

Abstract
Revision total hip arthroplasty in the setting of acetabular bone loss is a challenging procedure and requires a solid understanding of current acetabular reconstruction options. Despite major developments in the field of revision hip surgery in recent decades, reconstruction of acetabular defects remains a major problem in order to achieve primary stability and durable fixation without sacrificing additional bone stock. Although there are several ways to classify acetabular bone defects, the Paprosky classification system is the most commonly used to describe the defects and guide treatment strategy. An understanding of the bone defects associated with detailed pre-operative assessment and planning are essential elements in order to achieve satisfactory outcomes. Multiple acetabular reconstructive options are currently available including impaction bone grafting with metal mesh, reinforcement rings and antiprotrusio cage, structural allografts, cementless hemispherical cups, extra-large “jumbo cups”, oblong cups, modular porous metal augments, cup-cage constructs, custom- made triflange cups, and acetabular distraction. To date, debate continues as to which technique is most effective due to the lack of long-term studies of modern reconstruction systems. Further long-term studies are necessary to assess the longevity of the different implants. The purpose of this study was to review the current literature and provide a comprehensive understanding of the available reconstruction options with their clinical outcomes.
Key words: Spinopelvic alignment, total hip arthroplasty, hip-spine, pelvic tilt, dislocation
Introduction
Revision total hip arthroplasty (THA) often involves bone loss that can represent a complex reconstructive challenge for the treating surgeon.1-7 Considering the rising number of primary THA, with a projected growth of 174% by 2030, the number of revisions associated with acetabular bone loss will grow as well.8 The goals of acetabular reconstruction in the setting of bone loss are the stability of the acetabular component and the restoration of the center of rotation of the hip joint in order to obtain a stable long-term mechanical fixation and prevent component migration, loosening and dislocation.2,3,9-13 To achieve these goals, a correct understanding of the bone defect and its classification are mandatory for a precise preoperative planning and proper reconstruction option.
Acetabular bone defects have been reconstructed using several cemented and uncemented methods including impaction bone grafting with metal mesh, reinforcement rings and antiprotrusio cage, structural allografts, cementless hemispherical cups, extra-large “jumbo cups”, oblong cups, modular porous metal augments, cup-cage constructs, custom-made triflange cups, and acetabular distraction.14 The choice to select a particular reconstruction option is often based on the defect type and severity, implants availability and surgical expertise.
The aim of this review is to provide a comprehensive understanding of the different acetabular reconstruction options and their clinical outcomes.
Classification of acetabular bone defects
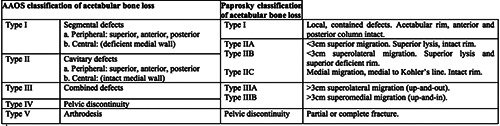
There are several published classification systems for acetabular bone defects in THA.15-17 The two most commonly cited classifications are those by D’Antonio (AAOS classification)16 and Paprosky.15
The American Academy of Orthopedic Surgeons (AAOS) acetabular bone loss classification system was introduced in 1989 by D’Antonio and associates. In this system, defects are divided into five progressive types and based into two categories: segmental (complete loss of the supporting bone) and cavitary defects (volumetric loss of the bony substance). A type I defect is defined as a minor segmental defect and can be peripheral (superior, anterior, posterior) or central (with deficient medial wall). A type II defect is defined as a cavitary defect as well divided in peripheral (superior, anterior, posterior) or central (with an intact medial wall). A Type III defect is a combination of segmental and cavitary defects with an intact posterior column. A Type IV defect includes pelvic discontinuity, in which the superior pelvis and the inferior pelvis are separated. Type V defect termed “arthrodesis” does not imply bone deficiency but difficulty in identifying the location of the true acetabulum and it is still included since it represents a technical deficiency. The major flaw of this classification system is that it does not address the management of these defects (Table 1).
The Paprosky classification was introduced in the early 1990’s (Table 1). This classification system relies on preoperative and intraoperative evaluation and it is based on the presence or absence of and intact acetabular rim and its ability to provide initial rigid support for an implanted acetabular component. The hip center migration and the integrity of four acetabular supportive structures are evaluated on preoperative antero-posterior (AP) radiograph of the pelvis: the teardrop (medial wall), the hip center (superior dome), the Kohler’s line (anterior column) and the ischium (posterior column). Type I defects have minimal focal bone loss, the hemispheric shape of the acetabulum is maintained with neither periprosthetic osteolysis nor migration of the components. Type II defects show a distortion of the acetabular shape; anterior and posterior columns are still present but is evident a deficit of the superior dome and/or the medial wall. This category is subclassified in IIA, with an ovalized acetabulum, superior lysis with a <2cm superior migration but an intact superior rim; IIB, similarly to the IIA but with a deficient superior rim so the implants migrates superolaterally; and IIC, where the implant may migrate medially due to a deficient medial wall. Type III defects involve major bone loss with >3cm migration of the implant, destruction of the acetabular rim and supportive structures. If the acetabulum is considered as a circular structure interpreted like a clock face, the IIIA pattern extends from ten o’clock to two o’clock (30% to 60% of bone stock destruction) with an intact Kohler’s line (medial wall) and ischium and a superolateral migration (known as “up-and-out” deformity). The IIIB defines a major bone loss from nine o’clock to five o’clock (>60% of the bone stock) that involves both walls and both columns with severe obliteration of the teardrop and severe lysis of the ischium with a superomedial migration (known as “up-and-in” deformity). Patients with type IIIB defect have a high risk of pelvic discontinuity (PD), defined as the loss of continuity between the superior and the inferior hemipelvis, resulting from bone loss or fracture of the acetabulum. In addition to providing a system for describing bone loss, the Paprosky classification also guides treatment strategy (Figure 1).
