

Abstract
Professional physical therapist education has experienced a transformation over the last few decades, moving to a doctoring profession with more autonomy and a broader scope of practice. These changes have occurred in parallel with systemic and structural changes in health care and higher education, both of which have experienced challenges with improving access and controlling costs, and have become a centerpiece of legislative and political discourse. At the same time, advances in technology have introduced new possibilities in education, with the emergence of online, blended, and “flipped” learning models that supplement or replace face-to-face instruction with distance learning. Hybrid education is a type of blended learning, utilizing both face-to-face and online instructional strategies. In a hybrid learning environment, online content may be delivered synchronously or asynchronously, replacing traditional face-to-face instructional time and reducing “seat time” for students. Recent attention has been brought to online and hybrid/blended learning in physical therapist education in the wake of the COVID-19 pandemic, as programs have been required to abruptly move from face-to-face to remote instruction. Hybrid and other forms of blended learning strategies have been described at the physical therapist education course level. However, there is no literature describing hybrid learning implementation at the physical therapist education program “levels,” and there has been limited discussion on best practices for delivering hybrid, blended, and online instruction in physical therapist education. This perspective provides an overview of hybrid education, describes theoretical frameworks that guide implementation of a hybrid education curriculum, and discusses future directions for hybrid physical therapist education and educational research.
Blended and hybrid learning have been widely adopted in higher education for some time. A 2008 report found that 35% of all 2- and 4-year degree-granting institutions offered hybrid/blended courses, and nearly two-thirds of 2-year institutions and institutions with >10,000 students had hybrid/blended offerings.1 As overall enrollments have declined across higher education, distance education enrollments have grown. As of the fall of 2016, 31.5% of students enrolled in higher education were taking at least 1 distance education course, up from 25.9% in 2012. Over 5 million undergraduate students and 1 million graduate students reported taking distance education courses in 2016.2 Although some academic leaders question the quality of online learning, they generally agree that blended courses hold more promise than fully online courses, and the vast majority believe the outcomes of hybrid/blended courses are the same or superior to face-to-face instruction.3 The 2016 NMC Horizon report identified “Blended Learning Designs” as 1 of the 6 key trends driving technology adoption and decision-making in higher education.4 Although many questions remain unanswered, advances in internet technology—particularly improvements in connection speeds that allow for creating, sharing, and streaming video—have accelerated the uptake of hybrid/blended learning. The promise of flexibility, increased access, and future innovation has led many scholars to refer to it as the “new normal.”5
A recent—and abrupt—shift in education and health care has emerged in the wake of the COVID-19 pandemic. During the spring of 2020, higher education institutions across the nation were required to close their campuses and quickly transition to virtual instruction. By the end of the 2020 spring term, it was estimated that over 4000 institutions and nearly 26 million students in the United States were affected by COVID-19–related closures.6 These campus closures forced programs that were not designed for online instruction to deliver course content using asynchronous and synchronous online instruction and plan virtual labs or delay labs for onsite instruction once face-to-face learning resumes. Additionally, many health care facilities, following guidance from the Centers for Disease Control to postpone non-emergent outpatient visits and limit visitors and non-essential personnel, canceled clinical internships and onsite training for health professions students. This has had a significant impact on physical therapist programs and students. A March 2020 report from the ACAPT National Consortium of Clinical Educators reported that 91% of programs had students removed from or unable to begin a clinical experience, and 86% of programs reported they had students whose graduation would potentially be delayed due to circumstances related to COVID-19.7
Online, blended, and “flipped” learning models in physical therapist education are not new or novel. They have been described in physical therapist education over the last decade, primarily at the course level.8–19 However, there is no literature describing online, blended, or hybrid physical therapist education at the program level. At its conception, before the COVID-19 pandemic, the purpose of this perspective was to begin that discussion. The authors set out to provide an overview of hybrid education and describe how leveraging technology to educate doctor of physical therapy students more efficiently and effectively at the program level may provide a mechanism for increasing access to doctor of physical therapy education while decreasing cost and time to degree. While this is still an important and necessary discussion, the authors believe that the overall purpose, relevance, and urgency of this perspective have evolved in the wake of COVID-19. Physical therapist education programs are navigating rapidly evolving education and health care landscapes that include interrupted onsite learning and sudden shifts to remote instruction during this international global pandemic. Now is the time to deepen the discussion of hybrid learning in physical therapist education, investigate recommended practices in online instruction, and explore the sound theory on which hybrid education should be based.
