

Abstract
Vertebral Hemangioma (VH) is a benign tumor usually symptomless and discovered incidentally. Pregnancy, because of several hormonal and physiologic changes, is a recognized risk factor coinciding with the development of a rapid onset of neurological symptoms in patients affected by VH. In the Literature, sporadic cases of neurological symptoms have been described, which occurred during pregnancy, but only rarely the onset of symptoms was reported after pregnancy and childbirth. Usually surgical treatment is reserved for severe cases with rapid onset of neurological symptoms. However, the use of conservative treatments is still a topic of debate In the present study, we report a series of patients affected by VH become symptomatic during or after pregnancy along with a systematic review of the Literature.
Key words: vertebral hemangioma, paraparesis, pregnancy, spine, spine tumors
Introduction
During pregnancy the most frequent oncologic lesions are breast cancer tumors, hematologic tumors and dermatologic tumors while spinal tumors are very rare.1 Vertebral Hemangioma (VH) is a benign tumor usually discovered incidentally.2 Because of several biological changes, pregnancy is recognized as a risk factor for the development of a rapid onset of symptoms from these normally asymptomatic lesions. Less than 1% of VH cause neurologic symptoms from spinal cord or nerve root compression; they can lead to serious neurologic deficits if not promptly treated.1,2 In the present investigation was reported a series of patients affected by VH become symptomatic during or after pregnancy. We also perform a systematic review of the Literature.
Materials and Methods
A systematic review of the literature indexed in PubMed, MEDLINE, Scopus and Cochrane Library databases, using as searchterms “Spine” OR “Spinal“ OR Vertebral” AND “Hemangioma” OR “Angioma” AND “Pregnancy” OR “Parturition” OR “Pregnant woman” and their MeSH terms combinations was performed. The Preferred Reporting Items for Systematically Reviews and Meta-Analyses (PRISMA) was follow as reported in Figure 1. The inclusion criteria of the review was the presence in the evaluated manuscript of: demographic features, symptoms, diagnostic settings, treatment, possible complications and outcomes in patients with symptomatic VH during or immediately following the pregnancy. Only English article with an available abstract were considered eligible for the reviews. Abstracts and full-texts were independently screened by two authors (A.P. and M.C.M.), any discordance was solved by consensus with a third author (D.A.S.).
Case Report #1
A 21-years-old previously healthy woman was referred to our emergency unit because of a right lower limb weakness started 2 weeks after delivery. No relevant clinical history or traumas were reported. Her pregnancy was unremarkable, and the new-born was normal. Physical examination showed bilateral strength deficit at lower limbs (2/5 MRC), hypo responsive knee-jerk reflex and Achilles reflex on both limbs, Babinski reflex positive to the right, urinary retention. Computer Tomography (CT) images showed L1 vertebral compression fracture (Figure 2a,b) with protrusion of bony fragments into the spinal canal with an honeycomb pattern (Figure 2c). Magnetic Resonance (MR) images showed an altered structure in L1 vertebra, marked by a hypo intense signal in T1 images and hyper intense in T2 (Figure 2d), the somatic collapse of L1 suggestive for an aggressive hemangioma induced by recent pregnancy. Other multiple hemanangiomas were localized in vertebral body of metameres T2-8 tract; the larger one is in T8. A surgical approach was necessary due to the severity of the symptoms and the rapidity of onset. In the first surgical stage a wide posterior thoracolumbar decompression by laminectomy with trans-pedicle screw fixation D12-L1, after endovascular embolization of the lesion, was performed (Figure 3). The second surgical stage consisted in percutaneous vertebroplasty of VH in T8 with the use of poly-methylmethacrylate (PMMA) and endovascular embolization of L1 with polyvinyl alcohol. After angiographic evaluation, corpectomy with titanium cage reconstruction was performed. Histological evaluation of the surgical samples showed typical characteristics of aggressive hemangioma. The day after surgery the patient reported an improvement in sensitivity in the lower limbs. After three days there was an improvement in strength in the legs and disappearance of urinary retention after removing the urinary catheter. A week after surgery, the patient walked with help and was therefore transferred to a rehabilitation facility. After 3 months’ neurological examination was normal, no signs of implant loosening or mobilization were noted in the control X-Ray images (Figure 2) and the patient was satisfied with the treatment received. At the last follow up visit, 24 months after surgery, the patient’s neurological examination was normal, and no signs of recurrence was found.