Figure 1.

Algorithmic approach to acetabular reconstruction (Redrawn from Sporer SM, Paprosky WG, O’Rourke MR: Managing bone loss in acetabular revision. Instr Course Lect 55:290, 2006.).
Table 1.
Classification systems for acetabular bone loss.
Patient evaluation and preoperative planning
Revision THA is indicated when a specific problem, caused by hip pathology, is identified and can be surgically corrected. Patient pre-operative evaluation considers the severity and the characteristics of the patient’s symptoms, along with the physical examination, including range of motion, limb length discrepancies, hip musculature and ambulatory capacity.14 A detailed laboratory work-up inclusive of white blood cell count, erythrocyte sedimentation rate (ESR), and C-reactive protein level (CRP) should be mandatory in order to exclude periprosthetic joint infection (PJI) given their high sensitivity and specificity when these tests are combined.18 Hip joint aspiration with synovial fluid cell count and differential culture should be performed as well.18
Plain radiographs are essential to make the correct diagnosis.19 The anteroposterior (AP), lateral, and cross-table views of the hip are important to understand the eventual migration of the implant, ischial osteolysis and teardrop obliteration. Oblique views of the pelvis (Judet views) are crucial for assessing anterior column (obturator oblique) and posterior column (iliac oblique) bone stock.19 However, they generally tend to underestimate the degree of osteolysis.20 CT-scan provides additional information despite the increased radiological exposition and its high costs.20,21 CT with three-dimensional reconstructions and artifact minimization is useful for planning acetabular revision in case of pelvic osteolysis and pelvic discontinuity when they are not clearly defined on plain radiographs.19,22 Metal artefact reduction sequence magnetic resonance imaging (MARS MRI) is inferior to CT-scan in quantifying the bone defects, however, it is an effective tool,when metalon- metal bearing or dissimilar metal junctions are present, in assessing associated soft tissue adverse reactions (pseudotumor and adverse reaction to metal debris).19 Additional studies such as angiography are suggested when the acetabular component has migrated medially to the ilio-ischial line.23 However, in the majority of the medial migration of the cups, there is either fibrous tissue or remodeling of medial bone separating the cup from the pelvic cavity.19
Once the reason for acetabular revision is identified and bone defects are correctly quantified, the definitive acetabular reconstruction option is designated according to patient’s characteristics and surgeon’s experience.
Reconstruction available options
Impaction Bone Grafting with Metal Mesh
Impaction bone grafting is indicated in segmental and combined defects (Paprosky types IIIA and IIIB). In case of uncontained peripheral acetabular defects supplemental devices such as metal mesh or reconstruction ring are required to transform them into contained defects.24-28 This technique should be avoided when severe segmental defects are combined with major medial deficiencies. 3,29,30 Failures are usually related to fracture and consequent migration of the stainless steel mesh, graft resorption and micromovement.29 In a recent systematic review Baauw et al,3 reported an overall reoperation rate of 7.4% (15 of 204 hips), an acetabular revision rate of 6.4% (14 of 204 hips) and an 8.8% of radiographic loosening (18 of 204 hips) at a mean 5.2 years. The main advantage of impaction bone grafting is the restoration of bone stock, especially in young patients who will eventually require a new cup revision. In addition, this technique should be avoided in patients with Paprosky type IIIB defect since it has been reported a higher risk of failure compared to type IIIA.30
Reinforcement Rings and Antiprotrusio Cages
Roof-reinforcement rings and anti-protrusio cages are indicated in severe bone loss and pelvic discontinuity (Paprosky types IIB, IIIA and IIIB; AAOS types 3 and 4).31-38 These devices are designed to protect morselized and structural grafts from highstress forces avoiding early bone resorption and cup loosening when a “bridge” is required to span the defect and transfer the load to the peripheral host bone.39,40 Primary stability is augmented with flanges and screws allowing large contact areas between the implant and pelvic bone.34 The distal side is inserted and fixed to the teardrop and superior border of the obturator foramen while the plate on the proximal side is fixed to the iliac bone.35,41 In a recent systematic review Baauw et al.,3 reported an overall revision rate of anti-protrusio cages of 3.5% (11 of 315 hips), a radiographic loosening of 7% (18 of 315 hips, with the majority due to fracture of the device or screws) and overall reoperation rate of 8.6% at mean 7.5 years. Rings and cages provide a relatively low-cost option for bridging acetabular defects with satisfactory clinical outcomes in cases of large bone defects in elderly and low demanding patients. With the advent of highly porous metal and improved cup designs, these devices are slowly falling out of favor. In addition, rings are contraindicated in medial wall deficiency, protrusio, pelvic discontinuity and inferior bone loss.39,42-44 Cages may still be useful as they span the acetabular defect whilst allowing a near anatomic center of rotation and providing a high structural support in case of inferior poor bone contact.2,43