Hybrid Education Defined
Hybrid education is one of the more recent developments in technology-based training, which began with mainframe and mini computers in the 1960s.20 According to Ross and Gage, hybrid education is a form of blended learning that reduces face-to-face classroom time, replacing it with out-of-class online learning activities.21 Early approaches to blended learning were first described in the literature in the mid-1990s.22 However, these approaches are still not well-understood across higher education, nor are they consistently described in the literature. In higher education, the term “hybrid” is often used synonymously with “blended” learning or alongside terms such as “flipped,” “online,” or “technology-enhanced” learning. Institutions have varied in the percentage of online instruction they consider as a cutoff for categorizing a course as online or blended/hybrid.1 An accepted definition for a blended/hybrid course, used by the Babson Survey Research Group in their yearly analysis of online and distance education, is one that includes 30% to 79% of content delivered online.3 For the purpose of this perspective, we will refer to hybrid/blended courses and programs as those that are at least 20% face to face, and we will adhere to the following definitions from the position paper adopted by the Commission on Accreditation in Physical Therapy Education:23
Online education—All instruction occurs online, synchronously or asynchronously;
Blended learning—Asynchronous online learning is used to enhance student learning between face-to-face sessions. Online instruction does NOT replace face-to-face time;
Flipped learning—a type of blended learning in which students receive content, usually through recorded lectures accessed asynchronously, then use face-to-face time for active learning;
Hybrid education—utilizes both online and face-to-face learning strategies in an effort to maximize both learning environments. Online learning may be synchronous or asynchronous and may replace face-to-face time;
Traditional face-to-face instruction: All learning experiences occur face to face in classroom, lab, or community settings; all formal instruction occurs synchronously at the same geographic location.
Hybrid Learning in Health Care Education
Hybrid learning has not been widely implemented in health care education, but the literature generally seems to support its success. Multiple studies—including meta-analyses, systematic reviews, and research reports—confirm that internet-based and blended learning delivered in health care education is at least as effective, and could at times be more effective, than traditional instruction.24–30 At the program level, high satisfaction, enhanced learning and technical skills acquisition, and decreased attrition rates have been noted with hybrid curriculum implementation in nursing education.29,31 At the course level, many studies comparing web-based learning with traditional instruction in health care education have noted equal or improved learning outcomes and higher student satisfaction in online and blended courses.32–35
In physical therapist education, at the time of this publication and to our knowledge, there have been no studies investigating hybrid learning as a distinct curricular model. However, there are a handful of studies that have examined the effects of “flipped” or “blended” learning applied to courses in physical therapist education. Studies investigating coursework in anatomy,14 cardiopulmonary care,10 musculoskeletal practice,11,12 neuroanatomy,15 neurological rehabilitation,8,16 therapeutic modalities,9 professionalism and administration,13,17 chronic health condition management,18 and patient self-management support19 have demonstrated that blended learning was at least as effective as traditional learning for student outcomes and satisfaction. In these studies, students reported that the ability to review lectures and patient management videos, self-direct the timing of online content delivery, and attend face-to-face classes designed to solidify and clarify concepts were important beneficial components of blended learning.
The paucity of literature describing online, hybrid, or blended learning in physical therapist education may be explained by concerns about whether key outcomes of physical therapist education, including professional formation and development of psychomotor skills, can be achieved in a largely online environment. To be sure, physical therapy is a “hands-on” and human profession with an ingrained traditional approach to education. This may make it difficult to conceptualize how content can be delivered in any way other than a face-to-face and/or hands-on format. In this perspective, we propose that—when implemented using sound theory—online, blended, and hybrid learning can be (and is being) utilized effectively within courses or across an entire program to guide students in the development of content knowledge, psychomotor skills, clinical reasoning abilities, and professional identity to successfully enter the physical therapy profession.
Evidence-Based Frameworks to Guide Implementation of a Hybrid Doctor of Physical Therapy Curriculum
Developing a hybrid curriculum does not involve simply taking a curriculum designed to be delivered face to face and “shrinking and linking” content within a learning management system so that students may access it remotely. Rather, faculty take on the responsibility of developing a curriculum that is designed to be delivered in a hybrid format and lead to deep and meaningful learning, the ability to connect and construct new knowledge, and the development of a professional identity and key clinical reasoning skills. In this way, delivery of the curriculum does not begin with or focus on instructional technology. Rather, the goal is to use sound learning theory to (1) provide instruction in the optimal format to maximize effective and efficient learning, (2) carefully select media and technologically driven tools to enhance the learning environment, (3) ensure all learning is “need to know” for entry-level practice, and (4) thoughtfully and intentionally construct and integrate synchronous, asynchronous, and face-to-face learning experiences to meet educational objectives and program outcomes. In many ways, a hybrid doctor of physical therapy curriculum is not different from any other doctor of physical therapy curriculum. It is subject to all of the same accreditation criteria and standards and includes similar coursework and clinical experiences. Like any curriculum, it must be based in sound theoretical frameworks to be implemented successfully and ensure student learning. However, it does present unique opportunities and novel challenges for instructional delivery. To guide administrators, faculty, and staff in meeting those challenges, hybrid education must be grounded in sound learning theory, provide faculty a framework for developing teaching expertise, contain processes for developing a community of learners, and—finally—create a plan for technology integration that best supports students and faculty.
