

Abstract
The current health pandemic that has plagued the global of which the global south‐Nigeria is not insulated from is the premise for this empirical investigation. The present study relies on recent annual time‐series data to conceptualize the hypothesized claim via Pesaran's Autoregressive distributed lag techniques. Empirical findings from the bounds test traces the long‐run relationship between public health expenditure and economic growth over the study span. However, unlike previous studies, we introduce life expectancy and death rates in the model framework. Although health expenditure is not significant, empirical results show that a 1% increase in life expectancy and death rate increases and decreases economic growth by 3.85 and 1.84%, respectively. This suggests the need for Health Policymakers in Nigeria to implement active strategies that reduce the death rate, which is a blueprint for active engagement in the face of a global pandemic such as COVID‐19.
1. INTRODUCTION
Good Health care and quality of life is said to be a life asset globally and affiliated to each other, that is, health and economic growth are correlated making it a fundamental factor of sustainable economic growth. The country's economy is propelled by building a healthy population, to understand the future generations income, the life cycle model explains the affiliation between the citizen's health status, wealth and expenditure (Interalia Lilliard & April, 1997; Rice & Smith, 1999). On the other hand, diminishing and unsustainable economic is seen when the quality of life and health status is poor but if otherwise then a fueled upswing of the economy is developed (see World Health Organization, 1999). For a stable economy, the united nation layout a vision for 2030 which is known as the “17 Sustainable Development Goals (SDGs)” which part includes Good healthcare services that reduce mortality at all level and engender sustainable economic growth, Economic growth, sustainability, education, and partnership to achieve the goal. These life‐changing goals signify that a healthy population is proportional to the economic growth of the country. Several quality studies have proven that building a healthy population is a lifetime asset concerning building undiminishing economic and strong economic development 1 (Fernandes, 2020; Yaqub, Ojapinwa, & Yussuff, 2012).
According to the WHO world health report, an agreement was made by Africa rulers in 2001 to focus on health expenditure to achieve the health Millennium Development Goals (MDGs) to raise the economics of Africa. Furthermore, 15% of the government's expenditure is to be allocated to the health sector to attain this goal but by 2013 only five countries accomplished this target, namely Botswana, Rwanda, Zambia, Madagascar, and Togo. Nigeria as a country could not meet up, nevertheless, enrolment of strategy and plans for an increase in Health capital expenditure and economic growth was implemented by the governments, according to the study carried out by Oni (2014), health expenditure, and labor force productivity are paramount to the economic development of Nigeria and positive outcome in health expenditure was recorded from 1970 to 2010, but the results were inconsistent yearly according to AFDB (2011); World Bank (2013) and UNECA (2012), the health expenditure budgetary are as follows respectively for each year from 2008 to 2014. 9.19, 7.63, 7.63, 7.42, 7.43, 6.48, and 8.17%. These results revealed the importance of good quality of life and its relationship with economic growth, and so the Nigerian government is encouraged to priorities building a healthy population (Yaqub et al., 2012).
In late 2019 a virus caused a disaster in Wuhan, Hubei province China named “Novel Pneumonia Coronavirus Disease‐2019 (COVID‐19)” and was declared as a global pandemic Andersen, Rambaut, Lipkin, Holmes, & Garry, 2020. The virus outbreak was disturbing due to its fast‐spreading ability and contagious, The world health organization daily record list for the virus cases keeps emerging globally, however, a decline was seen from China infected cases where it was first prominent as of when this article was drafted, meanwhile, a drastic increase in infected cases emerged in Europe, America, and Africa. Emergency action was taken by the WHO to protect human life due to the risk prevalent of the virus. The global pandemic of COVID‐19 has increased mortality rate and beyond that, a severe diminish is seen on the global economy due to the decrease in production, consumption, unemployment, and decrease in quality of life. Even thou the global economic diminish seems unavoidable the governments are putting more effort to sustain the economic development during and after the pandemic. Fernandes (2020).
Based on the highlighted position, the current study seeks to explore to what extent public health expenditure impede/engender sustainable economic growth for the case of global south‐Nigeria. In a nutshell, the present study aims to find solution to the question? Looking at the severe outbreak of (COVID‐19), Will economic growth be sustainable or crash amidst the global health pandemic crises? This study aims to use Nigeria as a case study for the global south blocs for more insightful and policy constructions in the country and region at large to attain the “vision 2030” of the UN and much more the goal‐3 of UNSDG's.
The remainder of this study is structured as: Section 2 presents the review of related literature. Section 3 renders the data and methodological sequences while empirical results and discussion. The conclusion and policy blueprint are highlighted in Section 5.
2. LITERATURE REVIEW
Various studies have been conducted for the past years similar to this by different scholars, aiming to draw the attention of government, public, and private sector to how health care, environment, and health status has a significant impact on economic growth and also to investigate if the government can establish sustainable growth in economic especially for the period of health crises. Piabuo and Tieguhong (2017) conducted an analytical research study on five African countries that achieved the MDGs goal from 2001 to 2013 and countries in the CEMAC sub‐region. Econometric technics analysis was used which results indicate an increase in GDP per capita by 0.38 unit for five African countries that meet the target of allocating 15% of their government expenditure on health and 0.3unit for CEMAC, signifying that significant change in GDP per capital can only be prominent if there is a positive change in health expenditure. Ibikunle (2019) supported this, indicating a positive increase in GDP using the Ordinary Least Square (OLS) and the Granger causality test techniques to analyze the impact of health on economic growth, which was concluded that an increase in government expenditure on health should be considered so to achieve the goal of economic growth. On contrary to this, Olisakwe (2019) argued that an increase in budgetary allocation for health has negative outcomes on economic growth this was proven by extracting data from 1981 to 2017 in Nigeria using a classical linear regression technique to conduct the investigation. Nwani and Kelikume (2019) deducted the same conclusion as Olisakwe (2019) using the Toda‐Yamamoto technique to investigate the causal relationship between health expenditure, health status and economic growth in Nigeria from the period of 1981–2018. The investigation results indicate a negative non‐interdependent between government health expenditure and economic development of the country and thereby suggests that focusing on the link between these two is pointless.