Structural Allograft
Historically, Paprosky et al.,15 described the use of bulk structural bone grafts in conjunction with hemispherical cementless acetabular components in case of moderateto- severe acetabular bone defects (Paprosky Type II and III). A femoral head allograft cut in “number of 7” is usually used for Paprosky Type IIA and IIB defects whilst a distal femur or proximal tibial allograft is used for Paprosky Type IIIA defects. In Type IIIB, a proximal femoral allograft can be transected in a coronal plane and laid over the defect. The authors reported no signs of major resorption or fracture of the graft with a 4% (6 out of 147 hips) of implants loosening (>3mm). DeWal et al,45 reported a 15% of implant loosening (2 out of 13 hips) with no signs of graft resorption at 6.8 years. Sporer et al,46 reported a survivorship of 78% from re-revision due to aseptic loosening in a cohort of 31 Paprosky Type IIIA bone defects at 10.3 years. Disadvantages related to bulk allografts are the risk of infection transmission, the variable mechanical characteristics, and the partial resorption or healing of the graft.3,47 However, given that structural allograft may enhance future bone stock, younger patients may be better candidates for structural allografts rather than porous metal augments.14
Cementless Hemispherical Cups
Cementless hemispherical cups are widely considered the recommended options in Parprosky Types I and II (AAOS 1 and 2) bone defects.15 Cancellous bone grafting can be added to fill the inner bone deficiency with satisfactory outcomes at mid-to-long term.48-50 Della Valle et al,50 reported a 15-year overall survivorship of 81%, and a 96% survivorship when considering revision due to aseptic loosening in a cohort of 138 hips. In case of a superior defects (Paprosky Type IIA) the cups can be positioned superiorly (“high hip center”) and the defects filled with particulate grafts.15 However, the “high hip center” technique is associated with an increased risk of dislocation due to the modification of the abductor and adductor lever arms. Advantages of un uncemented hemispherical cup are a stable and biologic fixation in mild-to-moderate bone defects and a surgical technique familiar to many arthroplasty surgeons; however, it is accepted that provide poor results in severe acetabular bone defects (>50% of bone stock).51
Extra-Large “Jumbo” Cups
Extra-large “jumbo” cups are an option in case of major defects (Paprosky Types II and III; AAOS Types 3 and 4). They are defined as having a diameter >66mm in males and >62mm in females, approximately 10mm larger than the mean diameter of the acetabular components used in primary THA.52 This technique has multiple advantages: it is technically straightforward, most bone defects are filled by the socket itself obviating the need for extensive bone-graft, there is an increased contact area between the implant and the host bone and the center of hip rotation is translated to a more lateral and inferior position.11,52-54 Disadvantages are that a large socket limit the bone stock restoration in case of additional re-revision of the acetabular component, and large, oblong bone defects cannot be filled in an inferior-to-superior direction without marked reaming of the anterior or posterior column (vital for the implant fixation) or superior placement of the cup.52 Relative contraindication are previous irradiation of the pelvis and massive acetabular bone loss of the superior-lateral rim or the posterior column that can preclude the initial implant stability.2,52 Von Roth et al,53 reported a survivorship of 83% (15 of 89 hips) at 20 years. In a recent systematic review Volpin et al,11 reported a failure rate of 12.1% (63 of 518 hips) at 10 years, with liner exchange as the most common causes of reoperation (7.1%).
Oblong Cups
Oblong cups are indicated in large superior segmental bone defects with a prevalent superior migration and a longitudinal diameters that are greater than their transverse diameters (Paprosky Types IIA, IIB and IIIA).55,56 Oblongs cups adapt better to large and oblong bone defects, that cannot be filled with hemispherical cups, avoiding marked reaming of the anterior and posterior columns.51,55-61 Three types of Oblong Cups have been described: the bilobed oblong acetabular component, the longitudinal oblong revision cup (LOR) and the BOFOR cup.56 In a recent systematic review, Volpin et al,11 reported good results for oblong cups in term of overall failure rate (5.9%, 12 of 203 hips) with an aseptic loosening rate of 3.9% (8 of 203 hips) and a dislocation rate of 2.4% (5 of 203 hips) at a mean follow-up of 7.6 years. These results are probably due to the ability of these cups to restore the hip center and achieve osseointegration through sufficient bone implant contact.51 The main advantage of the cups is their relative ease of implantation and the oblong shape that almost enables a press-fit incorporation.