Learning Theory and Development of Teaching Expertise
No matter the educational format—online, face to face, or hybrid/blended—good teaching is good teaching and bad teaching is bad teaching. Both can and do occur in all learning environments. Like all doctor of physical therapy programs, a hybrid curriculum should be planned, developed, and implemented consistent with current learning theory. Doctor of physical therapy students are adult learners. According to the theory of andragogy, an adult learning theory first proposed by Knowles, adult learners differ from children in that their maturity makes them less dependent and more self-directed, they draw on past experiences to drive learning, and they demonstrate readiness and motivation to learn when they perceive relevance and immediate value and application of learning.36 When designing a hybrid education experience, doctor of physical therapy educators should tap into adult learning theory and create a cooperative learning environment that gives students a say in their learning process, centers on problem-solving and application rather than memorization of content, and builds sequentially so that learners can draw on prior experiences to construct new knowledge.37
A hybrid curriculum may also be designed using principles of cognitivist and constructivist learning theory. The most widely known and used applications of cognitivism are based on Bloom’s taxonomies, which organize learning processes into a hierarchy through which learners must progress from remembering/understanding to applying, analyzing, evaluating, and creating.38 Learning objectives across a hybrid curriculum and within hybrid courses should intentionally and sequentially ensure that students are progressing through Bloom’s hierarchy as they process and make sense of new information.39 Much like adult learning theory, constructivism holds that learning is not a passive process of “content delivery” from teacher to student. Rather, learning is dynamic, contextual, and social. It emphasizes active learning, problem solving, and collaboration and involves learners drawing on past experience and reflecting on new knowledge to construct meaning.40 Tam (2000) outlines key practices for constructivist teaching and learning, including presenting learners with a “good” problem to actively solve, learning through collaboration with peers, and a teacher who acts as a facilitator, as opposed to an expert, who guides learning.41
While all educators should apply sound learning theory—such as andragogy, cognitivism, and constructivism—to their teaching, faculty in a hybrid learning environment must develop expertise to integrate sound theory into that learning environment. A framework for teaching expertise may be used to guide faculty in their own development across the domains of educational leadership, teaching and learning, professional development, mentorship, and scholarship. Central to this framework are 3 foundational “habits of mind” for creating educational environments that are (1) learning centered, (2) inclusive, and (3) collaborative.42 In a hybrid learning environment, faculty should be intentional about threading these 3 elements through both online and face-to-face instruction. Table 1 outlines key concepts in contemporary learning theory and sample indicators of implementation of these concepts for faculty in a hybrid learning environment.
Table 1.
Key Concepts in Contemporary Learning Theory and Examples of How This Theory May Be Used to Develop a Learning-centered, Collaborative, and Inclusive Hybrid Learning Environment
| Development of Teaching Expertise: Habits of Mind 42 | Adult Learning Theory 36 , 37 | Cognitivism 38 , 39 | Constructivism 40 , 41 | Examples/Indicators |
|---|---|---|---|---|
| Learning centered | Adult learners are motivated and ready to learn | Learners are provided clear objectives that address multiple levels/domains of learning | Learning occurs actively through solving realistic, meaningful, and complex problems | Course syllabi clearly outline course expectations and learning objectives based on learners’ needs and skill levels |
| Adult learners are problem oriented | Teachers serve as a guide, not an expert | Encourage learners to establish their own learning goals (within course objectives) | ||
| Use synchronous online and face-to-face time for learning at mid-high levels of Bloom’s taxonomy: application, analysis, evaluation, and creation | ||||
| Inclusive | Adults bring their lived experiences to the learning environment | Learners are given opportunities for guided practice and to connect learning to real-life situations | Learners must draw on their own experiences to make meaning out of new information | Use readings, iconography, videos, and case studies that represent diverse backgrounds, perspectives, and ethnicities |
| When possible, include diversity in faculty, lab assistants, guest speakers, and standardized patients | ||||
| Use principles of universal design, including captioning video, text-to-speech functions, using multiple examples to activate prior knowledge and experience, accessible LMS or course website | ||||
| Collaborative | Adult learners are self-directed | Teachers give timely, constructive feedback | Learning occurs through interaction with others | During online instruction, create virtual office hours and communicate clearly how and when students can reach you |
| Use multimedia (video, chat, email, social media, and other apps) to facilitate synchronous and asynchronous peer-to-peer communication. Humanize instruction by using video when possible. | ||||
| Make time for peer-to-peer and student-teacher collaboration during both online and face-to-face learning experiences | ||||
| Utilize small group discussion and student “teams” |
Building a Community of Learners
Creating inclusive, learner-centered, and collaborative educational opportunities for students involves building a community of learners, which can be challenging in an online environment. The community of inquiry (CoI) framework developed by Garrison et al43 describes 3 interacting elements that are essential for online teaching and learning: cognitive presence, social presence, and teaching presence. Further, it provides guidance to instructors on how to build educational experiences for online students. The relationship of social, cognitive, and teaching presence with one another and the educational experience is depicted in Figure 1.
Figure 1.