Case Report #2
A 34-year-old healthy woman was referred to our spine surgery unit for worsening back pain started immediately after a natural vaginal delivery. The pregnancy was unremarkable and the newborn was normal. The patient had no notable medical history. A physical examination revealed signs of lumbar tightness with back pain scored 9/10 on the Visual Analogue Scale (VAS). The back pain getting worse in up stand and sitting position while relieved in down stand position. No neurological symptoms were found. A spinal X-Ray showed a L1 compression fracture. CT images confirmed a L1 compression fracture (Figure 4a-c) without protrusion of bony fragments into the spinal canal and a honeycomb aspect of L1 vertebra. MR images showed an altered structure in L1 vertebra, with somatic collapse, suggestive for an aggressive hemangioma exacerbated by pregnancy. Surgical approach was necessary for the worsening symptoms. A percutaneous trans-pedicle screw fixation between D12 and L2 was performed. Transpedicle percutaneous somatic biopsy of L1 vertebra was done. Histological exams showed aggressive hemangioma. The day after surgery the patient demonstrated good pain relieve in up stand and sitting position. She was able to walk with semi-rigid thoracolumbar brace. The post-operative course was uncomplicated and the patient was discharged 4 days after surgery. At 3 moths follow up visit the patient was able to walk without aids and the back pain was completely resolved. At 1 year follow up visit no X-Ray loosening sings of the implant were found (Figure 4d,e) and the patient planned a second pregnancy.
Case Report #3
A 33-year-old healthy woman, gravid 1 para 0, was admitted to our spine unit due to an acute onset of progressive paraplegia with lack of sphincters continence and acute intrascapular pain in her 14th week of pregnancy. A physical examination revealed a flaccid paraplegia in the lower limbs with abolition of deep tendon reflexes in lower extremities, decreased sensation below the T2 level and bilateral positive Babinski sign. MR imaging showed a vertebral lesion occupying the T2 vertebral body with massive epidural extension and spinal cord compression (Figure 5a).
Due to the rapid onset of symptoms, an attempt of urgent surgical decompression by extensive laminectomy of T1-T3 after fixation with trans-pedicle screws was made. However, due to the massive intra-operative bleeding, decompression could not be completed. The day after surgery the neurological condition was unchanged therefore an arteriography was performed with subsequent embolization of the lesion by Contour (250-355 microns) (Figure 5b). Afterwards, laminectomy was completed along with a peace-meal excision of the lesion in a second stage. At the end of the procedure, the spinal cord appeared free of significant compressions. Histological examination of intra-operative samples leads to diagnosis of aggressive hemangioma.
Figure 1.

PRISMA Flow-chart.
Figure 2.
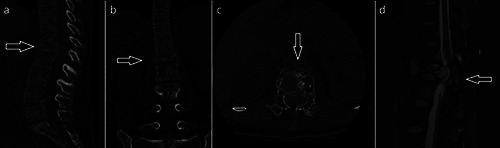
a-c) TC images showing complete collapse of L1with back wall protruding into the spinal canal, in figure c there was bone changes extended to both the pedicles (honey comb pattern). d, MR images showing vertebral body collapse and cord compression.
The day after surgery no neurological improvement was noted, however the patient reported a sensation improvement up to T8 level. The post-operative course was uncomplicated. In the 10th day after surgery the patient was able to sustain sitting position. An improvement of the motor power in the lower limb (2/5 MRC) was found. She was transferred in rehabilitation facility 15 days after surgery. Thirty days after surgery the patient had an abortion. At the follow-up visit performed 3 months after surgery, the MR images showed a reduction of the T2 lesion with a compression-free epidural space (Figure 5c). The patient showed a partial recovery of strength in the lower limbs (4/5 MRC) and was able to walk on crutches. Her bladder and rectal function returned to normal. It was not possible to get further evaluation of this patient because she was lost during follow up.
Systematic Literature review
Patients features and demographical data
Only a few cases of VH became symptomatic during pregnancy or immediately after delivery were reported in the Literature. A total of 357 reports, excluding duplicates, were independently screened, thereby 39 were finally included in our review (Figure 1). Numbers software (Apple Inc., Cupertino, CA) was used to tabulate the obtained data. Our review showed 49 cases, including our patients, of VH reported in the Literature.1-39 The mean age of included patients was 28.2 (+/- 6.6) years, the mean follows up time was 16.1 months (+/-16.1). Demographic and clinical features are summarized in Table 1.
Figure 3.

Radiograph at 3 month of follow-up.
