

Abstract
Objectives
To explore the mechanisms of reduced suicide mortality in Japan, which decreased from 25.7 to 16.5 per 100 000 people following the comprehensive suicide prevention programme from 2009 to 2018, the present study determined the relationship between regional suicide mortality, socioeconomic data (GDP per capita, unemployment rates) and financial support for regional suicide prevention programmes.
Design and setting
Stepwise multiple regression analysis was used to determine the effects of regional GDP per capita, unemployment rates and implementation amount of financial support for regional suicide prevention programmes (Emergency Fund to Enhance Community-Based Suicide Countermeasures—EFECBSC) on age and gender disaggregated suicide mortalities in Japan between 2009 and 2018. Data on each prefecture’s complete unemployment rates, GDP per capita and implementation amount of EFECBSC sub-divisions were derived from an official Japanese governmental database.
Results
Both prefectural enlightenment and intervention model programmes were found to lead to a decrease in male suicide mortality, but were less effective in reducing female suicide mortality. Municipal enlightenment and intervention model programmes were also less effective in reducing suicide mortality. Municipal development programmes for listener and leader led to a greater decrease in suicide mortality for both men and women compared with such programmes at the prefectural level. Contrary to our expectations, reduced complete unemployment rate only reduced suicide mortality in the older male population without affecting female suicide mortality.
Conclusion
The study findings suggest an inverse relationship between financial support and suicide mortality in Japan. Furthermore, independent factors in the reduction of suicide mortality rates provide important information for planning evidence-based and cost-effective regional suicide prevention programmes.
Keywords: epidemiology, health economics, public health, suicide & self-harm
Strengths and limitations of this study.
To better inform public health policies, the effects of regional GDP per capita, regional unemployment rate and financial support for regional suicide prevention programmes on regional suicide mortality in Japan are analysed using stepwise multiple regression analysis.
Financial support for suicide prevention programmes and reduced unemployment rates were found to be related to reduced suicide mortality in the older male population in Japan, but GDP per capita did not seem to have an effect; additionally, financial support contributes to a greater reduction in male suicide mortality compared with female suicide mortality.
These findings reinforce the importance of governmental financial support for regional suicide prevention programmes and improvement of socioeconomic disability through the enhancement of regional welfare/social safety nets and improvement of regional social protection vulnerability.
In spite of an increasing older population which is at high risk of suicide, the decrease in national suicide mortality suggests the effectiveness of financial support for regional activities on suicide mortality rates in other Asian countries, which are ageing populations with higher suicide mortality rates.
The present study has several limitations: only prefectural (but not municipal) suicide mortality was analysed and only the Japanese case was considered, lacking an Asian perspective.
Introduction
Suicide is a major public health concern worldwide. In 2016, the global suicide mortality rate was approximately 800 000, and the annual global age-standardised suicide rate is 10.53 per 100 000 population (WHO model SDR).1 It is well known that unemployment and2–4 recessions are fundamental risk factors for increasing suicide mortality, referred to as ‘economic suicide’ in Europe, North America and Asia.5–10 Indeed, in Japan, following the collapse of the asset bubble in 1991 and the Asian economic crisis in 1997, both the unemployment rate and suicide mortality drastically increased in Japan (online supplementary appendix 1).11 12 This Japanese public health crisis started to improve in 2009. Suicide mortality remained at approximately 26 per 100 000 between 2000 and 2009 (raw data), but has decreased to 16.5 per 100 000 as of 2018 (online supplementary appendix 1).12 The complete unemployment rate in Japan also decreased 50% during 2010–2018, in line with the reduction of suicide mortality (online supplementary appendix 1).11 Contrary to rates of suicide mortality and complete unemployment, Japanese GDP per capita has remained tardily/slightly increasing during the early 1990s to 2018 (online supplementary appendix 1).13 Therefore, the period of change for suicide crisis in Japan is considered to have started in 2009.
bmjopen-2020-037537supp001.pdf (198KB, pdf)
In the face of this public health crisis, during this period of change (2009), the Cabinet Office (CAO) established an ‘Emergency Fund to Enhance Community-Based Suicide Countermeasures’ (EFECBSC), which contributed to the development of regional (prefectural/municipal) suicide prevention programmes between 2009 and 2014.10 14 15 The main framework of EFECBSC was the enhancement of regional (prefectural/municipal) welfare/social safety nets and a social protection system. It was composed of 10 independent sub-divisions which supported five independent prefectural and five municipal regional programmes, such as the personal consultation support programme (PCS), the telephone consultation support programme (TCS), the development programme of leaders and listeners (DLL), the enlightenment programme (ELM), and the intervention model programme (IVM) (figure 1).14 Each municipality submitted its municipal suicide prevention programme to its prefecture. Prefectures then submitted their prefectural programmes, along with municipal programmes, to EFECBSC of CAO, which allocated funds to each prefecture, including budgets for prefectures and municipalities (figure 1).14 In this way, prefectural and municipal suicide prevention programmes were independent of each other (figure 1).14 EFECBSC enhanced regional welfare and social safety nets, and improved regional social protection vulnerability.10 Therefore, these data in Japan suggest the possibility that financial support, such as EFECBSC, plays an important role in the reduction of suicide mortality via enhancement of regional welfare/social safety nets and the social protection system.
Figure 1.
