

ABSTRACT
Background
To describe the implementation of a medicalized hotel in the community of Madrid as a public health resource for the containment of coronavirus disease (COVID-19) and to describe the characteristics of population benefitted.
Methods
A descriptive study of the implementation of the Via Castellana Medicalised Hotel (VCMH) was conducted. The average monthly household income, educational level and occupational social class of the subjects admitted were obtained through a survey conducted during their stay.
Results
There was no guidance for launching; however the hotel was coordinated by a tertiary referral hospital and attended the preventive medicine regulations and the decrees of legal regimes and authorization of health services in Madrid. Between 19 March and the 9 May 2020, 399 patients were admitted; 59% (235) were migrant; the main reason for referral (58%) was a lack of house conditions for quarantining, including overcrowding, which when compared with the migrant status a positive correlation was found. Some other reasons for referral were homelessness and eviction. Most of the survey participants had low monthly household income, educational level and social class.
Conclusions
This medicalized hotel provided medical care and offered housing to a subgroup of vulnerable population who could not afford a safe quarantine.
Keywords: Covid-19, medicalized hotel, vulnerable groups, quarantine
Introduction
The first case of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-COV2) in Spain was registered in a German tourist in the Canary Islands on 31 January 2020.1 Afterwards, new cases were detected in other regions and a rapid spreading was observed.2 When the World Health Organization declared the coronavirus disease (COVID-19) a pandemic on 12 March 2020,3 Spain was one of the countries with the highest incidence rates of COVID-19 with 5753 confirmed cases and 12.23 infections per 100 000 individuals4; which caused the Spanish government to declare a State of Emergency with mandatory confinement on 14 March.5
As reported worldwide, the distribution of cases was unequal across the country, and Madrid became the autonomous community with the highest infection rates.4 The first case was registered on 25 February but, by 14 March there were 2940 confirmed cases, accounting for 51% of the total cases in Spain.4,6 As a result, the health resources were insufficient to the high demand of patients and both, the emergency rooms and the intensive care units (ICUs) were rapidly overwhelmed.7 In addition, the available human resources were exceeded by the hospitals’ admissions. Thus, in order to optimize the provision of health care in Madrid, a massive hiring of health professionals occurred, and from 8195 new hirings, 857 were retired and new graduate doctors, as well as medicine and nursing students.8,9 However, taking into account that the incorporation of new health graduates to the Spanish National Healthcare System is regularly followed by an annual national examination, this was considered as an exceptional situation.
The State of Emergency allowed the Minister of health taking actions to ensure the provision of services to protect the public health. Among the containment measures adopted, it was included the enabling of public locations to treat COVID-19 patients, such as the Trade Fair Institution of Madrid (IFEMA),whose pavilions were turned into the largest field hospital in Europe equipped with conventional hospital beds and ICUs and which capacity was to care >5000 patients.10 On the other hand, the Madrilenian government together with The Business Association of Hoteliers of Madrid announced the medicalization of hotels, which aimed at following up and isolating clinically established patients who could not complete their respective quarantine in their living places, bringing to the most vulnerable groups, not only shelter to quarantine, but also medical care.11
In Madrid, 13 hotels—including the Via Castellana Hotel—were medicalized and it was estimated that around 2500 patients were attended within these resources.12 In addition, other 22 were used for health professionals’ accommodations, which all together required an investment of >8 million Euros.13 Similarly, in Barcelona other hotels were turned into temporary hospitals for mild patients who needed surveillance, and in Tenerife a hotel was locked down for quarantine after the detection of positive cases among the guests.14–16 However, the use of hotels was not limited to Spain. It was a common containment measure adopted worldwide which bound to ease the strain that hospitals were facing. For instance, in the USA these resources were launched to isolate patients but also medical staff17; in Brazil 1000 hotel rooms were offered to elder and other vulnerable population, and other accommodation facilities were turned into medical centers in the UK.18,19
Nevertheless, the organization of medicalized hotels is unknown and the scientific reports in this regard are scarce. Moreover, their role in epidemic outbreaks and the characteristics of the population benefited has not been widely portrayed. Therefore, the aim of our study was to describe the implementation of a medicalized hotel in the community of Madrid as a public health resource for the containment of COVID-19 and to describe the characteristics of population admitted.