Investigating more proves either positive or negative impact of health status, environmental economic growth, and expenditure on health care, respectively. Nwani, Kelani, Ozegbe, and Babatunde (2018) explored a study to investigate the influence of the environment on health status and the effect of health expenditure on Nigeria health status from 1981 to 2017 by ARDL estimation technique, the result points out a significant negative effect of environmental pollution in Nigerians Focusing on the bad effect of capita CO2 emission on human health. According to the finding, a positive outcome was prominent on health expenditure outcomes for the past 37 years. The government should allocate more budgetary to the health care sector as well as monitor environmental pollution to maintain good wellbeing. Eneji, Dickson, and Onabe (2013) also reported a similar outcome by supporting the positive interrelationship between health expenditure, health status, and economic development, focusing on applied economics in public healthcare expenditure between 1999 and 2012 in Nigeria. The result of the investigation implied that good health is a country's big asset, so people's health status portrays the country's economic growth. The investigation by Edeme, Emecheta, and Omeje (2017) validates Eneji et al. (2013) result outcomes.
Ahmad and Hasan (2016) conducted a study in Malaysia between 1984 and 2009. The result based on Autoregressive Distributed Lag (ARDL) cointegration framework classified that health status outcomes, public health expenditure, and governance have a stable long‐run relationship making them correlated. Sharma (2018) validates the result outcomes by Ahmad and Hasan (2016). Similarly, with the same method Erçelik (2018) examined turkey health output and economic growth for the period of 1980–2015, bound test results revealed that co‐integration shows a positive variable connection between Turkey's government health output and economic growth. It can be deduced that health expenditure has a positive impact on economic development in the long run.
Dinçer and Yuksel (2019) used the Pedroni panel cointegration method and Dumitrescu Hurlin panel causality analysis to evaluate the total, public, and private health expenditure and economic growth of E7 countries between the period of 1996 and 2016. The result discovers two important aspects, an obvious long‐run relationship between total/public health expenditure with Economic growth and Negative economic growth contribution in private health care expenditure. The impact of the private health sector on economic growth is quite low, the private sector should improve and be re‐evaluated.
Kim and Lane (2013) studied the 17 OECD countries with a mixed‐effect model to critically evaluate the link connecting Public health output, national health outcomes, and impact of recent changes in healthcare policy in the United States. The study focused on infant mortality rate and life expectancy at birth, the finding indicated negative and positive result accordingly, no link between government health expenditure and infant mortality rate meanwhile and an obvious link between government health expenditure and life expectancy at birth was seen. Doğan, Tülüce, and Doğan (2014) also used OECD countries to analyze the health expenditure for the period of 1995–2011 by ARDL methodology. The result proved positivity in the age Dependency Ratio on health care expenditures but unexpected influence in a decrease in expenditure is seen in the increased population among young workers.
3. DATA, MODEL, AND METHOD
3.1. Data and variables
This section presents the data, variables description and methodological procedures applied to address the hypothesized study claim for the case of Nigeria. 2 Subsequently the materials and method accordingly.
3.2. Model and method
To carry out the empirical assessment necessary to achieve the aim of this study, we present a standard growth equation with labor, capital, trade and foreign direct investment as the required control variable. However, as a novelty, we introduced three different measures for the health sector. First is the standard health expenditure as a percentage of GDP. Results from this are compared with other health sector proxies such as life expectancy and death rate. Given that COVID‐19 has significantly influenced the death rate across many countries, the death rate and its impact on real GDP will provide valuable insights in times of pandemic such as this. Hence, our model is shown in the following equations below:
| (1) |
| (2) |
| (3) |
The autoregressive distributed lag model is used to estimate the models in Equations (1) to (3). Before doing this, however, pre‐estimation diagnostics are conducted as well as post estimation check after all model diagnostics and main estimations are concluded.
4. DISCUSSION OF RESULTS AND IMPLICATION OF FINDINGS
4.1. Pre‐estimation diagnostics
Table 2 gives the descriptive statistics of the variables of interests employed in the study which includes mean value, SD, minimum and maximum. The total number of observations is pegged at 30. As shown in Table 2, the results of the descriptive statistics are presented in log and variable. When the variables are logged, real GDP is shown to have the highest mean value of $7.492 million with the minimum and maximum values of $7.207 million and $7.849 million, respectively while the least of the logged variables is the foreign direct investment (FDI) with the mean value of $0.431 million and with minimum and maximum of $ − 0.693 million and $1.756 million, respectively. At level, the same result is found with changes in the values. Lastly, the table also presents the SD which explains the degree at which the data varies from their mean values.
TABLE 1.
