

Abstract
Recent media articles have suggested that women-led countries are doing better in terms of their responses to the COVID-19 pandemic. We examine an ensemble of public health metrics to assess the control of COVID-19 epidemic in women-versus men-led countries worldwide based on data available up to June 3. The median of the distribution of median time-varying effective reproduction number for women- and men-led countries were 0.89 and 1.14 respectively with the 95% two-sample bootstrap-based confidence interval for the difference (women – men) being [−0.34, 0.02]. In terms of scale of testing, the median percentage of population tested were 3.28% (women), 1.59% (men) [95% CI: (−1.29%, 3.60%)] with test positive rates of 2.69% (women) and 4.94% (men) respectively. It appears that though statistically not significant, countries led by women have an edge over countries led by men in terms of public health metrics for controlling the spread of the COVID-19 pandemic worldwide.
Keywords: Public health, public policy
INTRODUCTION
The remarkable success of the chancellor of Germany Angela Merkel, the prime minister of New Zealand Jacinda Ardern, the prime minister of Finland Sanna Marin, the Icelandic prime minister Katrín Jakobsdóttir and the president of Taiwan, Tsai Ing-Wen in controlling the COVID-19 pandemic has received much attention [1][2]. There has been a wave of articles in the media that applaud the COVID-19 response efforts in women-led countries [3] along with the promotion of progressive policies which would reduce severe COVID-19 outcomes [4]. A recent preprint [5] investigates if there are any significant and systematic differences in COVID-outcomes of men and women-led countries in the first quarter of the pandemic. The authors compare country specific COVID-outcomes (specifically, COVID-cases and COVID-deaths) up to May 19 for 194 countries, using a variety of socio-demographic variables (such as GDP per capita, population, size of urban population and of elderly, health expenditure and openness to tourism) to match pairs of women- and men-led countries. The nearest neighbor matching method pairs each women-led country in the sample with its closest comparator and estimates the effect of being women-led on COVID-outcomes. The authors report that controlling for various socio-demographic factors, women-led countries perform significantly better than men-led countries. However, the efficiency of this matching process is attenuated by the imbalance in the number of women-led countries (19) in the dataset, as compared to a much larger number (175) of men-led countries in the dataset. In our opinion, raw case and death counts are poor descriptors of the control of the pandemic over time and focus on more informative public health metrics in our analyses.
In this note, we attempt to quantify the effect of women leaders more broadly across the world in terms of public health and policy relevant measures that have been widely discussed in the last three months for controlling a pandemic. Instead of qualitative comparisons and statements, we assess statistical significance of the hypotheses that performance is indeed different between women and men heads of nations.
METHODS
Since the world is full of data, we use data from the Johns Hopkins COVID-19 data repository [6] to carry out a two-group comparison of countries led by men and women. The list of countries with women leaders was retrieved from Wikipedia [7]. Comparison between women- and men-led countries is done without differentiating whether each woman was a governing leader, such as Bolivia’s president Jeanine Áñez, or serving in more of a titular role, such as Nepal’s president Bidhya Devi Bhandari. We restrict our analysis to countries with at least 100 cumulative reported cases of COVID-19 infections and at least 10 days of reported data as of June 3, 2020. Of the 159 countries so chosen, 18 have women heads of state (Table 1) while the other 141 have men heads of state.
Table 1.
Summary case-count, death count and testing data for 18 countries led by women.