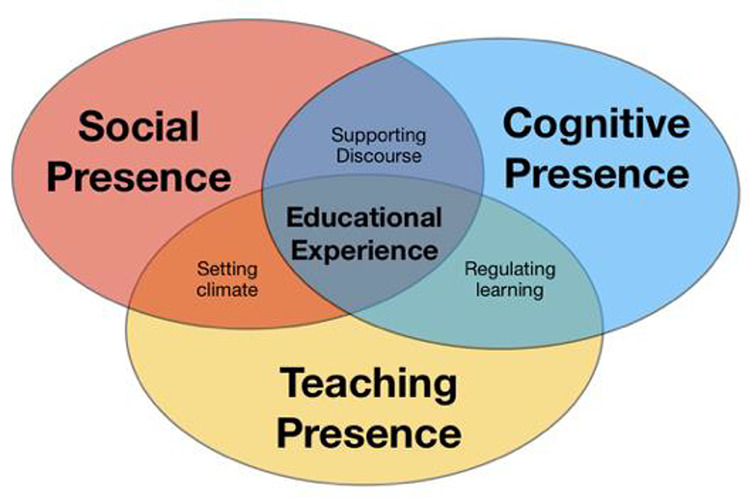
Community of inquiry theoretical framework. Adapted from: The Community of Inquiry, a project of Athabasca University Centre for Distance Education. http://www.thecommunityofinquiry.org/coi. Accessed May 14, 2020. Creative Commons Attribution-ShareAlike 4.0 International License.
Interactions between students may happen more naturally in face-to-face classrooms, where students are located geographically in the same community. However, in an online environment, where students may be located regionally, nationally, or even internationally, students may feel isolation, loneliness, and lack of human interaction. Because a large portion of a hybrid doctor of physical therapist program occurs in an online environment, there is a great need—and opportunity—to use social, cognitive, and teaching presence to build a community of inquiry among learners. Faculty, accrediting bodies, and even students often focus on the teaching presence element of online instruction, which may be simply operationalized as “content delivery.” But, as depicted in the CoI model, a strong teaching presence must exist alongside a strong social presence to “set climate” and build a collaborative learning environment that engages all learners. Cognitive presence must intersect with teaching presence to “regulate learning” and ensure that teachers guide students through higher level learning processes and help them draw on past experiences to make meaning of new knowledge. Finally, cognitive and social presences overlap to support discourse and create an environment in which all learners are engaged, mutual respect exists between and among teachers and learners, and learners feel safe to speak up and contribute to the community. Table 2 provides a definition for each element of the CoI framework, with examples of strategies for developing each element within hybrid doctor of physical therapy education.
Table 2.
Definitions of Social Presence, Teaching Presence, and Cognitive Presence and Examples of How Each of These Elements May Be Developed in a Hybrid Learning Environment
| Element | Definition | Examples/Indicators |
|---|---|---|
| Social presence | “The ability of participants to identify with the community (eg, course of study), communicate purposefully in a trusting environment, and develop interpersonal relationships by way of projecting their individual personalities.”44 | Synchronous online interactions via video conferencing with simultaneous live chat |
| Asynchronous interactions via video, including video-based discussions and assignments with video feedback from the instructor | ||
| Maintenance of low student to instructor ratio during face-to-face labs | ||
| Teaching presence | “Design, facilitation, and direction of cognitive and social processes for the purpose of realizing personally meaningful and educationally worthwhile learning outcomes.”45 | Meaningful asynchronous learning activities organized in the learning management system, including recorded lectures and readings, low-stakes interactive quizzes and “click and reveal” online flashcards, and high-stakes online assessment |
| Direct instruction during online synchronous sessions, including in-class quizzing and providing case-based discussion prompts | ||
| Faculty teams (consisting of experienced faculty, board-certified specialists, and clinical experts in the course content) model authentic clinical reasoning and professional discourse | ||
| Cognitive presence | “Extent to which learners are able to construct and confirm meaning through sustained reflection and discourse”46 | Video- or text-based assignments that require students to construct and connect knowledge and apply key concepts to clinical scenarios |
| Facilitation of case-based discussion and application of concepts during synchronous sessions | ||
| Application of clinical reasoning framework in face-to-face labs |
Using Technology Intentionally and Strategically
Intentional utilization of technology is what allows instructors to create social presence, teaching presence, and cognitive presence in a largely virtual environment. The Substitution, Augmentation, Modification, Redefinition (SAMR) model may be used to guide faculty in technology utilization in online and hybrid learning environments.47 This SAMR model (Fig. 2) describes 4 levels of technology use in teaching. They may be conceptualized as a hierarchy. At the lower level, also referred to by the SAMR model as “below the line,” are substitution and augmentation. These describe using technologies in ways that directly augment or substitute for traditional practices but may or may not result in functional change. This may include practices such as posting handouts as PDF files instead of printing and distributing them to the class (substitution) or recording a lecture of voiceover slides for students to watch on their own time or at their own pace rather than delivering the lecture in a live classroom (augmentation). These “below the line” activities may enhance the learning experience for students by improving accessibility, flexibility, and convenience; and almost all educators use technology for educational enhancement in online, face-to-face, and blended learning environments. However, technology used only at the substitution and augmentation levels may automate teaching and learning, and over-utilization may threaten to remove the human element from instruction. To humanize the online learning experience for students, faculty must thoughtfully integrate technology at a higher level. The SAMR model describes relatively