Description of variables
| Variable symbol | Description | Source |
|---|---|---|
| RGDP = GDP per capita, constant 2010 dollars | GDP per capita is gross domestic product divided by midyear population. GDP is the sum of gross value added by all resident producers in the economy plus any product taxes and minus any subsidies not included in the value of the products. It is calculated without making deductions for depreciation of fabricated assets or depletion and degradation of natural resources. Data are in constant 2010 U.S. dollars. | The World Bank |
| CAP = capital investment as a percent of GDP | Gross capital formation (formerly gross domestic investment) consists of outlays on additions to the fixed assets of the economy plus net changes in the level of inventories. Fixed assets include land improvements (fences, ditches, drains, and so on); plant, machinery, and equipment purchases; and the construction of roads, railways, and the like, including schools, offices, hospitals, private residential dwellings, and commercial and industrial buildings. Inventories are stocks of goods held by firms to meet temporary or unexpected fluctuations in production or sales, and “work in progress.” According to the 1993 SNA, net acquisitions of valuables are also considered capital formation. | The World Bank |
| LAB = labor force, million people | Labor force comprises people ages 15 and older who supply labor for the production of goods and services during a specified period. It includes people who are currently employed and people who are unemployed but seeking work as well as first‐time jobseekers. Not everyone who works is included, however. Unpaid workers, family workers, and students are often omitted, and some countries do not count members of the armed forces. Labor force size tends to vary during the year as seasonal workers enter and leave. | The World Bank |
| TOT = terms of trade, base year = 2000 | Net barter terms of trade index is calculated as the percentage ratio of the export unit value indexes to the import unit value indexes, measured relative to the base year 2000. Unit value indexes are based on data reported by countries that demonstrate consistency under UNCTAD quality controls, supplemented by UNCTAD's estimates using the previous year's trade values at the standard international trade classification three‐digit level as weights. To improve data coverage, especially for the latest periods, UNCTAD constructs a set of average prices indexes at the three‐digit product classification of the standard international trade classification revision 3 using UNCTAD's commodity Price statistics, internaχtional and national sources, and UNCTAD secretariat estimates and calculates unit value indexes at the country level using the current year's trade values as weights. | The United Nations |
| FDI = foreign direct investment, percent of GDP | Foreign direct investment is the net inflows of investment to acquire a lasting management interest (10% or more of voting stock) in an enterprise operating in an economy other than that of the investor. It is the sum of equity capital, reinvestment of earnings, other long‐term capital, and short‐term capital as shown in the balance of payments. This series shows net inflows (new investment inflows less disinvestment) in the reporting economy from foreign investors and is divided by GDP. | The World Bank |
| HEA = health spending per capita | Current expenditures on health per capita in current US dollars. Estimates of current health expenditures include healthcare goods and services consumed during each year. | The World Bank |
| LEXP = life expectancy, in years | Life expectancy at birth indicates the number of years a newborn infant would live if prevailing patterns of mortality at the time of its birth were to stay the same throughout its life. | The World Bank |
| DRT = death rate, per 1,000 people | Crude death rate indicates the number of deaths occurring during the year, per 1,000 population estimated at midyear. Subtracting the crude death rate from the crude birth rate provides the rate of natural increase, which is equal to the rate of population change in the absence of migration. | The World Bank |
TABLE 2.
Summary statistics
| Variable | Obs. | Mean | SD | Min | Max |
|---|---|---|---|---|---|
| Variables at log | |||||
| LRGDP | 30 | 7.492 | 0.242 | 7.207 | 7.849 |
| LCAP | 30 | 3.302 | 0.426 | 2.701 | 3.974 |
| LLAB | 30 | 3.724 | 0.225 | 3.367 | 4.106 |
| LTOT | 30 | 4.712 | 0.497 | 3.781 | 5.415 |
| LFDI | 30 | 0.431 | 0.610 | ‐0.693 | 1.756 |
| LHEA | 19 | 4.074 | 0.582 | 2.875 | 4.681 |
| LLEXP | 30 | 3.883 | 0.060 | 3.825 | 3.988 |
| LDRT | 30 | 2.769 | 0.154 | 2.473 | 2.923 |
| Variables at level | |||||
| RGDP | 30 | 1845.52 | 452.05 | 1,348.68 | 2,563.90 |
| CAP | 30 | 29.59 | 12.18 | 14.90 | 53.19 |
| LAB | 30 | 42.46 | 9.57 | 28.98 | 60.70 |
| TOT | 30 | 124.72 | 58.73 | 43.88 | 224.77 |
| FDI | 30 | 1.85 | 1.25 | 0.50 | 5.79 |
| HEA | 19 | 66.73 | 27.84 | 17.72 | 107.87 |
| LEXP | 30 | 48.65 | 2.95 | 45.84 | 53.95 |
| DRT | 30 | 16.12 | 2.37 | 11.86 | 18.60 |
To have a better understanding of the variables, Figure 1 shows the graphical illustrations of the trend of the variables of interest. As shown in Figure 1, capital investment (CAP) is revealed to be the most fluctuating variable followed by the real GDP and health expenditure. This implies the inconsistencies of the variables over time.
FIGURE 1.
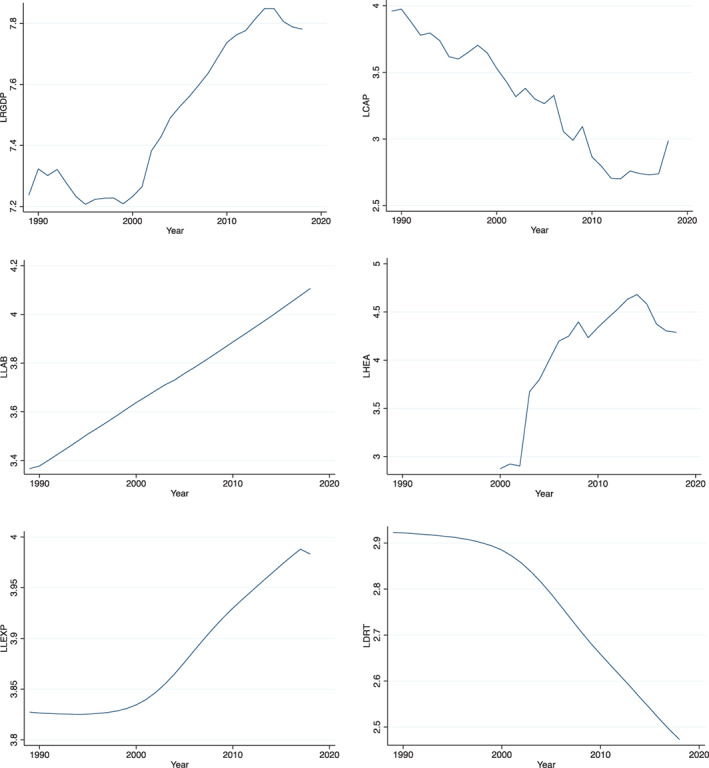
Trend of variables
Table 3 presents the results of the correlation analysis between the variables of interest. The result of the association between real GDP and health expenditure as well as life expectancy reveals that there is a strong and significant positive association that supports the theoretical construct in the literature while a strong and significant negative relationship is discovered between real GDP and death rate. The association between real GDP and terms of trade as well as labor force is found to be strong, positive and significant, whereas, a weak and significant negative relationship is found between real GDP and foreign direct investment. Capital investment is shown to have a strong and significant negative relationship with real GDP.