| Country (Head of Nation) | Total number of tests per 100,0001,2 | Total number of cases per 100,0001,2 | Pct. (%) of population tested1,3 | Pct. (%) of test positive cases1,4 | Total number of deaths per 100,0001,2 |
|---|---|---|---|---|---|
| Bangladesh (Sheikh Hasina) | 167.45 | 23.25 | 0.17 | 13.89 | 0.45 |
| Belgium (Sophie Wilmès) | 5681.92 | 494.77 | 5.68 | 8.71 | 82.16 |
| Bolivia (Jeanine Áñez) | 214.73 | 61.13 | 0.21 | 28.47 | 3.43 |
| Denmark (Mette Frederiksen) | 8291.13 | 197.3 | 8.29 | 2.38 | 10.01 |
| Estonia (Kersti Kaljulaid) | 6085.38 | 138.25 | 6.09 | 2.27 | 5.20 |
| Ethiopia (Sahle-Work Zewde) | 84.00 | 0.64 | 0.08 | 0.76 | 0.01 |
| Finland (Sanna Marin) | 3187.53 | 119.62 | 3.19 | 3.75 | 5.79 |
| Germany (Angela Merkel) | 4718.05 | 212.79 | 4.72 | 4.51 | 10.27 |
| Greece (Katerina Sakellaropoulou) | 1635.48 | 27.85 | 1.64 | 1.70 | 1.72 |
| Iceland (Katrín Jakobsdóttir) | 17611.72 | 528.64 | 17.61 | 3.00 | 2.93 |
| Nepal (Bidhya Devi Bhandari) | 200.01 | 2.65 | 0.20 | 1.32 | 0.03 |
| New Zealand (Jacinda Ardern) | 5634.11 | 23.93 | 5.63 | 0.42 | 0.46 |
| Norway (Erna Solberg) | 4474.95 | 154.63 | 4.47 | 3.46 | 4.37 |
| Serbia (Ana Brnabić) | 3372.5 | 164.99 | 3.37 | 4.89 | 3.60 |
| Singapore (Halimah Yacob) | 3743.3 | 540.41 | 3.74 | 14.44 | 0.41 |
| Slovakia (Zuzana Čaputová) | 3035.25 | 27.75 | 3.04 | 0.91 | 0.51 |
| Myanmar (Aung San Suu Kyi) | 41.89 | 0.38 | 0.04 | 0.90 | NA |
| Taiwan (Tsai Ing-wen) | 300.55 | 1.85 | 0.30 | 0.62 | NA |
Note:
As of June 3rd, 2020. Some countries release testing data one week after testing.
Figures reported are per 100,000 of population size.
Calculated as 100 × (total number of tests/population size).
Calculated as 100 × (total number of positive cases/total number of tests).
We first create a plot of the effective time-varying reproduction number at time t, namely, R(t) [8] for all 159 countries (Figure 1). Time zero in the figure is defined as the day when each country crossed at least 50 cases. We construct smoothed trajectories of median R(t) across countries, stratified by gender of head of state. We calculate the mean, median and maximum R(t) over the course of the pandemic (from time zero till June 3) for each country based on the computed R(t) trajectories. We also consider the most recent value of R (on June 3) to gauge where we stand now. We present density plots of these summaries stratified by gender of head of state, along with most recent values of country-level effective R (Figure 2). We create a forest plot of country-specific medians and associated 95% confidence intervals (CI) of R(t) values over the course of the pandemic (Figure 3).
Fig. 1.