Modular Porous Metal Augments
Porous modular metal augments in conjunction with highly porous cup represent a viable option for the reconstruction of moderate- to-severe acetabular bone defects (Paprosky Types IIIA, IIIB and pelvic discontinuity). 62-64 Porous metal augments are made with highly porous tantalum or titanium. The higher porosity (up to 80%) allows a proportionate increase in interface strength compared to conventional implants and the high coefficient of friction improves the primary stability.2,63 Highly porous cups, usually used alone in mild-to-moderate bone defects (Paprosky Types I and II), can be supported with porous metal augments and/or cage when bone loss is >50% of the original bone stock or in presence of pelvic discontinuity.48,62 Highly porous revision shells have a multi-hole configuration (8-12 screw holes) in order to position additional screws and increase stability.2 Highly porous augments are usually fixed to the bone before the fixation of the acetabular cup in case of large intracavitary defects (anterosuperior and posteroinferior). In case of extracavitary defects (posterosuperior) the augments can be positioned after the acetabular cups since they provide a supplemental fixation.14 The use of metallic material, instead of bone grafts, avoid certain risks associated with allografting like transmission of infections, variable mechanical characteristics and partial resorption or healing; on the other hand it is necessary to remove some extra host bone to accommodate the metallic augment and achieve the indispensable press-fit.3,47 For the majority of the porous metal augment systems available in the market, the junctions between the porous metal augments and the highly porous cups need to be filled with cement, to avoid the release of metal fragments and induced metallosis.47,65 Jenkins et al,66 reported a survivorship from aseptic loosening of 97% (2 out of 58 hips) for aseptic loosening at a minimum 5-year follow-up and proposed variable configurations in order to achieve stability in different bone defects:
Cup + “flying buttress” augment configuration: in peripheral segmental defect, particularly in the posterosuperior quadrant (Paprosky type IIIA).
Cup + “dome” augment configuration: in elliptical, contained cavitary defects, when the anteroposterior dimension of the acetabulum precluded simply reaming up to a jumbo socket (Paprosky type IIIA).
Cup + “footing” augment: in massive medial cavitary or segmental defects to support the cup (Paprosky type IIIB).
All the junctions between tantalum components need to be filled with cement, except for the “footing” conformation. The remaining cavitary defects are filled with cancellous bone chips.48
In case of severe medial bone defects (Paprosky Types IIC, IIIA and IIIB), Blumenfeld et al,67 described the “cup-incup” technique with ah highly porous “Jumbo” cup combined with cementation of a similar highly porous cup into the initial jumbo cup. Webb et al,68 described the “double-cup” technique (Paprosky type IIIA, IIIB) using a highly porous cup as a “super-augment” to buttress the superior medial or lateral defect.
In a recent systematic review, Baauw et al,3 reported on the use of porous metal augments in large acetabular defects (Paprosky Types IIIA and IIIB; AAOS Types 3 and 4). They found a survivorship from re-revision of 98.4% (2 of 125 hips), a radiographic loosening of 2.4% (3 of 125 hips), an overall reoperation rate of 15.2% (19 of 125 hips) and a dislocation rate of 4.8% (10 of 125 hips) at mean follow-up of 3.8 years.
Cup-Cage Reconstruction Systems
Cup-cage reconstruction is indicated in case of severe bone defects (Paprosky Type III) and chronic pelvic discontinuity. Described by Nehme et al,64 it is a hybrid technique based on a highly porous cup with partial press-fit in combination with morselized host-bone or allograft, supported by a cage that provides load relief. The liner is then cemented into the cage and the hip center is brought back to a more physiologic position. Once the cup is well integrated the cage is offloaded preventing mechanical loosening.69 Early outcomes reported a survivorship of more than 85%,70,71 and encouraging mid-term clinical and radiological outcomes have been reported in case of pelvic discontinuity. 69,72,73 Abolghasemian et al,69 reported a survivorship of 88.5% at a mean 3.9 years (3 of 26 hips); Martin et al,73 reported a survivorship of 100% in a cohort of 27 hips at 5 years with 74% of healing of the discontinuity; Amenabar et al,72 reported an overall survivorship of 91% (4 of 45 hips) at a mean follow-up of 6.4 years when cup-cage constructs were used for the treatment of pelvic discontinuity. Concerns are addressed regarding the positioning of the cup, typically placed too vertical and relatively retroverted in order to accommodate the cage; particular attention is needed in cementing the liner with the right anteversion and inclination.74 In addition, “half cage” technique (without the ischial flange) has been described with a “kick-stand” screw positioned in the ischium or in the superior pubic ramus in order to avoid abduction failure of the cup.14
Custom Triflange Acetabular Components
Custom triflange acetabular components (CTACs) are a valid option in massive periacetabular bone defects (Paprosky Types IIIA and IIIB). The main advantage, despite their high costs compared to other reconstruction implants, is the possibility to completely customize the implant starting from a thin-cut computed tomography scan.75 The surgeon can decide the characteristics of the component by selecting the position of flanges, location and direction of screws, and number of holes. In addition, the surgeon is able to plan the location, inclination, and anteversion of the acetabular cup. In order to facilitate osseointegration, porous coatings and hydroxyapatite are often applied to the flanges and backside acetabular portion of the implant. A modular liner is placed into the central hemispherical cup and engaged with either a modular locking mechanism or bone cement.10,22 However, if osseointegration is incomplete this implants are prone to mechanical complications, especially in case of deficient superior support or in pelvic discontinuity.10 In a recent systematic review, De Martino et al,22 reported that CTACs are a viable and effective way to manage complex acetabular bone defects with an overall complication rate of 29% (168 of 579 hips), reoperation rate of 17.3% (100 of 579 hips) and dislocation rates of 11% (57 of 516 hips) at mean 4.8 years showing a considerable improvement in multiple functional scores. The authors also reported that the relatively high complication rate in the CTACs may reflect the complexity of revisions and severity of acetabular bone defects. In fact, the surgical technique involves extensive soft tissue dissection with possible neuro-muscular damage11 (Figure 2).
