

Abstract
Reconstruction of long tracheal defects still proves to be a challenge. Free fasciocutaneous flaps with cartilaginous struts or an allotransplant trachea have been reported but not been widely performed. This article reports with the experience of using a tracheal allotransplant in such a defect.
A 43-year-old lady presented with adenoid cystic carcinoma involving the entire trachea from subglottic area up to the carina, leading to a life-threatening airway occlusion. After preliminary stenting, allotransplant trachea obtained from a brain-dead individual was revascularized in the forearm of the patient after mechanical decellularization to reduce the immune load and fulfil the need for immunosuppression in the background of active cancer. Subsequently, the trachea and larynx were resected. The vascularized neotrachea was transferred successfully into the neck. The patient did well initially but succumbed to a fatal hemorrhage due to innominate vein aneurysmal rupture on the 22nd day after the transplant.
The technical details of resection, fabrication of the neotrachea, its transfer, and the lessons learnt in this tracheal allotransplant are described.
Keywords: tracheal allotransplantation, composite tissue allotransplantation, revascularization
Introduction
Airway reconstruction has long posed significant challenges. For circumferential defects > 5 cm, few reconstructive options provide the structural stability required to prevent collapse during inspiration, while the rest remain pliable enough to allow neck flexion. 1 No standardized recommendations exist for reconstruction of these defects. We report our experience in tracheal allotransplantation based on the Delaere technique 2 and the lessons we learned from this procedure.
Case Report
Our patient was a 43-year old female, presenting with a 3-month history of dyspnea. Bronchoscopy showed diffuse circumferential tracheal narrowing from the subglottis to carina, with PET-CT showing disease restricted to the trachea ( Fig. 1a ). Biopsy showed adenoid cystic carcinoma.
Fig. 1.
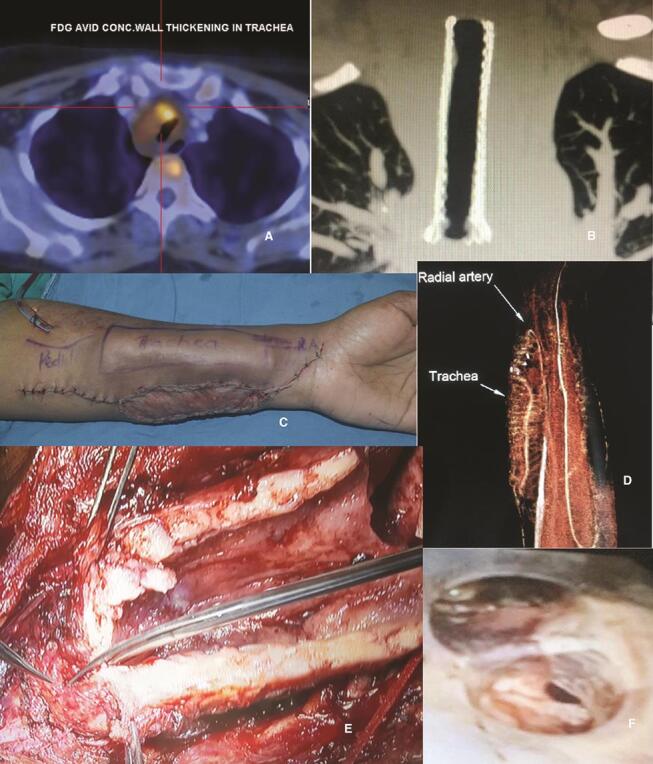
Intraoperative images as described in the text.
The treatment options were insertion of a luminal stent with palliative radiotherapy or radical resection, reconstruction and adjuvant radiotherapy 3 ; they were discussed with the patient and her family. Given her age and performance status, they wanted aggressive management and potential cure over palliative treatment.
The patient underwent temporary tracheal stenting to relive stridor ( Fig. 1b shows fluoroscopic image of stent in situ). After ethical clearance and informed consent, the procedure was undertaken. The tracheal graft was harvested from a male brain-dead donor, stored in University of Wisconsin solution and ice for transportation. Mechanical stripping of epithelium left only basal lamina intact. A radial adipofascial free flap was raised from the recipient’s right forearm and sutured to the inside of donor tracheal allograft cartilaginous framework. Anastomoses were performed to vessels of the left forearm. Part of the wound was surfaced with a skin graft ( Fig. 1c ).
Two weeks later, the left forearm showed an area of pressure necrosis for which a paraumbilical jump flap was raised, which was detached after 2 weeks. CT angiography of the allograft revealed good vessel patency ( Fig. 1d ). A Y-stent was placed to ensure luminal patency.
Seven weeks after implantation, tracheal resection and reconstruction were performed. The tumor was a circumferential growth involving the cricoid cartilage to 3 cm above the carina ( Fig. 1e ). The involved trachea was excised; however, additional margins from the subglottis were positive for tumor on frozen section, following which it was decided after discussing with the patient’s family to proceed with laryngectomy for clearance.
The tracheal allograft was harvested from the left forearm with the donor vessels. The allograft was trimmed to 10 cm, and it was placed in position to bring the proximal end at the level of the neck incision and the distal end at the level of the carinal stump. The anastomosis was performed with 3–0 polydioxanone suture (PDS) to approximate the posterior tracheal wall to the allograft, limbs of the silastic stent were threaded past the anastomotic site and anterior wall sutures were placed. Anastomosis was performed to the neck vessels. End-tracheostomy was fashioned, and closure of sternal and neck wound was performed.