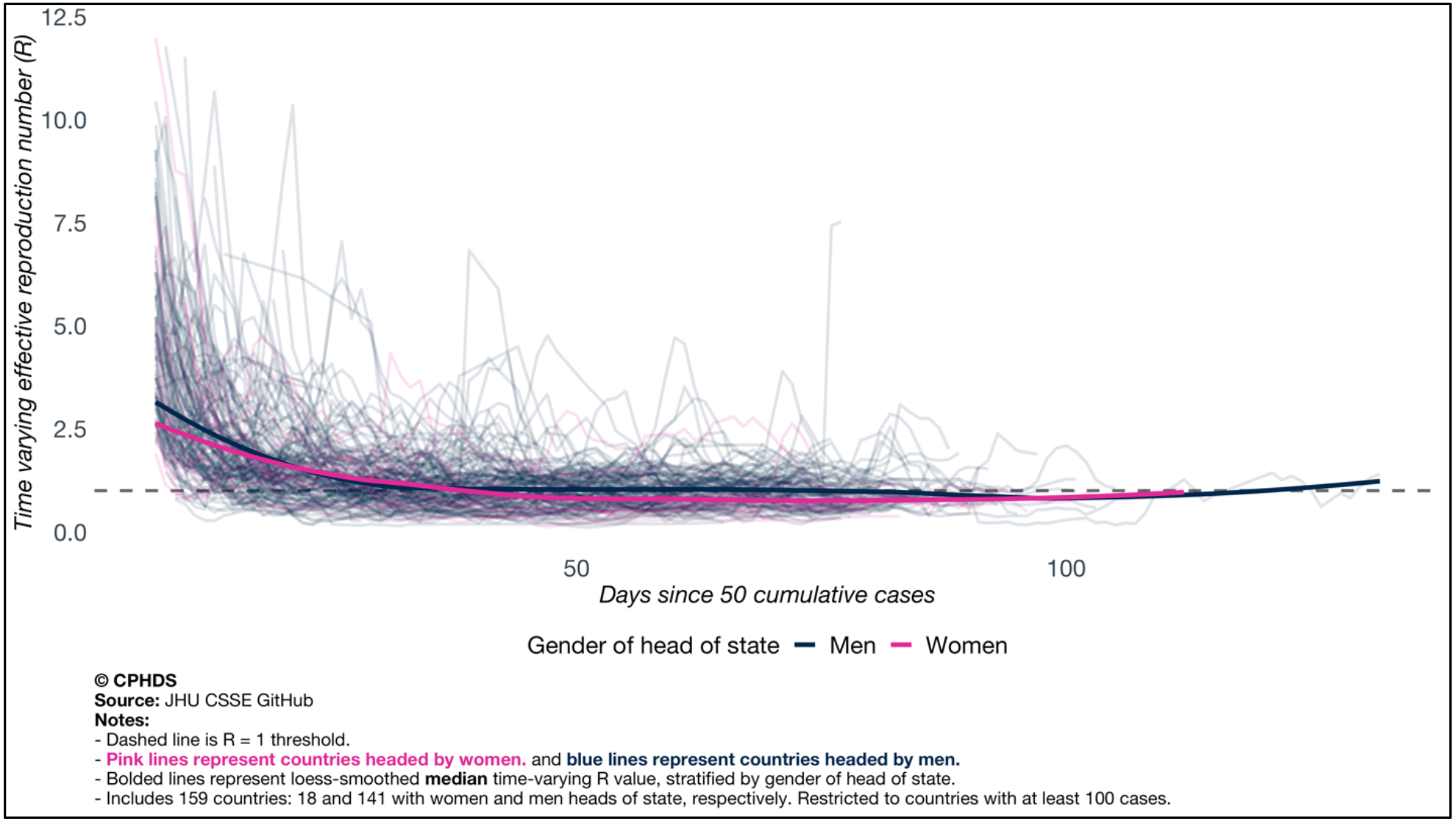
Time varying plot of the effective time varying reproduction number of all 159 countries, with locally smoothed trajectories of median of time-varying reproduction number, stratified by gender of head of state.
Fig. 2.