Acetabular Distraction
Acetabular distraction has been described as an alternative treatment in case of pelvic discontinuity (PD).76 The technique is based upon the placement of and extra-acetabular distractor to allow peripheral or lateral distraction and central or medial compression at the discontinuity. The technique provides initial mechanical stability and, once bone healing occurs, biologic fixation through a highly porous cup placed into a distracted pelvic discontinuity. The presence of PD is usually confirmed intraoperatively. A stable fit of the cup with the anterosuperior and posteroinferior columns is mandatory in order to be a successful reconstruction option. Cement is apposed in the interface between the augment and the AC to reduce micromotions and the cup is additionally stabilized with cancellous screws, two of which inferiorly into the ischium or superior pubic ramus (“kickstand” screw) to avoid abduction failure of the cup. Finally, the liner is then cemented with the right version and inclination. 74,76 Sporer et al,76 reported survivorship from aseptic loosening of 95% (1 out of 20, at minimum 2 years) and 20% of early migration of the acetabular component (4 out of 20) that stabilized with time and did not present clinical relevance. Sheth et al,77 reported survivorship from re-revision due to aseptic loosening of 97% (1 failure out of 32 cases) and radiographic loosening of 6% (2 out of 32) at 5 years. Radiographically, 69% of the cases (22 out of 32) showed good healing of the discontinuity. Advantages of the acetabular distraction may result in more reproducible healing of a chronic pelvic discontinuity with a theoretically decreased risk of subsequent implant loosening. Disadvantages are its technically complexity and the not well defined magnitude of distraction required for adequate fixation.14 Further long-term high-quality studies are needed to confirm the survivorship of the implants and the clinical results.
Conclusions
Acetabular bone defects are a major concern in the setting of revision THA. Paprosky classification system is the most commonly used to describe the defects and guide treatment strategy. To date, as assessed from this review, multiple reconstruction options are available, and each technique presents advantages and disadvantages; however, the optimal method should be selected according to the surgeon’s experience, the appropriate preoperative evaluation and classification of the bone defect associated with a correct planning. Hemispherical uncemented cups supported by screw fixation are recommended to address mild and moderate defects. Highly porous metal cups and augments showed satisfactory results in enhancing bone ingrowth and fixation when used to address severe bone defects. In case of pelvic discontinuity good mid-term results have been reported with the use of cupcage, custom triflange acetabular components and acetabular distraction technique. However, despite the overall good mid-term outcomes, there is no consensus regarding which reconstruction technique guarantees better long-term survivorship due to the lack of high-quality long-term studies on the modern reconstructive options.
Finally, the outcome of revision THAs depends on multiple factors including patient selection, appropriate preoperative evaluation of the bone defects, correct planning and templating, consideration of alternative strategies, proper reconstruction options, and good postoperative care and rehabilitation.
Figure 2.

Example of highly porous cup with caudal hook and fins to ensure additional stability. (Curtesy of LimaCorporate)
Funding Statement
Funding: None.
References
- 1.Bou Monsef J, Parekh A, Osmani F, Gonzalez M. Failed Total Hip Arthroplasty. JBJS Rev 2018;6:e3. [DOI] [PubMed] [Google Scholar]
- 2.Jain S, Grogan RJ, Giannoudis P V. Options for managing severe acetabular bone loss in revision hip arthroplasty. A systematic review. HIP Int 2014;24: 109-22. [DOI] [PubMed] [Google Scholar]
- 3.Baauw M, Van Hooff ML, Spruit M. Current construct options for revision of large acetabular defects: A systematic review. JBJS Rev 2016;4:e2. [DOI] [PubMed] [Google Scholar]
- 4.Jafari SM, Coyle C, Mortazavi SMJ, et al. Revision hip arthroplasty: Infection is the most common cause of failure. Clin Orthop Relat Res 2010;468:2046-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Howie DW, Neale SD, Haynes DR, et al. Periprosthetic osteolysis after total hip replacement: Molecular pathology and clinical management. Inflammo-pharmacology 2013;21:389-96. [DOI] [PubMed] [Google Scholar]
- 6.Patel PD, Potts A, Froimson MI. The Dislocating Hip Arthroplasty. Prevention and Treatment. J Arthroplasty 2007;22:86-90. [DOI] [PubMed] [Google Scholar]
