

Abstract
Background and aims
Chronic pain is a significant health care problem which is often encountered in medical institute out-patient clinics . In previous studies we have reported on the benefits of low level laser therapy (LLLT) for chronic musculoskeletal pain patients. The present study is a report on the effects of LLLT in patients with pain in major muscles which govern the motion of two joints (2-joint muscles).
Materials and methods
Over the past 5 years, 19 subjects visited our out-patient clinic with complaints of pain in 2-joint muscles (biceps brachii muscle or gastrocnemius muscle). They were treated with LLLT using a 1000 mW semi-conductor laser device delivering 20.1 J/cm2 per point at 830 nm in continuous wave. Four shots were given per session (1 treatment) twice a week for 2 months (total of 16 treatments).
Results
A treatment approach modified from the methods of Shiroto and Ohshiro, was used, and the efficacy of LLLT for pain attenuation in the affected muscle was determined. After the end of the treatment regimen, excellent and good improvement was observed in 16 patients out of 19. Discussions with the patients revealed that it was important for them to learn how to modify their everyday life to avoid posture and activities of daily life that could cause them pain in the 2-joint muscles, in order to enjoy continuous benefits from the treatment.
Conclusion
The present study demonstrated that LLLT was an effective form of treatment for pain in the biceps brachii and gastrocnemius muscles. To maximize and prolong treatment efficacy, advice should be given to patients to avoid adopting any posture and activities of daily living which would cause pain in these specific muscles.
Keywords: Low Level Laser Therapy, two-joint muscle pain, biceps brachii muscle, gastrocnemius muscle, postural education, advice for activities of daily living
Introduction
Muscles are attached to bones in a characteristic manner with specific insertion joints. Each muscle exerts a pull across the joint, and the action line of the muscle in relation to the joint determines the movement which will be produced within the limitations of the joint structure. There are three identifiable types of muscle contraction designated according to the change in muscle length: isometric, isotonic and eccentric contraction. In isometric contraction, no change of muscle length occurs during the contraction. Under the current definition, an isometric contraction is one in which the external length of the muscle remains unchanged, and is called static contraction. An isotonic contraction occurs when a muscle contracts, the muscle length changes and the joint angle changes. The muscle shortens producing joint movement, this is called a shortening contraction. In eccentric contraction, the muscle is allowed to lengthen while continuing to maintain muscle tension, and this is called lengthening contraction. In the usual activities of daily living (ADL), eccentric contractions in joint movement are common. Examples include squatting or lying down, bending forward, going down stairs, stopping suddenly, placing any object down onto a surface, and so on. Muscles associated with two joints with long moment arms, even when the limbs are in the anatomical position, are for the most part large muscles which have the capability of exerting considerable force, two specific examples being the eccentric contraction of the biceps brachii and gastrocnemius muscles.
We have occasionally experienced patients with pain caused by eccentric contraction of these two-joint muscles. The present study was designed to evaluate the efficacy of low level laser therapy for chronic pain in these two specific muscles due to misuse or overuse.
Subjects and Methods
1: Subjects
Nineteen patients (9 males and 10 females) between the age of 20 and 83 (average age 50.2 ± 18.8) took part in this study. All subjects were out-patients who visited the rehabilitation department of our hospital between April, 2012 and March, 2017 (Table 1). All patients visited the out-patient clinic within one week of onset of pain. They all had a definitive diagnosis of muscle tenderness in the biceps brachii (11 patients) or gastrocnemius muscles (8 patients) for which surgery was not indicated. Diagnosis was based on physical symptoms: complaints caused by chronic sports trauma and misuse or overuse of eccentric muscle contraction in the activities of daily life.
Table 1: Patient demographics, diagnoisis, VAS scores and Evaluation.