Methods
Hotel logistics
A descriptive study of the implementation of the VCMH was conducted. The logistics of the hotel, the referral and discharge criteria, as well as the role of the professionals involved were described carrying out discussion groups three times a week during two consecutive weeks, which were performed by seven general practitioners who worked at the VCMH.
Characteristics of the patients
The data from the clinical electronic register were used to create a database which included sociodemographic variables such as age, gender and country of origin. The severity and treatment of COVID-19 and the psychiatric history were also gathered.
The patients’ socioeconomic status and their educational level were obtained from a survey conducted during their stay at the VCMH. It was administered through printed questionnaires that were delivered and collected meeting the standardized prevention measures. One of the ad hoc questionnaires was specifically designed to evaluate the socioeconomic status of the participants at that time. It consisted on three questions which assessed material deprivation: Q1) average monthly household income; Q2) educational level and Q3) occupational social class (a free box to describe their occupation, which was later codified according to the newest Spanish classification of occupational social class CSO-SEE12-see Table 1).20 The administration of this survey was approved by a local ethics committee and an informed consent was obtained from every participant.
Table 1.
Social class classification
| Occupational social class-CSO-SEE12 |
|---|
| I. Managerial of business of 10 or more employees and professionals with university degrees |
| II. Managerial of business of 10 or less employees and professionals with university diplomatures and other professions of technical support. Artists and athletes. |
| III. Intermediate occupations: employees with administrative function and other services (nursing assistant, security services) |
| IV. Self-employed workers |
| V. Supervisors and skilled workers |
| VI. Primary sector and other semi-skilled workers |
| VII. Non-skilled workers |
The results of Q1 and Q2 were compared with the general population statistics published on the National Statistical Institute website as follows: Q1 with the Household Budget Survey (2018) and Q2 with the Education Statistics (2018).
Finally, due to the patients referred to the VCMH were sent from La Paz Hospital Complex (LPHC), the number of patients attended at the medicalized hotel was contrasted to the number of patients seen at this hospital during the same period of time. Moreover, the length of stay at the VCMH and the duration from symptoms onset of COVID-19 to discharge were also calculated.
Statistical analysis
To describe the demographic characteristics of the patients an observational and retrospective study was conducted. The qualitative variables were presented as absolute and relative frequencies, whereas the numeric variables were reported as means and standard derivation (±SD). The Pearson and χ2 tests were used to compare the categorical data of the survey and statistical significance was set at a P < 0.05.This analysis was conducted using Stata 15 software.
Results
Implementation and performance of the medicalized hotel
The performance of the VCMH was coordinated by LPHC due to its proximity (distance of 1.5 kilometers), which facilitated the ambulance referral of patients and the transportation of pharmaceuticals and medical equipment. Most of the main areas of the VCMH performed within this facility, but some of them were located at LPHC (Fig. 1).
Fig. 1.
