

Abstract
Background:
Laser interstitial thermal therapy (LITT) is a minimally invasive surgical treatment for multiple intracranial pathologies that are of growing interest to neurosurgeons and their patients and is emerging as an effective alternative to standard of care open surgery in the neurosurgical armamentarium. This option was initially considered for those patients with medical comorbidities and lesion-specific characteristics that confer excessively high risk for resection through a standard craniotomy approach but indications are changing.
Methods:
The PubMed database was searched for studies in the English literature on LITT for the treatment of primary and metastatic brain tumors, meningiomas, as well as for radiation necrosis (RN) in previously irradiated brain tumors.
Results:
This review provides an update of the relevant literature regarding application of LITT in neurosurgical oncology for the treatment of de novo and recurrent primary gliomas and brain metastases radiographically regrowing after previous irradiation as recurrent tumor or RN. In addition, this review details the limited experience of LITT with meningiomas and symptomatic peritumoral edema after radiosurgery. The advantages and disadvantages, indications, and comparisons to standard of care treatments such as craniotomy for open surgical resection are discussed for each pathology. Finally, the literature on cost-benefit analyses for LITT are reviewed.
Conclusion:
The studies discussed in this review have helped define the role of LITT in neurosurgical oncology and delineate optimal patient selection and tumor characteristics most suitable to this intervention.
Keywords: Brain metastasis, Craniotomy, Glioma, Laser interstitial thermal therapy, Meningioma, Radiation necrosis

INTRODUCTION
With the almost universal availability of Stereotaxis and increasing availability of magnetic resonance imaging (MRI) guidance in surgery, laser interstitial thermal therapy (LITT) has emerged as a popular alternative to standard of care open surgery in the neurosurgical armamentarium, particularly for the management of lesions where access through craniotomy might confer higher morbidity. Laser therapy is based on the delivery of nonionizing radiation as light into targeted tissues which transforms into heat that diffuses out through the tissues causing cellular thermal damage and coagulative necrosis. For LITT in tumors, higher levels of proteins and hemoglobin within the tumor facilitate light absorption compared with water in the surrounding edematous tissue and therefore facilitate preferential heating of the tumor. While thermal ablation has been used for decades to treat tumor, what has revolutionized the field is the ability to monitor tissue temperature change using MR thermometry and then calculate an estimated cell damage zone based on computational estimates of amount of heat delivered overtime to any particular voxel of tissue to control extent of ablation.[20]
This work reviews the relevant literature regarding application of MRI-guided LITT (MRgLITT) in neurosurgical oncology for the treatment of de novo and recurrent primary gliomas and brain metastases regrowing after previous irradiation as recurrent tumor or radiation necrosis (RN). The limited literature on MRgLITT for meningioma and symptomatic peritumoral edema is also reviewed. The advantages, disadvantages, and considerations for MRgLITT over open surgical resection are presented for both high-grade gliomas (HGGs) [Figure 1] and recurrent lesions after prior radiosurgery [Figure 2]. In addition, clinical outcomes and cost-benefit analysis between MRgLITT and standard of care craniotomy are discussed.
Figure 1:

Summary of application for laser interstitial thermal therapy in high-grade glioma.
Figure 2:

Summary of application for laser interstitial thermal therapy in recurrent lesions after prior radiosurgery.
MRGLITT FOR MALIGNANT TUMORS
Recurrent gliomas
Treatment of HGG remains one of the greatest challenges of neurosurgical oncology. The goal of initial neurosurgical management remains to confer maximal cytoreduction while minimizing morbidity to the patient.[12,33] However, at the time of inevitable tumor recurrence, surgical options can be limited and diminishing advantages of further cytoreduction need to weighed against the morbidity of reoperation with craniotomy. In this age of precision, medicine, however, obtaining a sample of the recurrent tumor may help with developing further treatment options. As such, under circumstances where repeat craniotomy seems less ideal, MRgLITT has become a reasonable alternative.