TABLE 3.
Pairwise correlation
| LRGDP | LCAP | LLAB | LTOT | LFDI | LHEA | LLEXP | LDRT | |
|---|---|---|---|---|---|---|---|---|
| LRGDP | 1 | |||||||
| – | ||||||||
| LCAP | −0.9371* | 1 | ||||||
| 0.0000 | – | |||||||
| LLAB | 0.9200* | −0.9635* | 1 | |||||
| 0.0000 | 0.0000 | – | ||||||
| LTOT | 0.8750* | −0.8482* | 0.7967* | 1 | ||||
| 0.0000 | 0.0000 | 0.0000 | – | |||||
| LFDI | −0.2385 | 0.2726 | −0.3587 | −0.0553 | 1 | |||
| 0.2043 | 0.145 | 0.0516 | 0.7716 | – | ||||
| LHEA | 0.9365* | −0.8460* | 0.7938* | 0.8405* | −0.2929 | 1 | ||
| 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.2236 | – | |||
| LLEXP | 0.9725* | −0.9381* | 0.9552* | 0.8059* | −0.3298 | 0.8381* | 1 | |
| 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0751 | 0.0000 | – | ||
| LDRT | −0.9603* | 0.9314* | −0.9612* | −0.7864* | 0.3594 | −0.8034* | −0.9980* | 1 |
| 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0511 | 0.0000 | 0.0000 | – |
4.2. Model diagnostics
We confirm the validity of the estimated model using analytical tests presented in Table 4 and Figure 2. The model validity tests carried out in this study include normality test using Lagrange Multiplier Jarque‐Bera technique, heteroscedasticity test using Breusch‐Pagan/Cook‐Weisberg approach, functional misspecification using Ramsey RESET test, multicollinearity test employing Variance inflation factor, IM‐test and CUSUM using Cameron & Trivedi's decomposition technique and lastly, stability test using CUSUMSQ graphical illustration.
FIGURE 2.
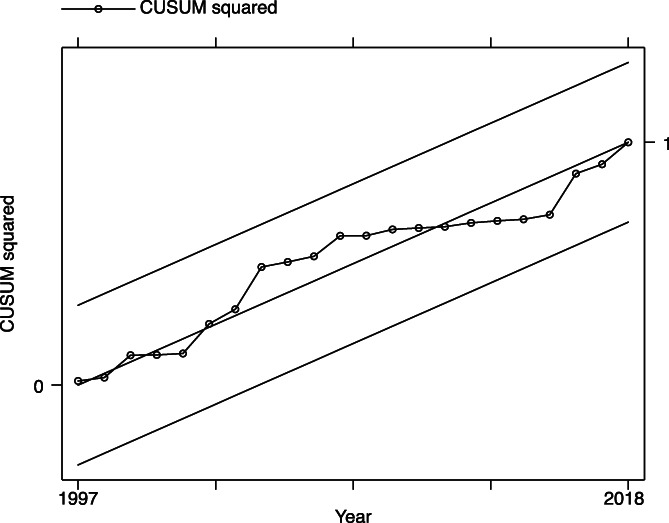
Recursive cusum
Subsequently, after exploring the summary statistics and correlation matrix, it is also imperative to examine the stationary properties of the variables of interest. Table 5 presents the Augmented Dickey‐Fuller (ADF) and Philip‐Perron (PP) unit root tests employed in the study to examine the order of integration of the variables. The estimates from the Dickey‐Fuller unit‐roots confirm that all the variables are non‐stationary at level but stationary at first difference except for the FDI that is stationary at both level and first difference. Also, the results obtained from Philip‐Perron unit root test reveals that all the variables of interest are stationary at first difference while only TOT and FDI are found to be stationary at level.
TABLE 4.
Model verification and validation
| Lagrange multiplier Jarque‐Bera normality test | |||
|---|---|---|---|
| Lags (p) | Chi2 | df | p>chi2 |
| 1 | 2.01776 | 2 | .36463 |
| Breusch‐pagan/cook‐Weisberg test for heteroskedasticity | |||
| Chi2 (1) | 0.33 | p>chi2 | .5634 |
| Ramsey RESET test | |||
| F (3, 20) | 4.75 | p>F | .0116 |
| Variance inflation factor | |||
| Variable | VIF | 1/VIF | |
| LLAB | 1.17 | 0.854413 | |
| LFDI | 1.14 | 0.879885 | |
| LLEXP | 1.11 | 0.899184 | |
| LCAP | 1.11 | 0.901391 | |
| LTOT | 1.09 | 0.92134 | |
| Mean VIF | 1.12 | ||
| Cameron and Trivedi's decomposition of IM‐test | |||
| Source | Chi2 | df | p value |
| Heteroskedasticity | 14.11 | 20 | .825 |
| Skewness | 2.56 | 5 | .767 |
| Kurtosis | 1.3 | 1 | .2538 |
| Total | 17.97 | 26 | .8768 |
4.3. Estimation results
After conducting the tests for the unit roots, the next step is to examine if at all there is the existence of long run equilibrium between the variables. Therefore, ARDL bound test technique coined by Pesaran et al (2001) is employed in this current study to test for cointegration as shown in Table 6. The results of ARDL bound test approach shows that, in most cases, the F‐statistics is valued above at least the 10% upper bound which is an avenue to establish long run equilibrium between the variables of interest.
