

Abstract
We describe a case of acute myocarditis, which was reported as the main COVID-19 clinical manifestation, with a favorabile outcome. In addition to symptoms, laboratory tests (BNP and troponin), echocardiogram and cardiac MRI contributed to diagnosis. Regardless heart biopsy was not obtained, it is likely an immunological pathogenesis of this condition which pave the way to further therapeutic implications, since there are currently no standardized treatments.
Key words: Myocarditis, COVID-19, SARS-CoV2, Coronavirus, COVID-19 Extrapulmonary Manifestations
Introduction
COVID-19 clinical presentation is characterized by respiratory impairment associated with interstitial pneumonia.1 Viral replication may be followed by a second phase driven by a host inflammatory response. SARS-CoV-2 infection may cause a host hyperimmune response that is associated with an acute respiratory distress syndrome characterized by typical radiological findings.2 The most severe patients may develop a so-called cytokine storm, characterized by the increase of many cytokines that produce long-term damage and lung tissue fibrosis.3 Extrapulmonary manifestations are mainly represented by thrombotic complications, but cardiovascular complications have also been described. Pre-existing cardiac comorbidity is associated with worse outcome while SARS-CoV-2 infection itself has been associated to acute myocardial infarction, massive thromboembolic phenomena and fatal arrhythmias.4,5
The pathogenesis of COVID-19 cardiovascular damage is unknown. At present there is no evidence of SARS-CoV2 infection of myocardial cells. It is considered more likely that cardiovascular impairment may be driven by host inflammatory response.6
Myocarditis mostly recognizes a viral etiology and presents variable clinical patterns, ranging from asymptomatic to cardiogenic shock. More commonly it occurs with symptoms such as tachycardia, tachypnea, dyspnea, and edemas, or more acutely with arrhythmias, chest pain, signs and symptoms of acute heart failure. During the disease status phase, functional investigations show significant alterations: the electrocardiogram (ECG) records alterations in rhythm and conduction or repolarization disorders; in other cases, the ECG simulates alterations observed in acute myocardial infarction or pericarditis. Echocardiography shows a variable reduction in the ejection fraction. Nuclear Magnetic Resonance Imaging (MRI) has progressively established as a reference diagnostic investigation, due to its high sensitivity in identifying even at an early stage the pattern of acute myocardial inflammation, described by a typical impregnation of the contrast medium both at early and late perfusion stage.7 We hereby describe a case of acute myocarditis as the sole extrapulmonary clinical picture of COVID-19.
Case Report
A 49-year-old Hispanic woman was admitted to the emergency room of the Modena University Hospital in March 2020 for fever, chest pain and cough lasting 3 days. Her medical history was not significant. She reported intermittent fever, with a peak at 38.5°, without shivering. Cough was dry, without sputum, associated with constrictive chest pain. She reported dyspnea to daily home living activities. In the emergency room, blood pressure was 120/70 mmHg, heart rate 140 beats per minute, respiratory rate 16 acts per minute, temperature 39°, oxygen saturation 98%. Arterial blood gas analysis showed PO2 69.7 mmHg, PCO2 24.1mmHg, pH 7.40, SO2 96%. PaO2/FiO2 ratio was 331 with no evidence of respiratory failure. The chest radiograph showed diffuse interstitial thickening with consolidation in the right paracardiac site. Blood tests showed leukocytosis with neutrophilia (white blood cells count 19600/mmc, neutrophil 90%), alteration of C reactive protein (44 mg/dl) and procalcitonin (5 ng/ml). Nose-pharyngeal swab was performed and resulted positive infor SARS-CoV2 (polymerase chain reaction, PCR). According to Regional Guidelines for COVID-19 treatment,8 she received hydroxychloroquine 400 mg x 2 on day 1 and 2 and then 200 mg x 2 from day 4 to day 6, and antithrombotic prophylaxis with low-molecular-weight heparin (4000 U once a day as a standard prophylactic dose for weight under 100 kg), and antibiotic therapy with ceftriaxone 2 g/day and azithromycin 500 mg/day due to the increase in neutrophils and procalcitonin under the suspicion of bacterial infection.