The first report of MRgLITT in recurrent HGG after prior gross total resection and chemoradiation demonstrated a median local progression-free survival (PFS) of 8 months in a series of 4 patients.[7] Subsequently, several other retrospective studies reported similar results.[13,19,26,28] These data prompted the first prospective Phase 1 clinical trial for MRgLITT in patients for recurrent HGG,[36] in which median OS of the 10 treated patients (mean tumor volume 6.8 cm3) was 10.2 months, comparing favorably to previously reported craniotomy results for recurrent HGG.[3] This was despite only 78% of the tumor volume being ablated, which was in part related to being limited to a single probe trajectory due to FDA-mandated trial design. The obvious question that arises then is whether or not increasing extent of ablation might improve outcome. To investigate this, Mohammadi et al. conducted a multicenter study of 34 patients who underwent MRgLITT for HGG, which included 15 patients with recurrent HGG.,[26] For the cases, in which tumor volume was almost completely ablated (≥91%), PFS was significantly improved compared to incomplete ablation (9.7 vs. 4.6 months, respectively). In the largest single institution experience of MRgLITT in glioma patients, in which tumor volumes were also nearly completely ablated (≥88%), Kamath et al. reported median PFS and OS of 7.7 months and 11.8 months, respectively, for patients with recurrent GBM. Taken together, these studies suggest that PFS and OS after MRgLITT for recurrent HGG may compare similarly to meta-analysis data of open surgical resection (median PFS of 5.6–11.2 months and OS of 4.7–11.4).[25] Furthermore, survival outcomes after MRgLITT may be superior to previously cited PFS and OS for patients with recurrent HGG treated with first-line bevacizumab therapy of 4.2 months and 9.1 months, respectively.[41]
One of the advantages of MRgLITT is its minimally invasive approach. In a recent publication looking at outcome, 83.2% of patients were able to be discharged home after hospital stay of a mean of only 33.8 h and with a only 1.5% rate of serious adverse events or repeat hospitalization within 30 days of the procedure.[22] Longest length of hospital stay in this same study, however, was 29 days. Studies have shown that LITT treatment of deep-seated gliomas led to longer intensive care unit stays for delayed neurological recovery.[13] In addition, larger tumors (60–70 cm3) may be at greater risk for developing malignant edema after MRgLITT, requiring hemicraniectomy.[19,28] While postoperative complication rates have been reported in some series to be as high as 20% of treated patients, the majority of these reflect mild- moderate neurological changes exacerbated by thermal ablation and resolved with conservative management.[26,28] Morbidity and mortality rates have also decreased over time with increased experience using LITT.[35] An example of this is the use of preoperative diffusion tensor imaging with white matter fiber tracking (DTI-FT) in avoiding postoperative motor deficits.[19,28,36]
Case illustration
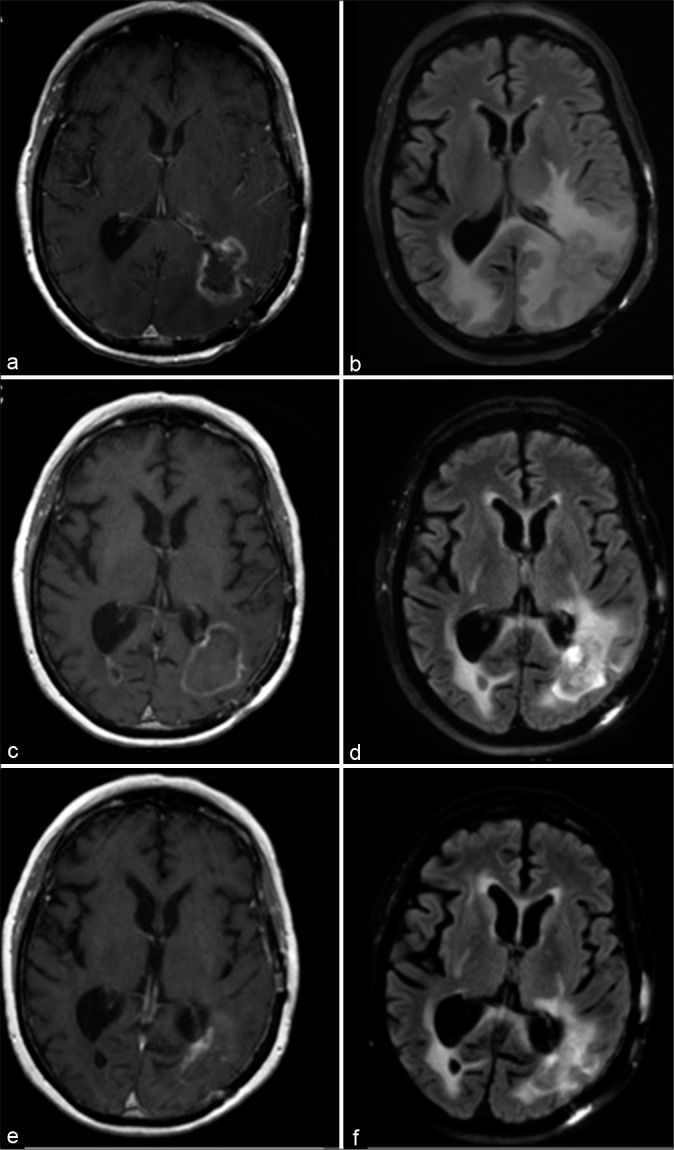
A 65-year-old male was referred to our institution with a prior history of a multifocal glioblastoma with lesions in the left posterior temporoparietal region and a second focus in the left hippocampus, the former of which was resected at an outside institution and subsequently treated with adjuvant temozolomide and radiation. His postoperative course was complicated by speech difficulties secondary to new-onset seizures that were mostly controlled with anticonvulsant therapy, as well as bowel perforation requiring colostomy and deep venous thrombosis, secondary to systemic therapy. At the time of referral, there was radiographic evidence of lesion regrowth at the site of hippocampal disease, concerning for tumor recurrence versus pseudo-progression [Figure 3a and b]. Given multiple medical complications since initial craniotomy including persistent speech and cognitive deficits, LITT was chosen for both diagnostic biopsy and minimally invasive thermal ablation of the lesion. The patient underwent LITT uneventfully with complete thermal coverage of the lesion, and intraoperative biopsy confirmed recurrent HGG. Postoperative MRI obtained at 2 weeks after LITT showed mildly increased size of the enhancing lesion but similarly decreased size of associated edema [Figure 3c and d], and the patient was otherwise at baseline speech difficulty off steroids. At 2-month follow-up, changes were more evident with stable to mildly decreased size of the enhancing lesion but more pronounced reduction of perilesional edema [Figure 3e and f]. Ultimately, at 6-month follow-up, there was radiographic evidence of tumor recurrence, and the patient eventually expired due to disease progression.
Figure 3:

Clinical imaging for case illustration of recurrent glioblastoma. Preoperative (a) T1-weighted postcontrast and (b) T2- weighted FLAIR magnetic resonance imaging (MRI) demonstrating an enhancing lesion in the left medial temporal region with surrounding edema. Imaging obtained 2 weeks after laser interstitial thermal therapy (LITT) showed a (c) mildly increased size of the enhancing lesion and (d) mild reduction of perilesional edema. An MRI obtained 2 months after LITT demonstrated more definitive (e) reduction in size of the enhancing lesion and (f) further diminishment of edema.