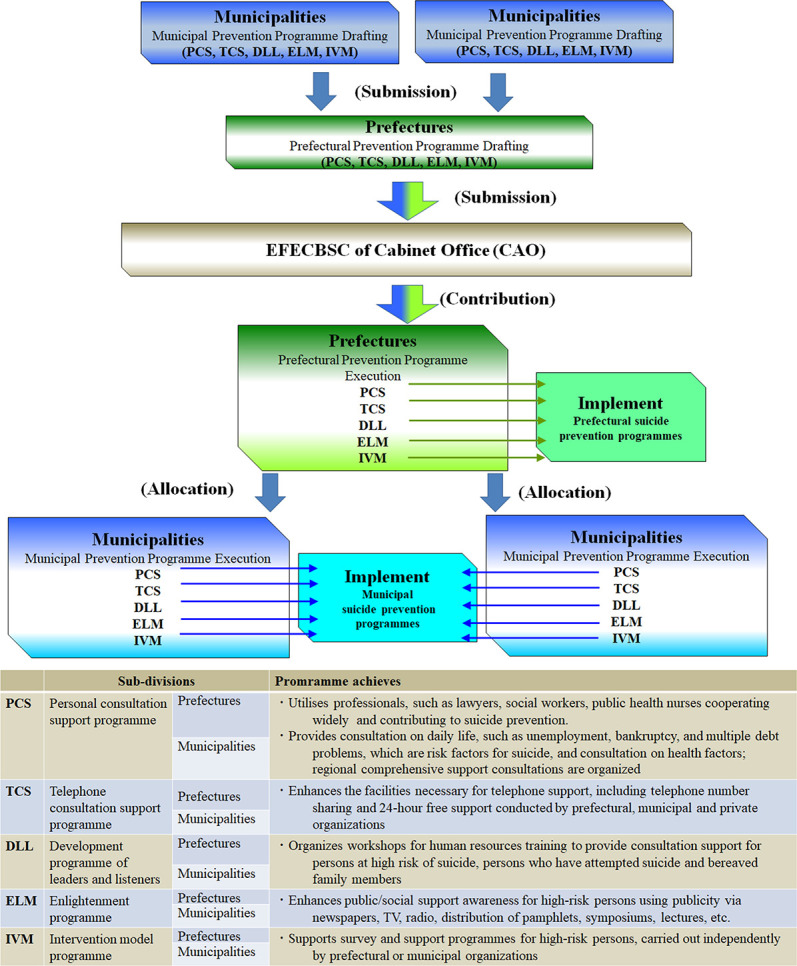
The ‘Emergency Fund to Enhance Community-Based Suicide Countermeasures’ (EFECBSC) submission and allocation process. EFECBSC was composed of five prefectural sub-divisions: personal consultation support programme (PCS), telephone consultation support programme (TCS), development programme of leaders and listeners (DLL), enlightenment programme (ELM), and intervention model programme (IVM), and five municipal sub-divisions: PCS, TCS, DLL, ELM and IVM. Each municipality submitted its suicide prevention programmes to its prefecture. Each Prefecture then submitted its own programme, together with the municipal programmes to EFECBSC of the cabinet office (CAO). EFECBSC then allocated funds to each prefecture, which included budgets for both prefectures and municipalities.14
Until recently, numerous public health studies reported that suicide mortality rates were increased by recessions and increasing unemployment rates. However, recent studies have reported that suicide mortality is affected not only by unemployment rates/recessions but by very complex multifactorial interactions among socioeconomic factors, including unemployment, reduced GDP per capita, social protection vulnerability, recessions and austerity.5–10 16 17 Specifically, vulnerability of social protection systems and high annual economic growth enhance and prevent the impact of unemployment on suicide mortality, respectively.6 8 Furthermore, the interaction between recession and austerity also increases suicide mortality as a double boost.16 Against this multifactorial risk interaction, enhancements of welfare/social safety nets and labour market programmes supported by governmental finance contribute to improving suicide mortality rates in Europe, North America and Asia.5 7 10 16
Based on achievements in reducing suicide mortality in the past decade, in 2019, the Japanese government introduced a new national suicide prevention programme, ‘Law Concerning the Promotion of Research and Utilisation of Results to Contribute to the Comprehensive and Effective Implementation of Suicide Prevention’. The major objectives of this programme include developing more cost-effective/evidence-based regional (prefectural/municipal) suicide prevention programmes compared with EFECBSC.12 According to the new governmental suicide prevention programme, we recently demonstrated that the regional (prefectural/municipal) implementation amount of EFECBSC was size-dependently and gender-specifically related to a decrease in suicide mortality between 2009 and 2018.10 In particular, the prefectural implementation amount of EFECBSC size-dependently decreased male suicide mortality, but had no effect on female suicide mortality; however, the municipal implementation amount of EFECBSC decreased both male and female suicide mortalities.10 These findings suggest that governmental financial support to enhance regional suicide prevention programmes has contributed to reducing Japanese national suicide mortality, whereas sensitivities of male and female suicide mortalities were independent of each other.10 The gender-specific suicide mortality15 18 19 sensitivity is also observed in Europe, North America and Asia. Economic downturns were associated with19 mainly increased male suicide mortality, whereas severe economic crises were associated with increased male and female suicide mortalities.5 7 9 In particular, in Italy governmental expenditure contributing to active labour market programmes provided buffering mechanisms for the negative effect of socioeconomic disability on male suicide mortality in those aged 45–54.7 Therefore, these gender-specifc and age-specific sensitivities against suicide mortality increasing and decreasing are notable findings7 10; however, the effects of EFECBSC on gender-specific and age-specific suicide mortality remains to be clarified.
In this study, we hypothesised that suicide mortality has gender-specific and age-specific sensitivities to unemployment rate, GDP per capita and EFECBSC, based on previous findings about the impacts of macroeconomic factors and governmental financial support on suicide mortality.5–10 Therefore, to develop a more cost-effective, evidence-based regional suicide mortality prevention programme, in this study, we analyse the impacts of prefecture-disaggregated unemployment rate, GDP per capita and the regional (prefectural/municipal) implementation amount of EFECBSC to 10 sub-divisions on gender and age disaggregated suicide mortalities between 2009 and 2018 when national suicide mortality has been decreasing.