Figure 4.

a-c) TC images showing compression fracture of L1body. d,e) Radiograph at 3 month of follow-up.
Symptoms onset, localization and diagnosis
Symptoms occurred during pregnancy in 38 patients (77%), mostly at the 29th week of gestation. In 11 patients (23%), including our, the symptoms began after delivery. Presentation symptoms were: paraplegia in 30 cases (61%), paraparesis in 16 (33%), back pain in 13 (26%). Seven patients (14%) reported a compression fracture of the affected vertebra.
VH seems to be prevalent in the thoracic segment (39 patients, 80%), followed by the lumbar spine (6 patients, 12%) and the cervical spine (4 patients, 8%). In all case except two (95.9%) a histological diagnosis was made.
Treatment and outcomes and complication
Forty-five patients (91.8%) were surgically treated. In 36 patients (73.4%) only surgical treatment was performed, while in 6 patients (12.2%) surgery was in association with VH embolization and in 3 patients (6.1%) with Radio-Therapy (RT). Only in two cases (4.1%) the patients were treated exclusively through RT. The chosen surgical approaches were: posterior decompression in 26 patients (53%), posterior decompression and fusion in 8 cases (16.3%), anterior decompression and fusion in 5 cases (10.2%), anterior and posterior decompression and fusion in 4 cases (8.2%) and only posterior fusion in two cases (4%). In 4 cases (8.2%) a vertebroplasty of the affected vertebra was associated with surgical treatment.
Concerning neurological outcomes: 32 patients (65.3%) demonstrated a complete recovery, 13 patients (26.5%) only partial recovery, whereas two patients (4.2%) does not demonstrated any neurological recovery; the same two patients died few day after surgery.
About complication: recurrence of the disease was found in 3 patients (6.1%), therefore they underwent reoperation; one patient had a P. Aureginosa infection treated with antibiotic therapy.
Concerning the new-borns and pregnancy: in 31 cases (63.2%) the delivery was unremarkable with normal baby, in 3 cases (6.3%) the new-borns were premature, in 2 cases (4.2%) the babies died during delivery and in one case a patient had an abortion.
Discussion
Background
Most of VH are asymptomatic and the thoracic spine represent the most commonly affected level. VH can cause neurological impairment through multiple mechanisms like expansion of bony elements, epidural expansion of tumor tissue, disturbance of local blood flow or rarely compression fracture of the vertebral body associated with epidural hematomas.2,40 Pregnancy, particularly during the third trimester, is also recognized as a risk factor for symptomatic conversion due to hormonal and biomechanical alterations.41 During pregnancy in fact, the increased blood volume leads to an increased venous pressure inside the hemangioma. The vertebral venous plexus becomes more congested due to the increased pressure of the vena cava compressed by the uterus leading to increased dimension of the hemangioma.1,22 The high levels of estrogen hormones also stimulate the endothelial proliferation with increased dimension of the lesion even without specific estrogen’s receptors. The increased size of the hemangioma and due to the high pressure level of the vertebral plexus can compress the spinal cord and reduce its perfusion.42,43 On one hand, the presence of aggressive hemangioma with onset of symptoms in the postpartum period is poorly described in the literature and reported only in some sporadic cases,43 on the other hand, usually, during pregnancy and post partum period, acute and sub-acute low back pain with the related symptoms are very common.44-46
When vertebral hemangioma becomes symptomatic prompt decompression and stabilization are necessary with a histological identification of the lesion. The rapid progression of the symptoms could have been associated with a recurrence of the lesion. Surgical decompression and fixation, open or hybrid/mini-invasive surgery (MIS), was reserved for cases of neurological symptoms; percutaneous posterior transpedicle screw fixation (without decompression) may be reserved for all cases of compression fractures without neurological impairment.32,47-50 As reported in the current Lliterature, post-operative radiotherapy is recommended in cases of aggressive vertebral hemangioma treated with partial resection to reduce the risk of recurrence.1,32 The meaning of radiation therapy is still under debate and there’s a lack of evidence about its results and about the criteria for eligible patients for this therapy.32,43
Figure 5.

a) MR images showing T2 vertebral body lesion with epidural invasion and cord compression. b) Fluoroscopic image obtained during embolization. c) MR images at 3 months of follow-up showing a reduction of the lesion in T2 and free-compression spinal cord.
Table 1.