- 7.Bozic KJ, Kurtz SM, Lau E, et al. The epidemiology of revision total hip arthroplasty in the united states. J Bone Jt Surg -Ser A 2009;91:128-33. [DOI] [PubMed] [Google Scholar]
- 8.Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Jt Surg -Ser A 2007;89:780-5. [DOI] [PubMed] [Google Scholar]
- 9.Howie DW, Neale SD, Martin W, et al. Progression of periacetabular osteolytic lesions. J Bone Jt Surg -Ser A 2012;94:1-6. [DOI] [PubMed] [Google Scholar]
- 10.Nieminen J, Pakarinen TK, Laitinen M. Orthopaedic reconstruction of complex pelvic bone defects. evaluation of various treatment methods. Scand J Surg 2013;102:36-41. [DOI] [PubMed] [Google Scholar]
- 11.Volpin A, Konan S, Biz C, et al. Reconstruction of failed acetabular component in the presence of severe acetabular bone loss: a systematic review. Musculoskelet Surg 2019;103:1-13. [DOI] [PubMed] [Google Scholar]
- 12.Maccauro G, Liuzza F, Scaramuzzo L, et al. Percutaneous acetabuloplasty for metastatic acetabular lesions. BMC Musculoskelet Disord 2008;9:1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Spinelli MS, Ziranu A, Piccioli A, Maccauro G. Surgical treatment of acetabular metastasis. Eur Rev Med Pharmacol Sci 2016;20:3005-10. [PubMed] [Google Scholar]
- 14.Fryhofer GW, Ramesh S, Sheth NP. Acetabular reconstruction in revision total hip arthroplasty. J Clin Orthop Trauma 2020;11:22-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty 1994;9:33-44. [DOI] [PubMed] [Google Scholar]
- 16.D’Antonio JA, Capello WN, Borden LS, et al. Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res 1989;126-37. [PubMed] [Google Scholar]
- 17.Saleh KJ, Holtzman J, Gafni A, et al. Development, test reliability and validation of a classification for revision hip arthroplasty. J Orthop Res 2001;19: 50-6. [DOI] [PubMed] [Google Scholar]
- 18.Parvizi J, Tan TL, Goswami K, et al. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J Arthroplasty 2018;33:1309-1314.e2. [DOI] [PubMed] [Google Scholar]
- 19.Reid C, Grobler G, Dower B, et al. Revision total hip arthroplasty: addressing acetabular bone loss. SA Orthop J 2012;11:34-46. [Google Scholar]
- 20.Egawa H, Powers CC, Beykirch SE, et al. Can the volume of pelvic osteolysis be calculated without using computed tomography? Clin Orthop Relat Res 2009;467:181-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cahir JG, Toms AP, Marshall TJ, et al. CT and MRI of hip arthroplasty. Clin Radiol 2007;62:1163-71. [DOI] [PubMed] [Google Scholar]
- 22.De Martino I, Strigelli V, Cacciola G, et al. Survivorship and Clinical Outcomes of Custom Triflange Acetabular Components in Revision Total Hip Arthroplasty: A Systematic Review. J Arthroplasty 2019;34:2511-8. [DOI] [PubMed] [Google Scholar]
- 23.Sporer SM. How to do a revision total hip arthroplasty: Revision of the acetabulum. J Bone Jt Surg -Ser A 2011;93:1359-66. [DOI] [PubMed] [Google Scholar]
- 24.Slooff TJ, Schimmel JW, Buma P. Cemented Fixation With Bone Grafts. Orthop Clin N Am 1993;24:667-77. [PubMed] [Google Scholar]
- 25.Schreurs BW, Bolder SBT, Gardeniers JWM, et al. Acetabular revision with impacted morsellised cancellous bone grafting and a cemented cup. J Bone Jt Surg -Ser B 2004;86:492-7. [PubMed] [Google Scholar]
- 26.Gie GA, Linder L, Lin RSM, et al. Impacted Cancellous Allografts and Cement for Revision Total Hip Arthroplasty. J Bone Jt Surg 1993;75: 14-21. [DOI] [PubMed] [Google Scholar]
- 27.Boldt JG, Dilawari P, Agarwal S, Drabu KJ. Revision total hip arthroplasty using impaction bone grafting with cemented nonpolished stems and charnley cups. J Arthroplasty 2001;16:943-52. [DOI] [PubMed] [Google Scholar]
- 28.Comba F, Buttaro M, Pusso R, Piccaluga F. Acetabular reconstruction with impacted bone allografts and cemented acetabular components. A 2-to 13-year follow-up study of 142 aseptic revisions. J Bone Jt Surg -Ser B 2006;88:865-9. [DOI] [PubMed] [Google Scholar]
- 29.Buttaro MA, Comba F, Pusso R, Piccaluga F. Acetabular revision with metal mesh, impaction bone grafting, and a cemented cup. Clin Orthop Relat Res 2008;466:2482-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Garcia-Cimbrelo E, Cruz-Pardos A, Garcia-Rey E, Ortega-Chamarro J. The survival and fate of acetabular reconstruction with impaction grafting for large defects. Clin Orthop Relat Res 2010;468:3304-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bostrom MP, Lehman AP, Buly RL, et al. Acetabular revision with the contour antiprotrusio cage: 2-to 5-Year followup. Clin Orthop Relat Res 2006;188-94. [DOI] [PubMed] [Google Scholar]
- 32.Gaiani L, Bertelli R, Palmonari M, Vicenzi G. Total hip arthroplasty revision in elderly people with cement and Burch-Schneider anti-protrusio cage. Chir Organi Mov 2009;93:15-9. [DOI] [PubMed] [Google Scholar]