Materials and methods
Data
Suicide mortality and population data for all 47 Japanese prefectures were obtained by using the same methods as in our previous study.10 Age, gender and prefecture disaggregated suicide mortalities of all 47 prefectures between 2009 and 2018 were obtained from the Ministry of Health, Labour and Welfare (MHLW) and from the Statistics Bureau of the Ministry of Internal Affairs and Communications (SBMIAC) of Japan.12 20 Annual age, gender and prefecture disaggregated suicide mortalities were derived from basic regional suicide data (MHLW), and population exposure (denominator) was obtained from the basic resident register (SBMIAC).20 Data on each prefectural complete unemployment rates, GDP per capita between 2009 and 2018 and regional (prefectural/municipal) implementation amount of EFECBSC to 10 sub-divisions from 2009 to 2014 were derived from SBMIAC,21 CAO13 and MHLW,22 respectively. The implementation amounts of 10 EFECBSC sub-divisions between 2009 and 2014 of each prefecture14 were calculated by dividing the EFECBSC for each year by the prefectural population of the same year.
Standardisation of suicide mortality rates
Both (male plus female), male and female suicide mortalities were calculated separately within eight age subgroups: less than 19 years (10s), 20–29 years (20s), 30–39 years (30s), 40–49 years (40s), 50–59 years (50s), 60–69 years (60s), 70–79 years (70s) and over 80 years (80s). All 47 prefectures have a large population distribution, with mean±SD=2.7±2.6 million, median=1.7 million, maximum=12.5 million, and minimum=0.6 million. Therefore, to eliminate small population artefacts, age and gender disaggregated prefectural suicide mortalities were calculated using the empirical Bayes standardised mobile ratio (EBSMR)23 by the EB estimator for the Poisson/gamma model version 2.1 (National Institute of Public Health, Wako, Japan) (https://www.niph.go.jp/soshiki/gijutsu/download/ebpoig/index_j.html).
Statistical analysis
The least squares method was used to analyse time-dependent reduction trends in EBSMR of age, gender and prefectural specific groups during 2009–2018 by using BellCurve for Excel version 3.2 (BellCurve, Tokyo, Japan).10 The trends of complete unemployment rate and GDP per capita between 2009 and 2018 were also calculated by the least squares method (BellCurve for Excel version 3.2). Implementation amounts of 10 EFECBSC sub-divisions, including prefectural and municipal PCS, TCS, DLL, ELM and IVM, were calculated as a sum of the implementation amounts of 10 EFECBSC sub-divisions in each year between 2009 and 2014. This study was conducted to improve financial budget structures for activation of the regional suicide prevention programme via cost-effective evaluation of EFECBSC and clarification of specific vulnerabilities, which were insufficiently covered by EFECBSC in regional welfare/social safety nets and regional social protection. Therefore, to quantify the effects of the regional implementation amounts of 10 EFECBSC sub-divisions, unemployment rate and GDP per capita on regional EBSMR trends, adopted stepwise multiple regression analysis was used.10 Stepwise multiple regression analysis with p values of 0.05 and 0.10 for respective entry and removal (SPSS for Windows, version 26, IBM, Armonk, NY, USA) was used to explore the effects of implementation amounts of 10 EFECBSC sub-divisions, regional trends of unemployment rate and GDP per capita on regional EBSMR trends of three groups: male, female and male plus female. The assumptions of multiple regression models were verified by normal P-P plot for standardised residual regression (SPSS for Windows, version 26). Multicollinearity of multiple regression analysis was suspected if the variance inflation factor (VIF) value was greater than 2.5.24
Patient and public involvement
No patient and public were involved in this study. Only secondary data were used for the analyses.
This study was exempt from ethical approval from Mie University.
Results
Stepwise multiple regression analysis detected significant effects of implementation amount of EFECBSC sub-divisions and unemployment rates on EBSMR trends of male plus female, male and female mortality rates, but in contrast to our expectations, GDP per capita did not affect these EBSMR trends (table 1 and online supplementary appendix 2).
Table 1.
Effects of the implementation amounts of EFECBSC sub-divisions, unemployment rate and per capita GDP on EBSMR trends
| Adjusted R2 | F | p | Factor | β | p | VIF | ||
| Male + female | ||||||||
| 20s | 0.450 | 13.547 | 0.001 | Prefectural | TCS | −0.234 | 0.05 | 1.12 |
| Prefectural | DLL | 0.376 | 0.01 | 1.10 | ||||
| Prefectural | ELM | −0.598 | 0.001 | 1.20 | ||||
| 30s | 0.264 | 9.247 | 0.001 | Prefectural | IVM | −0.323 | 0.05 | 1.04 |
| Municipal | ELM | −0.38 | 0.01 | 1.04 | ||||
| 40s | ||||||||
| 50s | 0.380 | 10.388 | 0.001 | Prefectural | PCS | 0.319 | 0.01 | 1.02 |
| Prefectural | ELM | −0.418 | 0.001 | 1.02 | ||||
| CUR | 0.440 | 0.001 | 1.00 | |||||
| 60s | 0.336 | 6.812 | 0.001 | Prefectural | IVM | −0.375 | 0.01 | 1.11 |
| Municipal | PCS | 0.369 | 0.01 | 1.20 | ||||
| Municipal | ELM | −0.308 | 0.05 | 1.11 | ||||