TABLE 5.
Unit root test
| Dickey‐Fuller test | Philip‐Perron | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Level | p | First diff. | p | Level | p | First diff. | p |
| LRGDP | −0.211 | .9373 | −3.370 | .0120 | −0.464 | .8989 | −3.564 | .0065 |
| LCAP | −1.398 | .5830 | −4.726 | .0001 | −1.414 | .5754 | −4.683 | .0001 |
| LLAB | 2.669 | .9991 | −9.122 | .0000 | 2.515 | .9991 | −7.467 | .0000 |
| LTOT | −1.203 | .6722 | −4.925 | .0000 | −1.074 | .7252 | −4.947 | .0000 |
| LFDI | −3.184 | .0209 | −6.675 | .0000 | −3.307 | .0146 | −7.063 | .0000 |
| LHEA | −2.455 | .1269 | −3.502 | .0079 | −2.609 | .0911 | −3.537 | .0071 |
| LLEXP | 2.427 | .9990 | −0.891 | .7909 | 1.265 | .9964 | −7.877 | .0000 |
| LDRT | 6.067 | 1.0000 | −7.446 | .0000 | 3.104 | 1.0000 | −7.101 | .0000 |
Since the ARDL bound test approach has confirmed that that the variables of interest to this study are cointegrated, the long run and short‐run equilibrium can then be estimated. Table 7 shows the empirical findings of the short run and long run equilibrium nexus using the ARDL modeling approach and the analysis covers three models with real GDP as the sole dependent variable. Accordingly, the result of the impact of health expenditure on real GDP is found to be negative and insignificant both in the short run and the long run. Specifically, a 1% increase in health expenditure will lead to an insignificant 0.09% reduction in the real GDP. This result is partially consistent with the empirical findings of Bakare, Sanmi, and S (2011) who discovered a positive and significant impact of health expenditure on the Nigerian economy. This result has shown the triviality of the effect of health expenditure on the advancement of the Nigerian economy and this can be best explained from the low budgetary allocation for healthcare in the country.
TABLE 6.
Pesaran, Shin, and Smith (2001) ARDL bounds test
| 10% | 5% | 1% | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Bound | I(0) | I(1) | I(0) | I(1) | I(0) | I(1) | I(0) | I(1) | F/t statistic |
| F | 2.634 | 3.923 | 3.221 | 4.704 | 4.672 | 6.63 | .013 | .065 | 4.404 |
| t | −2.559 | −3.856 | −2.934 | −4.315 | −3.718 | −5.275 | .003 | .059 | −4.208 |
Life expectancy in the contrary exhibits a significant positive impact on the real GDP in both the short run and the long run. This result validates the empirical findings of Mahyar (2016) for Iran and Ngague and Manfred (2015) for 141 developing countries. The findings show that a 1% increase in life expectancy will directly cause a significant increase in GDP by 3.16 and 3.85 in the short run and long run respectively. The implication of this is that having a high life expectancy will provide the Nigerian economy with the necessary labor force to improve the productivity of the country in terms of her GDP.
As expected, death rate is found to pose a significant threat to the economic advancement of the country. The findings reveal that a 1% increase in the number of death cases recorded in the country will directly cause a significant reduction in the GDP by about 1.84% in the long term and by about 1.54% in the short run. This result implies that high death rate in a country could render the country with lesser manpower to efficiently carry out her productive activities which in turn influence the economic advancement of the country.
For the control variables, the estimated coefficients of capital investments show that both in the short run and long run, capital investment has negative and insignificant effects on the dependent variable. Specifically, a 1% increase in capital investment will cause the GDP to reduce by 0.03, 0.002, and 0.05%, respectively in the short run and by 0.1, 0.002, and 0.05% in the long run across the three models. However, the results are not significant. The empirical findings of Obialor (2017) for three Sub‐Saharan African countries including Nigeria. This implies that more capital accumulation tends to cause the Nigerian economy to experience a downturn due to ways through which the capital is channeled. The results obtained from the analysis also indicate that labor force across the three models has negative but insignificant impact on health expenditure both in short run and long run in such a way that a 1% increase in results 28.26% reduction in GDP for the first model. Meanwhile, the results of analyses modeled for life expectancy and death rate reveal a negative and significant effect of labor force on GDP both in the short run and long run such that a percent increase in labor force will reduce the GDP by 7.05 and 9.04%, respectively in the short run and by 8.58 and 10.83%, respectively in the long run. This implies that labor force has neutrally disrupted the advancement of the economy of Nigeria.
The coefficients of terms of trade are positive and insignificant across all the three models exemplified in the study both in the short run and long run. Specifically, the results indicate that 1% increase in terms of trade will cause the GDP to increase by 0.16% in the first model, to increase by 0.02% in the second model and increase by 0.01% for the third model in the long run while the short run coefficients of the GDP for the first model is 0.04% rise, rises by 0.02 and 0.01% rise in GDP when terms of trade increases by 1%. The result obtained is in contrary to the study conducted by Jebran, Iqbal, Bhat, and Ali (2018) for Pakistan. However, the effect of terms of trade tends to be insignificant to the Nigerian economy owing to the excessive reliance of the economy on importation.