higher level, or above the line, technologies as transformative technologies that result in significant redesign of the learning activity (modification) or allow for completely new tasks that are inconceivable without the technology (redefinition). In hybrid doctor of physical therapy education, transformative use of technology comes largely in the form of video-based platforms. For example, students use video conferencing to participate in live class sessions with faculty to discuss and apply knowledge. This allows not only for synchronous large discussion but also for interactive multimedia communication such as chat, messaging, and polling. Students can move in and out of breakout rooms for small group discussion with the click of a button. This can also be combined with other technologies, such as cloud-based software to collaboratively create and edit documents in real time or an online student response system for in-class quizzing and polling to create an engaging, collaborative learning experience for students and faculty. Video discussion and assessment platforms allow students to asynchronously share ideas, ask questions, demonstrate psychomotor skills, practice verbal communication, and receive feedback from peers and faculty to grow those skills. These video tools can all be seamlessly integrated into the learning management system to create an effective virtual classroom with rich, multi-media opportunities for engagement, sharing, and collaboration. When faculty focus on using above the line strategies for integrating technology into their instructional design and teaching practices, technology and geographic separation are no longer barriers to building community. Rather, technology erases geographic borders, connects students and faculty virtually from remote geographical locations, facilitates a sense of connection and community between learners, and provides transformative, human, and hands-on learning experiences. Table 3 includes an example of how the SAMR model may be applied to both enhance and transform learning in a hybrid doctor of physical therapy course.
Figure 2.
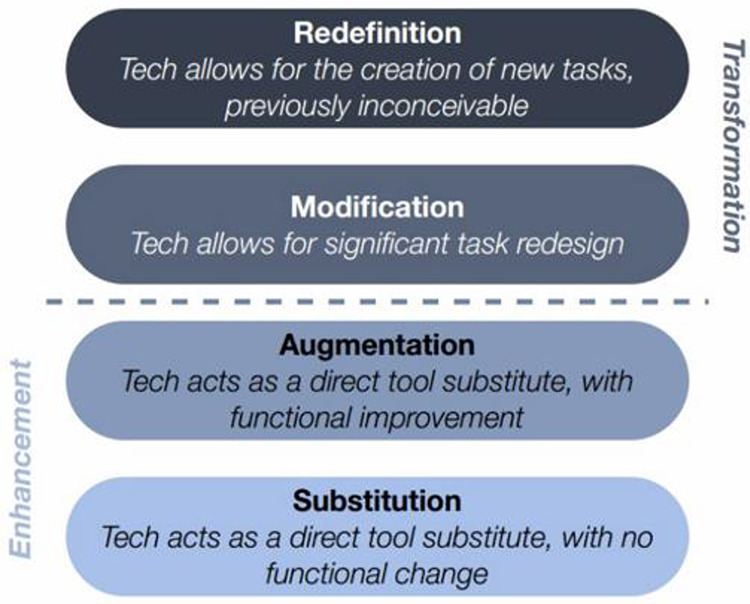
The SAMR (Substitution, Augmentation, Modification, Redefinition) model. From: Puentedura RR. “Learning, technology, and the SAMR model: goals, processes, and practice.” Hippasus website. http://www.hippasus.com/rrpweblog/archives/2014/06/29/LearningTechnologySAMRModel.pdf. Published 2014. Accessed May 14, 2020. Creative Commons Attribution-Noncommercial-Share Alike 3.0 License.
Table 3.
Descriptions of How Technology Is Implemented at the Levels of Substitution, Augmentation, Modification, and Redefinition in a Pediatric Doctor of Physical Therapy Coursea
| Level of Technology Utilization | Sample Implementation in a Hybrid Pediatric Doctor of Physical Therapy Course 48 |
|---|---|
| Redefinition | Students evaluate a video case featuring a child with a developmental disability, develop a plan of care, and use a video assessment platform to upload a video role-playing communicating the plan of care to a child’s family member and demonstrating an intervention strategy. Pediatric clinical experts across the country provide private video feedback assessing students’ clinical reasoning, family-centeredness, and communication skills. Peers may review submissions and provide public peer feedback. Students can respond to teacher and peer feedback and questions, and revise and resubmit their submission if desired. This results in an interactive online asynchronous process of learning, feedback, and assessment of procedural knowledge, conceptual reasoning, communication (peer feedback and role-playing information sharing with family), and professional formation (expert clinical feedback and interaction). This prepares students for authentic experiential learning experiences with clinical experts, children, and families at the onsite lab. |
| Modification | Synchronous online class sessions are led by at least 2 expert faculty via video conferencing. Students may engage in the session using multi-media: audio, video, private and public chat, interactive polling, raise-hand button, etc. A primary faculty member leads the session and engages students through audio, video, polling, and “raised hands.” A secondary faculty engages with students via private and public chat, brings key concepts from the backchannel to the primary instructor, and provides technical support as needed to the primary faculty and students. Virtual “breakout” rooms are used strategically for small group discussion and students and faculty take collaborative notes during the session using a cloud-based word processing platform. |
| Augmentation | Lecture content is broken up into short “lecturettes,” recorded as voiceover slides or white-board videos, and posted to the LMS with features for students to download or stream to watch where/when it works best for them. Videos include features to forward/reverse/pause, speed and slow the pace, or add captions. Lectures may be recorded by a variety of clinical experts in various pediatric specialties rather than all content delivered by the course instructor. This provides accessibility and flexibility in content delivery tailored to individual and collective student needs. |
| Substitution | The course syllabus, readings, and all handouts are posted to the LMS. An introductory overview video is recorded by the instructor and posted to the course home page. This provides students with clear expectations for the course communicated directly from the instructor. |
aLMS = learning management system.
