients because of infusion-related reactions. In 1 patient, rituximab was stopped during cycle 2 of maintenance after receiving 7 of the planned 10 doses of rituximab, for a rituximab dose intensity of 70%. In the other patient, rituximab was stopped during cycle 5 of maintenance after receiving 2 doses of rituximab, for a rituximab dose intensity of 20%. The 2 patients in whom rituximab was stopped early completed all the remaining cycles of the study without rituximab and progressed within 2 years of treatment initiation. The ixazomib dose was reduced to 3 mg in 1 patient during cycle 5 of induction because of failure to thrive, and IDR was stopped after cycle 5, for an ixazomib dose intensity of 95%. No patient had to discontinue ixazomib because of toxicity.
TP53 mutations
One of the patients with a nonsense CXCR4 S338X mutation also harbored a TP53 R196X mutation. This patient presented with symptomatic anemia, a serum IgM level of 1310 mg/dL, 80% bone marrow involvement, and no evidence of lymphadenopathy or extramedullary disease. TTR and TTMR were 6 and 14 months, respectively. At best response, the patient attained PR. As of last follow-up visit, the patient had not yet progressed, for a PFS of 47 months.
Discussion
Proteasome inhibition is a standard of care for the treatment of patients with WM, with an approximate rate of use as primary therapy in 10% to 15% of patients with WM, reported in a United States Surveillance, Epidemiology, and End Results–Medicare database population-based study.22 Similarly, a large registry study from Europe reported an approximate rate of use of 5% to 10% of PIs in the treatment of patients with WM.23 Several studies have reported encouraging results on the combination of PIs and rituximab as primary therapy in patients with WM, with ORR between 85% to 95%, major response rates between 60% to 80%, and median PFS between 40-60 months.1-4 However, peripheral neuropathy leading to treatment discontinuation and cardiac events, especially in elderly patients, have been described with bortezomib and carfilzomib, respectively.3,5 In addition, bortezomib and carfilzomib are parenteral agents, requiring once or twice weekly visits to infusion centers for treatment administration. Ixazomib is a novel, oral PI that has been shown to be safe and effective in patients with multiple myeloma.24,25 To our knowledge, this is the first clinical trial evaluating ixazomib in patients with WM.
IDR showed efficacy as a primary therapy in patients with WM. The responses were rapid with median TTR and TTMR of 2 and 6 months, respectively. IDR also induced high rates of response with ORR, major response, and VGPR rates at 96%, 77%, and 19%, respectively. Finally, the median PFS, DOR, and TTNT were 40, 38, and 40 months, respectively. The sample size of this study was estimated based on the assumption that IDR would induce a 40% VGPR rate and, on the basis of this factor alone, one could argue that the study did not meet the primary outcome. However, prior PI-based combination regimens have been associated with similar time to response, depth of response, and DOR than IDR. It could be argued that disease control, rather than depth of response, should be the main objective of therapy in a large proportion of patients with WM.26 Thus, given the rapid, deep, and durable responses associated with IDR, it should not be dismissed as an ineffective option for patients with WM.
A salient aspect of IDR therapy is the benign safety profile with few grade 3 and no grade 4 adverse events reported. One patient had a grade 3 neuropathy that was considered to be related to uncontrolled diabetes. In contrast, twice-weekly bortezomib, in combination with dexamethasone and rituximab (BDR), was associated with 30% rates of grade ≥3 neutropenia and peripheral neuropathy, leading to premature bortezomib discontinuation in 60% of patients.3 Once-weekly BDR had lower rates of grade ≥3 neutropenia and peripheral neuropathy than twice-weekly BDR, at 15% and 7%, respectively, leading to bortezomib dose reduction in 37% and discontinuation in 8% of patients.1 Carfilzomib, in combination with dexamethasone and rituximab (CaRD), was not associated with neuropathy but the rates of grade ≥3 hyperglycemia, hyperlipasemia, neutropenia, and cardiomyopathy were 23%, 16%, 10%, and 3%, respectively.4 In this study, ixazomib dose reduction was needed in 1 patient, and no patient discontinued ixazomib prematurely. Moreover, oral administration of ixazomib permitted fewer visits (once per month) to the treating center for rituximab administration. By comparison, 1 to 2 visits per week are required with BDR or CaRD therapy. Therefore, IDR provides an easier-to-administer regimen that is well tolerated among the PI-based treatment options for patients with WM.