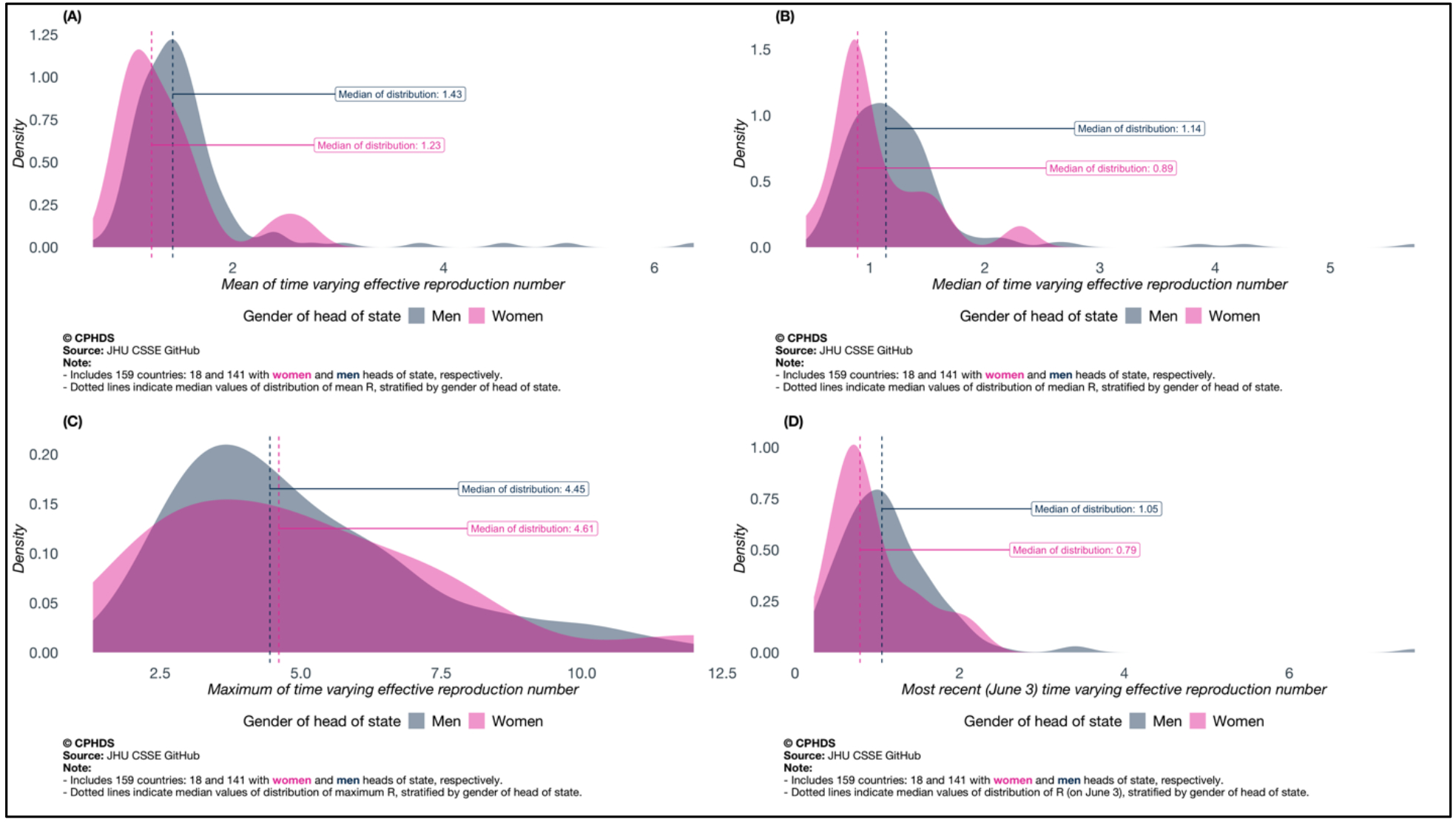
Distributions of (A) mean, (B) median, (C) maxima and (D) most recent values of time-varying reproduction number, stratified by gender of head of state. Mean, median, maximum are taken over the time course with time zero defined as the day the reported counts crossed 50 and the last day considered is June 3.
Fig. 3.