- 33.Hsu CC, Hsu CH, Yen SH, Wang JW. Use of the Burch-Schneider cage and structural allografts in complex acetabular deficiency: 3-to 10-year follow up. Kaohsiung J Med Sci 2015;31:540-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Jones L, Grammatopoulos G, Singer G. The Burch-Schneider cage: 9-year survival in Paprosky type 3 acetabular defects. clinical and radiological followup. HIP Int 2012;22:28-34. [DOI] [PubMed] [Google Scholar]
- 35.Kerboull M, Hamadouche M, Kerboull L. The Kerboull acetabular reinforcement device in major acetabular reconstructions. Clin Orthop Relat Res 2000;155-68. [DOI] [PubMed] [Google Scholar]
- 36.Okano K, Miyata N, Enomoto H, et al. Revision with impacted bone allografts and the kerboull cross plate for massive bone defect of the acetabulum. J Arthroplasty 2010;25:594-9. [DOI] [PubMed] [Google Scholar]
- 37.Regis D, Sandri A, Bonetti I, et al. A Minimum of 10-Year Follow-Up of the Burch-Schneider Cage and Bulk Allografts for the Revision of Pelvic Discontinuity. J Arthroplasty 2012;27: 1057-1063.e1. [DOI] [PubMed] [Google Scholar]
- 38.Wegrzyn J, Pibarot V, Jacquel A, et al. Acetabular reconstruction using a kerboull cross-plate, structural allograft and cemented dual-mobility cup in revision THA at a minimum 5-year follow-up. J Arthroplasty 2014;29:432-7. [DOI] [PubMed] [Google Scholar]
- 39.Regis D, Magnan B, Sandri A, Bartolozzi P. Long-Term Results of Anti-Protrusio Cage and Massive Allografts for the Management of Periprosthetic Acetabular Bone Loss. J Arthroplasty 2008;23:826-32. [DOI] [PubMed] [Google Scholar]
- 40.Gill TJ, Sledge JB, Müller ME. The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty. Indications, principles and long-term results. J Bone Jt Surg -Ser B 1998;80:946-53. [DOI] [PubMed] [Google Scholar]
- 41.Makita H, Kerboull M, Inaba Y, et al. Revision Total Hip Arthroplasty Using the Kerboull Acetabular Reinforcement Device and Structural Allograft for Severe Defects of the Acetabulum. J Arthroplasty 2017;32:3502-9. [DOI] [PubMed] [Google Scholar]
- 42.Paprosky WG, Sporer SS, Murphy BP. Addressing Severe Bone Deficiency. What a Cage Will Not Do. J Arthroplasty 2007;22:111-5. [DOI] [PubMed] [Google Scholar]
- 43.Haddad FS, Shergill N, Muirhead-Allwood SK. Acetabular reconstruction with morcellized allograft and ring support: A medium-term review. J Arthroplasty 1999;14:788-95. [DOI] [PubMed] [Google Scholar]
- 44.Schatzker J, Wong MK. Acetabular revision. The Role Of Rings and Cages. Clin Orthop Relat Res 1999;369:187-97. [PubMed] [Google Scholar]
- 45.DeWal H, Chen F, Su E, Di Cesare PE. Use of structural bone graft with cementless acetabular cups in total hip arthroplasty. J Arthroplasty 2003;18:23-8. [DOI] [PubMed] [Google Scholar]
- 46.Sporer SM, O’Rourke M, Chong P, Paprosky WG. The Use of Structural Distal Femoral Allografts for Acetabular Reconstruction. Average Ten-Year Follow-up. J Bone Jt Surg -Am 2005;87:760-5. [DOI] [PubMed] [Google Scholar]
- 47.Migaud H, Common H, Girard J, et al. Acetabular reconstruction using porous metallic material in complex revision total hip arthroplasty: A systematic review. Orthop Traumatol Surg Res 2019;105:S53-61. [DOI] [PubMed] [Google Scholar]
- 48.Flecher X, Sporer S, Paprosky W. Management of Severe Bone Loss in Acetabular Revision Using a Trabecular Metal Shell. J Arthroplasty 2008;23: 949-55. [DOI] [PubMed] [Google Scholar]
- 49.Della Valle CJ, Shuaipaj T, Berger RA, et al. Revision of the Acetabular Component Without Cement After Total Hip Arthroplasty. A Concice Follow-up, At Fifteen To Nineteen Years, Of A Previous Report. J Bone Jt Surg -Am Vol 2005;87:1795-800. [DOI] [PubMed] [Google Scholar]
- 50.Della Valle CJ, Berger RA, Rosenberg AG, et al. Cementless Acetabular Reconstruction in Revision Total Hip Arthroplasty. Clin Orthop Relat Res 2004;60612:96-100. [DOI] [PubMed] [Google Scholar]
- 51.García-Rey E, Fernández-Fernández R, Durán D, Madero R. Reconstruction of the rotation center of the hip after oblong cups in revision total hip arthroplasty. J Orthop Traumatol 2013;14:39-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Whaley AL, Berry DJ, Scott Harmsen W. Extra-large uncemented hemispherical acetabular components for revision total hip arthroplasty. J Bone Jt Surg -Ser A 2001;83:1352-7. [DOI] [PubMed] [Google Scholar]
- 53.Von Roth P, Abdel MP, Harmsen WS, Berry DJ. Uncemented jumbo cups for revision total hip arthroplasty: A concise follow-up, at a mean of twenty years, of a previous report. J Bone Jt Surg -Am Vol 2015;97:284-7. [DOI] [PubMed] [Google Scholar]
- 54.Lachiewicz PF, Soileau ES. Fixation, survival, and dislocation of jumbo acetabular components in revision hip arthroplasty. J Bone Jt Surg -Ser A 2013;95:543-8. [DOI] [PubMed] [Google Scholar]