Challenges, Opportunities, and Vision for the Future
As outlined in the sections above, planning and implementing hybrid/blended doctor of physical therapy education requires alignment with contemporary learning theory, building community through online presence, intentional and transformational utilization of technology, and development of teaching expertise to support competencies in hybrid teaching and learning. In the wake of COVID-19, physical therapy educators were abruptly required to suspend onsite learning and provide virtual instruction. It is important to note that—although these efforts have been innovative, thoughtful, and may prove to be successful—this shift of learning designed for face-to-face delivery to virtual delivery may be best described as remote instruction. This should not be confused with online or blended/hybrid learning, as these terms should be reserved for describing teaching and learning designed to be delivered—in whole or part—online. At the time of this writing, college campuses remain closed and there is much uncertainty about if and when onsite instruction will resume. But it seems clear that online instruction will be the “new normal” for all or most doctor of physical therapy programs for the near future, with the possibility that onsite and online instruction may be cyclical as the pandemic progresses. As faculty work to meet the needs of students in this environment, they may use the frameworks, practices, and strategies in this perspective to guide them in conceptualizing, reimagining, and redesigning their courses and curricula to be delivered in an online, blended, or hybrid environment.
As more programs are developed using a hybrid curricular model and/or utilize hybrid instruction as a short-term response to the COVID-19 pandemic, and more graduates of such programs enter physical therapist practice, it will be critical to assess a variety of outcomes. This includes student outcomes such as demographics of the hybrid doctor of physical therapy student, NPTE passage rate, progression into residency, and career satisfaction/trajectory. It will also be necessary to assess institutional/program outcomes such as revenue/expenditures, faculty workload, and administrative load. But beyond that, it will be critical to explore the more broad impact on the profession, health care, and society. Is educational quality maintained in a hybrid environment? Do these programs provide a pathway to physical therapist education for a more diverse population of prospective students? Can they produce a workforce to meet the needs of underserved communities? Does a shorter time to degree and greater ability to control cost of living impact student debt load? Outcomes analysis will certainly prove to be challenging due to variation in programs. There may be large differences in factors such as admissions practices, curriculum delivery, frequency and duration of face-to-face sessions, and how programs use the technology to deliver education (eg, to accelerate vs decelerate the curriculum). Further, because most programs developed using a hybrid education curriculum have done so in partnership with an Online Program Management organization, program differences may be highly influenced by external factors that result from these relationships.
Hybrid doctor of physical therapy education is on the rise and holds great promise for addressing significant challenges facing physical therapist education, such as access, flexibility, faculty shortage, and student debt load. However, there is much that is misunderstood and unknown about hybrid doctor of physical therapy education. As hybrid programs continue to emerge and develop, physical therapist educators, program administrators, institutions that house these programs, and online program management with which they partner should be deliberate about the way in which these programs are implemented and intentional about program assessment in order to balance meeting the needs of the profession with meeting the needs of society.
Author Contributions and Acknowledgments
Concept/idea/research design: K. Gagnon, R. Severin, M.J. Walker
Writing: K. Gagnon, B. Young, T. Bachman, T. Longbottom, R. Severin, M.J. Walker
Project management: K. Gagnon
Disclosures
The authors completed the ICMJE Form for Disclosure of Potential Conflicts of Interest and reported no conflicts of interest.
References
- 1. Parsad B, Lewis L, Tice P. Distance Education at Degree-Granting Postsecondary Institutions: 2006–2007. Washington, DC, USA: National Center for Education Statistics; 2008. [Google Scholar]
- 2. Seaman J, Allen I, Seaman J. Grade Increase: Tracking Distance Education in the United States. Babson Park, MA, USA: Babson Survey Research Group; 2019. [Google Scholar]
- 3. Online report card: tracking online education in the United States. Allen IE, Seaman J, Poulin R, Straut TT; Babson Survey Research Group and Quahog Research Group; 2016. http://celt.li.kmutt.ac.th/research/okmd1/km/wp-content/uploads/2016/10/onlinereportcard.pdf. Accessed May 14, 2020. [Google Scholar]
- 4. Johnson L, Becker SA, Cummins M, Estrada V. NMC horizon report: 2016 higher education edition. https://www.learntechlib.org/p/171478/. 2016. Accessed May 14, 2020.