She was weaned off ventilator support by the postoperative day (POD) 4. On POD12, she was extubated. On POD14, a detailed inspection of the tracheal allograft was performed, with the stent in situ ( Fig. 1f ).
On POD22, the patient had a large bout of hemoptysis. Intubation was performed; however, the source of hemorrhage was noted to be from around the neotrachea in the mediastinum. An emergency bedside sternotomy was performed to identify the source and two rents were noted in the brachiocephalic vein. The rents were isolated, and transfusions were administered; however, the patient suffered cardiac arrest and could not be resuscitated.
Discussion
Our reconstructive approach was essentially different from previous reports ( Fig. 2 shows an algorithm used in malignancy); the indication for tracheal replacement was essentially life-saving. Radiotherapy and synthetic stents or conduits would have been of palliative value only. Resection and radiation with appropriate reconstruction would be necessary to offer a cure. This necessitated the transfer of well-vascularized tissue for reconstructing the tracheal defect. For all of these reasons, tracheal allotransplantation was our procedure of choice. However, this procedure has never been performed in malignancy, with good reason. Unlike in isolated defects associated with benign disease, there were many unpredictable factors that complicated her treatment and impacted outcomes. Ideally, the procedure could have been refined with experimental models in animals; however, this was not feasible in her case.
Fig. 2.
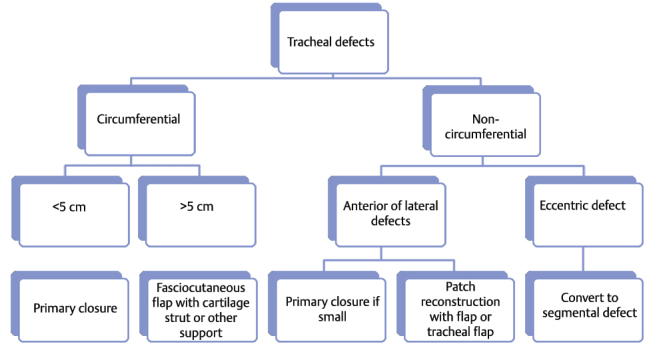
Approach to tracheal defect reconstruction following ablation for malignancy, adapted from Ch’ng et al. 4
The cause of hemorrhage from the brachiocephalic vein was likely erosion of the vessel wall from constant trickling of exudative fluid from the neotrachea into the mediastinum or minor repetitive trauma, leading to an ectatic segment and rupture. This was likely due to several factors that we had not accounted for preoperatively. First, frozen sections showed involvement of the larynx by tumor, necessitating laryngectomy for disease clearance. As a result, the neotrachea had to be exposed as an end-tracheostomy. Unlike in an end-tracheostomy performed during laryngectomy, the edges of the neotrachea could not be buried sufficiently by surrounding skin without the risk of compromising its blood supply; this resulted in a potential space around the tracheostomy, tracking down into the mediastinum. Second, the neotrachea was considerably thicker than the native trachea, because of the number of layers (cartilaginous framework, buccal mucosa and skin grafts, radial forearm, granulation tissue and the additional external lining added by paraumbilical flap). It added to the bulk of the graft, causing the neotrachea to sag forward due to its considerable weight, resulting in pressure necrosis of the edge of the tracheal cartilage overhanging the manubrium sterni. It was either exudative fluid from this necrosis, tissue fluid produced by the air-exposed external lining of the neotrachea, or leak from around the lower tracheal anastomosis that may have caused erosion of the brachiocephalic vein. Another possibility was constant erosion from the neotrachea itself, as the brachiocephalic vein was stretched over the neotrachea under slight tension due to its significant girth.
Conclusion
Although the patient did not survive, we were able to successfully vascularize the cartilaginous framework of the donor trachea and use it to successfully reconstruct the airway. Whether we would perform this procedure again in a patient requiring laryngectomy or such an extensive tracheal resection is uncertain. Careful patient selection and technical refinements may improve outcomes.
Acknowledgments
No additional acknowledgments.
Funding Statement
Financial Support No financial support was taken for this article, and there are no financial disclosures for any of the authors.
Footnotes
Conflicts of Interest There are no conflicts of interest for any of the authors.
References
- 1.Grillo H C, Donahue D M, Mathisen D J, Wain J C, Wright C D. Postintubation tracheal stenosis. Treatment and results. J Thorac Cardiovasc Surg. 1995;109(03):486–492, discussion 492–493. doi: 10.1016/S0022-5223(95)70279-2. [DOI] [PubMed] [Google Scholar]
- 2.Leuven Tracheal Transplant Group . Delaere P, Vranckx J, Verleden G, De Leyn P, Van Raemdonck D. Tracheal allotransplantation after withdrawal of immunosuppressive therapy. N Engl J Med. 2010;362(02):138–145. doi: 10.1056/NEJMoa0810653. [DOI] [PubMed] [Google Scholar]
- 3.Kanematsu T, Yohena T, Uehara T et al. Treatment outcome of resected and nonresected primary adenoid cystic carcinoma of the lung. Ann Thorac Cardiovasc Surg. 2002;8(02):74–77. [PubMed] [Google Scholar]
- 4.Ch’ng S, Palme C E, Wong G L et al. Reconstruction of the (Crico) trachea for malignancy in the virgin and irradiated neck. J Plast Reconstr Aesthet Surg. 2012;65(12):1645–1653. doi: 10.1016/j.bjps.2012.07.008. [DOI] [PubMed] [Google Scholar]