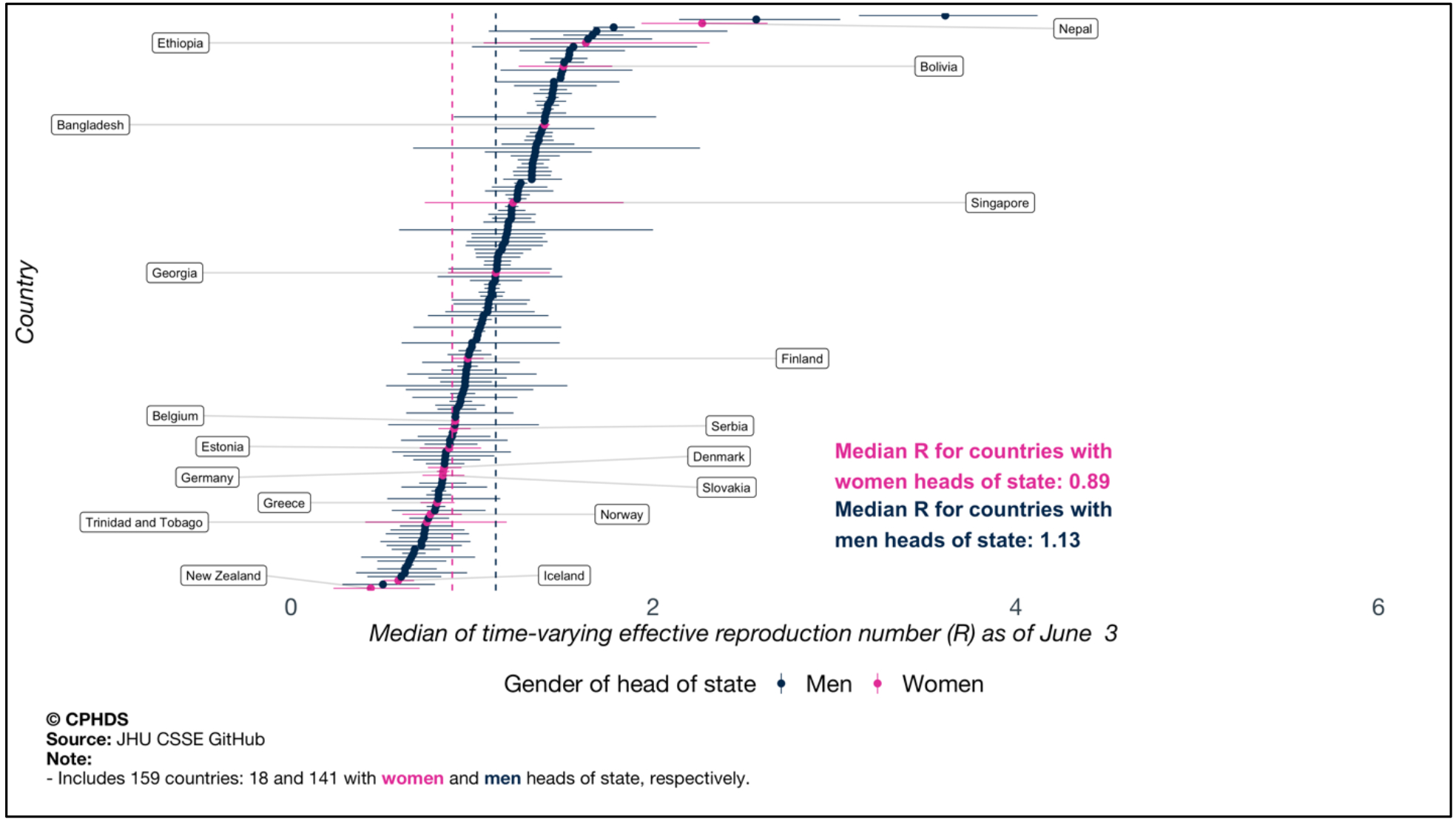
Forest plot of country-specific median and associated 95% CI of time-varying effective reproduction number R, stratified by gender of head of state.
In addition to visual inspection, we do some formal statistical inference. Since the sample sizes of the two groups are unbalanced (18 versus 141) and the distributions are visibly not normal-like, we use resampling procedures. For median, mean, maximum and most recent (as of June 3) values of time-varying R(t), we perform a two-sample bootstrap procedure-based comparison of medians and construct 95% CI based on empirical 2.5th and 97.5th percentile of the bootstrap distributions.