Chest pain suggested an electrocardiogram, which documented right bundle branch block detection and widespread alterations of repolarization. The troponin curve, performed at 6 hour interval after admission showed the following values 820, 699, 593, 326 ng/L with further decrease in the following days, until negative at day 5. The type B natriuretic peptide (BNP) was 950 pg/mL and normalized at day 4. The echocardiogram showed a slight reduction in the ejection fraction (45%), slight pericardial effusion without signs of cardiac tamponade, moderate mitral insufficiency, a pattern compatible with myocarditis. Cardiac MRI performed on day 5, showed slight depression of the ejection fraction (54%), without significant alterations in the contractility of both ventricles (Table 1), widespread increase in myocardial T2 signal intensity (ratio with skeletal muscle 2.2-2.5), moderate pericardial effusion at the posterior lateral wall of the left ventricle (Figure 1). In accordance with the position statement of the European Society of Cardiology of 2013 and the subsequent focus on the diagnostic value of Cardiac MRI of 2017,9,10 the patient had two clinical presentation criteria (acute chest pain, newonset of dyspnoea at rest or exercise, and/or fatigue) and three diagnostic criteria (ECG alterations such as previously unknown bundle branch block, myocardiocytolysis markers, functional and structural abnormalities on cardiac imaging at echo and MRI) of myocarditis.
The consultant cardiologist suggested therapy with sotalol 50 mg x 2, acylsalicylic acid 100 mg/day and ramipril 2.5 mg per day. The patient presented a progressive general improvement, with reduction up to disappearance of chest pain on day 7 after admission. During the second week of hospitalization echocardiogram showed a clear reduction in pericardial effusion and normal ejection fraction (55%). Holter ECG showed no significant changes in the records. ECG discharge showed only nonspecific abnormalities of repolarization. On day 12, the patient was discharged at home.
Discussion and Conclusions
Cardiac involvement is an established feature of many viral infections and notably also in infections by other members of the Coronaviridae family, including MERSCoV. 11,12 Myocarditis during COVID-19 disease may be the cause of death. A Chinese autoptic study that analyzed 68 deaths from SARS-CoV2 infection showed that 7% were due to myocardial damage or acute heart failure.13 We described a new case of COVID-16 related myocarditis with benign evolution. Two previous case reports with adverse outcome were recently reported. 12,14 The second one, with a fulminant course, required corticosteroid-based rescue therapy. In this case the pulmonary component was less significant than the cardiac component.15
A similar case of fulminant myocarditis in the absence of lung infection had been described by Zeng et al. in a patient with SARS-CoV2 infection.16 The main limitation in this case report is the lack of a heart biopsy, which could have proven the viral or the immune-mediated pathogenesis. Nevertheless MRI is very sensible in the diagnosis of myocarditis supporting clinical and ultrasound signs. From a clinical point of view, it is important to underline that dyspnea and chest pain symptoms are present both in pneumonia and myocarditis. Clinician should therefore pay great attention to discriminate between the two different possible organ involvement of the same infection, in order to better direct the diagnostic- therapeutic process. BNP was the markers that better correlated with symptoms and recovery and should be considered as a routine marker to be evaluated in COVID-19.17 No standard treatment for myocarditis due to COVID-19 infection exists. Our case had a favorable outcome in the context of a general clinical improvement and underwent to a standard therapeutic protocol of our centre for the treatment of hospitalized SARS-CoV2 patients (hydroxychloroquine and anticoagulant).
In consideration of the inflammatory driven pathogenetic hypothesis of this condition, steroids or IV immunoglobulins could be considered in severe cases in analogy to the treatment of other virally inducted myocarditis.18
In conclusion, myocarditis may represent the main clinical picture of COVID-19. The prognosis of this condition may vary. Troponin, BNP, echocardiogram and cardiac MRI were useful to guide diagnosis and monitor clinical evolution.
Table 1.
Volume parameters at cardiac MRI (body surface area 2,18 m2).
| Volume parameters | Normal values (female 18-80 years) | |
|---|---|---|
| Left ventricle volume parameters | ||
| ED volume | 169,3 mL | (90-174 mL) (61-95 mL/m²) |
| ES volume | 77,4 mL | (25-63 mL) (17-35 mL/m²) |
| Stroke volume | 91,9 mL | (60-116 mL) (40-64 mL/m²) |
| Ejection fraction | 54,2% | (58-76 %) |
| Cardiac output | 6,9 L/min | |
| LV mass ED | 132,1 g | (70-142 g) (47-77 g/m²) |
| Right ventricle volume parameters | ||
| ED volume | 171,6 mL | (89-177mL) (60-96 mL/m²) |
| ES volume | 82,2 mL | (23-75 mL) (14-42 mL/m²) |
Figure 1.