Review of the recent literature.
| Study | Case | Week of Pregnacy | Age (Year) | Baby | Symptoms | Level involved | Complication | Treatment | Neurological Outcome | Follow Up (month) |
|---|---|---|---|---|---|---|---|---|---|---|
| Guthkelch AN et al., 1948 | 1 | 36 | 34 | Normal | Paraplegia, BP | T6 | Died | PD | Unchanged | _ |
| Lam LM et al., 1951 | 2 | 34 | 36 | Normal | Paraplegia | T3 | _ | PD | Complete Recover | _ |
| Askenasy H et al., 1957 | 3 | 38 | 20 | Normal | Paraplegia | T11 | _ | PD | Complete Recover | 24 |
| Fields WS et al., 1957 | 4 | 28 | 30 | Normal | Paraplegia | T6 | _ | PD | Complete Recover | _ |
| Newman MJD 1958 | 5 | 39 | 24 | Normal | Paraplegia | T2 | _ | PD | Complete Recover | 3 |
| 6 | 32 | 34 | Normal | Paraplegia | T4-5 | Died | PD | Unchanged | _ | |
| 7 | 32 | 35 | Normal | Paraplegia, BP | L3 | _ | RT | Partial Recover | 24 | |
| Newquist RE et al., 1959 | 8 | 24 | 18 | Premature | Paraplegia, UR | C7-T1 | Infection P. Aureginosa | PD | Partial Recover | 12 |
| Nelson DA et al., 1964 | 9 | 28 | 16 | Died | Paraplegia | T3 | _ | PD, RT | Partial Recover | 10 |
| Esparza et al., 1978 | 10 | 24 | 22 | _ | Paraplegia | T5-T7 | _ | PD, Emb | Complete Recover | _ |
| Faria SL et al., 1985 | 11 | 32 | 40 | _ | Paraplegia | T3 | _ | RT | Complete Recover | _ |
| Lavi E et al., 1986 | 12 | 29 | 25 | 1 Died 1 Hydrocephalus 2 Normal | Paraplegia, BP | T4 | _ | PD | Complete Recover | 1 |
| 13 | 34 | 21 | Normal | Paraparesis, Sciatica | T2 | _ | PD | Complete Recover | _ | |
| CL Liu et al., 1988 | 14 | 22 | 25 | Normal | Paraparesis | T4 | _ | ADF | Complete Recover | 21 |
| Schwartz DA 1989 et al., | 15 | 30 | 30 | _ | Paraplegia | T5 | _ | _ | Complete Recover | _ |
| Poungvarin N et al., 1991 | 16 | 8 | 20 | _ | Paraparesis | T2 | _ | PD | Partial Recover | |
| Redekop GJ et al., 1992 | 17 | 7 AD | 20 | Normal | Paraplegia, BP | T12 | _ | ADF; Emb | Partial Recover | 9 |
| Tekkök IH et al., 1993 | 18 | 1 AD | 25 | Normal | Paraplegia, BP, UR | T5 | Reintervention | PD | Complete Recover | 1 |
| Ogasawara KK et al., 1995 | 19 | 35 | 23 | Mild respiratory distress sydrome | Paraplegia | T5 | _ | PD | Partial Recover | _ |
| Castel E et al., 1999 | 20 | 24 | 27 | Normal | Paraplegia | T8 | _ | Partial Recover | _ | |
| Schwartz TH 2000 et al., | 21 | 1 AD | 29 | Normal | Paraplegia | T11 | Compression Fracture T11 | ADF, RT | Complete Recover | _ |
| Shapiro GS et al., 2001 | 22 | 8 AD | 39 | Normal | Paraparesis | T5-T9 | - | PD | Complete Recover | 18 |
| Chi JH et al., 2005 | 23 | 24 | 26 | Normal | Paraplegia | C7 | _ | ADF | Complete Recover | 4 |
| Inamasu J et al., 2006 | 24 | 33 | 20 | _ | Paraplegia, BP | L2 | Compression Fracture L2 | Complete Recover | 6 | |
| Yuksel M et al., 2007 | 25 | 28 | 21 | _ | Paraplegia | T9 | _ | PD | Partial Recover | _ |
| Hakan T et al., 2007 | 26 | 1 AD | 36 | Normal | Paraparesis | T5-T6 | _ | PD | Complete Recover | 2 |
| Vijay K et al., 2008 | 27 | 26 | 22 | Normal | Paraplegia | T11 | Recurrence, Reintervention | PDF, VP | Complete Recover | 28 |
| Kiroglu Y et al., 2009 | 28 | 36 | 22 | Normal | Paraplegia | T4 | _ | PDF, Emb, VP | Complete Recover | 6 |
| Blecher R et al., 2010 | 29 | 37 | 35 | Normal | Paraparesis | L4 | PD, VP | Complete Recover | 12 | |
| Shinozaki M et al., 2010 | 30 | 28 | 27 | _ | Paraplegia | T2 | _ | APDF, Emb | Complete Recover | 18 |