We also consider the doubling time (DT) metric and case-fatality rate (CFR) metric under the same analytical lens. To evaluate the scale of diagnostic testing to identify new COVID-19 cases, we compare 85 countries which have released testing data (67 led by men and 18 led by women) on the basis of two metrics: percentage of population tested and percentage of positive tests. We present clustered bar plots comparing percentage of population tested and percentage of positive tests for these 85 countries (Figure 4).
Fig. 4.
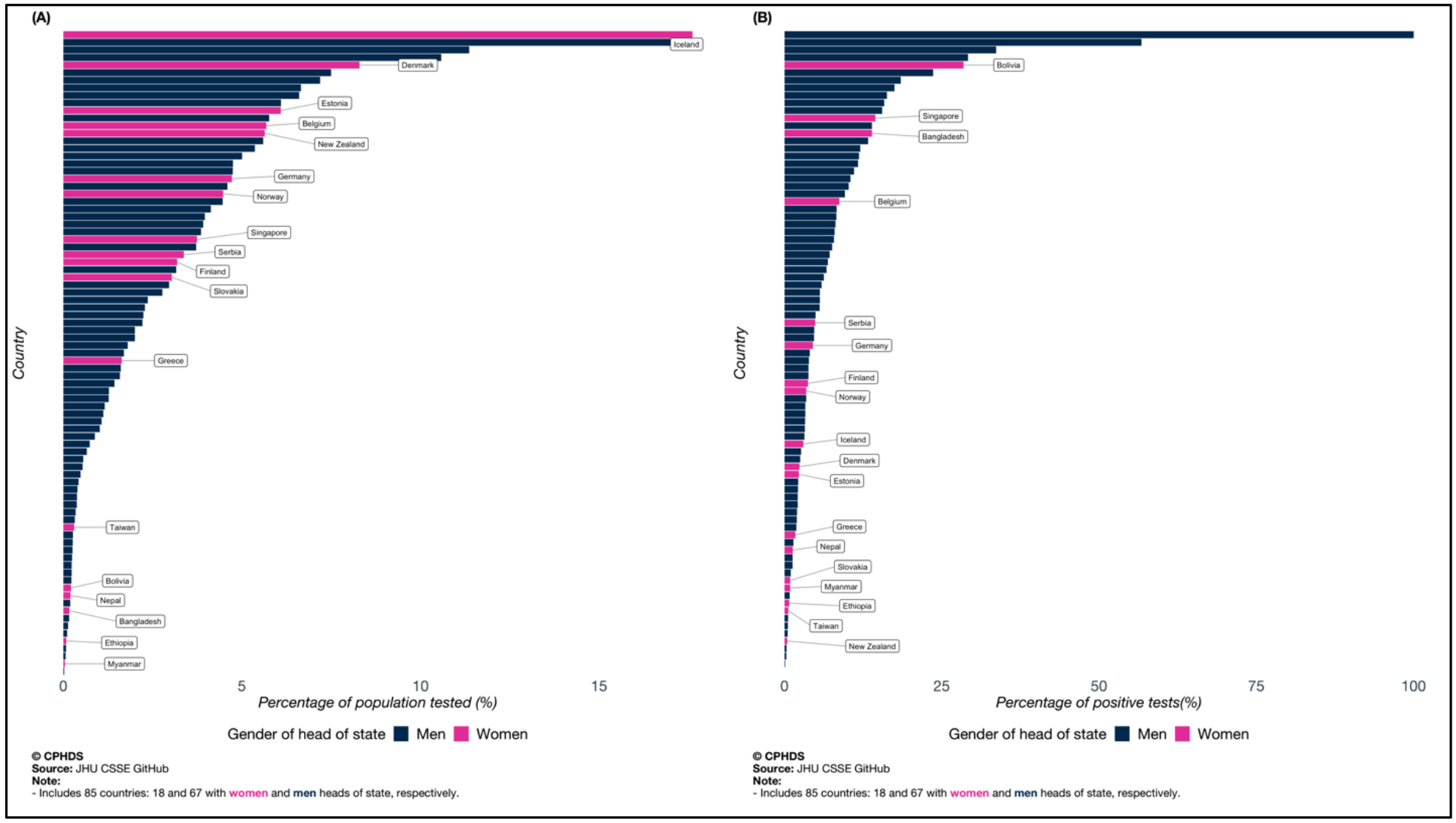
Bar plots of country-specific testing data (A: percentage of population tested and B: percentage of positive tests), stratified by gender of head of state.