| CUR | 0.325 | 0.05 | 1.11 | |||||
| 70s | 0.406 | 11.463 | 0.001 | Prefectural | ELM | −0.300 | 0.05 | 1.15 |
| Municipal | TCS | −0.352 | 0.01 | 1.15 | ||||
| Municipal | ELM | −0.427 | 0.001 | 1.09 | ||||
| 80s | 0.359 | 9.595 | 0.001 | Prefectural | PCS | −0.268 | 0.05 | 1.04 |
| Prefectural | ELM | −0.346 | 0.01 | 1.08 | ||||
| Prefectural | IVM | −0.321 | 0.05 | 1.08 | ||||
| Male | ||||||||
| 20s | 0.419 | 34.151 | 0.001 | Prefectural | ELM | −0.657 | 0.001 | 1.00 |
| 30s | 0.196 | 6.613 | 0.01 | Prefectural | IVM | −0.328 | 0.05 | 1.04 |
| Municipal | ELM | −0.295 | 0.05 | 1.04 | ||||
| 40s | 0.133 | 8.034 | 0.01 | Municipal | DLL | −0.389 | 0.01 | 1.00 |
| 50s | 0.497 | 16.122 | 0.001 | Prefectural | PCS | 0.265 | 0.05 | 1.02 |
| Prefectural | ELM | −0.552 | 0.001 | 1.02 | ||||
| CUR | 0.455 | 0.001 | 1.00 | |||||
| 60s | 0.291 | 7.281 | 0.001 | Prefectural | PCS | 0.267 | 0.05 | 1.02 |
| Prefectural | ELM | −0.417 | 0.01 | 1.02 | ||||
| CUR | 0.363 | 0.01 | 1.00 | |||||
| 70s | 0.322 | 11.934 | 0.001 | Prefectural | ELM | −0.460 | 0.001 | 1.03 |
| Municipal | DLL | −0.305 | 0.05 | 1.03 | ||||
| 80s | 0.343 | 8.995 | 0.001 | Prefectural | ELM | −0.408 | 0.01 | 1.07 |
| Prefectural | IVM | −0.367 | 0.01 | 1.16 | ||||
| Municipal | PCS | 0.274 | 0.05 | 1.09 | ||||
| Female | ||||||||
| 20s | ||||||||
| 30s | ||||||||
| 40s | ||||||||
| 50s | 0.136 | 8.264 | 0.01 | Prefectural | PCS | 0.394 | 0.01 | 1.00 |
| 60s | ||||||||
| 70s | 0.217 | 13.726 | 0.01 | Municipal | DLL | −0.483 | 0.001 | 1.00 |
| 80s | 0.146 | 8.854 | 0.01 | Municipal | ELM | −0.405 | 0.01 |
Effects of implementation amount of 10 EFECBSC sub-divisions, trends of complete unemployment rates (CUR) and GDP per capita on EBSMR trends of male plus female, male and female mortality analysed by stepwise multiple regression analysis.
CUR, complete unemployment rate; DLL, development programme of leaders and listeners; EBSMR, empirical Bayes standardised mobile ratio; EFECBSC, Emergency Fund to Enhance Community-Based Suicide Countermeasures; ELM, enlightenment programme; IVM, intervention model programme; PCS, personal consultation support programme; TCS, telephone consultation support programme; VIF, variance inflation factor.
Effects of implementation amounts of EFECBSC sub-divisions, unemployment rate and GDP per capita on male plus female EBSMR trends
Stepwise multiple regression analysis detected significant effects of implementation amount of EFECBSC sub-divisions and unemployment rates on male plus female EBSMR trends, but GDP per capita did not affect these trends (table 1, figure 2 and online supplementary appendix 2). 20s EBSMR trends were decreased by prefectural TCS and ELM, but were increased by prefectural DLL. 30s EBSMR trends were decreased by prefectural IVM and municipal ELM. 50s EBSMR trends were decreased by prefectural ELM and complete unemployment rate (CUR), but were increased by prefectural PCS. 60s EBSMR trends were decreased by prefectural IVM, municipal TCS and ELM, but were increased by municipal PCS. 70s EBSMR trends were decreased by prefectural ELM, municipal TCS and ELM. 80s EBSMR trends were decreased by prefectural PCS, ELM and IVM. Implementation amount of EFECBSC, CUR and GDP per capita did not affect 40s male plus female EBSMR trends.
Figure 2.

Effects of the implementation amount of EFECBSC (Emergency Fund to Enhance Community-Based Suicide Countermeasures) sub-divisions and complete unemployment rate on empirical Bayes standardised mobile ratio (EBSMR) trends of male plus female mortalities. Ordinates indicate EBSMR trends of male plus female mortalities of age-disaggregated populations, and abscissas indicate implementation amount of EFECBSC sub-divisions: personal consultation support programme (PCS), telephone consultation support programme (TCS), development programme of leaders and listeners (DLL), enlightenment programme (ELM), and intervention model programme (IVM), and five municipal sub-division: PCS, TCS, DLL, ELM and IVM (¥ per population). Brown and light blue spheres indicate prefectural and national EBSMR trends and population size, respectively. Black and red lines indicate the regression lines of significantly positive (reduced suicide mortality) and negative (increased suicide mortality) factors, respectively. CUR, complete unemployment rate.
Effects of implementation amounts of EFECBSC sub-divisions, unemployment rates and per capita GDP on male EBSMR trends
Stepwise multiple regression analysis detected significant effects of implementation amount of EFECBSC sub-divisions and unemployment rates on male EBSMR trends, but GDP per capita did not affect male EBSMR trends (table 1, figure 3 and online supplementary appendix 2). 20s EBSMR trends were decreased by prefectural ELM. 30s EBSMR trends were decreased by prefectural IVM and municipal ELM. 40s EBSMR trends were decreased by prefectural DLL. Both EBSMR trends of 50s and 60s were decreased by prefectural ELM and CUR, but were increased by prefectural PCS. 70s EBSMR trends were decreased by prefectural ELM and municipal DLL. 80s EBSMR trends were decreased by prefectural ELM and IVM, but were increased by municipal PCS.
Figure 3.