- 55.Köster G, Rading S. Revision of failed acetabular components utilizing a cementless oblong cup: An average 9-year follow-up study. Arch Orthop Trauma Surg 2009;129:603-8. [DOI] [PubMed] [Google Scholar]
- 56.Desai AS, Dramis A, Board TN, et al. Acetabular revision surgery with the uncemented oblong BOFOR Cup -Early to midterm results. HIP Int 2012;22:280-5. [DOI] [PubMed] [Google Scholar]
- 57.Civinini R, Capone A, Carulli C, et al. Acetabular revisions using a cementless oblong cup: Five to ten year results. Int Orthop 2008;32:189-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Št’astný E, Trč T, Handl M, et al. Midterm results of revision total hip arthroplasty using the oval-shaped uncemented Trč-Cingr cup. Int Orthop 2014;38:935-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.DeBoer DK, Christie MJ. Reconstruction of the deficient acetabulum with an oblong prosthesis: Three-to seven-year results. J Arthroplasty 1998;13:674-80. [DOI] [PubMed] [Google Scholar]
- 60.Chen WM, Engh CA, Hopper RH, et al. Acetabular revision with use of a bilobed component inserted without cement in patients who have acetabular bone-stock deficiency. J Bone Jt Surg -Ser A 2000;82:197-206. [DOI] [PubMed] [Google Scholar]
- 61.Berry DJ, Sutherland CJ, Trousdale RT, et al. Bilobed oblong porous coated acetabular components in revision total hip arthroplasty. Clin Orthop Relat Res 2000;154-60. [DOI] [PubMed] [Google Scholar]
- 62.Weeden SH, Schmidt RH. The Use of Tantalum Porous Metal Implants for Paprosky 3A and 3B Defects. J Arthroplasty 2007;22:151-5. [DOI] [PubMed] [Google Scholar]
- 63.Bobyn JD, Stackpool GJ, Hacking SA, et al. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J Bone Jt Surg -Ser B 1999;81:907-14. [DOI] [PubMed] [Google Scholar]
- 64.Nehme A, Lewallen DG, Hanssen AD. Modular porous metal augments for treatment of severe acetabular bone loss during revision hip arthroplasty. Clin Orthop Relat Res 2004;201-8. [DOI] [PubMed] [Google Scholar]
- 65.Abolghasemian M, Tangsataporn S, Sternheim A, et al. Combined trabecular metal acetabular shell and augment for acetabular revision with substantial bone loss: A mid-term review. J Bone Jt Surg -Ser B. 2013;95B:166-72. [DOI] [PubMed] [Google Scholar]
- 66.Jenkins DR, Odland AN, Sierra RJ, et al. Minimum Five-Year Outcomes with Porous Tantalum Acetabular Cup and Augment Construct in Complez Revision Total Hip Arthroplasty. J Bone Jt Surg 2017;49:1-7. [DOI] [PubMed] [Google Scholar]
- 67.Blumenfeld TJ, Bargar WL. Surgical technique: A cup-in-cup technique to restore offset in severe protrusio acetabular defects. Clin Orthop Relat Res 2012;470:435-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Webb JE, McGill RJ, Palumbo BT, et al. The Double-Cup Construct: A Novel Treatment Strategy for the Management of Paprosky IIIA and IIIB Acetabular Defects. J Arthroplasty 2017;32:S225-31. [DOI] [PubMed] [Google Scholar]
- 69.Abolghasemian M, Tangsataporn S, Kuzyk PRT, et al. Cup-Cage Solution for Pelvic Discontinuity. Semin Arthroplasty 2012;23:171-5. [Google Scholar]
- 70.Kosashvili Y, Backstein D, Safir O, et al. Acetabular revision using an anti-protrusion (ilio-ischial) cage and trabecular metal acetabular component for severe acetabular bone loss associated with pelvic discontinuity. J Bone Jt Surg -Ser B 2009;91:870-6. [DOI] [PubMed] [Google Scholar]
- 71.Konan S, Duncan CP, Masri BA, Garbuz DS. The cup-cage reconstruction for pelvic discontinuity has encouraging patient satisfaction and functional outcome at median 6-year follow-up. HIP Int 2017;27:509-13. [DOI] [PubMed] [Google Scholar]
- 72.Amenabar T, Rahman WA, Hetaimish BM, et al. Promising Mid-term Results With a Cup-cage Construct for Large Acetabular Defects and Pelvic Discontinuity. Clin Orthop Relat Res 2016;474:408-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Martin JR, Barrett I, Sierra RJ, et al. Construct rigidity: Keystone for treating pelvic discontinuity. J Bone Jt Surg -Am Vol 2017;99:e43. [DOI] [PubMed] [Google Scholar]
- 74.Hasenauer MD, Paprosky WG, Sheth NP. Treatment options for chronic pelvic discontinuity. J Clin Orthop Trauma 2018;9:58-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Berasi CC, Berend KR, Adams JB, et al. Are Custom Triflange Acetabular Components Effective for Reconstruction of Catastrophic Bone Loss? Clin Orthop Relat Res 2015;473: 528-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Sporer SM, Bottros JJ, Hulst JB, et al. An alternative for severe defects with chronic pelvic discontinuity? Clin Orthop Relat Res 2012;470:3156-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Sheth NP, Melnic CM, Brown N, et al. Two-centre radiological survivorship of acetabular distraction technique for treatment of chronic pelvic discontinuity. Bone Jt J 2018;100B:909-14. [DOI] [PubMed] [Google Scholar]