In contrast, foreign direct investment is found to influence the GDP negatively and insignificantly across the three models. For instance, 1% increase in foreign direct investment will inversely cause GDP by 0.02, 0.01, 0.01%, respectively across the three models in the short run while the long run estimations show a negative and insignificantly such that a 1% increase in FDI leads to 0.07, 0.01, and 0.01% in the long run across the three models. The result of the analysis is partially consistent with the study conducted by Alvarado, Iniguez and Ponce (2017) for lower‐middle‐income countries. This shows that FDI has neutral effect on the economic growth in Nigeria.
While Table 7 indicates that all the tests carried out in the study are well behaved and align with expectations attached to the estimated results, the stability of the estimated model is also confirmed with Figure 2 that presents the CUSUM and CUSUMSQ plotted within 95% degree of confidence. Therefore, there is a possibility of making unbiased statistical derivations, interpretations and policy recommendations.
TABLE 7.
ARDL regression with short‐run and long‐run equilibrium relationship
| Variables | Model 1 with health expenditure per capita | Model 2 with life Expectancy in years | Model 3 with death rate per 1,000 people |
|---|---|---|---|
| EC (−1) | −0.244 | −0.822*** | −0.835*** |
| (0.462) | (0.195) | (0.194) | |
| Long run | |||
| LCAP | −0.103 | −0.00235 | −0.0542 |
| (0.285) | (0.0716) | (0.0680) | |
| LLAB | −28.26 | −8.576* | −10.83** |
| (51.90) | (4.314) | (4.179) | |
| LTOT | 0.157 | 0.0247 | 0.0139 |
| (0.464) | (0.0337) | (0.0330) | |
| LFDI | −0.0691 | −0.0134 | −0.00932 |
| (0.189) | (0.0134) | (0.0130) | |
| LHEA | −0.356 | ||
| (0.956) | |||
| LLEXP | 3.847** | ||
| (1.513) | |||
| LDRT | −1.839** | ||
| (0.683) | |||
| Short run | |||
| D.LCAP | −0.0252 | −0.00193 | −0.0453 |
| (0.0685) | (0.0588) | (0.0565) | |
| D.LLAB | −6.888 | −7.047* | −9.043** |
| (4.369) | (3.845) | (3.998) | |
| D.LTOT | 0.0384 | 0.0203 | 0.0117 |
| (0.0542) | (0.0260) | (0.0266) | |
| D.LFDI | −0.0169 | −0.0110 | −0.00778 |
| (0.0222) | (0.0101) | (0.0102) | |
| D.LHEA | −0.0867 | ||
| (0.0777) | |||
| D.LLEXP | 3.161** | ||
| (1.476) | |||
| D.LDRT | −1.536** | ||
| (0.680) | |||
| Constant | 0.189 | 0.178* | 0.222** |
| (0.119) | (0.101) | (0.103) | |
| Observations | 18 | 28 | 28 |
| R‐squared | 0.474 | 0.557 | 0.566 |
Note: Dependent variable: LRGDP. Standard errors in parentheses.***p < .01, ** p < .05, *p < .1.
TABLE 8.
Granger causality tests
| Causality test (H0) | Statistics | p value | Direction of causality |
|---|---|---|---|
| LCAP does not granger‐cause LRGDP | 3.25* | .0818 | Bi‐directional |
| LRGDP does not granger‐cause LCAP | 3.67* | .0636 | |
| LLAB does not granger‐cause LRGDP | 0.38 | .7709 | Unidirectional |
| LRGDP does not granger‐cause LLAB | 11.04** | .0032 | |
| LTOT does not granger‐cause LRGDP | 3.05* | .0922 | Unidirectional |
| LRGDP does not granger‐cause LTOT | 2.05 | .1792 | |
| LFDI does not granger‐cause LRGDP | 2.01 | .2128 | No causality |
| LRGDP does not granger‐cause LFDI | 2.37 | .1650 | |
| LHEA does not granger‐cause LRGDP | 0.13 | .7227 | Unidirectional |
| LRGDP does not granger‐cause LHEA | 29.55*** | .0002 | |
| LLEXP does not granger‐cause LRGDP | 1.50 | .2480 | No causality |
| LRGDP does not granger‐cause LLEXP | 2.36 | .1214 | |
| LDRT does not granger‐cause LRGDP | 1.31 | .3173 | No causality |
| LRGDP does not granger‐cause LDRT | 1.85 | .1790 |
Note: *, **, and *** represent significance at 10, 5, and 1%, respectively.
4.4. Granger causality tests
The presence of cointegration between the variables of interest has provided the evidence for the existence of at least one causality nexus between the variables though could not provide the direction of the causality. Thus, we employ the popular Granger causality test in this study to examine which variable serves as a causative agent to the other. The Granger causality test results are presented in Table 8. Empirical evidence shows that, there exists a one‐way directional relationship moving from the health expenditure to productivity growth while no causal relationship is found between economic growth and life expectancy and also between economic growth and death rate.
The empirical results obtained from the causality tests reveal the validity of feedback hypothesis such that bi‐directional causal relationship is discovered between economic growth and capital investment, unidirectional relationship separately running from labor force and terms of trade to economic growth. Meanwhile, no causality is discovered between foreign direct investment (FDI) and productivity growth.
Efforts to compare the results of the current study to the previous show that one‐way directional causal relationship exists moving from expenditure on healthcare to productivity growth found in this current study is contrary to the empirical study of Dincer, Hacioglu, and Yüksel (2018) and Mehrara and Musai (2011) who also found a one‐way directional causal relationship running from economic growth to health expenditure for E7 countries and Iran respectively. Another conflicting result is that of Ecevit (2013) who found a one‐way directional causal relationship moving from life expectancy to productivity growth.