Effects of the implementation amount of EFECBSC (Emergency Fund to Enhance Community-Based Suicide Countermeasures) sub-divisions and complete unemployment rate on male empirical Bayes standardised mobile ratio (EBSMR) trends. Ordinates indicate male EBSMR trends of age-disaggregated populations, and abscissas indicate implementation amount of EFECBSC sub-divisions: personal consultation support programme (PCS), telephone consultation support programme (TCS), development programme of leaders and listeners (DLL), enlightenment programme (ELM), and intervention model programme (IVM), and five municipal sub-division: PCS, TCS, DLL, ELM and IVM (¥ per population). Blue and light blue spheres indicate prefectural and national EBSMR trends and population size, respectively. Black and red lines indicate the regression lines of significantly positive (reduced suicide mortality) and negative (increased suicide mortality) factors, respectively. CUR, complete unemployment rate.
Effects of implementation amounts of EFECBSC sub-divisions, unemployment rates and per capita GDP on female EBSMR trends
Stepwise multiple regression analysis detected significant effects of implementation amount of EFECBSC sub-divisions and unemployment rates on female EBSMR trends, but GDP per capita did not affect these trends (table 1, figure 4 and online supplementary appendix 2). EBSMR trends of 70s and 80s were decreased by municipal DLL and ELM, respectively. By contrast, 50s EBSMR trends were increased by prefectural PCS. Implementation amount of EFECBSC, CUR and GDP per capita did not affect female EBSMR trends of 20s, 30s, 40s and 60s.
Figure 4.

Effects of the implementation amount of EFECBSC (Emergency Fund to Enhance Community-Based Suicide Countermeasures) sub-divisions and complete unemployment rate on female empirical Bayes standardised mobile ratio (EBSMR) trends. Ordinates indicate female EBSMR trends of age-disaggregated populations, and abscissas indicate implementation amount of EFECBSC sub-divisions: personal consultation support programme (PCS), telephone consultation support programme (TCS), development programme of leaders and listeners (DLL), enlightenment programme (ELM), and intervention model programme (IVM), and five municipal sub-divisions: PCS, TCS, DLL, ELM and IVM (¥ per population). Red and light blue spheres indicate prefectural and national EBSMR trends and population size, respectively. Black and red lines indicate the regression lines of significantly positive (reduced suicide mortality) and negative (increased suicide mortality) factors, respectively.
Discussion
This study shows the age-specific and gender-specific sensitivities of suicide mortalities to implementation amount of EFECBSC and unemployment rate, whereas GDP per capita did not have an impact. In environments in which individual (possibly masculine) identity is bound up with work, unemployment poses a greater status threat; conversely, where women’s labour force participation rates are lower, the threat or experience of unemployment may have a less significant effect on women’s mental health.5 Similarly, economic downturns could increase male suicide mortality only, whereas recession increased both male and female suicide mortalities.7 Taken together with previous findings in Europe and North America, the present results suggest that unemployment is a risk factor for an increase in male suicide mortality compared with female suicide.
Female EBSMR was not affected by complete unemployment rates and was less sensitive to EFECBSC compared with male EBSMR, since only female EBSMR of older populations (70s and 80s) were sensitive to the municipal development programme of leaders and listener and the enlightenment programme, respectively. In contrast to female EBSMR, the age-dependent sensitivity of male EBSMR can be broadly classified into two categories. The male EBSMR trends of the over 50s were decreased by the prefectural enlightenment programme, and the 50s and 60s male EBSMR trends were decreased by reduced complete unemployment rate, but surprisingly increased by the prefectural personal consultation support programme. However, the male EBSMR trends of the under 40s could not be detected by specific factors. These results suggest that improvement of socioeconomic conditions and comprehensive suicide prevention programmes which targeted older male suicide mortality have successfully decreased suicide mortality in the older male population, resulting in reduced national suicide mortality rates.
In most regions of the world, including Japan, male suicide mortality is over twice that of female suicide mortality.10 25 The suicide mortality of middle/working-aged and older populations is also higher than that of younger/adolescent populations in most regions.25 Moreover, there are gender differences in attitudes towards suicide, with men tending to possess more maladaptive attitudes about suicide.26 These patterns are found in all age groups, from adolescents to older adults.27 28 Furthermore, non-lethal suicide attempts are more common among women,29 and men are more likely to use more lethal means than females.27 30 Taking such robust gender differences into consideration, one might expect that it would be common for validated approaches to suicide prevention to consider gender differences when planning and evaluating interventions. Unfortunately, insufficient attention has been paid to gender differences when considering suicide risk and intervention responses.31–33 Several studies have evaluated gender but failed to show gender differences.34
In contrast to previous research, prior to the ‘Basic Act on Suicide Prevention’ and ‘General Policies for Comprehensive Measures against Suicide’, some preliminary research was conducted in Japan35 about intervention model programmes and regional suicide prevention programmes. These preliminary studies reported the reduction in suicide mortality rates among over 65s, and that 70% of the reduced suicide mortality rate was due to addressing female risk factors.36 The suicide prevention programmes reported in these studies were composed of workshops run by municipal public health nurses and social, recreational, physical or volunteering group activities to enhance social support resources.36 In EFECBSC, these already implemented activities were categorised as the municipal personal consultation support programme, developmental programme of leaders and listeners, and intervention model programme. Women are less resistant to social/municipal resources and group meetings than men,37 resulting in a greater sensitivity of females to municipal systems of leaders and listeners. Moreover, the impairment of physical and mental functions associated with ageing is exhibited in community and social communication dysfunction.38 In general, men are more socially affected than women.39 40 Therefore, the physical or psychological dysfunctions of older partners often means the loss of social relationships for both individuals.41 For individuals with ageing social dysfunction, it is easy to understand why interventional active suicide prevention programmes, such as the personal consultation support programme and the intervention model programme, are more effective than passive programmes, such as the enlightenment programme and the development programme of leaders and listeners. In fact, based on these concepts, regional suicide prevention programmes in various prefectures have targeted the reduction of suicide mortality rates among the older population.