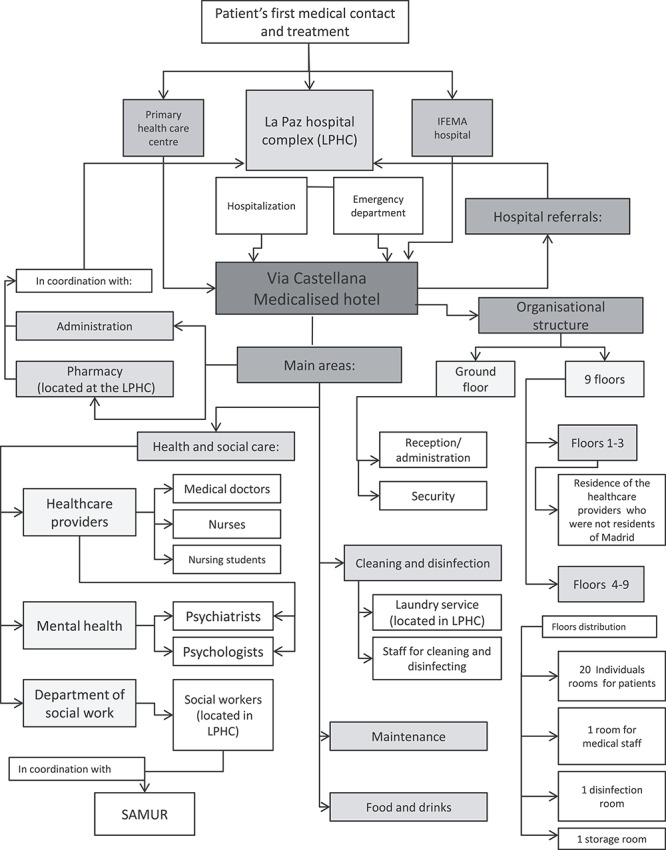
Hotel logistics. The performance of the VCMH involved: 29 nursing students; 21 medical doctors (including 2 psychiatrists); 20 nurses; 7 hospital administrators; 4 hospital wardens; 3 information technologists; 3 maintenance workers; and 2 volunteers (1 chiropodist and 1 priest).
There was no guidance for launching; however the hotel facility had to be modified attending the preventive medicine regulations and the decrees of the legal regime and procedure of authorization and registration of centers, services and health in the community of Madrid.21,22 Thus, the floor was protected with special materials (linoleum), the furniture was changed to ensure the correct sanitation of the areas and the provision of medicines and medicals was ensured trough the supervision and collaboration with LPHC.
The hotel had a capacity to attend 120 patients at a time distributed in six floors. Its performance was held by 89 professionals, including two volunteers (Fig. 1). During the day shifts there were a medical doctor, a nurse, and a nursing student per floor; whereas at night shifts, besides the nursing staff per floor, a single medical doctor was responsible for the care of all patients. However, when necessary, an interconsultation with another medical specialist or a social worker was conducted. A daily medical telephone follow-up was performed and vital signs were monitored from one to three times a day according to the patients’ clinical status. Room visits were carried out wearing a Personal Protective Equipment; however if social distancing could be ensured—for instance, to talk to the patient from the hall—a mask, facial protection and a sterile mixed gown were used. The performance of the medical and nursing staff were supervised by an intensive care specialist and a nurse manager, respectively.
Characteristics of the patients
Regardless the severity of COVID-19 during the hospitalization, certain clinical and functional conditions were required to be admitted at the medicalized hotel. For instance, patients must be independent for the activities of daily living; they needed to have preserved cognitive-motor skills, and be hemodynamically stable (no requirements of oxygen or intravenous medication).
Between 19 March and the 9 May 2020, 399 patients were admitted to the VCMH. Figure 2 shows the admissions and discharges records among this period. From them, 64% (257) were referred from LPHC and due to the upcoming closure of the IFEMA hospital, the referrals from this center incremented during the month of April, reaching 32% (129) of the overall admissions. Only 2%7 of the patients were sent from a primary healthcare-center and another 2%6 from other hospitals. Considering the VCMH as an extension of LPHC, the subjects attended at the hotel accounted for 5–12% of the overall hospital admissions.
Fig. 2.
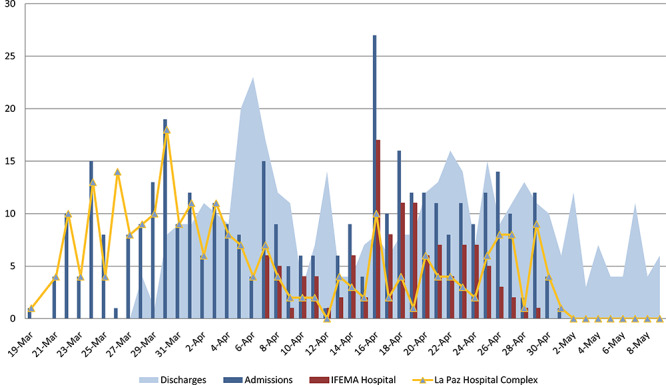
Admissions and discharges records.