5. CONCLUSION AND POLICY IMPLICATIONS
This study employs the ARDL model and Granger causality to investigate the relevance of life expectancy, death rate and public health expenditure to the sustainability of economic growth in Nigeria amidst the Nobel Coronavirus Disease‐2019 (COVID‐19).
The empirical findings from the ARDL approach reveal that health expenditure has negative impact on economic growth. However, the impact is found to be insignificant. As regards the Granger causality tests, unidirectional causal relationship is found running from health expenditure to economic growth. These findings show that health expenditure is a core factor that can be undertaken to improve the economic growth and development of the Nigerian economy. It indicates that Nigeria could gain from the agility of her labor force if more investments are directed towards improving the healthcare system.
The empirical results also show the significant positive effect of life expectancy on economic growth. Surprisingly, the results obtained from the Granger causality tests reveal that there is no causal relationship between the two variables. The results indicate the influence of high life expectancy span on the promotion of economic growth in Nigeria given the fact that there is no evidence to support the existence of a causal relationship between the variables in question.
The expected empirical result is found for the impact of death rate on economic growth and of which is negative and significant. Regarding the causality test, no causal relationship is found between economic growths between death rate as duly expected theoretically. This result suggests that if death rate becomes consistent in the country, it could hinder the economic growth and development of the country through labor force channel.
From the findings stated above, it is therefore recommended that the Nigerian government to prioritize investment in human capital development through the provision of healthcare facilities, personnel training, monitoring and evaluation, and making the access to the healthcare facilities affordable. Embarking on these will not only assure the provision of the quality labor force but also translate to an increase in the productive capacity of the country and an increase in economic growth.
Furthermore, since it is clear that the health sector in Nigeria is underfunded and underdeveloped, this is a call on the government to increase the investment in the health sector in the country and such investments should be directed towards fighting off leading death‐causing diseases such as tuberculosis, pneumonia and influenza that tend to cut the life expectancy in the country short.
Lastly, the Nigerian government should strongly consider the provision of an economically friendly environment as well as a secured environment for business to grow and this should be the ultimate responsibility of people in power and managers of the economy. Facts have been duly established in this current study that unemployment increases mortality and negatively affects life expectancy and increased unemployed youths tend to increase the number of dependents in the country, increase the inequality gap and make medical access care burdensome. Thus, it is recommended in this study that the government should focus on making policies that increase employment opportunities and productive capacities of the citizens.
Biographies
Gloria Nnadwa Alhassan is currently a Ph.D. student at the faculty of Pharmacy, Cyprus International University, Turkish Republic of Northern Cyprus (TRNC), and also doubles as a research/demonstration research assistant at Cyprus International University. She obtained a bachelor's and a master's degree in Pharmacy. Her research interest covers clinical pharmacy, public health, and more recently biotechnology although not limited to these. Her research papers are indexed in top‐tier outlets like the Journal of Public Affairs. She can be further contacted via galhassan@ciu.edu.tr alternatively gloriaalhassan@yahoo.com
Festus Fatai Adedoyin is a fellow of the Higher Education Academy, UK and a demonstrator at the Department of Accounting, Economics and Finance, Bournemouth University, UK. His research interests include energy and tourism economics, tourism taxation and consumer behaviour.
Festus Victor Bekun currently serves as an Assistant professor at Istanbul Gelisim University Turkey and a senior research fellow at South Ural State University Russia. His research interests is in the areas of agricultural economics, energy and environmental economics, and tourism economics. His research studies have appeared in top‐tier journals including Science of The Total Environment, Energy & Environment, Heliyon, Environmental Science and Pollution Research, Journal of Public Affairs, International Journal of Green Energy, Sage Open, Resources Policy, Journal of Economic Structures, The Journal of Economic Asymmetries. He could further be contacted via this email: fbekun@gelisim.edu.tr or bekunfestusvictor@yaho.com
Terhemen Justine Agabo is a researcher at the deparment of Econonomics, University of Ibadan, Nigeria. His research interests cover development economics, energy economics and tourism economics.
Alhassan GN, Adedoyin FF, Bekun FV, Agabo TJ. Does life expectancy, death rate and public health expenditure matter in sustaining economic growth under COVID‐19: Empirical evidence from Nigeria? J Public Affairs. 2021;21:e2302. 10.1002/pa.2302
Endnotes
For brevity, more insights into UNSDG's see https://www.sightsavers.org/policy-and-advocacy/global-goals/?gclid=EAIaIQobChMIl8SI8Y-76AIVk08YCh3KGAVDEAAYAiAAEgL-1fD_BwE
The data span is from 1989 to 2018. The selected variables are described in Table 1. All data accessed May 2020 from WDI database
REFERENCES
- AFDB , 2011. Africa Economic outlook 2011. African Development Bank Annual Report.
- Ahmad, R. , & Hasan, J. (2016). Public health expenditure, governance and health outcomes in Malaysia. Jurnal Ekonomi Malaysia, 50(1), 29–40. [Google Scholar]
- Alvarado, R. , Iniguez, M. , & Ponce, P. (2017). Foreign direct investment and economic growth in Latin America. Economic Analysis and Policy, 56, 176–187. 10.1016/j.eap.2017.09.006 [DOI] [Google Scholar]
- Andersen, K. G. , Rambaut, A. , Lipkin, W. I. , Holmes, E. C. , & Garry, R. F. (2020). The proximal origin of SARS‐CoV‐2. Nature Medicine, 26, 450–452. 10.1038/s41591-020-0820-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bakare, A. S. , Sanmi, O. , & S, C. A. B . (2011). Health care expenditure and economic growth in Nigeria: An Empirical Study, 2(2), 83–87. [Google Scholar]
- Bank, T. W . (2013). Government Expenditure on Education. Available from http://data.worldbank.org/indicator/SE.XPD.TOTL.GD.