As our previous research has suggested, the different sensitivities of male and female suicide mortality to prefectural suicide prevention programmes are, at least partially, explained by the gender-specific socioeconomic background of suicide.10 Based on those previous findings, this study determined the effects of EFECBSC on suicide mortality of gender and age disaggregated populations, and hypothesised that enriching prefectural social community support, including the enlightenment programme and the intervention model programme, will prevent an increase in male suicide mortality. Meeting our expectations, the prefectural enlightenment programme contributed significantly to the reduction in suicide mortalities of a wide range of age groups. However, contrary to expectations, although EFECBSC primarily targets the reduction of male suicide mortality, the effects of EFECBSC were limited to female suicide mortality. Moreover, male plus female and female 40s EBSMR trends were not related to any sub-division of EFECBSC. The less sensitive suicide mortalities of middle/working-aged groups (20s, 30s and 40s) to EFECBSC means that regional suicide prevention programmes do not address the welfare/social safety nets and regional social protection vulnerability associated with suicide in working-age populations. These disappointing results may be reasonable because, due to preliminary findings, older populations were the primary targets of regional suicide prevention programmes across prefectures and municipalities.36
After the collapse of the asset bubble in 1991, the unemployment rate increased but neither male nor female suicide mortalities changed (online supplementary appendix 1). Following the Asian economic crisis in 1997, both male and female suicide mortalities in Japan were drastically increased (online supplementary appendix 1). Therefore, the increasing Japanese suicide mortality in 1998 was affected by both the collapse of the asset bubble in 1991 and the Asian economic crisis in 1997. In detail, the increased suicide mortality was due to the synergistic effects of unemployment and long-term unemployment (more than 12 months) induced by these two recessions, similar to the case in Italy.7 Long-term unemployment increases the incidence of several mental disorder through a lower level of social integration.7 Additionally, fear of losing one’s job and/or corporate restructuring are risk factors for suicide.10 18 42 Indeed, over the past two decades, increases in suicide mortality among middle-aged (working-age) men as a result of modifications in the corporate environment have been observed in other Asian countries, such as South Korea, Hong Kong and Taiwan.9 Enhancement of welfare/social safety nets and labour market programme supported by governmental finance protected against socioeconomic disability induced suicide in Japan and Europe.7 10 Conversely, employment insecurity and lack of social protection in economically active environments have been associated with high suicide mortality rates among middle-aged Japanese men.18 Therefore, improvement in employment insecurity, welfare/social safety nets and social protection vulnerability via regional suicide prevention programmes supported by EFECBSC plays an important role in the reduction of male suicide mortality in Japan.
Contrary to male suicide mortality, female suicide mortality was affected by severe economic downturns rather than financial cycle fluctuations.7 Although Japanese women have experienced some social advancement, they continue to have primary responsibility for childcare in a social system that offers poor childcare support. Indeed, unemployment rates did not affect female suicide mortality. Many women are forced to play subordinate roles to men due to limited childcare support resources, leading to temporary employment interruptions and decreasing social circles due to childcare demands.10 In addition, Japan’s declining birth rate and ageing population place greater pressure on women to bear and rear children.43–45 If this proves to be a factor in female suicide, then improvements in childcare support resources, and supporting mothers in finding satisfaction in a relatively small childcare community, may contribute to a reduction in female suicide mortality. If improvements in socioeconomic disabilities, that is, a supportive system to prevent childcare and employment insecurity, can contribute to prevention of suicide mortality rates, the target of regional suicide prevention programmes must be modified as soon as possible. Although various legal arrangements are required, the development of comprehensive support systems for women who attempt to commit suicide could contribute to reduced female suicide mortality, since non-lethal suicide attempts are more common among women.29
Although the present study demonstrated that governmental financial support for regional suicide prevention programmes plays an important role in the reduction of suicide mortality of gender-specific and age-specific vulnerable groups, the study has several limitations. Suicide mortality (EBSMR) was disaggregated by prefecture but not by municipality. This might have provided more detailed information on the role of the implementation amount of financial support in regional suicide prevention programmes and ageing in the change in level. EFECBSC has contributed to the development of prefectural and municipal suicide prevention programmes, but the management of these programmes is not limited to EFECBSC, and may also include prefectural or municipal finances. The present results indicated that the prefectural enlightenment programme and intervention model programme, and the municipal development programme of leaders and listeners, and enlightenment programme are most effective suicide prevention programmes; however, more detailed research is needed to confirm this conclusion. We cannot deny the importance of the implementation amount threshold for the function of each suicide prevention programme. In other words, it should be considered that the prefectural development programme of leaders and listeners, and the prefectural and municipal personal consultation programme have not yet been developed sufficiently to contribute to reducing suicide mortality. Indeed, the implementation amount of the prefectural enlightenment programme (28%), intervention model programme (17%), and the municipal enlightenment programme (13%) were the largest in the 10 EFECBSC sub-divisions, whereas the implementation amounts of the prefectural development programme of leaders and listeners (7%), the prefectural (6%) and municipal personal consultation support programme (5%) were smaller.
Conclusions
Further interventions for working-age populations (20s~40s) and women are necessary in order to further address the major causes of suicide mortality in Japan. Indeed, this study determined that EFECBSC is less effective in reducing the female suicide mortality rate compared with the male rate. In an ageing country, such as Japan, having a detailed understanding of suicide mortality based on age structure, and identifying specific innovations in suicide prevention programmes are essential for effective suicide prevention. Nevertheless, the general downward trend in suicide mortality suggests that Japan is making progress in developing a comprehensive prevention programme. Regional public health planners and policymakers at prefectural and municipal levels should consider specific actions to reduce regional suicide mortality by identifying the social drivers, and by offering programmes, such as personal and telephone consultation support, the development programme of leaders and listeners, the enlightenment programme, the intervention model and unemployment. In the future, the budget structure should be made more cost-effective and, following several more detailed observations of suicide mortality rates in Japan, other Asian countries with ageing populations and high suicide mortality rates can also reduce their suicide mortality rates.