The mean age of the patients admitted was 55.24 years (SD 14.81); 57% were male (231) and 59% (235) were migrant. The main reason for referral (58%) was a lack of house conditions for quarantining, including overcrowding, and when this condition was compared with the migrant status, a positive correlation was found (Table 2). In the rest of the cases, 16% (64) cohabitated with a family member in a high-risk group for COVID-19, and 8% (32) had no permanent address due to homelessness or eviction. In another 16% (64), the reasons for referral could not be classified within the previous definitions because a possibility of being home-quarantined was found in the medical records; therefore when this situation occurred an unclassified referral was considered. In 3%13 of the patients, the reason for referral was not identified.
Table 2.
Sociodemographic variables in patients admitted to the Hotel. Migrant status and lack of house conditions for quarantining (including house overcrowding)
| Nationality ** | Lack of house conditions for quarantining ** | Total | Pearson | |
|---|---|---|---|---|
| NO (%) | SI (%) | |||
| Spanish | ||||
| YES | 87 (21%) | 74 (19%) | 399a | 19.4 (P = 0.00)* |
| NO | 72 (18%) | 155 (39%) | ||
*Obtained by χ2 test.
**Extracted from electronic clinical register.
aProportions estimated over the whole sample including missing data (2.2%).
According to the questionnaires administered to measure household income, educational level and occupational social class, the rate of respondents differed for each question: 150 valid responses were obtained for the educational level item (99%), 131 valid for the monthly household income item (86%) and 108 for the occupational social class item (71%) (Table 3). Most of the participants (92%) had a monthly household income under 1900 Euros, which is twice the current Spanish interprofessional minimum wage. Conversely, the Household Budget Survey reflects that 63% of Spanish families have an income >1999 Euros in 2015.23 On the other hand, the participants had lower educational level than reported in the general population: only 27% had superior studies versus 35% of men and 40% of women from the national survey.24 However, it has to be noticed that the samples are not totally comparable because the latter only includes population between 25 and 65 years old. Regarding the occupational social class item, there was an overrepresentation of the classes III and VI (29% and 35%, respectively), and the most common occupations within these classes were nursing and cleaning.
Table 3.
Socioeconomic characteristics of the patients admitted to the VCMH
| Characteristic | Frequency | % |
|---|---|---|
| Studies level | ||
| Elementary studies | 36 | 24 |
| High-school studies | 87 | 58 |
| University studies | 27 | 18 |
| Total | 150 | 100 |
| Monthly household incomea | ||
| <950 Euros | 55 | 41,98 |
| Between 950 and 1900 Euros | 65 | 49,62 |
| Between 1900 and 2850 Euros | 4 | 3,05 |
| >2850 Euros | 7 | 5,34 |
| Total | 131 | 100 |
| Occupational social classb | ||
| Class I | 1 | 0,93 |
| Class II | 4 | 3,7 |
| Class III | 32 | 29,63 |
| Class IV | 6 | 5,56 |
| Class V | 14 | 12,96 |
| Class VI | 13 | 12,04 |
| Class VII | 38 | 35,19 |
| Total | 108 | 100 |
aMultiples similar to interprofessional minimum wage.
bOccupational Social Class–CSO-SEE12.
Regarding the severity of COVID-19, 82% (326) had mild to severe pneumonia, and only 2%8 had respiratory distress syndrome or septic shock prior to their admission to the VCMH. One hundred and one (25%) patients had a medical history of a mental health condition; however most of them were not under medical treatment at the moment of referral. Fifty-one (13%) subjects required metal health support. Psychological advice was given through telephone calls, and if a psychiatric consultation was needed the patients were visited in their rooms. Forty-three (10%) patients required a hospital social worker support, which in the cases of homelessness or eviction, aimed at coordinating a discharge plan together with the Municipal Assistance and Rescue Emergency Service of Madrid-known as SAMUR for its spanish acronym-.
The discharge criteria followed included the evaluation of the social conditions of the patients—especially when being homeless—, the period of time from onset of symptoms of COVID-19, the clinical status, and being a health worker (Fig. 3). The length of stay at the VCMH was a mean of 7 days, and the mean time from onset of symptoms to discharge was 25 days. Nevertheless, after it patients were advised to strictly follow personal hygiene recommendations in order to protect household contacts.