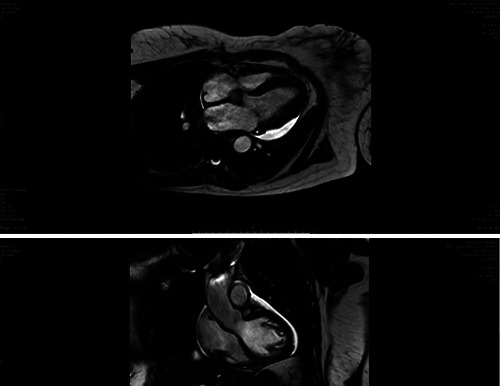
Cardiac MRI findings.
Acknowledgements
Vanni Borghi, Luca Corradi, Andrea Bedini, Gabriella Orlando, Marianna Meschiari, Cinzia Puzzolante, Antonella Santoro, Carlotta Rogati, Giacomo Ciusa, Marco Tutone, Erica Bacca, Matteo Faltoni, Giacomo Franceschi, Vittorio Iadisernia, Giulia Burastero, Sara Volpi, Dina Yaacoub, Jovana Milic, from Azienda Ospedaliero-Universitaria di Modena, Infectious Diseases Clinic – University of Modena and Reggio Emilia. Ivana Castaniere, Roberto Tonelli, Luca Tabbì, Riccardo Fantini, Filippo Gozzi, from Azienda Ospedaliero- Universitaria di Modena, Pneumology Clinic – University of Modena and Reggio Emilia. Caterina Vacchi, from Azienda Ospedaliero- Universitaria di Modena, Rheumatology Clinic – University of Modena and Reggio Emilia.
Funding Statement
Funding: None.
References
- 1.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel corona-virus in Wuhan, China. Lancet 2020;395:497-506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shi H, Han X, Jiang N, et al. Radiological findings from 81 patients with COVID-19 pneu-monia in Wuhan, China: a descriptive study. Lancet Infect Dis 2020;20:425-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm' in COVID-19. J Infect 2020;S0163-4453:30165-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Driggin E, Madhavan MV, Bikdeli B, et al. Cardiovascular Considerations for Patients, Health Care Workers, and Health Systems During the Coronavirus Disease 2019 (COVID-19) Pan-demic. J Am Coll Cardiol 2020;S0735-1097:34637-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Car-diovascular System: A Review. JAMA Cardiol 2020. doi:10.1001/jamacardio.2020.1286. [DOI] [PubMed] [Google Scholar]
- 6.Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respira-tory di-stress syndrome. Lancet Respir Med 2020;8:420-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Friedrich MG, Sechtem U, Schulz-Menger J, et al. ; International Consensus Group on Cardio-vascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocar-ditis: A JACC White Paper. J Am Coll Cardiol 2009;53:1475-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Indirizzi terapeutici della Regione E-R per il trattamento della infezione da SARS-CoV2 (COVID-19). Available from: https://salute.regione.emiliaromagna.it/farmaci/covid-19/indirizziterapeutici-covid19-rer.pdf. [Google Scholar]
- 9.Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagno-sis, ma-nagement, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013;34:2636-48. [DOI] [PubMed] [Google Scholar]
- 10.Biesbroek PS, Hirsch A, Zweerink A, et al. Additional diagnostic value of CMR to the Euro-pean So-ciety of Cardiology (ESC) position statement criteria in a large clinical population of patients with su-spected myocarditis. Eur Heart J Cardiovasc Imaging 2018;19: 1397-407. [DOI] [PubMed] [Google Scholar]
- 11.Alhogbani T. Acute myocarditis associated with novel Middle east respiratory syndrome coro-navirus. Ann Saudi Med 2016;36:78-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Riski H, Hovi T, Frick MH. Carditis associated with coronavirus infection. Lancet 1980;2:100-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an ana-lysis of data of 150 patients from Wuhan, China. Intensive Care Med 2020;1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Inciardi RM, Lupi L, Zaccone G, et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID- 19). JAMA Cardiol 2020. doi:10.1001/jamacardio.2020.1096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hu H, Ma F, Wei X, Fang Y. Coronavirus fulminant myocarditis treated with glucocorticoid and hu-man immunoglobulin. Eur Heart J 2020. doi:10.1093/eurheartj/ehaa190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zeng JH, Liu YX, Yuan J, et al. First case of COVID-19 complicated with fulminant myocar-ditis: a case report and insights. Infection 2020. doi:10.1007/s15010-020-01424-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with corona-virus di-sease 2019: retrospective study. BMJ 2020;368:m1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Maisch B, Alter P. Treatment options in myocarditis and inflammatory cardiomyopathy : Fo-cus on i. v. immunoglobulins. Herz 2018;43:423–30. [DOI] [PMC free article] [PubMed] [Google Scholar]