In addition to our experience in treatment-naive patients, IDR is currently being evaluated in patients with previously treated WM in a phase I/II study by the Haemato-Oncology Foundation for Adults in the Netherlands. Preliminary data from this study were presented at the 61st Annual Meeting of the American Society of Hematology.27 Sixty patients were enrolled, and with a median follow-up of 20 months, ORR, major response and VGPR rates or better were 88%, 68%, and 24%, respectively. The median PFS was not yet reached. Expected in a more heavily pretreated population, grade ≥3 adverse events were reported in 38% of patients, and there were 6 deaths on study. IDR may therefore represent a reasonable treatment option for patients with previously treated WM.
Current evidence shows that CXCR4 mutations impact disease presentation in WM, as well as time to response, depth of response, and DOR in patients with WM treated with BTK inhibitors.28 Our results are consistent with prior studies associating CXCR4 mutations with higher serum IgM levels and lower rates of extramedullary disease in patients with WM.29 Our study also suggests that CXCR4 mutations, especially nonsense mutations, associate with longer TTR and possibly TTMR to IDR. The depth of response to IDR is also adversely affected by CXCR4 mutations, especially attainment of VGPR. These aspects should therefore be considered when considering optimal treatment of patients with WM with CXCR4 mutations who require rapid and deep responses. However, despite longer TTR and lower rate of VGPR, median PFS, DOR, and TTNT were not affected by CXCR4 mutational status, consistent with prior reports with bortezomib and carfilzomib,4,12 supporting the use of IDR in CXCR4-mutated patients with WM in whom rapid disease control is not a priority.
In conclusion, we present the long-term follow-up of a prospective, phase II study of IDR as primary therapy for symptomatic patients with WM. On the basis of the findings of our study, IDR represents an easy-to-administer, safe, and effective treatment option for patients with WM, with high rates of durable responses and an excellent adverse event profile.
Acknowledgment
J.J.C. acknowledges the support of the WMR fund.
Footnotes
Portions of this research were presented at the Ninth International Workshop for Waldenström’s Macroglobulinemia, Amsterdam, The Netherlands, 7 October 2016; at the 58th annual meeting of the American Society of Hematology, San Diego, CA, 5 December 2016; and at the 59th annual meeting of the American Society of Hematology, Atlanta, GA, 11 December 2017.
Send data sharing requests to the corresponding author, Jorge J. Castillo (jorgej_castillo@dfci.harvard.edu).
Authorship
Contribution: J.J.C. and S.P.T. designed the study and performed the analysis; J.J.C. and K.M. collected patients’ data; J.C., M.G.D., M.L.G., A.K., X.L., M.M., N.T., C.J.P., G.Y., and Z.H. performed molecular testing in patients’ samples; J.J.C., C.A.F., and S.P.T. took care of the patients; J.J.C. drafted the manuscript; and all authors critically reviewed and approved the final manuscript.
Conflict-of-interest disclosure: J.J.C. has received honoraria and/or research funds from AbbVie, Beigene, Janssen, Kymera, Millennium, Pharmacyclics, and TG Therapeutics. S.P.T. has received research funding and/or consulting fees from BMS, Pharmacyclics, and Janssen. The remaining authors declare no competing financial interests.
Correspondence: Jorge J. Castillo, Bing Center for Waldenström Macroglobulinemia, Dana-Farber Cancer Institute, 450 Brookline Ave, Mayer 221, Boston, MA 02215; e-mail: jorgej_castillo@dfci.harvard.edu.