- 5. Dziuban C, Graham CR, Moskal PD, Norberg A, Sicilia N.. Blended learning: the new normal and emerging technologies. International Journal of Educational Technology in Higher Education. 2018;15:3. [Google Scholar]
- 6. COVID-19 : entangled solutions; Higher education resource center 2020. Accessed May 14, 2020. https://www.entangled.solutions/coronavirus-he/. [Google Scholar]
- 7. Clinical educator COVID-19 report ACAPT—National Consortium of Clinical Educators. https://www.acapt.org/docs/default-source/consortium-(ncce)/nccecovid193ca3e570d79d6aa08906ff0000592408.pdf?sfvrsn=1e3e8fd8_2. March 30, 2020 Accessed May 14, 2020.
- 8. Deprey SM. Outcomes of flipped classroom instruction in an entry-level physical therapy course. J Phys Ther Educ. 2018;32:289. [Google Scholar]
- 9. Adams CL. A comparison of student outcomes in a therapeutic modalities course based on mode of delivery: hybrid versus traditional classroom instruction. J Phys Ther Educ. 2013;27:20. [Google Scholar]
- 10. Bayliss AJ, Warden SJ. A hybrid model of student-centered instruction improves physical therapist student performance in cardiopulmonary practice patterns by enhancing performance in higher cognitive domains. J Phys Ther Educ. 2011;25:14. [Google Scholar]
- 11. Boucher B, Robertson E, Wainner R, Sanders B. “Flipping” Texas State University’s physical therapist musculoskeletal curriculum: implementation of a hybrid learning model. J Phys Ther Educ. 2013;27:72–77. [Google Scholar]
- 12. Murray L, McCallum C, Petrosino C. Flipping the classroom experience: a comparison of online learning to traditional lecture. J Phys Ther Educ. 2014;28:35. [Google Scholar]
- 13. Dal Bello-Haas V, Proctor P, Scudds R. Comparison of knowledge and knowledge application confidence in physical therapist students completing a traditional versus blended learning professional issues course. J Phys Ther Educ. 2013;27:10. [Google Scholar]
- 14. Shead DA, Roos R, Olivier B, Ihunwo AO. Curricular and pedagogical aspects of gross anatomy education for undergraduate physiotherapy students: a scoping review. JBI Evidence Synthesis. 2020;8:893–951. [DOI] [PubMed] [Google Scholar]
- 15. Ge W. Meeting the challenge of instructor shortages: a blended teaching and learning model for a neuroscience course in a doctor of physical therapy program. J Allied Health. 2018;47:103–106. [PubMed] [Google Scholar]
- 16. Veneri DA, Gannotti M. A comparison of student outcomes in a physical therapy neurologic rehabilitation course based on delivery mode: hybrid vs traditional. J Allied Health. 2014;43:e75-e81. [PubMed] [Google Scholar]
- 17. Hyland MR, Pinto Zipp G, Olson V, Lichtman SW. A comparative analysis of computer-assisted instruction and traditional lecture instruction for administration and management topics in physical therapy education. 1 2010;7. [Google Scholar]
- 18. Gardner P, Slater H, Jordan JE, Fary RE, Chua J, Briggs AM. Physiotherapy students’ perspectives of online e-learning for interdisciplinary management of chronic health conditions: a qualitative study. BMC Med Educ. 2016;16:62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Munro V, Morello A, Oster C et al. E-learning for self-management support: introducing blended learning for graduate students—a cohort study. BMC Med Educ. 2018; 18:219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Bersin J. The Blended Learning Book: Best Practices, Proven Methodologies, and Lessons Learned. Hoboken, NJ, USA: John Wiley & Sons; 2004. [Google Scholar]
- 21. Bonk CJ, Graham CR. The Handbook of Blended Learning: Global Perspectives, Local Designs. John Wiley & Sons; 2012. [Google Scholar]
- 22. Goldberg MW, Salari S, Swoboda P. World wide web—course tool: an environment for building WWW-based courses. Computer Networks and ISDN Systems. 1996;28(7–11): 1219–1231. [Google Scholar]
- 23. Swisher D, Marcoux B, Blackinton M, Jette D, Johnson B, Ploeger D, Rouillier K, Rudeen K. Implementing distance education in physical therapist/physical therapist assistant programs. Commission on the Accreditation of Physical Therapy. 2019. http://www.capteonline.org/uploadedFiles/CAPTEorg/About_CAPTE/Resources/Accreditation_Handbook/PositionPapers.pdf. Accessed May 14, 2020. [Google Scholar]
- 24. Cook DA, Levinson AJ, Garside S, Dupras DM, Erwin PJ, Montori VM. Internet-based learning in the health professions: a meta-analysis. JAMA. 2008;300:1181–1196. [DOI] [PubMed] [Google Scholar]