De novo gliomas
Typically, patients with HGG who were either medically unfit for surgery or harbored tumors in surgically inaccessible areas underwent biopsy, followed by standard chemoradiation, resulting in poorer survival outcomes than those undergoing maximal surgical resection.[27] Historical data by Stupp et al. of patients who underwent biopsy only followed by chemoradiation exhibited median survival of 9.4 months,[38] which is consistent with more recent meta-analysis data showing median survival of 9.2 months.[23] Ivan et al. performed a meta-analysis,[18] comprised 25 total patients from three LITT series,[13,19,26] as well as their own unpublished data and reported a median PFS of 5.1 months and an improved OS of 14.2 months. In their series, mean targeted tumor volume was 16.5 cm3 and average extent of ablation was 82.9%.
In contrast, Kamath et al. in their single institution experienced with MRgLITT for gliomas, reported no significant improvement in outcome after LITT with median PFS and OS of 5.9 months and 11.4 months, respectively, for the treatment of de novo gliomas.[21] Further, in a multi-institutional retrospective study, Mohammadi et al. compared MRgLITT to matched biopsy-only patients, both followed by chemoradiation.[27] Overall, median PFS and OS were again not found to be different between MRgLITT and biopsy cohorts (4.3 months and 14.4 months vs. 5.9 months and 15.8 months, respectively).
Based on these limited data, it remains unclear if MRgLITT offers an advantage over biopsy alone in patients with HGG not amenable to open surgery.
Craniotomy versus MRgLITT for gliomas
The ability to compare MRgLITT to standard craniotomy for both recurrent and de novo HGG is limited by a lack of well-designed studies. Barnett et al. performed a systematic review and meta-analysis of outcomes after MRgLITT or craniotomy for gliomas specifically near eloquent areas of the brain.[4] The authors identified 8 MRgLITT studies totaling 77 patients comprised 51 recurrent gliomas and 24 de novo gliomas, and 11 craniotomy studies totaling 1036 patients, comprised 198 recurrent gliomas and 699 de novo gliomas. Patients who underwent MRgLITT tended to be older (54.3 vs. 45.6 years), had lower preoperative KPS (73.4 vs. 78.4), and were being treated for recurrent gliomas rather than upfront treatment (51/75, 68% vs. 198/897, 22%). There were significantly lower rates of major complications in MRgLITT (5.7%) versus craniotomy (13.9%) with 10% absolute risk reduction. Mean extent of resection for MRgLITT was 85.4% which was significantly better than 77% for craniotomy and compared favorably to previous data analyzing use of intraoperative stimulation brain mapping.[10] Although definitive conclusions were limited by the disproportionately greater number of craniotomy versus limited MRgLITT cases, these data demonstrated that MRgLITT could be a reasonable alternative for patients with glioma undergoing consideration for surgical management of tumors involving eloquent brain matter.
Taken together, MRgLITT may be a viable option for patients with recurrent or de novo HGG who may not be amenable to standard surgical resection and results of LITT may compare favorably to standard medical management with bevacizumab. More appropriate patients may be those of older age, with lower preoperative performance status, and/ or existing medical comorbidities, all of whom may benefit from the minimally invasive nature of LITT with shorter associated hospitalization stays. On the other hand, larger tumors over 60–70cm3 may be unfavorable for MRgLITT due to the potential need for mass decompression, secondary to expected immediate postoperative swelling that occurs in the lesion after LITT. In addition, for tumors near eloquent white matter fiber tracts, use of preoperative DTI may help avoid inadvertent thermal ablation of these tracts and prevent permanent postoperative neurological deficits.
MRGLITT FOR RECURRENT LESIONS AFTER PRIOR SRS TO BRAIN METASTASES
With increasing survival of patients with systemic cancers, local control of brain metastases is becoming more problematic than ever before. In the modern era, brain metastases are managed through a multimodality approach through surgery, adjuvant, and/or upfront radiation therapy with whole brain radiation (WBRT) or stereotactic radiosurgery (SRS) and often novel systemic agents. It is now well recognized that with survival greater than 1 year after brain metastasis treatment, SRS-treated lesions may regrow radiographically due to recurrent tumor, RN, or both. In those who are eligible and willing, surgical management has been an effective salvage treatment. However, in patients unable or unwilling to undergo open surgery, MRgLITT has been proposed as an alternative surgical option.
Recurrent tumors
Carpentier et al. were the first to describe an early pilot clinical trial of 7 patients with 15 total lesions for MRgLITT in regrowing lesions after SRS.[8] While there was no differentiation between recurrent tumor and RN, they were able to report median PFS of 6 and 15 months for partially and fully ablated lesions, respectively, and an OS of 18.4 months. Several other LITT studies have reported comparable 6-month PFS rates of 75.8%,[32,39] including a large series of 59 patients exhibiting local control rates of 83.1% at median follow-up of 11 months.[14] Kamath et al. differentiated between recurrent tumor and RN by intraoperative biopsy at time of MRgLITT.[21] Among the 25 patients treated for tumor progression, the average volume was 7.88 cm3 with 94% ablation achieved. Median PFS was not reached at median follow-up of 9.8 months while median OS was 17.2 months, mostly secondary to systemic disease progression. Further improvement in outcome was described by Ali et al. who reported superior PFS in cases where over 80% of thermal ablation was achieved and adjuvant hypofractionated SRS was used post-LITT for sustained local control of incompletely ablated tumors.[2]
In 2018, results were reported from laser ablation after stereotactic radiosurgery (LAASR), a multicenter prospective Phase 2 clinical trial of MRgLITT in patients with radiographic progression after SRS for brain metastases,[1] which included 20 patients with recurrent tumor diagnosed by intraoperative biopsy. In these patients, the 3-month PFS rate was 54% while 3-month OS rate was 71%. Notably, only four patients achieved total ablation of their lesion, likely accounting for the lower PFS, but none of these patients exhibited progressive disease at time of last follow-up of 6.5 months.