| Oppenlander ME et al., 2012 | 31 | 16 AD | 36 | Normal | Paraparesis, AW | C5 | _ | APDF | Partial Recover | 6 |
| Gupta M et al., 2014 | 32 | 28 | 23 | Normal | Paraparesis | T3-T5 | _ | PD | Partial Recover | 3 |
| Jain RS et al., 2014 | 33 | 1 AD | 26 | Normal | Paraplegia | T9 | _ | Refused | _ | _ |
| Moles A et al., 2014 | 34 | 35 | 28 | _ | Paraparesis, BP | T3 | _ | PD, VP | Complete Recover | 18 |
| 35 | 36 | 35 | _ | BP | T7 | Compression Fracture T7 | Complete Recover | 21 | ||
| Silmani O et al., 2014 | 36 | 38 | 19 | _ | Paraplegia | T4 | _ | ADF | Complete Recover | 3 |
| Meng T et al., 2015 | 37 | 24 | 28 | Normal | Paraparesis, BP | T3 | _ | PD | Complete Recover | 63 |
| 38 | 24 | 29 | Premature | Paraparesis, BP | T7 | _ | PD | Complete Recover | 46 | |
| 39 | 24 | 28 | Premature | Paraplegia | T6 | _ | PD | Complete Recover | 43 | |
| 40 | 24 | 39 | Normal | Paraparesis, BP | L1, L3 | _ | PD | Complete Recover | 32 | |
| Staikou C et al., 2015 | 41 | 1 AD | 32 | Normal | BP, LW | L2 | Compression Fracture L2 | PF | Complete Recover | 6 |
| Demirkale I et al., 2016 | 42 | 23 | 40 | Normal | Paraparesis | T1 | _ | Complete Recover | 24 | |
| Korkmaz M et al., 2016 | 43 | 35 | 33 | _ | Paraparesis | T6-T8 | _ | PD, Emb | Complete Recover | _ |
| Fereydonyan N et al., 2017 | 44 | 34 | 28 | Normal | Paraplegia | T5 | Recurrence, Reintervention | APDF | Partial Recover | 3 |
| Bennis A et al 2019 | 45 | 34 | 33 | Normal | Paraplegia | T9-T10 | _ | PD | Complete Recover | 1 |
| Wang GX et al 2019 | 46 | 1 AD | 35 | Normal | Paraparesis | T5 | Compression Fracture T5 | PDF, VP | Partial Recover | 6 |
| Present series | 47 | 2 AD | 21 | Normal | Paraparesis | L1 | Compression Fracture L1 | APDF, Emb | Complete Recover | 24 |
| 48 | 1 AD | 34 | Normal | BP | L1 | Compression Fracture L1 | PF | Complete Recover | 12 | |
| 49 | 14 | 33 | Abortion | Paraplegia, BP | T2 | _ | PDF, Emb | Partial Recover | 3 |
AD: After delivery; ADF: Anterior Decompression with fusion APD: Anterior and Posterior Decompression; APDF: Anterior and Posterior Decompression with fusion; AW: Arm Weakness BP: Back Pain; Emb: Embolization; FI: Fecal Incontinence; LW: Leg Weakness; NC: neurogenic claudication; PD: Posterior Decompression; PDF: Posterior Decompression with Fusion; PF: Posterior Fusion; RT: Radiotherapy; UI: Urinary Incontinence; UR: urinary retention VP: Vertebroplasty.
Present case series
Due to the rapid onset of symptoms in the first case, a prompt decompression and fixation was necessary, but, in consideration of the size of the lesion and the high risk of bleeding, a second stage was requested to complete the L1 corpectomy. First surgical stage was important to regain the lower limb mobility and to guarantee a partial regression of the neurological symptoms that improved more after the second surgical stage. In this case since two different vertebral body were involved the histological analysis was absolutely necessary to differentiate it from other neoplastic lesions.32,43 In the second case, due to the absence of neurological symptoms and in presence of a compression fracture of L1 vertebra, a percutaneous fixation was adequate to obtain good clinical results with all advantages reserved to MIS surgery.47-55
In the third case, the major bleeding during urgent surgery made evident the effectiveness of embolization procedures in angiomatous lesions.