- 25. Liu Q, Peng W, Zhang F, Hu R, Li Y, Yan W. The effectiveness of blended learning in health professions: systematic review and meta-analysis. J Med Internet Res. 2016;18:e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. George PP, Papachristou N, Belisario JM et al. Online eLearning for undergraduates in health professions: a systematic review of the impact on knowledge, skills, attitudes and satisfaction. J Glob Health. 2014;4:010406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Kearns SP, Kelly AL, Barrett J et al. The one day per week nursing program: a web-assisted (hybrid) associate degree nursing program. Teach Learn Nurs. 2006;1:10–17. [Google Scholar]
- 28. Davidson SC, Metzger R, Lindgren KS. A hybrid classroom-online curriculum format for RN-BSN students: cohort support and curriculum structure improve graduation rates. J Contin Educ Nurs. 2011;42:223–232. [DOI] [PubMed] [Google Scholar]
- 29. Robinia KJ, Maas NA, Johnson MM, Nye RM. Program outcomes following implementation of a hybrid curriculum at the certificate level. Nurs Educ Perspect. 2012;33:374–377. [PubMed] [Google Scholar]
- 30. Mu K, Coppard BM, Bracciano AG, Bradberry JC. Comparison of on-campus and hybrid student outcomes in occupational therapy doctoral education. Am J Occup Ther. 2014;68Suppl 2:S51-S56. [DOI] [PubMed] [Google Scholar]
- 31. Buxton T, Buxton J, Jackson A. Hybrid and flipped strategies in a blended RN-BSN program: determining student and faculty perceptions. Nurse Educ. 2016;41:1–2. [DOI] [PubMed] [Google Scholar]
- 32. Bata-Jones B, Avery MD. Teaching pharmacology to graduate nursing students: evaluation and comparison of web-based and face-to-face methods. J Nurs Educ. 2004;43:185–189. [DOI] [PubMed] [Google Scholar]
- 33. Kumrow DE. Evidence-based strategies of graduate students to achieve success in a hybrid web-based course. J Nurs Educ. 2007;46:140–145. [DOI] [PubMed] [Google Scholar]
- 34. Anderson LC, Krichbaum KE. Best practices for learning physiology: combining classroom and online methods. Adv Physiol Educ. 2017;41:383–389. [DOI] [PubMed] [Google Scholar]
- 35. Ilic D, Nordin RB, Glasziou P, Tilson JK, Villanueva E. A randomised controlled trial of a blended learning education intervention for teaching evidence-based medicine. BMC Med Educ. 2015;15:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Knowles MS, et al. The modern practice of adult education. 1980. https://pdfs.semanticscholar.org/8948/296248bbf58415cbd21b36a3e4b37b9c08b1.pdf. Accessed May 14, 2020.
- 37. Blondy LC. Evaluation and application of andragogical assumptions to the adult online learning environment. Journal of interactive online learning. 2007;6:116–130. [Google Scholar]
- 38. Krathwohl DR. A revision of Bloom’s taxonomy: an overview. Theory Pract. 2002;41:212–218. [Google Scholar]
- 39. Picciano AG. Theories and frameworks for online education: seeking an integrated model. Online Learning. 2017;21: 166–190. [Google Scholar]
- 40. Bada SO, Olusegun S. Constructivism learning theory: a paradigm for teaching and learning. Journal of Research & Method in Education. 2015;5:66–70. [Google Scholar]
- 41. Tam Maureen. Constructivism, instructional design, and technology: implications for transforming distance learning. J Educ Techno Soc. 2000;3:50–60. [Google Scholar]
- 42. Kenny N, Berenson C, Chick N et al. A developmental framework for teaching expertise in postsecondary education In: Poster Presented at the International Society for the Scholarship of Teaching and Learning Conference ,Calgary, Alberta, Canada: 2017. http://connections.Ucalgaryblogs.ca/2017/11/04/developing-a-Learning-Culture-a-Framework-for-Thegrowth-of-Teaching-Expertise. Accessed May 14, 2020. [Google Scholar]
- 43. Garrison DR, Anderson T, Archer W. Critical inquiry in a text-based environment: computer conferencing in higher education. Internet High Educ. 1999;2:87–105. [Google Scholar]
- 44. Garrison DR. Communities of inquiry in online learning In: Encyclopedia of Distance Learning. 2nd ed. Hershey, PA, USA: IGI Global; 2009: 352–355. [Google Scholar]
- 45. Anderson T, Liam R, Garrison DR, Archer W.. Assessing teaching presence in a computer conferencing context. Online Learning. 2001;5:1–17. [Google Scholar]
- 46. Garrison DR, Anderson T, Archer W. Critical thinking, cognitive presence, and computer conferencing in distance education. Am J Distance Educ. 2001;15:7–23. [Google Scholar]
- 47. Transformation, technology, and education. Puentedura RR. http://hippasus.com/resources/tte/. 2006. Accessed May 14, 2020.
- 48. DPT 6350: management of the pediatric patient. Baylor University https://www.baylor.edu/canvas/. Spring; 2020. Accessed May 14, 2020. [Google Scholar]