References
- 1.Dimopoulos MA, García-Sanz R, Gavriatopoulou M, et al. Primary therapy of Waldenstrom macroglobulinemia (WM) with weekly bortezomib, low-dose dexamethasone, and rituximab (BDR): long-term results of a phase 2 study of the European Myeloma Network (EMN). Blood. 2013;122(19):3276-3282. [DOI] [PubMed] [Google Scholar]
- 2.Ghobrial IM, Xie W, Padmanabhan S, et al. Phase II trial of weekly bortezomib in combination with rituximab in untreated patients with Waldenström macroglobulinemia. Am J Hematol. 2010;85(9):670-674. [DOI] [PubMed] [Google Scholar]
- 3.Treon SP, Ioakimidis L, Soumerai JD, et al. Primary therapy of Waldenström macroglobulinemia with bortezomib, dexamethasone, and rituximab: WMCTG clinical trial 05-180. J Clin Oncol. 2009;27(23):3830-3835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Treon SP, Tripsas CK, Meid K, et al. Carfilzomib, rituximab, and dexamethasone (CaRD) treatment offers a neuropathy-sparing approach for treating Waldenström’s macroglobulinemia. Blood. 2014;124(4):503-510. [DOI] [PubMed] [Google Scholar]
- 5.Waxman AJ, Clasen S, Hwang WT, et al. Carfilzomib-associated cardiovascular adverse events: a systematic review and meta-analysis. JAMA Oncol. 2018;4(3):e174519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hunter ZR, Xu L, Yang G, et al. The genomic landscape of Waldenstrom macroglobulinemia is characterized by highly recurring MYD88 and WHIM-like CXCR4 mutations, and small somatic deletions associated with B-cell lymphomagenesis. Blood. 2014;123(11):1637-1646. [DOI] [PubMed] [Google Scholar]
- 7.Castillo JJ, Xu L, Gustine JN, et al. CXCR4 mutation subtypes impact response and survival outcomes in patients with Waldenström macroglobulinaemia treated with ibrutinib. Br J Haematol. 2019;187(3):356-363. [DOI] [PubMed] [Google Scholar]
- 8.Treon SP, Gustine J, Meid K, et al. Ibrutinib monotherapy in symptomatic, treatment-naïve patients with Waldenström macroglobulinemia. J Clin Oncol. 2018;36(27):2755-2761. [DOI] [PubMed] [Google Scholar]
- 9.Treon SP, Tripsas CK, Meid K, et al. Ibrutinib in previously treated Waldenström’s macroglobulinemia. N Engl J Med. 2015;372(15):1430-1440. [DOI] [PubMed] [Google Scholar]
- 10.Roccaro AM, Sacco A, Jimenez C, et al. C1013G/CXCR4 acts as a driver mutation of tumor progression and modulator of drug resistance in lymphoplasmacytic lymphoma. Blood. 2014;123(26):4120-4131. [DOI] [PubMed] [Google Scholar]
- 11.Sklavenitis-Pistofidis R, Capelletti M, Liu CJ, et al. Bortezomib overcomes the negative impact of CXCR4 mutations on survival of Waldenstrom macroglobulinemia patients. Blood. 2018;132(24):2608-2612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Castillo JJ, Gustine JN, Meid K, et al. CXCR4 mutational status does not impact outcomes in patients with Waldenström macroglobulinemia treated with proteasome inhibitors [published online ahead of print 13 January 2020]. Am J Hematol. doi:10.1002/ajh.25730. [DOI] [PubMed] [Google Scholar]
- 13.Gustine JN, Xu L, Tsakmaklis N, et al. CXCR4S338X clonality is an important determinant of ibrutinib outcomes in patients with Waldenström macroglobulinemia. Blood Adv. 2019;3(19):2800-2803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cao Y, Hunter ZR, Liu X, et al. The WHIM-like CXCR4(S338X) somatic mutation activates AKT and ERK, and promotes resistance to ibrutinib and other agents used in the treatment of Waldenstrom’s Macroglobulinemia. Leukemia. 2015;29(1):169-176. [DOI] [PubMed] [Google Scholar]