RESULTS
Table 1 presents a snapshot of the raw data for the 18 countries led by women in terms of numbers of cases and deaths per 100,000 population, percentage of population tested and percentage of test positives. There is significant variation across countries and continents. Figure 1 presents the median trajectory of the time-varying reproduction number R through the time-course of the pandemic and it shows lower trend for the trajectory for countries led by women. Figure 2 reveals a shift in the gender-stratified distributions of median, mean, maximum and most recent values of R(t) --- they have more probability weight towards smaller values for the women (lower the R, slower is the transmission). Comparing the two distributions (women vs men) on the basis of median of time-varying R(t) yields a median value of 0.89 for women and 1.14 for men. Values of R below one are desirable. The bootstrap procedure comparing difference of median (women-men) yields a 95% CI of [−0.34, 0.02]. Similar comparisons between gender-stratified distributions of mean of time-varying R(t) yields a median of 1.23 for women and 1.43 for men and a 95% CI of the difference as [−0.39, 0.07]. Comparing maximum of the time-varying R(t) yields a median value of 4.61 for women and 4.45 for men, with the 95% CI for their difference given by [−1.60, 1.65]. A group-wise comparison of most recent R(t) (as of June 3) yields a median of 0.79 for women and 1.05 for men, with 95% CI [−0.42, 0.09]. From Figure 3, we note that most women-led countries have median R(t) values towards the lower end of the scale. It appears that in terms of all features (barring the maximum) of the time varying reproduction number curve, women are ahead, but since all the confidence intervals contain zero, the results are not statistically significant at 5% level of significance.
Comparing the gender-stratified distribution of median of country-specific doubling times (longer is better for slowing down the virus), we note a similar pattern, with the distribution for women-countries having more mass on longer doubling times than men-led countries – with 16.6 and 16.1 days as the median values of doubling time for women and men respectively (the 95% bootstrap CI of the median difference of the two distributions is [−0.77, 3.17] days). The same goes for case-fatality rates (lower is better), women-led countries have lower median case-fatality rate, with the median for countries with women heads of state being 2.46%, while that for countries with men heads of state is 2.73%. Comparing CFRs stratified by gender of head of state by a two-sample bootstrap procedure yields a 95% CI of the median difference given by [−1.4%, 1.8%].
We know that extensive testing and contact tracing is key benchmark for success in this public health crisis. A comparison of percentage of population tested between the two groups yields median values of 3.28% and 1.59% for women- and men-led countries respectively (more testing is better). The 95% CI estimate of the difference of medians is [−1.29%, 3.60%]. Comparing women and men leaders on the basis of another testing metric – percentage of positive tests (lower is better) – yields a median 2.69% and 4.94% for women and men respectively, with [−4.89%, 0.30%] as the 95% CI of the difference of median values. Figure 4 shows a visual overview of testing and we see countries led by women having on balance, more testing and lower test positives.
DISCUSSION
Comparing three measures summarizing the trajectory of time varying reproduction number R(t) as well as most recent values of R(t), we note that the group of countries led by women appear to have better public health metrics measuring spread of the virus, although the median difference between the two groups of countries is not statistically significant. A similar comment can be made while investigating group-differences of doubling time and case-fatality rates. As far as scale of testing is concerned, we note that countries with women heads of state tend to do better with more testing and lower test positive rates, although this difference is again, not statistically significant.