Fig. 3.
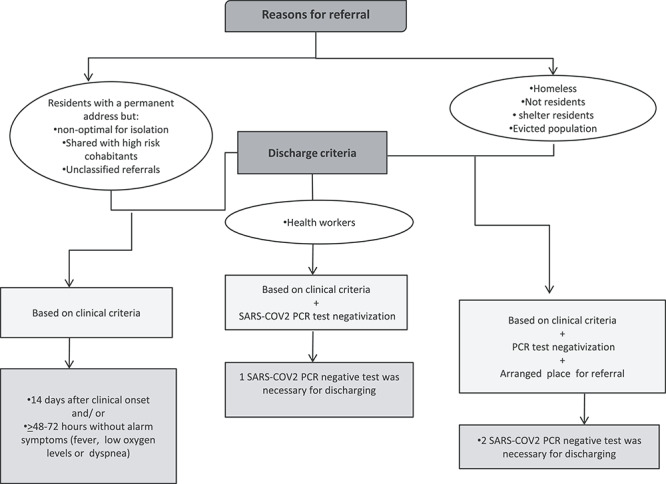
Reasons for referral and discharge criteria.
Discussion and conclusion
Main findings of this study
The European Network of Infectious Diseases defines a high level isolation unit (HLIU) as a ‘health-care facility specifically designed to provide safe, secure, high-quality, and appropriate care, with optimal infection containment and infection prevention and control procedures, for a single patient or a small number of patients who have, or who may have, a highly infectious disease’.25 The VCMH did not meet all the technical requirements of a HLIU; however it shared certain operational management and clinical care characteristics. For instance, it was led and directed by an intensive care specialist who was responsible for the medical staff coordination and a nurse manager who ward the performance of the nursing workforce. Protocols for personnel protection, hygiene and sanitation were launched and there were secure communication and control access systems. In addition, the hotel operated under the supervision of LPHC, a tertiary referral center located at a distance of 1.5 km.
On the other hand, hospitals and hotels have common characteristics, such as individual rooms and toilets, which made the VCMH not only a viable solution for the containment of COVID-19, but for the caring of patients, especially because hospitalization is not necessary in most of the cases but some level of clinical care is usually required. The reasons of referral to the VCMH depended on the patients’ living conditions; however many of them were symptomatic at the moment of admission and were discharge after clinical recovery. Hence, not only the need of having a place to quarantine, but of being followed up justifies the implementation of medicalized hotels.
Taking into account that the ratio of specialized medical attention and nursing per 1000 habitants in Spain is 1.9 and 3.2, respectively.26 The 24-hour hotel performance and the availability of 21 medical doctors and 49 nurses, resulted in 5.7 physicians and 2.4 nurses per bed, which highlight the personalized patients’ attention.
Considering that the viral clearance among mild cases occurs within the first 2 weeks after clinical manifestations,27 the fact that patients were discharged, in average, 25 days from symptoms onset reduced the likelihood of spreading the virus after leaving the hotel. However, it has to be noticed that SARS-COV2 tests by polymerase chain reaction (PCR) were only performed in health professionals and residences of public shelters before discharge.
The survey of material deprivation confirmed that the patients admitted to the VCMH had socioeconomic features which make them more vulnerable than the general population. For instance, the majority of patients were migrants and having a lack of house conditions for quarantining was the main reason for referral. In addition, the most common occupations were nursing and cleaning assistants, which increased their risk of contagion.
What is already known on this topic
Poverty modulates how individuals face the crisis. Firstly, conditions like house overcrowding or labor insecurity hamper social distancing or hygiene measures. Secondly, the virus has more morbimortality among chronic illnesses related to social class.
Socioeconomic inequalities act as fundamental cause of the disease, and as sociomedical literature suggests, not only the pandemic but also public health interventions could deepen the existing health inequalities.28
What this study adds
An economic crisis is expected to increase the pressure over the most vulnerable groups. Thus, every government is in the duty of making a response which includes equality principles, and as this paper describes, this Medicalised Hotel had served to this principle offering housing to a subgroup of population who could not afford a safe quarantine.