| Cases | Age | Sex | Diagnosis | Pre.VAS score | Post VAS score | Improvement of VAS Score | Evaluation |
|---|---|---|---|---|---|---|---|
| 1 | 58 | M | BB | 70 | 65 | 5 | P |
| 2 | 50 | M | BB | 70 | 55 | 15 | F |
| 3 | 83 | M | BB | 100 | 50 | 50 | E |
| 4 | 24 | M | BB | 70 | 50 | 20 | G |
| 5 | 62 | F | BB | 90 | 70 | 20 | E |
| 6 | 23 | F | BB | 100 | 40 | 60 | E |
| 7 | 43 | M | BB | 90 | 50 | 40 | E |
| 8 | 67 | F | BB | 50 | 30 | 20 | G |
| 9 | 70 | M | BB | 50 | 20 | 30 | G |
| 10 | 59 | F | BB | 100 | 70 | 30 | G |
| 11 | 45 | M | BB | 75 | 65 | 10 | P |
| 12 | 55 | F | G | 70 | 30 | 40 | E |
| 13 | 67 | F | G | 80 | 20 | 60 | E |
| 14 | 33 | F | G | 60 | 10 | 50 | E |
| 15 | 57 | F | G | 70 | 30 | 40 | E |
| 16 | 25 | M | G | 70 | 40 | 30 | G |
| 17 | 73 | F | G | 70 | 30 | 40 | E |
| 18 | 20 | F | G | 50 | 5 | 45 | E |
| 19 | 40 | M | G | 90 | 20 | 70 | E |
VAS: Visual Analogue Scale BB: Biceps brachii muscle
Evaluation: Table 3 G: Gastrocnemius muscle
2: Methods
We used a 1000 mW semiconductor laser device, the MDL 2001 (Matsushita Electric Corporation, Tokyo Japan), delivering 830 nm in continuous wave. We treated the 19 patients with the laser system for each session at an energy density per 30 s treatment of 20.1 J/cm2 (Table 2). Four points were irradiated (Figure 1) per session (comprising 1 treatment) twice a week for 2 months (total 16 treatments). No medication was used, because in the present study we wished to assess the effectiveness of the LLLT intervention on its own. The study was conducted under the principles of the Declaration of Helsinki (2013). The trail was conducted with the approval of the Ethics Committee of the Toho University School of Medicine, Institutional Review Board (IRB). The purpose and potential outcomes of the trial were explained to all participants, and they gave written informed consent to participate the study.
Table 2: Specification and characteristics of the LLLT device used in the present study.
| Laser Element | : Laser Semiconductor Diode Ga-Al-AS: Gallium -Aluminum-Arsenide |
| Model & Manufacturer | : MDL9001 (#) Matsushita Electric Corporation, Tokyo, Japan |
| Wavelength | : 830 nm ± 15 nm |
| Output | : 1000 mW ± 20% |
| Mode | : Continuous wave mode Contact mode with positive pressure |
| Irradiation area | : diameter: 14 mm: treatment area, 1.5 cm2 |
| Irradiation time | : 30 s |
| Energy density | : 20.1 J/cm2 |
| Power supply | : 100 AC, 50–60 Hz |
Figure 1:
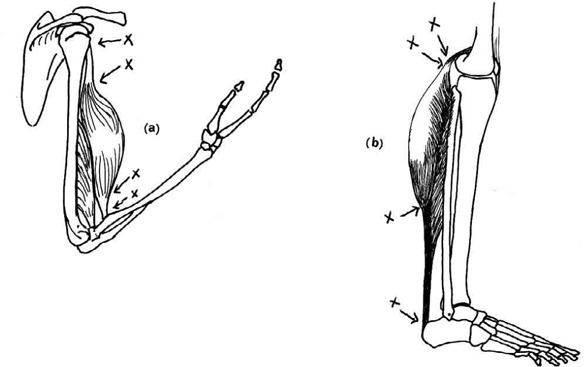
A schematic illustration of the biceps brachii (a) and gastrocnemius muscles (b).
(x: irradiation points)
Evaluation of Muscle Pain Attenuation
A treatment approach modified from the methods of Shiroto and Ohshiro, was used to determine the effects of LLLT for the pain attenuation in the 2-joint muscles. 1) Pain was scored using a visual analog scale (VAS) where 100 was the worst possible pain and zero was no pain.
Lifestyle guidance for the patients:
Patients were advised to continue their normal activities of daily living (ADL). However, we give them written advice sheets on maintaining a good posture to avoid any trigger position related with pain in eccentric muscle contraction in everyday life.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 24, IBM Company. The Wilcoxon signed rank test was applied to compare the VAS scores before and after LLLT. The level of significance was set at ≤ 0.05.
Results
Evaluation of pain relief efficacy in the biceps brachii and gastrocnemius muscles
The VAS scores at baseline and the final assessment are shown in Table 1 and summarized in Table 3. The results were Excellent in 11 patients, Good in 5, Fair in 1, Poor in 2 and Worse in 0. No side effects were noted and pain was not exacerbated in any patient. The average VAS score before treatment 75.0 ± 16.4, and after treatment the average VAS score was 39.7 ± 20.1.