RN
In contrast to recurrent tumor, the most compelling evidence for the role and efficacy of MRgLITT has been in the treatment of RN after prior SRS to brain metastases. Early case studies of biopsy-proven RN treated with MRgLITT demonstrated the ability to rapidly wean steroids and improve neurological symptoms.[29,39] Subsequently, larger series of MRgLITT for biopsy-confirmed RN by Smith et al.[37] and Rammo et al.[30] demonstrated encouraging outcomes with reported median PFS of 11.4 months and 6-month survival rates of 77.8%, respectively. Chaunzwa et al. reported the first multicenter retrospective study encompassing 30 patients across four institutions, treated with MRgLITT following SRS failure, of which 19 patients had biopsy-proven RN.[9] Although reported outcomes were not subdivided by pathology of the lesion, MRgLITT was effective in rapid steroid weaning in nearly 75% of patients, while providing symptom relief in 48% of patients with a median time to improvement of symptom resolution being 2 weeks. Shortly afterward, the LAASR prospective study demonstrated significantly better outcomes in its cohort of 19 patients with biopsy-proven RN, with 91% PFS and 82.1% OS rates at last follow-up (6.5 months).[1] In addition, despite having had a surgical intervention, no significant changes in median KPS, quality of life metrics, and neurocognitive testing were seen over the duration of survival after MRgLITT. Similar durable local control was reported in a recent large single institution series of 31 patients undergoing MRgLITT for RN, in which PFS rates persisted over 75% at 24 months.[5] Similar to LAASR, pathology of the lesion and extent of ablation were significantly associated with improved local control.
Separate from local control, MRgLITT has also proven to be effective for alleviating perilesional edema associated with RN. In their case series of 10 patients with RN, Rammo et al. performed volumetric analyses on T1-weighted postcontrast imaging and found that immediate postoperative lesion volumes increased 220%, further increasing to 430% by 1–2 weeks[30] and only decreased to 69% of initial preoperative values beyond 6-month postoperatively. Despite the radiographic enlargement of the enhancing size of the lesion initially, 7 of the 10 patients were able to be successfully weaned off of steroids within 2 weeks after ablation. Many other studies have demonstrated similar increases in enhancing lesion size after MRgLITT, typically taking months to demonstrate radiographic resolution.[6,32,39] In contrast, perilesional FLAIR volumes seemed to respond earlier to ablation with significant reductions seen as early as 2 weeks after ablation that likely explains the ability to rapidly taper steroids despite increasing enhancing lesion size in the months after MRgLITT.[39] In their multicenter retrospective study, Chaunzwa et al. reported decreased FLAIR volume at 6 weeks post-MRgLITT with further reductions that extended to 6 months.[9] Not surprisingly, larger reductions in FLAIR edema were significantly associated with increased ability to stop steroids after MRgLITT.
Craniotomy versus MRgLITT for metastatic recurrence and RN
In a recent single-institution retrospective review by Hong et al., 75 patients with lesions regrowing after SRS were compared. Forty-two patients had biopsy-proven tumor and 26 had undergone craniotomy versus 16 how were treated with LITT. The remaining 33 patients had RN – 15 underwent craniotomy versus 18 treated with LITT. Overall, craniotomy was shown to be more effective for providing relief of preoperative neurological symptoms but a larger number of the craniotomy patients with symptoms had lesions >3 cm diameter. Subset analysis of patient with tumors <3 cm in diameter eliminated the symptom relief advantage of craniotomy and further exhibited equivalent 12-month PFS rates (72.2% for LITT vs. 61.1% for craniotomy) and 12-month OS rates (69.0% vs. 69.3%). Further, no difference was found between the two groups with regard to ability to wean off steroids (35% for LITT vs. 47% for craniotomy).
While MRgLITT compares favorably to standard of care craniotomy for the treatment of recurrent brain metastases after prior SRS for lesions <3 cm, what became evident was that pathology of the lesion contributed more significantly to survival outcomes than surgical method. Patients with RN treated with LITT had 12 month PFS of 87.8% and OS of 73.8% not significantly different from patients with RN treated with craniotomy who had 12-month PFS of 86.7% and OS of 93.3%. However, these rates were significantly greater than those seen in patients with tumor, regardless of treatment modality. Patients with tumor treated with LITT had 12-month PFS of 54.7% and OS of 62.5%, statistically similar to patients with tumor treated with craniotomy who had 12-month PFS of 44.4% and OS of 54.3%.[16]
Taken together, while craniotomy remains better for the management of larger lesions, MRgLITT may be a viable equivalent alternative in patients with lesions with diameters <3 cm, particularly given its effectiveness in the treatment of RN.
Case illustration
A 60-year-old male with known metastatic nonsmall cell lung cancer underwent surgical resection of a symptomatic left parieto-occipital metastasis followed by consolidative SRS for symptomatic speech difficulty and hemiparesis. Three months later, he underwent additional SRS to a right occipital lesion found on surveillance imaging. Due to lesion regrowth at the site of prior surgery and new dural lesions in the left parietal region, he was treated with whole brain radiation therapy 8 months after initial resection. Nineteen months after surgery, he developed worsening speech comprehension and confusion in the context of regrowing lesions in both parieto-occipital lobes, more radiographically pronounced and symptomatic from the left side, and an inability to be tapered off of steroids [Figure 4a and b]. Given his history of prior craniotomy in the same region, he underwent LITT of the symptomatic left-sided regrowing lesion with intraoperative biopsy demonstrating no viable tumor, consistent with RN pathology. MRI obtained 1 month after LITT showed mildly increased size of the enhancing lesion but definite decreased perilesional edema, and the patient demonstrated clinical improvement in speech comprehension [Figure 4c and d]. Surveillance imaging obtained over 1 year after LITT revealed further decreases in edema and reduction in the size of the enhancing lesion [Figure 4e and f].