- 15.Castillo JJ, Meid K, Gustine JN, et al. Prospective clinical trial of ixazomib, dexamethasone, and rituximab as primary therapy in Waldenström macroglobulinemia. Clin Cancer Res. 2018;24(14):3247-3252. [DOI] [PubMed] [Google Scholar]
- 16.Owen RG, Treon SP, Al-Katib A, et al. Clinicopathological definition of Waldenstrom’s macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom’s Macroglobulinemia. Semin Oncol. 2003;30(2):110-115. [DOI] [PubMed] [Google Scholar]
- 17.Kyle RA, Treon SP, Alexanian R, et al. Prognostic markers and criteria to initiate therapy in Waldenstrom’s macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom’s Macroglobulinemia. Semin Oncol. 2003;30(2):116-120. [DOI] [PubMed] [Google Scholar]
- 18.Treon SP, Xu L, Yang G, et al. MYD88 L265P somatic mutation in Waldenström’s macroglobulinemia. N Engl J Med. 2012;367(9):826-833. [DOI] [PubMed] [Google Scholar]
- 19.Kluk MJ, Lindsley RC, Aster JC, et al. Validation and implementation of a custom next-generation sequencing clinical assay for hematologic malignancies. J Mol Diagn. 2016;18(4):507-515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kimby E, Treon SP, Anagnostopoulos A, et al. Update on recommendations for assessing response from the Third International Workshop on Waldenstrom’s Macroglobulinemia. Clin Lymphoma Myeloma. 2006;6(5):380-383. [DOI] [PubMed] [Google Scholar]
- 21.Common Terminology Criteria for Adverse Events (CTCAE). Version 4.03. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf. Accessed 21 March 2020.
- 22.Olszewski AJ, Treon SP, Castillo JJ. Evolution of management and outcomes in Waldenström macroglobulinemia: a population-based analysis. Oncologist. 2016;21(11):1377-1386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Buske C, Sadullah S, Kastritis E, et al. ; European Consortium for Waldenström’s Macroglobulinemia . Treatment and outcome patterns in European patients with Waldenström’s macroglobulinaemia: a large, observational, retrospective chart review. Lancet Haematol. 2018;5(7):e299-e309. [DOI] [PubMed] [Google Scholar]
- 24.Kumar SK, Berdeja JG, Niesvizky R, et al. Safety and tolerability of ixazomib, an oral proteasome inhibitor, in combination with lenalidomide and dexamethasone in patients with previously untreated multiple myeloma: an open-label phase 1/2 study. Lancet Oncol. 2014;15(13):1503-1512. [DOI] [PubMed] [Google Scholar]
- 25.Kumar SK, LaPlant BR, Reeder CB, et al. Randomized phase 2 trial of ixazomib and dexamethasone in relapsed multiple myeloma not refractory to bortezomib. Blood. 2016;128(20):2415-2422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kastritis E, Dimopoulos MA. Disease control should be the goal of therapy for WM patients. Blood Adv. 2017;1(25):2483-2485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kersten MJ, Minnema MC, Vos JM, Nasserinejad K, Kap M, Kastritis E, et al. Ixazomib, rituximab and dexamethasone (IRD) in patients with relapsed or progressive Waldenstrom’s macroblobulinemia: results of the prospective phase I/II HOVON 124/Ecwm-R2 trial [abstract]. Blood. 2019;134(suppl 1):Abstract 344. [Google Scholar]
- 28.Castillo JJ, Moreno DF, Arbelaez MI, Hunter ZR, Treon SP. CXCR4 mutations affect presentation and outcomes in patients with Waldenström macroglobulinemia: a systematic review. Expert Rev Hematol. 2019;12(10):873-881. [DOI] [PubMed] [Google Scholar]
- 29.Treon SP, Cao Y, Xu L, Yang G, Liu X, Hunter ZR. Somatic mutations in MYD88 and CXCR4 are determinants of clinical presentation and overall survival in Waldenstrom macroglobulinemia. Blood. 2014;123(18):2791-2796. [DOI] [PubMed] [Google Scholar]