Table 3: Evaluation of the VAS score.
| Evaluation | Improvement of the VAS score after LLLT | Number of Cases |
|---|---|---|
| • Excellent (E) | 35 and over | 11 |
| • Good (G) | 20–34 | 5 |
| • Fair (F) | 15–19 | 1 |
| • Poor (P) | 14 or under | 2 |
| • Worse (W) | 0 |
Evaluation of efficacy with the VAS score: most severe pain scored at 100, pain free scored at zero.
See Table 1 for individual scores and evaluations.
Results of statistical analysis
The VAS score after LLLT was highly significantly lower than the score before LLLT (0.0001).
Patient Lifestyle Guidance
Patients were advised to avoid adopting any posture that could induce pain, and we counselled the patients how to avoid incorrect positions which could exacerbate discomfort or pain in the biceps brachii and gastrocnemius muscles during their normal ADL, as already mentioned in the Subjects and Methods. After discussions with the patients, it was reported in all cases that the lifestyle guidance was well understood, and the advice that was given was realized. However, in the score-sheet filled out by patients after the treatment, there were some patients who did not precisely follow the lifestyle guidelines, therefore statistical analysis was not performed on this parameter.
Discussion
The attachments of a skeletal muscle are its origin and insertion; anatomically the origin is the more proximal attachment and the insertion is the more distal attachment. A single joint muscle (SJM) involves one joint, on the other hand, a two-joint muscle (TJM) extend over two joints (referred to as 2-joint muscles in the present study). SJMs affect one joint, and TJMs affect two joints of the skeleton affecting their work efficiency, but sometimes we have some cases where chronic pain has resulted from the overuse, misuse or incomplete sport injury involving 2-joint muscles. For example, when the upper arm is moved forward, tension developing in the biceps brachii contributes, simultaneously, to flexing the elbow and rotating the forearm. When the knee is moved backward, tension in the gastrocnemius contributes, simultaneously, to flexion of the knee and dorsiflexion of ankle joint 2, 3).
Therefore, the complex mechanics associated with TJM action compared with SJM involvement are obvious. Because of these complex rotational forces, cases of chronic pain associated with TJM misuse/overuse are not uncommon. As mentioned above, we experience two-joint muscle pain in daily life. In many cases, pain can develop in the biceps brachii (BB) muscle and gastrocnemius (G) muscle pain due to overuse, misuse, a variety of exercise activities, sports and so on. From our experience, in these chronic cases of BB and G muscle pain the site most prone to pain has been the transitional portion between the muscle and tendon.
In general, this site of interest is located close to the area where the muscle is attached to the bone. From the standpoint of posture control, when the posture is such that the body fails to follow the line denoting its center of gravity, chronic pain is more liable to develop in the muscles involved. There has been a lot of basic research 4, 5, 6), and many clinical studies 7, 8, 9, 10, 11, 12, 13) carried out involving LLLT. Some previous reports have discussed the type of LLLT device 14), wavelength-specific benefits 15) and evaluation of treatment methods. Recently, basic research on LLLT is gaining validity. As an example of this, if a PubMed search is carried out using ‘LLLT’ as the keyword, over 5,700 results will be displayed.
There are various possible explanations for the positive effects of LLLT treatment 16, 17, 18). The authors believe that a rise in the pain threshold, improved blood flow and regeneration of the compromised structure of 2-joint muscle are the main contributing factors 19, 20).
In this study, we treated the disease with LLLT irradiation, as one of the tools available in physical therapy. LLLT is simple and easy to administer without any side effects. Regarding the evaluation of pain, a statistically significant effect was observed in the VAS scores after irradiation (p < 0.0001).
However, one limitation of this cross-sectional study was the lack of a demographically-matched control and or placebo (sham irradiation) group. Another limitation is the lack of a long-term follow-up after the final treatment session to assess the latency of the efficacy. To validate the results of this study, such controlled and placebo studies with a long-term follow-up are required and warranted in the future.
Conclusion
The present study demonstrated that LLLT was an effective form of treatment for 2-joint muscle pain. Patients should be advised regarding adopting an inappropriate posture and inappropriate activities of daily living which could result in developing 2-joint muscle pain, or exacerbating such preexisting pain. Therefore, for patients to continue to reap the benefits of LLLT intervention, we discovered that education regarding posture during patients' ADL was also very important.