Figure 4:
Clinical imaging for case illustration of radiation necrosis. Preoperative (a) T1-weighted postcontrast and (b) T2- weighted FLAIR magnetic resonance imaging (MRI) demonstrating an enhancing lesion in the left parieto-occipital region with surrounding edema. Imaging obtained 1 month after laser interstitial thermal therapy (LITT) showed a (c) mildly increased size of the enhancing lesion but (d) reduction of perilesional edema. An MRI obtained 1 year after LITT demonstrated (e) drastic reduction in size of the enhancing lesion and (f) further diminishment of edema.
MRGLITT FOR MENINGIOMA
Meningiomas remain one of the most common primary brain tumors and differ from gliomas and brain metastases by nature of their extra-axial location and typically benign pathology. Surgical resection has remained first-line treatment with radiosurgery reserved for cases of refractory occurrence not amenable to further surgery or higher grade lesions that cannot be totally resected. As such, experience with MRgLITT for meningioma pathology is limited. Ivan et al. reported a case series of five patients treated with MRgLITT at their institution for recurrent radiographically progressing dural-based lesions, comprised three WHO I meningiomas, one WHO III meningioma, as well as a solitary fibrous tumor.[17] All patients were deemed poor candidates for open surgery, given prior histories of multiple craniotomies and multiple treatments with radiotherapy. MRgLITT was well tolerated with no worsening of symptoms and patients were neurologically stable at last follow-up. All patients with WHO Grade I meningiomas demonstrated durable decrease in tumor size, persisting to last follow-up of 8–24 months after ablation, while the case of WHO III meningioma had early recurrence at 2 months. More recently, Rammo et al. reported a case series of three patients, comprised two WHO III meningiomas and one of indeterminate grade.[31] Indications for MRgLITT were again failure of prior resection and maximal radiation although one patient elected for laser ablation after failure of prior surgery alone. One patient experienced acute hemiparesis and dysphasia secondary to edema in the adjacent motor strip that improved to baseline after 6 months. Similar to findings by Ivan et al., the two cases of WHO III meningioma experienced progression within 3 months after MRgLITT while the case of indeterminate grade did not have progression at last follow-up of 28 months.
Symptomatic peritumoral edema (PTE) is a known complication after SRS for meningiomas that may occur in 5–10% of cases.[11,34] Whether its development after SRS is due to tumor progression or postradiation changes in the surrounding irradiated brain remains unclear, but typically these cases have been managed like RN with high-dose steroids as first-line therapy. When this fails, further options are limited, particularly for patients where further surgery carries high risk. In the studies by Rammo et al. and Ivan et al. on MRgLITT for meningiomas, the patients at time of ablation were either asymptomatic or experiencing mild symptoms (i.e., headache), were not dependent on high-dose steroids, and exhibited excellent KPS of 90–100.[17,31] In contrast, a recent report described successful use of MRgLITT for symptomatic PTE in a patient with a regrowing lesion that had undergone previous maximal radiation and multiple surgeries for WHO Grade I meningioma.[15] While intraoperative biopsy demonstrated viable tumor, laser ablation resulted in significant reduction in enhancing lesion size and surrounding edema at 6-week follow-up, accompanied by successful weaning off of steroids and resolution of hemiparesis and dysphasia. Durable local control, comprised minimal nodular enhancement and absence of edema, was noted at last follow-up 3 years after treatment.
While the first-line therapies for meningiomas remain surgical resection through craniotomy and radiotherapy for select cases of residual or higher grade tumors, MRgLITT may be an option for patients who demonstrate lesional regrowth and have exhausted further surgical or radiation options. Based on the limited experience reported in the literature, laser ablation may be more optimal for providing local control in radiographically progressing WHO Grade I tumors, as opposed to higher grades. Likewise, MRgLITT may be efficacious in alleviating symptomatic PTE in cases treated with prior SRS that is not amenable to further surgery. Further studies describing experience with MRgLITT for meningiomas are needed to better determine indications and expected outcomes in these patients.
SOCIOECONOMIC COMPARISON BETWEEN MRGLITT AND CRANIOTOMY
All examinations of novel technology need to take into account cost comparisons with standard of care. Leuthardt et al. analyzed acute care costs for MRgLITT and craniotomy at their institution for both primary and metastatic brain tumors involving difficult to access areas or eloquent brain matter.[24] Twenty-seven patients treated with MRgLITT (19 with gliomas and 8 with metastases) were compared to 340 patients treated with craniotomy (248 with gliomas and 92 with metastases). Overall, for gliomas and metastases combined, they found no significant differences overall in acute and postcare costs for MRgLITT versus craniotomy. Interestingly, when analyzed by tumor type, however, they did find significantly less costs with MRgLITT for the management of metastatic disease compared to craniotomy, related to shorter hospital length of stay and higher likelihood of being discharged home rather than to a center for rehabilitation therapy. While there were no differences in incidence of 30-day readmissions in the overall cohort, among patients with metastatic disease, readmissions were statistically more frequent in patients treated with craniotomy adding on average $3400 per patient. This study suggests that MRgLITT at the very least is economically comparable to craniotomy for the treatment of primary and metastatic disease in patients with difficult to access or eloquent cortex involving tumors.