- Dincer, H. , & Hacioglu, Ü . (2018). Strategic design and innovative thinking in business operations, Series: Contributions to Management Science, Springer International Publishing. 10.1007/978-3-319-77622-4 [DOI] [Google Scholar]
- Dinçer, H. , & Yuksel, S. (2019). Identifying the causality relationship between health expenditure and economic growth: An application on E7 countries. Journal of Health Systems and Policies, 1(1), 5–23. [Google Scholar]
- Doğan, İ. , Tülüce, N. S. , & Doğan, A. (2014). Dynamics of health expenditures in OECD countries: Panel ARDL approach. Theoretical Economics Letters, 4(08), 649–655. [Google Scholar]
- Ecevit, E. (2013). The impact of life expectancy on economic growth: Panel cointegration and causality analyses for OECD countries. The International Journal of Social Sciences, 16(1), 1–14. [Google Scholar]
- Edeme, R. K. , Emecheta, C. , & Omeje, M. O. (2017). Public health expenditure and health outcomes in Nigeria. American Journal of Biomedical and Life Sciences, 5(5), 96–102. [Google Scholar]
- Eneji, M. A. , Dickson, V. J. , & Onabe, B. J. (2013). Health care expenditure, health status and national productivity in Nigeria (1999–2012).
- Erçelik, G. (2018). The relationship between health expenditure and economic growth in Turkey from 1980 to 2015. Journal of Politics, 1(1), 1–8. [Google Scholar]
- Fernandes, N. (2020). Economic effects of coronavirus outbreak (COVID‐19) on the world economy. Available from SSRN 3557504.
- Ibikunle, J. A. (2019). Life expectancy, public health spending and economic growth in Nigeria. Social Sciences, 8(6), 369–376. [Google Scholar]
- Jebran, K. , Iqbal, A. , Bhat, K. , & Ali, A. (2018). Effect of terms of trade on economic growth of China effect of terms of trade on economic growth of China, (September). 10.1177/2394901518795068 [DOI]
- Kim, T. K. , & Lane, S. R. (2013). Government health expenditure and public health outcomes: A comparative study among 17 countries and implications for US health care reform. American International Journal of Contemporary Research, 3(9), 8–13. [Google Scholar]
- Lilliard, L. A. , & April, Y. W. (1997). Uncertain health and survival: Effects on endof‐life consumption. Journal of Business & Economic Statistics, 15, 254–268. [Google Scholar]
- Mahyar, H. (2016). Economic growth and life expectancy: The case of Iran. Studies in Business and Economics, 11(11), 80–87. 10.1515/sbe-2016-0007 [DOI] [Google Scholar]
- Mehrara, M. , & Musai, M. (2011). The Causality between Health Expenditure and Economic Growth, 2(August), 13–19.
- Ngague, N. , & Manfred, K. (2015). The impact of life expectancy on economic growth in developing countries. Asian Economic and Financial Review, 5(4), 653–660. [Google Scholar]
- Nwani, S. E. , Kelani, F. A. , Ozegbe, A. E. , & Babatunde, O. H. (2018). Public health expenditures, environmental pollution and health outcomes: Evidence from Nigeria. South Asian Journal of Social Studies and Economics, 1–15. [Google Scholar]
- Nwani, S. E. , & Kelikume, I. (2019). Causal linkage amongst public expenditure on health, health status and Growth: New empirical evidence from Toda‐Yamamoto approach for Nigeria. Journal of Scientific Research and Reports, 1–13. [Google Scholar]
- Obialor, M. C. (2017). Effect of government human capital investment on economic growth in sub‐Saharan Africa: Evidence from Nigeria, South Africa and Ghana ( 1980–2013) contribution/originality. International Journal Of Asian Social Science, 7(4), 328–339. 10.18488/journal.1/2017.7.4/1.4.328.339 [DOI] [Google Scholar]
- Olisakwe, O. (2019). Public health expenditure, economic growth and health outcomes in Nigeria. Public Health, 6(1), 23–32. [Google Scholar]
- Oni, L. B. (2014). Analysis of the growth impact of health expenditure in Nigeria. Journal of Economics and Finance, 3(1), 77–84. [Google Scholar]
- Pesaran, M. H. , Shin, Y. , & Smith, R. J. (2001). Bounds testing approaches to the analysis of level relationships. Journal of Applied Econometrics, 16(3), 289–326. [Google Scholar]
- Piabuo, S. M. , & Tieguhong, J. C. (2017). Health expenditure and economic growth‐a review of the literature and an analysis between the economic community for central African states (CEMAC) and selected African countries. Health Economics Review, 7(1), 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rice, N. , & Smith, P. (1999). Approaches to capitation and risk adjustment in health care: an international survey, University of York, England: The Centre for Health Economics. [Google Scholar]
- Sharma, R. (2018). Health and economic growth: Evidence from dynamic panel data of 143 years. PLoS One, 13(10), e0204940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UNECA , 2012. Economic transformation for Africa's development. United Nations Economic Commission for Africa, macroeconomic policy division, C‐10 Meeting April, Washington D, C. [Google Scholar]
- World Health Organization . (1999). WHO on health and economic productivity. Population and Development Review, 25(2), 396–401. [Google Scholar]
- Yaqub, J. , Ojapinwa, T. , & Yussuff, R. (2012). Public health expenditure and health outcome in Nigeria: The impact of governance. European Scientific Journal, 8(13), 189–201. [Google Scholar]