References
- 1: Shiroto Chiyuki, Ohshiro Toshio. (2014). A new standard of Efficacy for Low Level Laser Therapy (LLLT) in Pain Attenuation in Japan. Laser Therapy 23:183-190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2: Rasch P. (1989). Kinesiology and Applied Anatomy. edi 7, Lea & Febiger, Philadelphia. [Google Scholar]
- 3: Lippert L. (1994). Clinical Kinesiology for Physical Therapist Assistants. edi 2, F.A. Davis Company, Philadelphia. [Google Scholar]
- 4: Tsuchiya K, Kawatani M, Takeshige C. (1994). Laser irradiation abates neuronal responses to nociceptive stimulation of rat-paw skin. Brain Res Bull 34:369-374. [DOI] [PubMed] [Google Scholar]
- 5: Maekawa Y, Hosokawa T, Itoh T. (2000). Effects of near infrared low level laser irradiation on microcirculation. Laser Surg Med 27:427-437. [DOI] [PubMed] [Google Scholar]
- 6: Knobloch K, Kraemer R, Jagodzinski M. (2007). Eccentric training decreases paratenon capillary blood flow and preserves paratenon oxygen saturation in chronic Achilles tendinopathy. J Orthop Sports Phys Ther 37:269-276. [DOI] [PubMed] [Google Scholar]
- 7: Saito K, Katagiri T, Ogawa M, Matsumoto S, Kubota J, Ohshiro T, Tsukamoto T, Nakaji S, Umeda T. (2005). Effects of Diode Laser Irradiation on Superficial Blood Flow in College Sumo Wrestlers: A Preliminary Study. Laser Therapy 14:83-86. [Google Scholar]
- 8: Stergioulas A, Stergioula M, Aarskog R. (2008). Effects of low level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic Achilles tendinopathy. Am J Sports Med 36:881-887. [DOI] [PubMed] [Google Scholar]
- 9: Tumilty S, Munn J, Abbot JH. (2008). Laser therapy in the treatment of Achilles tendinopthy: a pilot study. Photomed Laser Surg 26:25-30. [DOI] [PubMed] [Google Scholar]
- 10: Takashima N. (2011). Sport injury of the foot and physical therapy. Medical Rehabilitation 128:41-49(in Japanese). [Google Scholar]
- 11: Macias MD, Coughlin MJ, Zang K. (2015). Low Level Laser Therapy at 635nm for Treatment of Chronic Plantar Fascilitis: A Placebo-Controlled,Randomized Study. J Foot Ankle Surg 54:768-772. [DOI] [PubMed] [Google Scholar]
- 12: Notarnicola A, Macagnano G, Tafuri (2014). CHELT therapy in the treatment of chronic insertional Achilles tendinopathy. Lasers Med Sci 29:1271-1225. [DOI] [PubMed] [Google Scholar]
- 13: Jastifer JR, Catena F, Doty JF, Stevens F, Coughlin MJ. (2014). Low Level Laser Therapy for the Treatment of Chronic Plantar Fasciitis: A Prospective Study. Foot Ankle Int 35:566-571. [DOI] [PubMed] [Google Scholar]
- 14: Akai M. (2006). Effects of LLLT from a viewpoint of EBM. Japan Laser Therapy Association 5: 20-24(in Japanese). [Google Scholar]
- 15: Silveira PC, Silva LA, Freitas TP, Latini A, Pinbo RA. (2011). Effects of low power laser irradiation at different wavelengths and doses on oxidative stress and fibrogenesis parameters in an animal model of wound healing. Laser Med 26:125-131. [DOI] [PubMed] [Google Scholar]
- 16: Rowe V, Hemmings S, Barton C, Malliaras P, Maffulli N, Morrissey D. (2012). Conservative management of midportion Achilles tnedinopathy. Sports Med 42:941-967. [DOI] [PubMed] [Google Scholar]
- 17: Whittaker P. (2004). Laser acupuncture; past, present and future. Laser Med Sci 19:69-80. [DOI] [PubMed] [Google Scholar]
- 18: Hosokawa T, Kawatani Y. (2012). Pain treatment with low reactive level laser therapy. Masui 6:718-727(in Japanese). [PubMed] [Google Scholar]
- 19: Yachnev IL, Plakhova VB, Podzorova SA. (2012). Mechanism of pain relief by low-power infrared irradiation: ATP is an IR-target molecule in nociceptive neurons. Med Chem 8:14-21. [DOI] [PubMed] [Google Scholar]
- 20: Chen CH, Tsai JL, Wang YH. (2009). Low-level laser irradiation promotes cell proliferation and mRNA expression of type 1 collagen and decorin in porcine Achilles tendon fibroblasts in vitro. J Orthop Res 27:646-650. [DOI] [PubMed] [Google Scholar]