Voigt and Barnett likewise analyzed cost-effectiveness of MRgLITT in 75 patients compared to standard open resection or biopsy only in 890 patients with HGG for whom maximal surgical resection was not feasible.[40] They reported an increased cost of $7508 per patient for an additional survival of 3.07 months in patients undergoing MRgLITT compared with subtotal resection through craniotomy or biopsy only. Baseline costs for MRgLITT were $89,839 for an OS of 19.04 months, compared to $82,331 for all other treatments (craniotomy or biopsy) for an OS of 15.86 months. This amounted to an additional $2445 of cost incurred for every month in survival gained. The authors also analyzed costs per year of life gained (LYG) and determined that MRgLITT costs $8458/LYG more compared to craniotomy and $48,552/LYG more compared to biopsy only, but the cost of MRgLITT still falls below the current US threshold value of $50,000/LYG for what is considered cost-effective health-care intervention (although it exceeds the $32,575/LYG threshold internationally). Balancing the higher costs of MRgLITT was the finding that MRgLITT resulted in a higher likelihood of good KPS (>70) postoperatively: 36% of cases with OS 22.58 months compared to only 8–9% for craniotomy with OS 21.75–25.05 months, that is, a 4 times higher likelihood of good functional outcome after MRgLITT compared to open surgical resection. While it is hard to place a dollar value on improved functionality, this study suggests that within the US, MRgLITT may be an acceptable albeit more expensive option for cases of HGG in which maximal surgical resection is not feasible.
The literature on the economic value of MRgLITT remains scarce and further studies may benefit from analysis of specific populations such as the elderly or those with multiple medical comorbidities for whom open surgery may otherwise drive up costs, secondary to longer hospitalization stays, and higher rates of perioperative complications requiring readmission. As evidence for the efficacy of MRgLITT continues to amount in the neurosurgical literature, further studies analyzing its economic value are expected to clarify the circumstances in which MRgLITT may be most cost- effective over standard treatments.
CONCLUSION
MRgLITT continues to grow in popularity as a minimally- invasive alternative to standard of care open surgical resection in neuro-oncology. This review shows that there is growing interest in its use in the treatment of HGG as both upfront therapy and for recurrent tumors, particularly in select patients who may otherwise not be fit for maximal surgical resection. Furthermore, MRgLITT may lead to more favorable outcomes in patients who otherwise are deemed only a surgical candidate for biopsy alone. For patients with recurring lesions after prior radiosurgery to brain metastases, MRgLITT may be an equally efficacious treatment for recurrent tumors as well as for RN after SRS in regard to both patient outcomes and cost-effectiveness. In particular, MRgLITT may confer rapid reductions in perilesional edema and steroid cessation in RN pathology. Preliminary experience with MRgLITT in meningiomas has also suggested a role for its use in recurrent tumors and symptomatic PTE, otherwise not amenable to repeat resection or further radiation. As the use of MRgLITT continues to become more commonplace across institutions, larger studies and clinical trials are expected to determine standardized protocols and indications for MRgLITT in neurosurgical oncology.
Footnotes
How to cite this article: Hong CS, Kundishora AJ, Elsamadicy AA, Chiang VL. Laser interstitial thermal therapy in neuro-oncology applications. Surg Neurol Int 2020;11:231.
Contributor Information
Christopher S. Hong, Email: christopher.hong@yale.edu.
Adam J. Kundishora, Email: adam.kundishora@yale.edu.
Aladine A. Elsamadicy, Email: aladine.elsamadicy@yale.edu.
Veronica L. Chiang, Email: veronica.chiang@yale.edu.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Chiang is a consultant for Monteris Medical Inc. (Minnesota, USA) and speaker for BrainLab, Inc. (Munich, Germany).
REFERENCES
- 1.Ahluwalia M, Barnett GH, Deng D, Tatter SB, Laxton AW, Mohammadi AM, et al. Laser ablation after stereotactic radiosurgery: A multicenter prospective study in patients with metastatic brain tumors and radiation necrosis. J Neurosurg. 2018;130:804–11. doi: 10.3171/2017.11.JNS171273. [DOI] [PubMed] [Google Scholar]
- 2.Ali MA, Carroll KT, Rennert RC, Hamelin T, Chang L, Lemkuil BP, et al. Stereotactic laser ablation as treatment for brain metastases that recur after stereotactic radiosurgery: A multiinstitutional experience. Neurosurg Focus. 2016;41:E11. doi: 10.3171/2016.7.FOCUS16227. [DOI] [PubMed] [Google Scholar]
- 3.Barker FG, 2nd, Chang SM, Gutin PH, Malec MK, McDermott MW, Prados MD, et al. Survival and functional status after resection of recurrent glioblastoma multiforme. Neurosurgery. 1998;42:709–20. doi: 10.1097/00006123-199804000-00013. discussion 720-3. [DOI] [PubMed] [Google Scholar]