Conclusions
To date the best treatment of aggressive VH in pregnancy is still controversial, many valid options are available, but, from our experience and the review of the literature, the suggestion is to be as radical as possible. A prompt and wide decompression, with or without fixation represent the treatment of choice in case of neurologic compression. Pre-operative embolization of the lesion, when possible, should be performed to avoid major bleeding during surgery. Other options are still a topic of debate.
Funding Statement
Funding: none.
References
- 1.Demirkale İ, De Iure F, Terzi S, Gasbarrini A. Aggressive hemangioma of the spine in a pregnant female: a case report and literature review. Eklem Hastalik Cerrahisi 2016;27:46-50. [DOI] [PubMed] [Google Scholar]
- 2.Moles A, Hamel O, Perret C, et al. Symptomatic vertebral hemangiomas during pregnancy. J Neurosurg Spine 2014;20:585-91. [DOI] [PubMed] [Google Scholar]
- 3.Guthekelch AN. Haemangiomas involving the spinal epidural space. J Neurol Neurosurg Psychiatry 1948;11:199-210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lam RL, Roulhac GE, Erwin HJ. Hemangioma of the spinal canal and pregnancy. J Neurosurg 1951;8:668-71. [DOI] [PubMed] [Google Scholar]
- 5.Askenasy H, Behmoaram A. Neurological manifestations in haemangioma of the vertebrae. J Neurol Neurosurg Psychiatry 1957;20:276-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Field WS, ones JR. Spinal epidural in hemangioma in pregnancy. Neurology 1957;7:825-8. [DOI] [PubMed] [Google Scholar]
- 7.Newman MJ. Spinal angioma with symptoms in pregnancy. J Neurol Neurosurg Psychiatry 1958;21:38-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Newquist RE, Mayfield FH. Spinal angioma presenting during pregnancy. J Neurosurg. 1960;17:541-5. [DOI] [PubMed] [Google Scholar]
- 9.Nelson DA. Spinal cord compression due to vertebral angiomas during pregancy. Arch Neurol 1964;11:408-13. [DOI] [PubMed] [Google Scholar]
- 10.Esparza J, Castro S, Portillo JM, et al. Vetebral hemangiomas: spinal angiography and preoperative embolization. Surg Neurol 1978;10:171-3. [PubMed] [Google Scholar]
- 11.Faria SL, Schlupp WR, Chiminazzo HJr. Radiotherapy in the treatment of vertebral hemangiomas. Int J Radiat Oncol Biol Phys 1985;11:387-90. [DOI] [PubMed] [Google Scholar]
- 12.Lavi E, Jamieson DG, Granat M. Epidural haemangiomas during pregnancy. J Neurol Neurosurg Psychiatry 1986;49:709-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Liu CL, Yang DJ. Paraplegia due to vertebral hemangioma during pregnancy. A case report. Spine 1988;13: 107-8. [DOI] [PubMed] [Google Scholar]
- 14.Schwartz DA, Nair S, Hershey B, et al. Vertebral arch hemangioma producing spinal cord compression in pregnancy. Diagnosis by magnetic resonance imaging. Spine 1989;14:888-90. [DOI] [PubMed] [Google Scholar]
- 15.Poungvarin N1, Bhoopat W. Symptomatic vertebral haemangiomas: report of two cases. J Med Assoc Thai. 1991;74:363-8. [PubMed] [Google Scholar]
- 16.Redekop GJ, Del Maestro RF. Vertebral hemangioma causing spinal cord compression during pregnancy. Surg Neurol 1992;38:210-5. [DOI] [PubMed] [Google Scholar]
- 17.Tekkök IH, Açìkgöz B, Sa!glam S, et al. Vertebral hemangioma symptomatic during pregnancy-Report of a case and review of the literature. Neurosurgery 1993;32:302-6. [DOI] [PubMed] [Google Scholar]
- 18.Ogasawara KK, Ogasawara EM, Hirata G. Pregnancy complicated by von Hippel-Lindau disease. Obstet Gynecol. 1995;85:829-31. [DOI] [PubMed] [Google Scholar]
- 19.Castel E, Lazennec JY, Chiras J, et al. Acute spinal cord compression due to intraspinal bleeding from a vertebral hemangioma: two case-reports. Eur Spine J 1999;8:244-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schwartz TH, Hibshoosh H, Riedel CJ. Estrogen and progesterone receptornegative T11 vertebral hemangioma presenting as a postpartum compression fracture: case report and management. Neurosurgery 2000;46:218-21. [PubMed] [Google Scholar]