Supplementary Material
Footnotes
Contributors: All authors were responsible for the development of the study design. MO is responsible for conceptualisation. MO, TH and RK are responsible for data collection and statistical analysis. MO and TS have been involved in writing the manuscript. All authors have read the manuscript, contributed to and approved the manuscript.
Funding: This study was supported by Regional Suicide Countermeasures Emergency Enhancement Fund of Mie Prefecture.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: All data relevant to the study are included in the article or uploaded as supplementary information. All raw data are available to any persons from Japanese National databases in Statistics Bureau of the Ministry of Internal Affairs and Communications (SBMIAC), Cabinet Office (CAO) and Ministry of Health, Labour and Welfare (MHLW).
References
- 1.World Health Organization Suicide rates (per 100,000 population). global health Observatory. Geneva, Switzerland: WHO, 2016. https://www.who.int/gho/mental_health/suicide_rates/en/accessed2019.12.12019 [Google Scholar]
- 2.Alothman D, Fogarty A. Global differences in geography, religion and other societal factors are associated with sex differences in mortality from suicide: an ecological study of 182 countries. J Affect Disord 2020;260:67–72. 10.1016/j.jad.2019.08.093 [DOI] [PubMed] [Google Scholar]
- 3.Norström T, Grönqvist H. The great recession, unemployment and suicide. J Epidemiol Community Health 2015;69:110–6. 10.1136/jech-2014-204602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blasco-Fontecilla H, Perez-Rodriguez MM, Garcia-Nieto R, et al. . Worldwide impact of economic cycles on suicide trends over 3 decades: differences according to level of development. A mixed effect model study. BMJ Open 2012;2:e000785. 10.1136/bmjopen-2011-000785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reeves A, McKee M, Stuckler D. Economic suicides in the great recession in Europe and North America. Br J Psychiatry 2014;205:246–7. 10.1192/bjp.bp.114.144766 [DOI] [PubMed] [Google Scholar]
- 6.Toffolutti V, Suhrcke M. Assessing the short term health impact of the great recession in the European Union: a cross-country panel analysis. Prev Med 2014;64:54–62. 10.1016/j.ypmed.2014.03.028 [DOI] [PubMed] [Google Scholar]
- 7.Mattei G, Pistoresi B, De Vogli R. Impact of the economic crises on suicide in Italy: the moderating role of active labor market programs. Soc Psychiatry Psychiatr Epidemiol 2019;54:201–8. 10.1007/s00127-018-1625-8 [DOI] [PubMed] [Google Scholar]
- 8.Mattei G, Pistoresi B. Unemployment and suicide in Italy: evidence of a long-run association mitigated by public unemployment spending. Eur J Health Econ 2019;20:569–77. 10.1007/s10198-018-1018-7 [DOI] [PubMed] [Google Scholar]
- 9.Chang S-S, Gunnell D, Sterne JAC, et al. . Was the economic crisis 1997-1998 responsible for rising suicide rates in East/Southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc Sci Med 2009;68:1322–31. 10.1016/j.socscimed.2009.01.010 [DOI] [PubMed] [Google Scholar]
- 10.Kato R, Okada M. Can financial support reduce suicide mortality rates? Int J Environ Res Public Health 2019;16:4797. 10.3390/ijerph16234797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Training TJIfLPa Complete unemployment rate and effective opening-to-application rate, 2020. Available: https://www.jil.go.jp/kokunai/statistics/timeseries/html/g0301.html [Accessed 12 Nov 2019].
- 12.Ministry of Health, Labour and Welfare Basic data on suicide in the region, 2019. Available: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html [Accessed 12 Nov 2019].
- 13.Cabinet Office GDP statistics, 2019. Available: https://www.esri.cao.go.jp/jp/sna/menu.html [Accessed 21 Jan 2020].
- 14.Ministry of Health, Labour and Welfare Regional suicide countermeasures emergency enhancement fund, 2019. Available: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000134741.html [Accessed 12 Nov 2019].
- 15.Nakanishi M, Yamauchi T, Takeshima T. National strategy for suicide prevention in Japan: impact of a national fund on progress of developing systems for suicide prevention and implementing initiatives among local authorities. Psychiatry Clin Neurosci 2015;69:55–64. 10.1111/pcn.12222 [DOI] [PubMed] [Google Scholar]
- 16.Toffolutti V, Suhrcke M. Does austerity really kill? Econ Hum Biol 2019;33:211–23. 10.1016/j.ehb.2019.03.002 [DOI] [PubMed] [Google Scholar]
- 17.Stuckler D, Basu S, Suhrcke M, et al. . The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet 2009;374:315–23. 10.1016/S0140-6736(09)61124-7 [DOI] [PubMed] [Google Scholar]
- 18.Kim SY, Kim M-H, Kawachi I, et al. . Comparative epidemiology of suicide in South Korea and Japan: effects of age, gender and suicide methods. Crisis 2011;32:5–14. 10.1027/0227-5910/a000046 [DOI] [PubMed] [Google Scholar]
- 19.Suzuki E, Kashima S, Kawachi I, et al. . Prefecture-level economic conditions and risk of suicide in Japan: a repeated cross-sectional analysis 1975-2010. Eur J Public Health 2014;24:949–54. 10.1093/eurpub/cku023 [DOI] [PubMed] [Google Scholar]
- 20.Statistics Bureau of the Ministry of Internal Affairs and Communications Population, demographics and number of households based on basic resident register, 2019. Available: http://www.soumu.go.jp/main_sosiki/jichi_gyousei/daityo/jinkou_jinkoudoutai-setaisuu.html [Accessed 12 Nov 2019].
