

Dear Editors,
We read with interest both the survey on impact of the COVID‐19 pandemic on functional investigations in Europe 1 and the ESNM recommendations to be applied in the recovery phase of the pandemic. 2
Besides complying with the ESNM recommendations, we felt reasonable to devise a modified surgical mask to be worn by the patient during esophageal manometry and pH (impedance) catheters positioning, two potentially aerosol‐generating procedures.
In order to adapt surgical masks for functional esophageal tests, two holes are made using a scalpel (Figure 1A): a smaller one (1‐2 mm) for introduction of topical lignocaine spray 3 and passage of the manometry catheter (hole A) on the upper border of the mask, just below the nose wire in the paramedian position (left or right, according to which nostril is chosen), and a slightly bigger one (3 mm) for the passage of the straw or needle adaptor of a syringe for water swallowing (hole B) placed just below the upper horizontal fold of the mask, one third the distance from the median line to the lateral border of the mask. Both holes are made by cutting the tissue along two perpendicular lines in order to preserve it.
FIGURE 1.
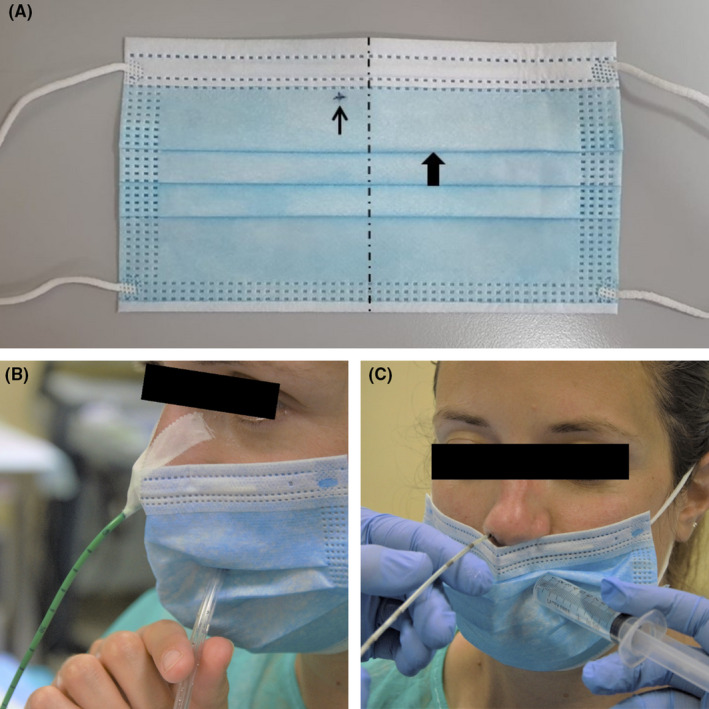
A, Modified surgical mask. Please note hole A (thin arrow) and hole B (thick arrow). B, Rapid drink challenge during high‐resolution esophageal manometry with the use of the modified mask. Please note the manometry catheter passing through hole A and the straw through hole B. C, pH impedance catheter positioning with the use of the modified mask. Please note the adaptor of the syringe through hole B
Procedure: Before intubating the patient, his/her mask is replaced with the adapted one. Then, lignocaine is sprayed through hole A followed by the catheter which is inserted into the nostril, positioned, and fixed to the nose with sticky tape. Single water swallows, multiple rapid swallowing, and rapid drink challenge are performed 4 with a syringe or a straw dipping in a glass passed through hole B, as shown in Figure 1B. At the end of the test, once the catheter has been removed, the mask is replaced with a standard one. If pH (impedance) needs performing after manometry, the modified mask is not removed and is positioned covering the mouth only. Intubation is performed while the nurse helps giving water through hole B, as shown in Figure 1C. Once the catheter is in place and secured with tape, the mask is removed and the patient is fitted with a standard one.
Since resumption of our activity in the recovery phase of the pandemic, we have performed 37 high‐resolution esophageal manometry procedures using this mask and no alteration in the quality of tracings has been observed.
We believe that this simply modified cheap mask is an add‐on measure to be used by HCPs in the forthcoming months, in order to ensure safe functional esophageal testing.
CONFLICT OF INTEREST
No competing interests declared.
AUTHOR CONTRIBUTIONS
RP devised the modified mask. RB, EA, and RP tested the mask, contributed to writing manuscript, and approved final version.
REFERENCES
- 1. Tack J, Schol J, Geeraerts A, et al. A survey on the impact of the COVID‐19 pandemic on motility and functional investigations in Europe and considerations for recommencing activities in the early recovery phase. Neurogastroenterol Motil. 2020;32(7):e13926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Tack J, Vanuytsel T, Serra J, et al. European Society for Neurogastroenterology and Motility recommendations for conducting gastrointestinal motility and function testing in the recovery phase of the COVID‐19 pandemic. Neurogastroenterol Motil. 2020;32(7):e13930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wahba G, Neshkova E, Vuille‐Lessard É, Bouin M. Is topical lidocaine beneficial before catheter insertion in esophageal manometry and ambulatory pH monitoring? Neurogastroenterol Motil. 2019;31(10):e13687. [DOI] [PubMed] [Google Scholar]
- 4. Savarino E, de Bortoli N, Bellini M, et al. Practice guidelines on the use of esophageal manometry – A GISMAD‐SIGE‐AIGO medical position statement. Dig Liver Dis. 2016;48(10):1124‐1135. [DOI] [PubMed] [Google Scholar]