- 4.Barnett GH, Voigt JD, Alhuwalia MS. A systematic review and meta-analysis of studies examining the use of brain laser interstitial thermal therapy versus craniotomy for the treatment of high-grade tumors in or near areas of eloquence: An examination of the extent of resection and major complication rates associated with each type of surgery. Stereotact Funct Neurosurg. 2016;94:164–73. doi: 10.1159/000446247. [DOI] [PubMed] [Google Scholar]
- 5.Bastos DC, Rao G, Oliva IC, Loree JM, Fuentes DT, Stafford RJ, et al. Predictors of local control of brain metastasis treated with laser interstitial thermal therapy. Neurosurgery. 2020;87:112–22. doi: 10.1093/neuros/nyz357. [DOI] [PubMed] [Google Scholar]
- 6.Beechar VB, Prabhu SS, Bastos D, Weinberg JS, Stafford RJ, Fuentes D, et al. Volumetric response of progressing post-SRS lesions treated with laser interstitial thermal therapy. J Neurooncol. 2018;137:57–65. doi: 10.1007/s11060-017-2694-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carpentier A, Chauvet D, Reina V, Beccaria K, Leclerq D, McNichols RJ, et al. MR-guided laser-induced thermal therapy (LITT) for recurrent glioblastomas. Lasers Surg Med. 2012;44:361–8. doi: 10.1002/lsm.22025. [DOI] [PubMed] [Google Scholar]
- 8.Carpentier A, McNichols RJ, Stafford RJ, Itzcovitz J, Guichard JP, Reizine D, et al. Real-time magnetic resonance-guided laser thermal therapy for focal metastatic brain tumors. Neurosurgery. 2008;63(Suppl 1):ONS21–8. doi: 10.1227/01.neu.0000335007.07381.df. discussion ONS28-9. [DOI] [PubMed] [Google Scholar]
- 9.Chaunzwa TL, Deng D, Leuthardt EC, Tatter SB, Mohammadi AM, Barnett GH, et al. Laser thermal ablation for metastases failing radiosurgery: A multicentered retrospective study. Neurosurgery. 2018;82:56–63. doi: 10.1093/neuros/nyx142. [DOI] [PubMed] [Google Scholar]
- 10.De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, Berger MS. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: A meta-analysis. J Clin Oncol. 2012;30:2559–65. doi: 10.1200/JCO.2011.38.4818. [DOI] [PubMed] [Google Scholar]
- 11.Fatima N, Meola A, Pollom E, Chaudhary N, Soltys S, Chang SD. Stereotactic radiosurgery in large intracranial meningiomas: A systematic review. World Neurosurg. 2019;129:269–75. doi: 10.1016/j.wneu.2019.06.064. [DOI] [PubMed] [Google Scholar]
- 12.Hardesty DA, Sanai N. The value of glioma extent of resection in the modern neurosurgical era. Front Neurol. 2012;3:140. doi: 10.3389/fneur.2012.00140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hawasli AH, Bagade S, Shimony JS, Miller-Thomas M, Leuthardt EC. Magnetic resonance imaging-guided focused laser interstitial thermal therapy for intracranial lesions: Single-institution series. Neurosurgery. 2013;73:1007–17. doi: 10.1227/NEU.0000000000000144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hernandez RN, Carminucci A, Patel P, Hargreaves EL, Danish SF. Magnetic resonance-guided laser-induced thermal therapy for the treatment of progressive enhancing inflammatory reactions following stereotactic radiosurgery, or PEIRs, for metastatic brain disease. Neurosurgery. 2019;85:84–90. doi: 10.1093/neuros/nyy220. [DOI] [PubMed] [Google Scholar]
- 15.Hong CS, Beckta JM, Kundishora AJ, Elsamadicy AA, Chiang VL. Laser interstitial thermotherapy for treatment of symptomatic peritumoral edema after radiosurgery for meningioma. World Neurosurg. 2020;136:295–300. doi: 10.1016/j.wneu.2020.01.143. [DOI] [PubMed] [Google Scholar]
- 16.Hong CS, Deng D, Vera A, Chiang VL. Laser-interstitial thermal therapy compared to craniotomy for treatment of radiation necrosis or recurrent tumor in brain metastases failing radiosurgery. J Neurooncol. 2019;142:309–17. doi: 10.1007/s11060-019-03097-z. [DOI] [PubMed] [Google Scholar]
- 17.Ivan ME, Diaz RJ, Berger MH, Basil GW, Osiason DA, Plate T, et al. Magnetic resonance-guided laser ablation for the treatment of recurrent dural-based lesions: A series of five cases. World Neurosurg. 2017;98:162–70. doi: 10.1016/j.wneu.2016.10.037. [DOI] [PubMed] [Google Scholar]
- 18.Ivan ME, Mohammadi AM, De Deugd N, Reyes J, Rodriguez G, Shah A, et al. Laser ablation of newly diagnosed malignant gliomas: A meta-analysis. Neurosurgery. 2016;79(Suppl 1):S17–23. doi: 10.1227/NEU.0000000000001446. [DOI] [PubMed] [Google Scholar]
- 19.Jethwa PR, Barrese JC, Gowda A, Shetty A, Danish SF. Magnetic resonance thermometry-guided laser-induced thermal therapy for intracranial neoplasms: Initial experience. Neurosurgery. 2012;71(Suppl 1):133–44. 144–5. doi: 10.1227/NEU.0b013e31826101d4. [DOI] [PubMed] [Google Scholar]
- 20.Jolesz FA, Talos IF, Schwartz RB, Mamata H, Kacher DF, Hynynen K, et al. Intraoperative magnetic resonance imaging and magnetic resonance imaging-guided therapy for brain tumors. Neuroimaging Clin N Am. 2002;12:665–83. doi: 10.1016/s1052-5149(02)00036-9. [DOI] [PubMed] [Google Scholar]
- 21.Kamath AA, Friedman DD, Hacker CD, Smyth MD, Limbrick DD, Jr, Kim AH, et al. MRI-guided interstitial laser ablation for intracranial lesions: A large single-institution experience of 133 Cases. Stereotact Funct Neurosurg. 2017;95:417–28. doi: 10.1159/000485387. [DOI] [PubMed] [Google Scholar]