An interesting observation here is that all 18 countries with women heads of state included in our analysis are releasing testing data whereas only 67 out of the 141 countries led by men have testing data available. One main limitation is the lack of power in the analysis, which is largely due to the small number of countries led by women. The unbalanced nature of the group sizes (18 vs 141) makes it difficult to design efficient matched analysis methods by stratifying countries with similar socioeconomic and demographic profile and conducting a matched pair analysis between the two groups. Sensitivity analysis when restricted to countries where the head of state took executive decisions extended the gender gap but reduced sample size. It is also true that many key members of the cabinet often contribute to the success of the government in a crisis. The ministry of health and home affairs are instrumental in implementing and managing policies for controlling the virus. We have not taken those factors into account, some of which may be hard to quantify.
CONCLUSION
This unadjusted ecological analysis is obviously wrinkled with several limitations and potential confounding that makes it impossible to conclude the causal impact of women leaders on pandemic outcomes. Several common causes can influence this pattern. However, it is clear that political leadership was critical for managing this public health crisis, coordinating different key sectors: namely, public health, health care, social support and economic recovery was of paramount importance. Leaders who have been able to bring the different arms of the government, the public, and the scientific experts to rally around a greater good beyond mere politicization of policies have shown exemplar progress. Perhaps it is not just the women leaders, but societies that are progressive and open enough to recruit diverse leaders and promote inclusive decision-making have a better chance of fighting the virus as a collective? Something to think about when we appoint and elect our future leaders.
TAKE-HOME MESSAGE:
Political leadership was critical for managing the COVID-19 health crisis, coordinating different key sectors: namely, public health, health care, social support and economic recovery was of paramount importance. Leaders who have been able to bring the different arms of the government, the public, and scientific experts to rally around a greater good beyond mere politicization of policies have shown exemplar progress. Perhaps it is not just the women leaders, but societies that are progressive and open enough to recruit diverse leaders and promote inclusive decision-making have a better chance of fighting the virus as a collective? Something to think about when we appoint and elect our future leaders.
Acknowledgments
The authors would like to thank the University of Michigan Rogel Cancer Center, Center for Precision Health Data Science, University of Michigan School of Public Health and Michigan Institute of Data Science for supporting this research: Competing interests: Authors declare no competing interests. Data and materials availability: Data sourced from public repositories. All codes are available at covind19.org.
References
- 1.Bali S, Dhatt R, Lal A, Jama A, Van Daalen K, Sridhar D, Off the back burner: Diverse and gender-inclusive decision-making for COVID-19 response and recovery. BMJ Global Health, 5(5), e002595. (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing. JAMA. 2020;323(14):1341–1342. doi: 10.1001/jama.2020.3151 [DOI] [PubMed] [Google Scholar]
- 3.Taub A, Why Are Women-Led Nations Doing Better With Covid-19? The New York Times, Retrieved May 30, 2020. https://www.nytimes.com/2020/05/15/world/coronavirus-women-leaders.html [Google Scholar]
- 4.Coscieme L, Fioramonti L, Trebeck K, Women in power: Countries with women leaders suffer six times fewer Covid deaths and will recover sooner from recession. OpenDemocracy, Retrieved May 30, 2020. https://www.opendemocracy.net/en/can-europe-make-it/women-power-countries-women-leaders-suffer-six-times-fewer-covid-deaths-and-will-recover-sooner-recession/
- 5.Garikipati S, & Kambhampati U (2020). Leading the Fight Against the Pandemic: Does Gender ‘Really’Matter?. Available at SSRN 3617953.
- 6.Johns Hopkins University, COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Retrieved June 3, 2020. https://coronavirus.jhu.edu/map.html [Google Scholar]
- 7.List of elected and appointed female heads of state and government, Wikipedia, Retrieved May 30, 2020. https://en.wikipedia.org/wiki/List_of_elected_and_appointed_female_heads_of_state_and_government
- 8.Cori A, Ferguson NM, Fraser C, Cauchemez S, A New Framework and Software to Estimate Time-Varying Reproduction Numbers During Epidemics. American Journal of Epidemiology, 178(9), 1505–1512 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]