On the other hand, the high number of COVID-19 patients worldwide and the lack of specific treatment and vaccinations represent great challenges to the entire global health community and enhance the need of preparedness and control of positive cases, especially among the most vulnerable social groups. This paper provides information regarding the medicalization of a hotel in Madrid and the population that resulted benefited, which could be useful for future similar containment measures.
Limitations of this study
There was a lack of scientific reports on medicalized hotels; therefore it was difficult to describe the differences between the VCMH and the characteristics of the population admitted with other similar facilities. On the other hand, the participation in the survey conducted was limited and varied among questions.
Acknowledgment
We would like to acknowledge the general practitioners of the VCMH Alfredo Nebreda de la Mora, Samuel Lijeron Farel, Alejandro Marcos Rodrigo and Julia San José Vargas, who participated in the discussion groups which helped to describe the logistics of the hotel.
K. L. Ramírez-Cervantes, Working team member
V. Romero-Pardo, Psychiatrist
C. Pérez-Tovar, Working team member
G. Martínez-Alés, Research Fellow
M. Quintana, Coordinator of the COVID@HULP working team, Associate Professor of the Faculty of Medicine of the Autonomous University of Madrid
Conflict of interest
None declared.
References
- 1. Linden, P. Sanidad confirma en La Gomera el primer caso de coronavirus en España. El País: 2020. Available from: https://cutt.ly/coEQqwi [Google Scholar]
- 2. Ministerio de Sanidad Coronavirus (COVID-19) - 08 de marzo 2020. Madrid, Spain: Sitio oficial del Departamento de Seguridad Nacional; 2020Available from: https://cutt.ly/FoEQGos. [Google Scholar]
- 3. WHO Regional Office for Europe. WHO announces COVID-19 outbreak a pandemic. Copenhagen, Denmark: World Health Organization (WHO), 2020Available from: https://cutt.ly/goEEkpS. [Google Scholar]
- 4. Ministerio de Sanidad Coronavirus (COVID-19)- 14 de Marzo 2020. Madrid, Spain: Sitio Oficial del Departamento de Seguridad Nacional; Available from: https://cutt.ly/coE5SMA. [Google Scholar]
- 5. Ministerio de la Presidencia RclCyMD. Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. Madrid, Spain: Boletín Oficial del Estado «BOE» núm. 67, de 14/03/2020.2020. [Google Scholar]
- 6. Consalud.es. El coronavirus se expande por España: confirmado un caso en Madrid. Madrid, Spain: Redacción Consalud, 2020. Available from: https://cutt.ly/zoRyL5u.
- 7. Soto A. Las UCI dejan atrás la saturación y ya ven la luz. Hoy: Madrid, Spain 2020. Available from: https://cutt.ly/ism1Z8F. [Google Scholar]
- 8. Gobierno de la Comunidad de Madrid. La Comunidad de Madrid ha reforzado la atención sanitaria frente al coronavirus con la contratación de 10.034 profesionales [press release]. Madrid, Spain: Portal comunidad.madrid, 2020. Available from: https://cutt.ly/ZoOrmCP. [Google Scholar]
- 9. Gobierno de España. Orden SND/232/2020, de 15 de marzo, por la que se adoptan medidas en materia de recursos humanos y medios para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. Boletín Oficial del Estado, BOE-A-2020-3700. Madrid, Spain 2020.