- 22.Kim AH, Tatter S, Rao G, Prabhu S, Chen C, Fecci P, et al. Laser ablation of abnormal neurological tissue using robotic NeuroBlate system (LAANTERN): 12-Month outcomes and quality of life after brain tumor ablation. Neurosurgery. 2020:nyaa071. doi: 10.1093/neuros/nyaa071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kole AJ, Park HS, Yeboa DN, Rutter CE, Corso CD, Aneja S, et al. Concurrent chemoradiotherapy versus radiotherapy alone for biopsy-only glioblastoma multiforme. Cancer. 2016;122:2364–70. doi: 10.1002/cncr.30063. [DOI] [PubMed] [Google Scholar]
- 24.Leuthardt EC, Voigt J, Kim AH, Sylvester P. A single-center cost analysis of treating primary and metastatic brain cancers with either brain laser interstitial thermal therapy (LITT) or craniotomy. Pharmacoecon Open. 2017;1:53–63. doi: 10.1007/s41669-016-0003-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lu VM, Jue TR, McDonald KL, Rovin RA. The survival effect of repeat surgery at glioblastoma recurrence and its trend: A systematic review and meta-analysis. World Neurosurg. 2018;115:453–459.e3. doi: 10.1016/j.wneu.2018.04.016. [DOI] [PubMed] [Google Scholar]
- 26.Mohammadi AM, Hawasli AH, Rodriguez A, Schroeder JL, Laxton AW, Elson P, et al. The role of laser interstitial thermal therapy in enhancing progression-free survival of difficult-to-access high-grade gliomas: A multicenter study. Cancer Med. 2014;3:971–9. doi: 10.1002/cam4.266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mohammadi AM, Sharma M, Beaumont TL, Juarez KO, Kemeny H, Dechant C, et al. Upfront magnetic resonance imaging-guided stereotactic laser-ablation in newly diagnosed glioblastoma: A multicenter review of survival outcomes compared to a matched cohort of biopsy-only patients. Neurosurgery. 2019;85:762–72. doi: 10.1093/neuros/nyy449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Patel P, Patel NV, Danish SF. Intracranial MR-guided laser-induced thermal therapy: Single-center experience with the Visualase thermal therapy system. J Neurosurg. 2016;125:853–60. doi: 10.3171/2015.7.JNS15244. [DOI] [PubMed] [Google Scholar]
- 29.Rahmathulla G, Recinos PF, Valerio JE, Chao S, Barnett GH. Laser interstitial thermal therapy for focal cerebral radiation necrosis: A case report and literature review. Stereotact Funct Neurosurg. 2012;90:192–200. doi: 10.1159/000338251. [DOI] [PubMed] [Google Scholar]
- 30.Rammo R, Asmaro K, Schultz L, Scarpace L, Siddiqui S, Walbert T, et al. The safety of magnetic resonance imaging-guided laser interstitial thermal therapy for cerebral radiation necrosis. J Neurooncol. 2018;138:609–17. doi: 10.1007/s11060-018-2828-2. [DOI] [PubMed] [Google Scholar]
- 31.Rammo R, Scarpace L, Nagaraja T, Lee I. MR-guided laser interstitial thermal therapy in the treatment of recurrent intracranial meningiomas. Lasers Surg Med. 2019;51:245–50. doi: 10.1002/lsm.23045. [DOI] [PubMed] [Google Scholar]
- 32.Rao MS, Hargreaves EL, Khan AJ, Haffty BG, Danish SF. Magnetic resonance-guided laser ablation improves local control for postradiosurgery recurrence and/or radiation necrosis. Neurosurgery. 2014;74:658–67. doi: 10.1227/NEU.0000000000000332. discussion 667. [DOI] [PubMed] [Google Scholar]
- 33.Sanai N, Polley MY, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011;115:3–8. doi: 10.3171/2011.2.jns10998. [DOI] [PubMed] [Google Scholar]
- 34.Seo Y, Kim DG, Kim JW, Han JH, Chung HT, Paek SH. Long-term outcomes after gamma knife radiosurgery for benign meningioma: A single institution’s experience with 424 Patients. Neurosurgery. 2018;83:1040–9. doi: 10.1093/neuros/nyx585. [DOI] [PubMed] [Google Scholar]
- 35.Shao J, Radakovich NR, Grabowski M, Borghei-Razavi H, Knusel K, Joshi KC, et al. Lessons learned in using laser interstitial thermal therapy for treatment of brain tumors: A case series of 238 Patients from a single institution. World Neurosurg. 2020;139:e345–4. doi: 10.1016/j.wneu.2020.03.213. [DOI] [PubMed] [Google Scholar]
- 36.Sloan AE, Ahluwalia MS, Valerio-Pascua J, Manjila S, Torchia MG, Jones SE, et al. Results of the NeuroBlate system first-in-humans Phase I clinical trial for recurrent glioblastoma: Clinical article. J Neurosurg. 2013;118:1202–19. doi: 10.3171/2013.1.JNS1291. [DOI] [PubMed] [Google Scholar]
- 37.Smith CJ, Myers CS, Chapple KM, Smith KA. Long-term follow-up of 25 Cases of biopsy-proven radiation necrosis or post-radiation treatment effect treated with magnetic resonance-guided laser interstitial thermal therapy. Neurosurgery. 2016;79(Suppl 1):S59–72. doi: 10.1227/NEU.0000000000001438. [DOI] [PubMed] [Google Scholar]
- 38.Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96. doi: 10.1056/NEJMoa043330. [DOI] [PubMed] [Google Scholar]
- 39.Torres-Reveron J, Tomasiewicz HC, Shetty A, Amankulor NM, Chiang VL. Stereotactic laser induced thermotherapy (LITT): A novel treatment for brain lesions regrowing after radiosurgery. J Neurooncol. 2013;113:495–503. doi: 10.1007/s11060-013-1142-2. [DOI] [PubMed] [Google Scholar]
- 40.Voigt JD, Barnett G. The value of using a brain laser interstitial thermal therapy (LITT) system in patients presenting with high grade gliomas where maximal safe resection may not be feasible. Cost Eff Resour Alloc. 2016;14:6. doi: 10.1186/s12962-016-0055-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wick W, Gorlia T, Bendszus M, Taphoorn M, Sahm F, Harting I, et al. Lomustine and bevacizumab in progressive glioblastoma. N Engl J Med. 2017;377:1954–63. doi: 10.1056/NEJMoa1707358. [DOI] [PubMed] [Google Scholar]