- 21.Shapiro GS, Millett PJ, DiCarlo EF, et al. Spinal epidural hemangioma related to pregnancy. Skeletal Radiol. 2001;30:290-4. [DOI] [PubMed] [Google Scholar]
- 22.Chi JH, Manley GT, Chou D. Pregnancy-related vertebral hemangioma. Case report, review of the literature, and management algorithm. Neurosurg Focus 2005;19:E7. [DOI] [PubMed] [Google Scholar]
- 23.Inamasu J, Nichols TA, Guiot BH. Vertebral hemangioma symptomatic during pregnancy treated by posterior decompression, intraoperative vertebroplasty, and segmental fixation. J Spinal Disord Tech 2006;19:451-4. [DOI] [PubMed] [Google Scholar]
- 24.Yuksel M, Yuksel KZ, Tuncel D, et al. Symptomatic vertebral hemangioma related to pregnancy. Emerg Radiol 2007;13:259-63. [DOI] [PubMed] [Google Scholar]
- 25.Hakan T, Demir M, Aker F, Berkman M. Pregnancy-related spinal epidural capillary-cavernous haemangioma: magnetic resonance imaging and differential diagnosis. Australas Radiol. 2007. Oct;51 Spec No.:B6-9. [DOI] [PubMed] [Google Scholar]
- 26.Vijay K, Shetty AP, Rajasekaran S. Symptomatic vertebral hemangioma in pregnancy treated antepartum. A case report with review of literature. Eur Spine J 2008;17:S299-303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kiroglu Y, Benek B, Yagci B, et al. Spinal cord compression caused by vertebral hemangioma being symptomatic during pregnancy. Surg Neurol 2009;71:487-92. [DOI] [PubMed] [Google Scholar]
- 28.Blecher R, Smorgick Y, Mirovsky Y. Symptomatic spinal hemangioma in pregnancy. Isr Med Assoc J 2010;12: 311-3. [PubMed] [Google Scholar]
- 29.Shinozaki M, Morita A, Kamijo K, et al. Symptomatic T2 vertebral hemangioma in a pregnant woman treated by one stage combination surgery; posterior stabilization and anterior subtotal tumor resection. Case report. Neurol Med Chir (Tokyo). 2010;50:674-7. [DOI] [PubMed] [Google Scholar]
- 30.Oppenlander ME, Kalani MY, Dickman CA. Spinal and paraspinal giant cervical cavernous malformation with postpartum presentation. J Neurosurg Spine 2012;16:447-51. [DOI] [PubMed] [Google Scholar]
- 31.Gupta M, Nayak R, Singh H, et al. Pregnancy related symptomatic vertebral hemangioma. Ann Indian Acad Neurol 2014;17:120-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jain RS, Agrawal R, Srivastava T, et al. Aggressive vertebral hemangioma in the postpartum period: an eye-opener. Oxf Med Case Reports. 2014;20;2014:122-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Slimani O, Jayi S, Fdili Alaoui F, et al. An aggressive vertebral hemangioma in pregnancy: a case report. J Med Case Rep. 2014;18;8:207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Meng T, Yin H, Li Z, et al. Therapeuticstrategy and outcome of spine tumors in pregnancy: a report of 21 cases and literature review. Spine (Phila Pa 1976). 2015;1;40:E146-53. [DOI] [PubMed] [Google Scholar]
- 35.Staikou C, Stamelos M, Boutas I, et al. Undiagnosed vertebral hemangioma causing a lumbar compression fracture and epidural hematoma in a parturient undergoing vaginal delivery under epidural analgesia: a case report. Can J Anaesth 2015;62:901-6. [DOI] [PubMed] [Google Scholar]
- 36.Korkmaz M, Gök M, Çınar C, et al. Progressive spinal epidural hemangioma in pregnancy. Spine J 2016;16:e523-5. [DOI] [PubMed] [Google Scholar]