- 10. El mundo. La Comunidad de Madrid habilita las primeras 1.396 camas en Ifema por el coronavirus. Madrid, Spain: The Trust Project, EM, 2020Available from: https://cutt.ly/uoOy4KK. [Google Scholar]
- 11. Gobierno de la Comunidad de Madrid. La Comunidad de Madrid habilita los dos primeros hoteles medicalizados para la recuperación de pacientes afectados por coronavirus [press release]. Madrid, Spain: Portal comunidad.madrid, 2020. Available from: https://cutt.ly/1smg2G1. [Google Scholar]
- 12. El mundo. La Comunidad de Madrid cierra dos de los 13 hoteles medicalizados ante la caída de pacientes con coronavirus. Madrid, Spain: The Trust Project, EM, 2020. Available from: https://cutt.ly/zoOoQS2. [Google Scholar]
- 13. Gobierno de la Comunidad de Madrid. Invertimos más de 8 millones en los hoteles para pacientes COVID-19 y profesionales [Press release]. Madrid, Spain: Portal comunidad.madrid, 2020. Available from: https://cutt.ly/QoOpHys. [Google Scholar]
- 14. La vanguardia. Los pabellones Salud y los hoteles sanitarios en Barcelona refuerzan la respuesta a la crisis de la COVID-19. Barcelona, Spain: La vanguardia Ediciones, 2020Available from: https://cutt.ly/ToOs88L. [Google Scholar]
- 15. Hoefer A, Pampaka D, Rivas Wagner E et al. Management of a COVID-19 outbreak in a hotel in Tenerife, Spain. Int J Infect Dis 2020;96:384–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Gironés-Bredy CE, Posca-Maina M, Pinto-Plasencia RG et al. First public health measures for the containment of COVID-19: a hotel in quarantine. Emergencias 2020;32(3):194–6. [PubMed] [Google Scholar]
- 17. Kromrei, G. St. Regis, Wythe Hotel open rooms to medical staff, patients as occupancy plummets. New York, USA: The Red Deal, 2020. Available from: https://trd.media/ny/u4ZqmR. [Google Scholar]
- 18. Cornali, F. ¿Por qué ancianos de Río de Janeiro se resisten a estar gratis en hoteles cuatro estrellas durante la cuarentena?. Rio de Janeiro, Brasil: Anadolu Agency, 2020. Available from: https://cutt.ly/uoOgrDL. [Google Scholar]
- 19. Gillert J, Hall J, Pastor C et al. Medicalisation of hotels in the context of coronavirus-COVID-19. London, United Kingdom: Baker McKenzie, 2020. Available from: https://cutt.ly/hoOgvTm. [Google Scholar]
- 20. Domingo-Salvany A, Bacigalupe A, Carrasco JM et al. Proposals for social class classification based on the Spanish National Classification of occupations 2011 using neo-Weberian and neo-Marxist approaches. Gac Sanit 2013;27(3):263–72. [DOI] [PubMed] [Google Scholar]
- 21. Gobierno de España. Decreto 51/2006, de 15 de junio, del Consejo de Gobierno, Regulador del Régimen Jurídico y Procedimiento de Autorización y Registro de Centros, Servicios y Establecimiento Sanitarios de la Comunidad de Madrid. Presidencia, Cd: Legislación de la comunidad de Madrid, Madrid, Spain, 2020. [Google Scholar]
- 22. Gobierno de España. Orden 288/2010, de 28 de mayo, por la que se regulan los requisitos técnicos generales y específicos de los centros y servicios sanitarios sin internamiento, y de los servicios sanitarios integrados en organización no sanitaria en la Comunidad de Madrid. Presidencia. Cd: Legislación de la comunidad de Madrid, 2020. [Google Scholar]
- 23. Instituto Nacional de Estadística. Distribución según nivel de ingresos mensuales netos regulares del hogar. INEbase. Madrid, Spain, 2015. [Internet]. Available from: https://www.ine.es/jaxiT3/Datos.htm?t=24992#!tabs-tabla.
- 24. Instituto Nacional de Estadística. Nivel de formación de la población adulta (de 25 a 64 años). [Internet]. Madrid, Spain: INEbase, 2015. Available from: https://cutt.ly/AoOmeO4.
- 25. Bannister B, Puro V, Fusco FM et al. Framework for the design and operation of high-level isolation units: consensus of the European network of infectious diseases. Lancet Infect Dis 2009;9(1):45–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Coduras-Martinez A, Del Llano-Señaris J. La sanidad Española en cifras. Madrid, Spain: Circulo de la Sanidad, 2018.
- 27. Liu Y, Yan L-M, Wan L et al. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis 2020;20(6):656–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav 2010;51Suppl:S28–40. [DOI] [PubMed] [Google Scholar]