- 21.Statistics Bureau of the Ministry of Internal Affairs and Communications Labor force survey, 2019. Available: https://www.stat.go.jp/data/roudou/pref/index.html [Accessed 21 Jan 2020].
- 22.Ministry of Health LaW Bugets for suicide prevention programmes, 2019. Available: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000133838.html [Accessed 12 Nov 2019].
- 23.Kawaguchi H, Koike S. Association between the density of physicians and suicide rates in Japan: nationwide ecological study using a spatial Bayesian model. PLoS One 2016;11:e0148288. 10.1371/journal.pone.0148288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Allison PD. Multiple regression: a primer. 1st edition SAGE Publications, Inc, 1999. [Google Scholar]
- 25.Organization WH Suicide data, 2017. Available: https://www.who.int/mental_health/prevention/suicide/countrydata/en/ [Accessed 1 Dec 2019].
- 26.Gould MS, Velting D, Kleinman M, et al. . Teenagers' attitudes about coping strategies and help-seeking behavior for suicidality. J Am Acad Child Adolesc Psychiatry 2004;43:1124–33. 10.1097/01.chi.0000132811.06547.31 [DOI] [PubMed] [Google Scholar]
- 27.World Health Organization Preventing suicide: a global imperative. World Health Organization, 2014. [Google Scholar]
- 28.Centers for Disease Control and Prevention (CDC) Suicide among adults aged 35-64 years--United States, 1999-2010. MMWR Morb Mortal Wkly Rep 2013;62:321–5. [PMC free article] [PubMed] [Google Scholar]
- 29.Tsirigotis K, Gruszczynski W, Tsirigotis M. Gender differentiation in methods of suicide attempts. Med Sci Monit 2011;17:PH65–70. 10.12659/MSM.881887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gould MS, Kramer RA. Youth suicide prevention. Suicide Life Threat Behav 2001;31 Suppl:6–31. 10.1521/suli.31.1.5.6.24219 [DOI] [PubMed] [Google Scholar]
- 31.Weisz JR, Sandler IN, Durlak JA, et al. . Promoting and protecting youth mental health through evidence-based prevention and treatment. Am Psychol 2005;60:628–48. 10.1037/0003-066X.60.6.628 [DOI] [PubMed] [Google Scholar]
- 32.Mann JJ, Apter A, Bertolote J, et al. . Suicide prevention strategies: a systematic review. JAMA 2005;294:2064–74. 10.1001/jama.294.16.2064 [DOI] [PubMed] [Google Scholar]
- 33.Klimes-Dougan B, Klingbeil DA, Meller SJ. The impact of universal suicide-prevention programs on the help-seeking attitudes and behaviors of youths. Crisis 2013;34:82–97. 10.1027/0227-5910/a000178 [DOI] [PubMed] [Google Scholar]
- 34.Oliver RJ, Spilsbury JC, Osiecki SS, et al. . Brief report: preliminary results of a suicide awareness mass media campaign in Cuyahoga County, Ohio. Suicide Life Threat Behav 2008;38:245–9. 10.1521/suli.2008.38.2.245 [DOI] [PubMed] [Google Scholar]
- 35.Ministry of Health LaW National plan for prevention of suicide, 2018. Available: https://www.mhlw.go.jp/kokoro/nation/about.html [Accessed 12 Nov 2019].
- 36.Oyama H, Sakashita T, Ono Y, et al. . Effect of community-based intervention using depression screening on elderly suicide risk: a meta-analysis of the evidence from Japan. Community Ment Health J 2008;44:311–20. 10.1007/s10597-008-9132-0 [DOI] [PubMed] [Google Scholar]
- 37.Drapeau A, Boyer R, Lesage A. The influence of social anchorage on the gender difference in the use of mental health services. J Behav Health Serv Res 2009;36:372–84. 10.1007/s11414-009-9168-0 [DOI] [PubMed] [Google Scholar]
- 38.Sugimoto T, Sakurai T, Ono R, et al. . Epidemiological and clinical significance of cognitive frailty: a mini review. Ageing Res Rev 2018;44:1–7. 10.1016/j.arr.2018.03.002 [DOI] [PubMed] [Google Scholar]
- 39.Hamilton E, Klimes-Dougan B. Gender differences in suicide prevention responses: implications for adolescents based on an illustrative review of the literature. Int J Environ Res Public Health 2015;12:2359–72. 10.3390/ijerph120302359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lapierre S, Erlangsen A, Waern M, et al. . A systematic review of elderly suicide prevention programs. Crisis 2011;32:88–98. 10.1027/0227-5910/a000076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Umberson D, Wortman CB, Kessler RC. Widowhood and depression: explaining long-term gender differences in vulnerability. J Health Soc Behav 1992;33:10. 10.2307/2136854 [DOI] [PubMed] [Google Scholar]
- 42.Chen Y-Y, Wu KC-C, Yousuf S, et al. . Suicide in Asia: opportunities and challenges. Epidemiol Rev 2012;34:129–44. 10.1093/epirev/mxr025 [DOI] [PubMed] [Google Scholar]
- 43.Phillips MR, Li X, Zhang Y. Suicide rates in China, 1995-99. Lancet 2002;359:835–40. 10.1016/S0140-6736(02)07954-0 [DOI] [PubMed] [Google Scholar]
- 44.Pearson V. Goods on which one loses: women and mental health in China. Soc Sci Med 1995;41:1159–73. 10.1016/0277-9536(94)00424-R [DOI] [PubMed] [Google Scholar]
- 45.Ji J, Kleinman A, Becker AE. Suicide in contemporary China: a review of China's distinctive suicide demographics in their sociocultural context. Harv Rev Psychiatry 2001;9:1–12. 10.1080/10673220127875 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2020-037537supp001.pdf (198KB, pdf)