- 37.Fereydonyan N, Taheri M, Kazemi F. Recurrent symptomatic vertebral hemangioma during two consecutive pregnancies: case report and review of the literature. Surg Neurol Int 2017;8: 105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bennis A, Hafiane R, Benouhoud J, et al. Epidural cavernous haemangioma during pregnancy: a case report and a literature review. Pan Afr Med J. 2019;15;33:202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Wang GX, Mu YD, Che JY, et al. Compressive myelopathy and compression fracture of aggressive vertebral hemangioma after parturition: A case report and review of literature. Medicine (Baltimore). 2019;98:e18285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Tamburrelli FC, Meluzio MC, Masci G, et al. Etiopathogenesis of Traumatic Spinal Epidural Hematoma. Neurospine. 2018;15:101-107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Vitiello R, Perisano C, Covino M, et al. Euthyroid sick syndrome in hip fractures: Valuation of vitamin D and parathyroid hormone axis. Injury. 2020. S0020-1383:30013-9. [DOI] [PubMed] [Google Scholar]
- 42.Mühmer M, Bostelmann R, Sarikaya-Seiwert S, et al. Clinical and radiological presentation of spinal epidural haemangiomas: clinical series in a tertiary care centre during a 10-year period. Eur Spine J. 2014;23:404-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Vasudeva VS, Chi JH, Groff MW. Surgical treatment of aggressive vertebral hemangiomas. Neurosurg Focus. 2016;41:E7.. [DOI] [PubMed] [Google Scholar]
- 44.Perna A, Ricciardi L, Barone G, et al. Medical management of acute nonspecific low back pain: comparison of different medical treatments, one center’s retrospective analysis. J Biol Regul Homeost Agents. 2018;32:121-129. [PubMed] [Google Scholar]
- 45.Ricciardi L, Sturiale CL, Pucci R, et al. Patient-Oriented Aesthetic Outcome After Lumbar Spine Surgery: A 1-Year Follow-Up Prospective Observational Study Comparing Minimally Invasive and Standard Open Procedures. World Neurosurg. 2019. 122:e1041-e1046 [DOI] [PubMed] [Google Scholar]
- 46.Proietti L, Schirò GR, Sessa S, Scaramuzzo L. The impact of sagittal balance on low back pain in patients treated with zygoapophysial facet joint injection. Eur Spine J. 2014. Suppl 6:628-33. [DOI] [PubMed] [Google Scholar]
- 47.Scaramuzzo L, Tamburrelli FC, Piervincenzi E, et al. Percutaneous pedicle screw fixation in polytrauma patients. Eur Spine J. 2013;22 Suppl 6:S933-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tamburrelli FC, Scaramuzzo L, Genitiempo M, Proietti L. Minimally invasive treatment of the thoracic spine disease: completely percutaneous and hybrid approaches. Minim Invasive Surg. 2013;2013:508920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Tamburrelli FC, Perna A, Proietti L, et al. The Feasibility of Long-Segment Fluoroscopy-guided Percutaneous Thoracic Spine Pedicle Screw Fixation, and the Outcome at Two-year Followup. Malays Orthop J. 2019;13:39-44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ricciardi L, Stifano V, Proietti L, et al. Intraoperative and Postoperative Segmental Lordosis Mismatch: Analysis of 3 Fusion Techniques. World Neurosurg. 2018;115:e659-e663. [DOI] [PubMed] [Google Scholar]
- 51.Tamburrelli FC, Meluzio MC, Burrofato A, et al. Minimally invasive surgery procedure in isthmic spondylolisthesis. Eur Spine J. 2018;27:237-243. doi: 10.1007/s00586-018-5627-8 [DOI] [PubMed] [Google Scholar]
- 52.Yang Z, Zhang Y, Xu D, et al. Percutaneous vertebroplasty combined with interstitial implantation of 125I seeds in banna mini-pigs. World J Surg Oncol. 2013. 26;11:46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Santagada DA, Meluzio MC, Piccone L, et al. Onset of rhabdomyolysis and acute renal failure after minimally invasive surgery for traumatic spine fracture: a case report. J Biol Regul Homeost Agents. 2019;33:171-174. [PubMed] [Google Scholar]
- 54.Logroscino CA, Tamburrelli FC, Scaramuzzo L, et al. Transdiscal L5-S1 screws for the treatment of adult spondylolisthesis. Eur Spine J. 2012;21: 128-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Barone G, Scaramuzzo L, Zagra A, et al. Adult spinal deformity: effectiveness of interbody lordotic cages to restore disc angle and spino-pelvic parameters through completely mini-invasive transpsoas and hybrid approach. Eur Spine J. 2017. Oct;26:457-463. [DOI] [PubMed] [Google Scholar]